
Human Papillomavirus Vaccine Impact and Effectiveness in Six High-Risk Populations: A Systematic Literature Review


Abstract
:1. Introduction
2. Methods
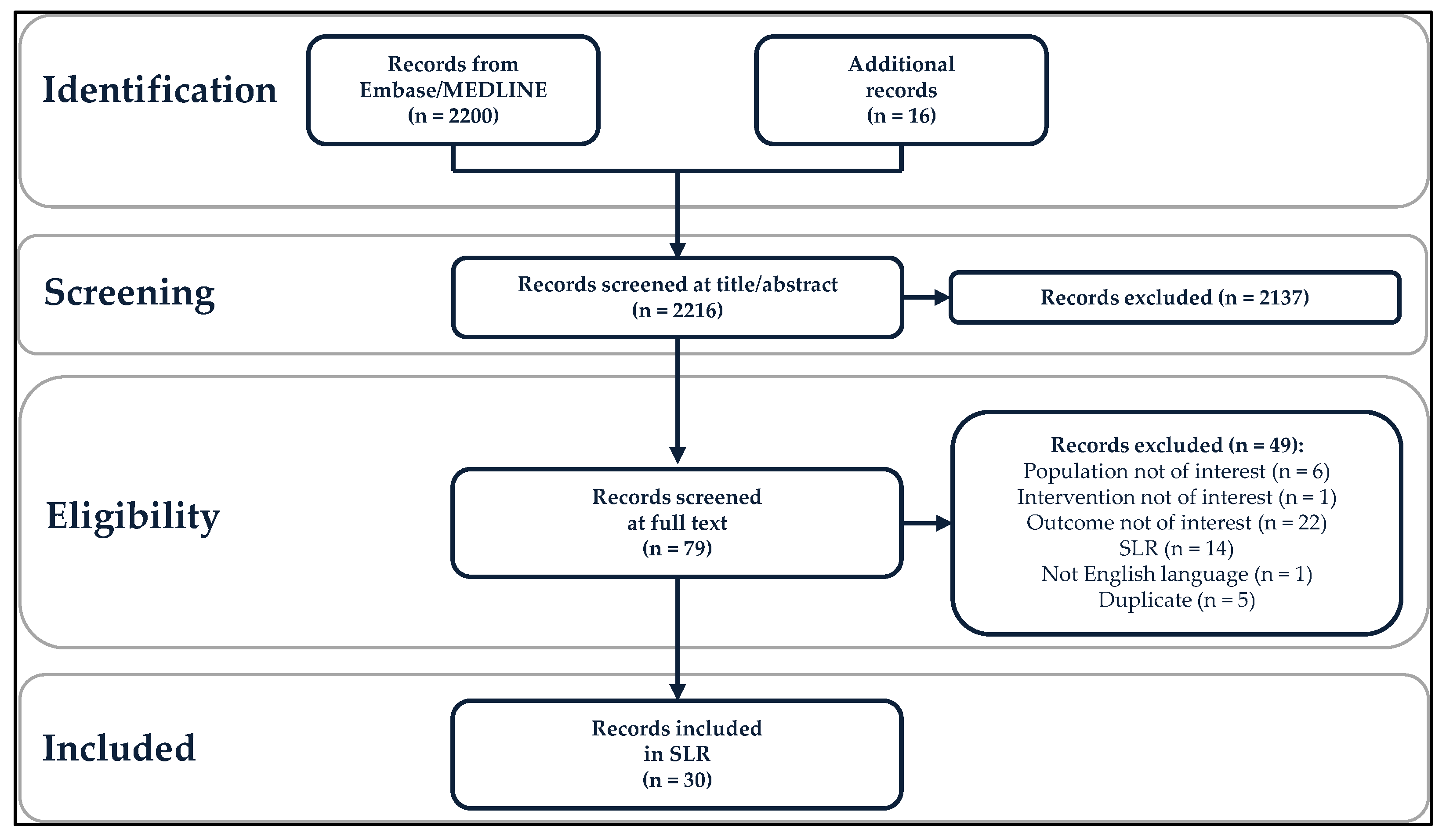
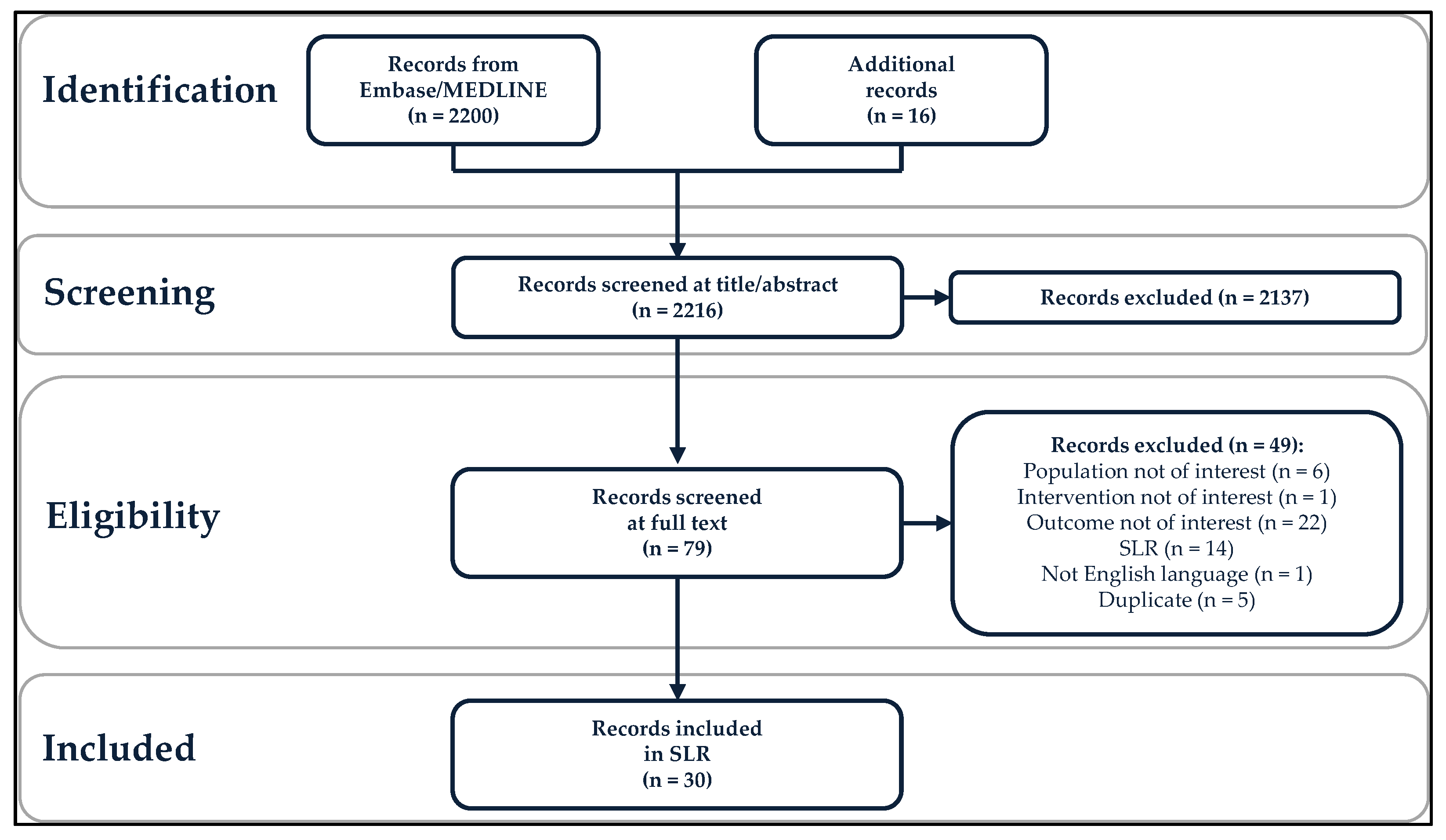
2.1. Study Inclusion Criteria and Search Strategy
2.2. Data Extraction and Data Analysis
3. Results
3.1. Vaccine Use in Included Studies
3.2. Effectiveness and Impact in High-Risk Groups
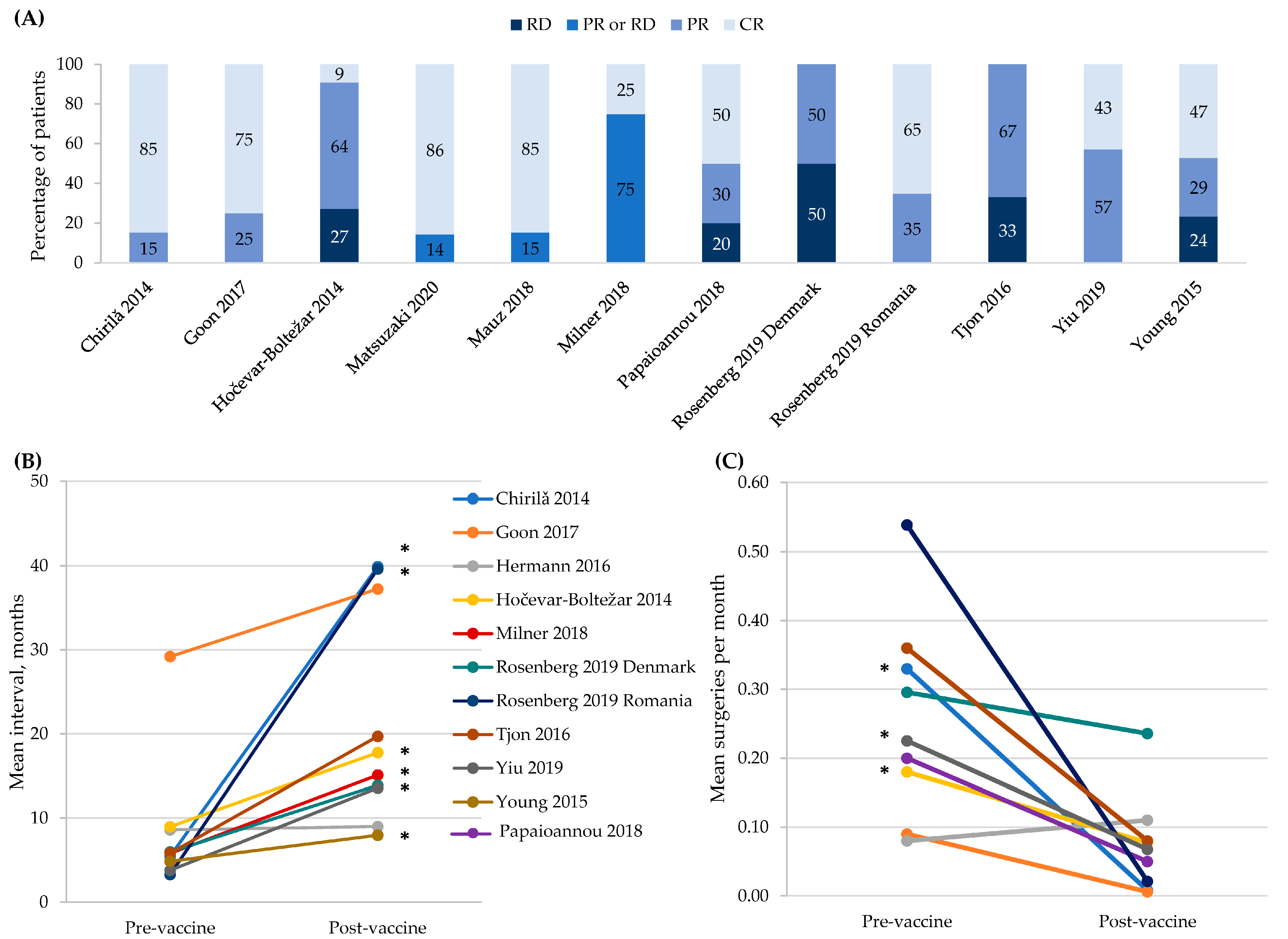
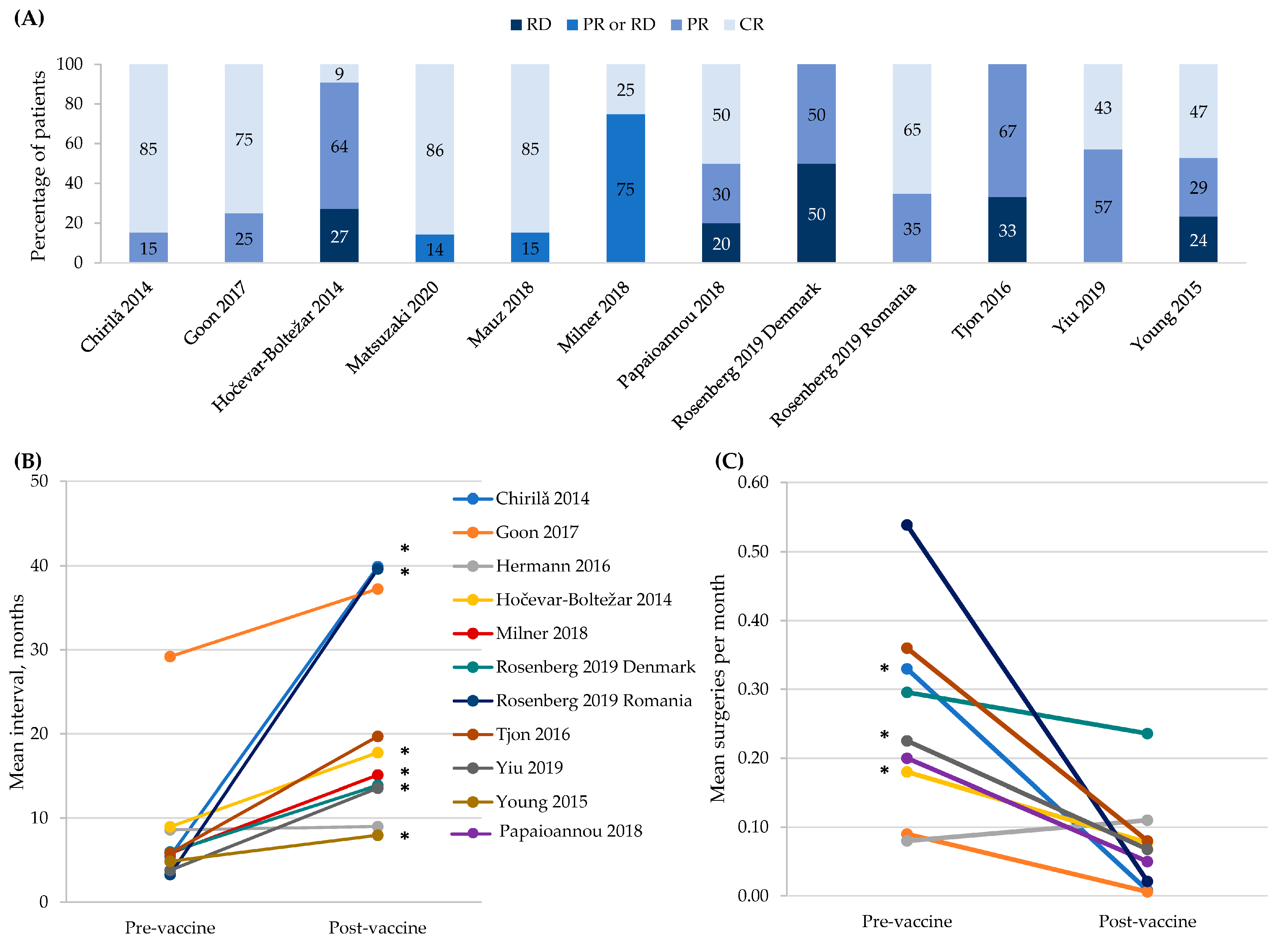
3.3. Patients with RRP
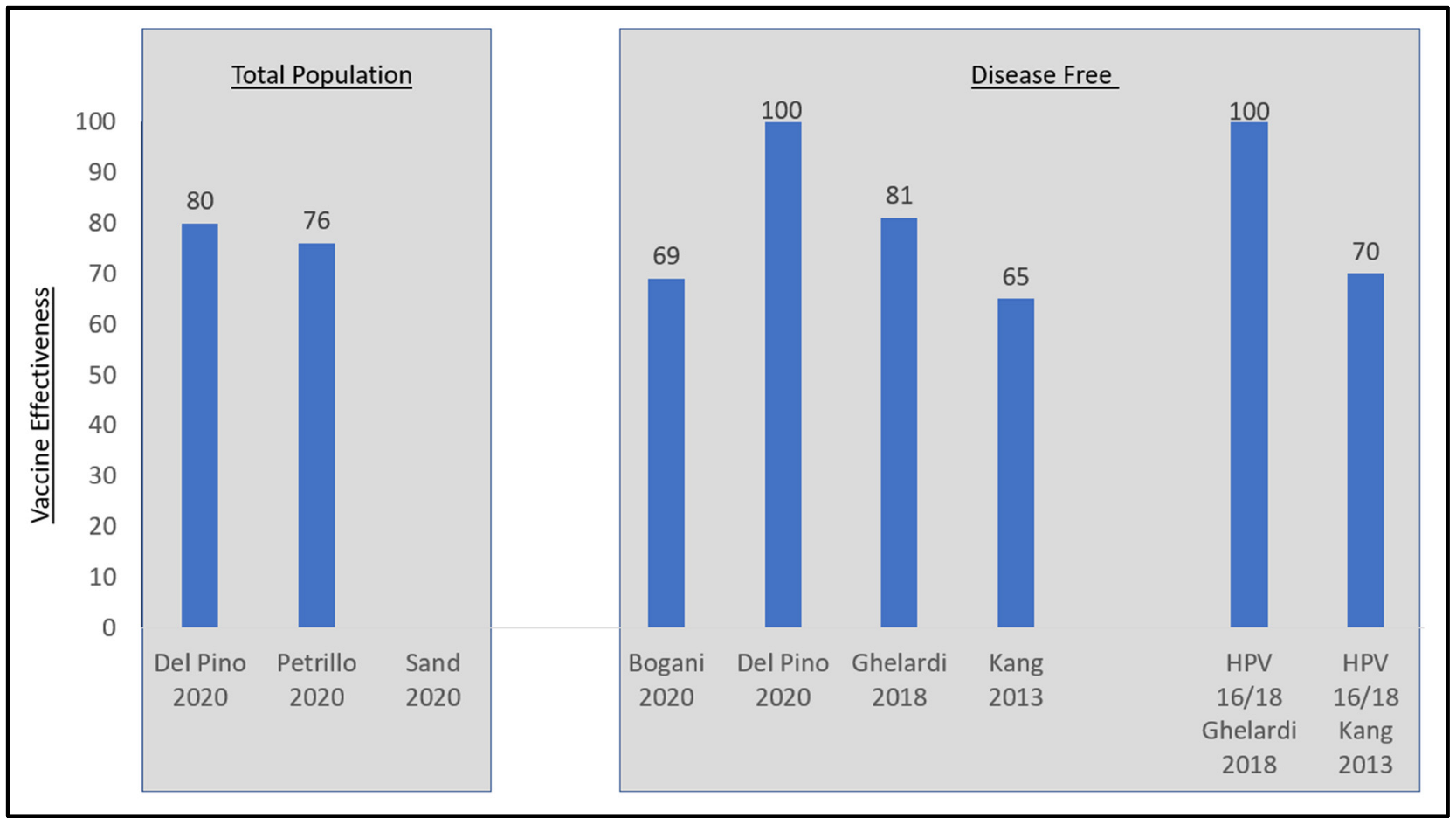
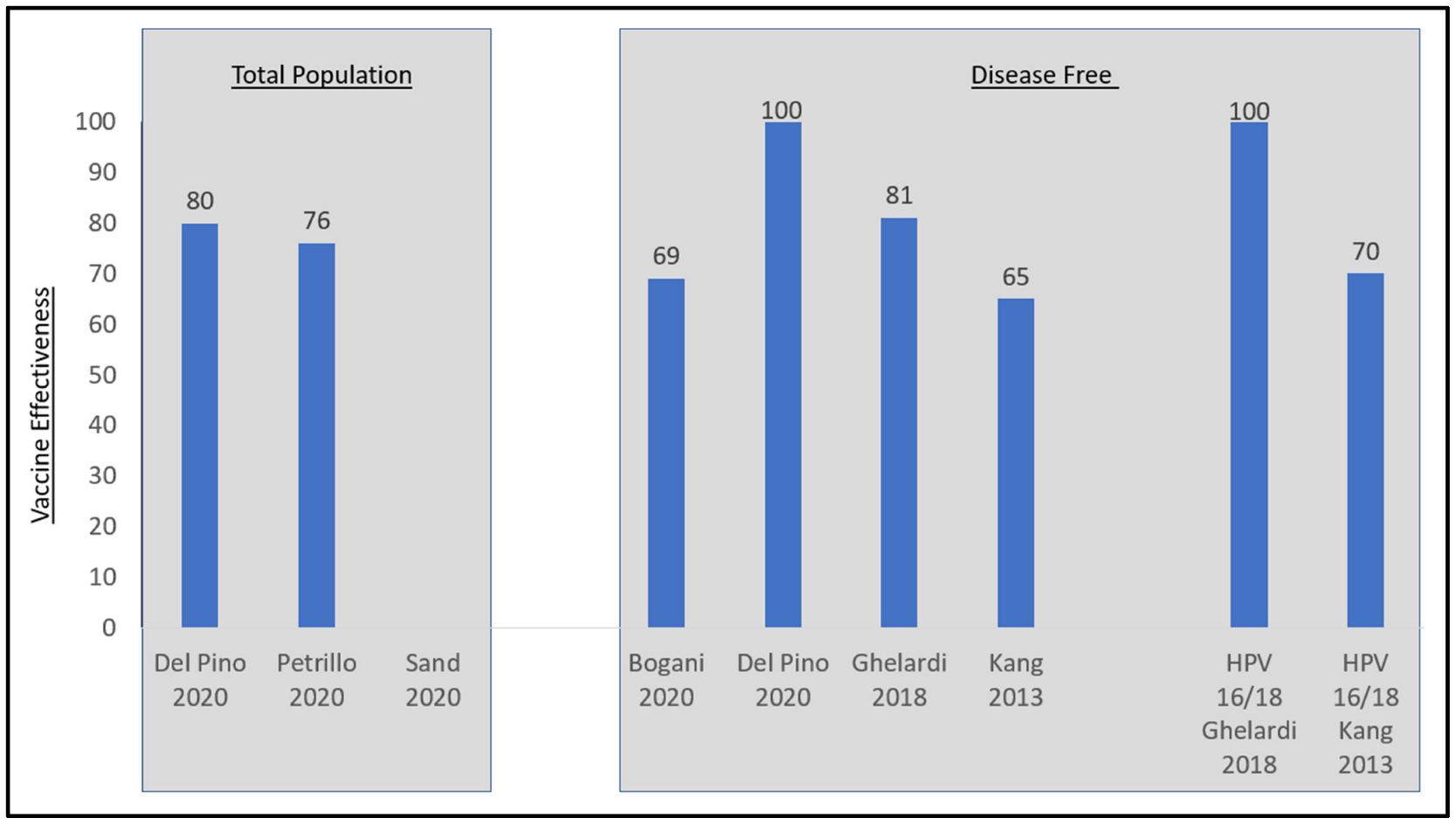
3.4. Women with Pre-Existing or Current Anogenital Disease
3.5. MSM
3.6. Immunocompromised or Immunosuppressed Individuals
3.7. Evidence Strength across the High-Risk Populations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Meites, E.; Gee, J.; Unger, E.; Markowitz, L. Human Papillomavirus. In Epidemiology and Prevention of Vaccine-Preventable Diseases; Centers for Disease Control and Prevention Public Health Foundation: Washington, DC, USA, 2021. [Google Scholar]
- de Sanjosé, S.; Serrano, B.; Tous, S.; Alejo, M.; Lloveras, B.; Quirós, B.; Clavero, O.; Vidal, A.; Ferrándiz-Pulido, C.; Pavón, M.Á.; et al. Burden of human papillomavirus (HPV)-related cancers attributable to HPVs 6/11/16/18/31/33/45/52 and 58. JNCI Cancer Spectr. 2018, 2, pky045. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Saura-Lázaro, A.; Montoliu, A.; Brotons, M.; Alemany, L.; Diallo, M.S.; Afsar, O.Z.; LaMontagne, D.S.; Mosina, L.; Contreras, M.; et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prev. Med. 2021, 144, 106399. [Google Scholar] [CrossRef] [PubMed]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M.; HPV Vaccination Impact Study Group. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef]
- Garland, S.M.; Kjaer, S.K.; Muñoz, N.; Block, S.L.; Brown, D.R.; DiNubile, M.J.; Lindsay, B.R.; Kuter, B.J.; Perez, G.; Dominiak-Felden, G.; et al. Impact and Effectiveness of the Quadrivalent Human Papillomavirus Vaccine: A Systematic Review of 10 Years of Real-world Experience. Clin. Infect. Dis. 2016, 63, 519–527. [Google Scholar] [CrossRef]
- Tyros, G.; Mastraftsi, S.; Gregoriou, S.; Nicolaidou, E. Incidence of anogenital warts: Epidemiological risk factors and real-life impact of human papillomavirus vaccination. Int. J. STD AIDS 2020, 32, 4–13. [Google Scholar] [CrossRef]
- Yakely, A.E.; Avni-Singer, L.; Oliveira, C.R.; Niccolai, L.M. Human Papillomavirus Vaccination and Anogenital Warts: A Systematic Review of Impact and Effectiveness in the United States. Sex. Transm. Dis. 2019, 46, 213–220. [Google Scholar] [CrossRef]
- Pham, C.T.; Juhasz, M.; Sung, C.T.; Mesinkovska, N.A. The human papillomavirus vaccine as a treatment for human papillomavirus–related dysplastic and neoplastic conditions: A literature review. J. Am. Acad. Dermatol. 2020, 82, 202–212. [Google Scholar] [CrossRef]
- Bartels, H.C.; Postle, J.; Rogers, A.C.; Brennan, D. Prophylactic human papillomavirus vaccination to prevent recurrence of cervical intraepithelial neoplasia: A meta-analysis. Int. J. Gynecol. Cancer 2020, 30, 777–782. [Google Scholar] [CrossRef]
- Brogden, D.R.L.; Walsh, U.; Pellino, G.; Kontovounisios, C.; Tekkis, P.; Mills, S.C. Evaluating the efficacy of treatment options for anal intraepithelial neoplasia: A systematic review. Int. J. Color. Dis. 2020, 36, 213–226. [Google Scholar] [CrossRef]
- Dion, G.R.; Teng, S.; Boyd, L.R.; Northam, A.; Mason-Apps, C.; Vieira, D.; Amin, M.R.; Branski, R.C. Adjuvant human papillomavirus vaccination for secondary prevention: A systematic review. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.R.; Le, T.; Lockhart, A.; Sanusi, A.; Dal Santo, L.; Davis, M.; McKinney, D.A.; Brown, M.; Poole, C.; Willame, C.; et al. Patterns of persistent HPV infection after treatment for cervical intraepithelial neoplasia (CIN): A systematic review. Int. J. Cancer 2017, 141, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Jentschke, M.; Kampers, J.; Becker, J.; Sibbertsen, P.; Hillemanns, P. Prophylactic HPV vaccination after conization: A systematic review and meta-analysis. Vaccine 2020, 38, 6402–6409. [Google Scholar] [CrossRef] [PubMed]
- Lichter, K.; Krause, D.; Xu, J.; Tsai, S.H.L.; Hage, C.; Weston, E.; Eke, A.; Levinson, K. Adjuvant Human Papillomavirus Vaccine to Reduce Recurrent Cervical Dysplasia in Unvaccinated Women: A Systematic Review and Meta-analysis. Obstet. Gynecol. Surv. 2020, 75, 475–476. [Google Scholar] [CrossRef]
- Martínez-Gómez, X.; Curran, A.; Campins, M.; Alemany, L.; Pendás, J.R.; Borruel, N.; Castellsagué, X.; de Heredia, C.D.; Moraga-Llop, F.A.; Del Pino, M.; et al. Multidisciplinary, evidence-based consensus guidelines for human papillomavirus (HPV) vaccination in high-risk populations, Spain, 2016. Eurosurveillance 2019, 24, 1700857. [Google Scholar] [CrossRef]
- Rosenberg, T.; Philipsen, B.B.; Mehlum, C.S.; Dyrvig, A.-K.; Wehberg, S.; Chirilǎ, M.; Godballe, C. Therapeutic Use of the Human Papillomavirus Vaccine on Recurrent Respiratory Papillomatosis: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2019, 219, 1016–1025. [Google Scholar] [CrossRef]
- Fortes, H.R.; von Ranke, F.M.; Escuissato, D.L.; Neto, C.A.A.; Zanetti, G.; Hochhegger, B.; Souza, C.A.; Marchiori, E. Recurrent respiratory papillomatosis: A state-of-the-art review. Respir. Med. 2017, 126, 116–121. [Google Scholar] [CrossRef]
- Riva, J.J.; Malik, K.M.P.; Burnie, S.J.; Endicott, A.R.; Busse, J.W. What is your research question? An introduction to the PICOT format for clinicians. J. Can. Chiropr. Assoc. 2012, 56, 167–171. [Google Scholar]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P.T. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 30 June 2021).
- GRADE Handbook. Quality of Evidence 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html#h.9rdbelsnu4iy (accessed on 10 November 2020).
- Ali, H.; McManus, H.; O’Connor, C.C.; Callander, D.; Kong, M.; Graham, S.; Saulo, D.; Fairley, C.K.; Regan, D.G.; Grulich, A.; et al. Human papillomavirus vaccination and genital warts in young Indigenous Australians: National sentinel surveillance data. Med. J. Aust. 2017, 206, 204–209. [Google Scholar] [CrossRef]
- Bogani, G.; Raspagliesi, F.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Simoncini, T.; Petrillo, M.; Plotti, F.; Lopez, S.; Casarin, J.; et al. Assessing the Long-Term Role of Vaccination against HPV after Loop Electrosurgical Excision Procedure (LEEP): A Propensity-Score Matched Comparison. Vaccines 2020, 8, 717. [Google Scholar] [CrossRef] [PubMed]
- Checchi, M.; Mesher, D.; Mohammed, H.; Soldan, K. Declines in anogenital warts diagnoses since the change in 2012 to use the quadrivalent HPV vaccine in England: Data to end 2017. Sex. Transm. Infect. 2019, 95, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Chirilă, M.; Bolboacă, S. Clinical efficiency of quadrivalent HPV (types 6/11/16/18) vaccine in patients with recurrent respiratory papillomatosis. Eur. Arch. Otorhinolaryngol. 2014, 271, 1135–1142. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Read, T.R.H.; Wigan, R.; Donovan, B.; Chen, M.Y.; Bradshaw, C.S.; Fairley, C.K. Ongoing decline in genital warts among young heterosexuals 7 years after the Australian human papillomavirus (HPV) vaccination programme. Sex. Transm. Infect. 2015, 91, 214–219. [Google Scholar] [CrossRef]
- Del Pino, M.; Martí, C.; Torras, I.; Henere, C.; Munmany, M.; Marimon, L.; Saco, A.; Torné, A.; Ordi, J. HPV vaccination as adjuvant to conization in women with cervical intraepithelial neoplasia: A study under real-life conditions. Vaccines 2020, 8, 245. [Google Scholar] [CrossRef] [PubMed]
- Donovan, B.; Franklin, N.; Guy, R.; Grulich, A.E.; Regan, D.G.; Ali, H.; Wand, H.; Fairley, C.K. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: Analysis of national sentinel surveillance data. Lancet Infect. Dis. 2011, 11, 39–44. [Google Scholar] [CrossRef]
- Ghelardi, A.; Marrai, R.; Bogani, G.; Sopracordevole, F.; Bay, P.; Tonetti, A.; Lombardi, S.; Bertacca, G.; Joura, E.A. Surgical Treatment of Vulvar HSIL: Adjuvant HPV Vaccine Reduces Recurrent Disease. Vaccines 2021, 9, 83. [Google Scholar] [CrossRef]
- Ghelardi, A.; Parazzini, F.; Martella, F.; Pieralli, A.; Bay, P.; Tonetti, A.; Svelato, A.; Bertacca, G.; Lombardi, S.; Joura, E.A. SPERANZA project: HPV vaccination after treatment for CIN2+. Gynecol. Oncol. 2018, 151, 229–234. [Google Scholar] [CrossRef]
- Goon, P.; Scholtz, L.U.; Sudhoff, H. Recurrent respiratory papillomatosis (RRP)—Time for a reckoning? Laryngoscope Investig. Otolaryngol. 2017, 2, 184–186. [Google Scholar] [CrossRef]
- Hermann, J.S.; Weckx, L.; Nürmberger, J.M.; Junior, G.F.D.S.; Pignatari, A.C.C.; Pignatari, S.S.N. Effectiveness of the human papillomavirus (types 6, 11, 16, and 18) vaccine in the treatment of children with recurrent respiratory papillomatosis. Int. J. Pediatr. Otorhinolaryngol. 2016, 83, 94–98. [Google Scholar] [CrossRef]
- Hočevar-Boltežar, I.; Matičič, M.; Šereg-Bahar, M.; Gale, N.; Poljak, M.; Kocjan, B.; Žargi, M. Human papilloma virus vaccination in patients with an aggressive course of recurrent respiratory papillomatosis. Eur. Arch. Otorhinolaryngol. 2014, 271, 3255–3262. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.D.; Choi, H.S.; Kim, S.M. Is vaccination with quadrivalent HPV vaccine after loop electrosurgical excision procedure effective in preventing recurrence in patients with high-grade cervical intraepithelial neoplasia (CIN2-3)? Gynecol. Oncol. 2013, 130, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Lukac, C.D.; Donken, R.; Otterstatter, M.; Mazo, O.; Wong, S.; Marra, F.; Smith, L.; Naus, M.; Money, D.; Krajden, M.; et al. Impacts of human papillomavirus immunization programs on rates of anogenital warts in British Columbia, Canada, 2000 to 2017. Sex. Transm. Dis. 2020, 47, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, H.; Makiyama, K.; Hirai, R.; Suzuki, H.; Asai, R.; Oshima, T. Multi-Year Effect of Human Papillomavirus Vaccination on Recurrent Respiratory Papillomatosis. Laryngoscope 2020, 130, 442–447. [Google Scholar] [CrossRef]
- Mauz, P.S.; Schäfer, F.A.; Iftner, T.; Gonser, P. HPV vaccination as preventive approach for recurrent respiratory papillomatosis—A 22-year retrospective clinical analysis. BMC Infect. Dis. 2018, 18, 343. [Google Scholar] [CrossRef]
- Milner, T.; Harrison, A.; Montgomery, J.; MacGregor, F.; Buchanan, M.; MacKenzie, K. A retrospective case-control analysis of the efficacy of Gardasil® vaccination in 28 patients with recurrent respiratory papillomatosis of the larynx. Clin. Otolaryngol. 2018, 43, 962–965. [Google Scholar] [CrossRef]
- Moscicki, A.-B.; Karalius, B.; Tassiopoulos, K.; Yao, T.-J.; Jacobson, D.L.; Patel, K.; Purswani, M.; Seage, G.R.; Yogev, R.; Sanders, M.A.; et al. Human Papillomavirus Antibody Levels and Quadrivalent Vaccine Clinical Effectiveness in Perinatally Human Immunodeficiency Virus–infected and Exposed, Uninfected Youth. Clin. Infect. Dis. 2019, 69, 1183–1191. [Google Scholar] [CrossRef]
- Papaioannou, V.-A.; Lux, A.; Voigt-Zimmermann, S.; Arens, C. Treatment outcomes of recurrent respiratory papillomatosis. HNO 2018, 66, 7–15. [Google Scholar] [CrossRef]
- Petráš, M.; Adámková, V. Impact of quadrivalent human papillomavirus vaccine in women at increased risk of genital warts burden: Population-based cross-sectional survey of Czech women aged 16 to 40 years. Vaccine 2015, 33, 6264–6267. [Google Scholar] [CrossRef]
- Petrillo, M.; Dessole, M.; Tinacci, E.; Saderi, L.; Muresu, N.; Capobianco, G.; Cossu, A.; Dessole, S.; Sotgiu, G.; Piana, A. Efficacy of HPV Vaccination in Women Receiving LEEP for Cervical Dysplasia: A Single Institution’s Experience. Vaccines 2020, 8, 45. [Google Scholar] [CrossRef]
- Sand, F.L.; Kjaer, S.K.; Frederiksen, K.; Dehlendorff, C. Risk of cervical intraepithelial neoplasia grade 2 or worse after conization in relation to HPV vaccination status. Int. J. Cancer 2020, 147, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, M.J.; Leyden, W.A.; Lam, J.O.; Chao, C.R.; Gregorich, S.E.; Huchko, M.J.; Kulasingam, S.; Kuppermann, M.; Smith-McCune, K.K.; Sawaya, G.F. Effectiveness of ‘catch-up’ human papillomavirus vaccination to prevent cervical neoplasia in immunosuppressed and non-immunosuppressed women. Vaccine 2020, 38, 4520–4523. [Google Scholar] [CrossRef] [PubMed]
- Swedish, K.A.; Factor, S.H.; Goldstone, S.E. Prevention of Recurrent High-Grade Anal Neoplasia with Quadrivalent Human Papillomavirus Vaccination of Men Who Have Sex with Men: A Nonconcurrent Cohort Study. Clin. Infect. Dis. 2012, 54, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Swedish, K.A.; Goldstone, S.E. Prevention of Anal Condyloma with Quadrivalent Human Papillomavirus Vaccination of Older Men Who Have Sex with Men. PLoS ONE 2014, 9, e93393. [Google Scholar] [CrossRef]
- Thompson, A.B.; Gillespie, S.E.; Mosunjac, M.B.; Hussen, S.A.; Flowers, L.C.; Camacho-Gonzalez, A.F. Prevalence of Anal Squamous Intraepithelial Lesions in HIV-1–Infected Young Men Who Have Sex with Men and Transwomen. J. Low. Genit. Tract Dis. 2018, 22, 340–347. [Google Scholar] [CrossRef]
- Tjon Pian Gi, R.E.; San Giorgi, M.R.; Pawlita, M.; Michel, A.; van Hemel, B.M.; Schuuring, E.; van den Heuvel, E.R.; van der Laan, B.F.; Dikkers, F.G. Immunological response to quadrivalent HPV vaccine in treatment of recurrent respiratory papillomatosis. Eur. Arch. Otorhinolaryngol. 2016, 273, 3231–3236. [Google Scholar] [CrossRef]
- Yiu, Y.; Fayson, S.; Smith, H.; Matrka, L. Implementation of Routine HPV Vaccination in the Management of Recurrent Respiratory Papillomatosis. Ann. Otol. Rhinol. Laryngol. 2019, 128, 309–315. [Google Scholar] [CrossRef]
- Young, D.L.; Moore, M.M.; Halstead, L.A. The Use of the Quadrivalent Human Papillomavirus Vaccine (Gardasil) as Adjuvant Therapy in the Treatment of Recurrent Respiratory Papilloma. J. Voice 2015, 29, 223–229. [Google Scholar] [CrossRef]
- San Giorgi, M.R.M.; van den Heuvel, E.R.; Tjon Pian Gi, R.E.A.; Brunings, J.W.; Chirila, M.; Friedrich, G.; Golusinski, W.; Graupp, M.; Horcasitas Pous, R.A.; Ilmarinen, T.; et al. Age of onset of recurrent respiratory papillomatosis: A distribution analysis. Clin. Otolaryngol. 2016, 41, 448–453. [Google Scholar] [CrossRef]
- BC Centre for Disease Control. History of Immunization in BC. In Communicable Disease Control Manual: Provincial Health Services Authority 2020; BC Centre for Disease Control: Vancouver, BC, Canada, 2020. [Google Scholar]
- Luna, J.; Plata, M.; Gonzalez, M.; Correa, A.; Maldonado, I.; Nossa, C.; Radley, D.; Vuocolo, S.; Haupt, R.M.; Saah, A. Long-Term Follow-up Observation of the Safety, Immunogenicity, and Effectiveness of Gardasil™ in Adult Women. PLoS ONE 2013, 8, e83431. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Nygård, M.; Sundström, K.; Munk, C.; Berger, S.; Dzabic, M.; Fridrich, K.E.; Waldstrøm, M.; Sørbye, S.W.; Bautista, O.; et al. Long-term effectiveness of the nine-valent human papillomavirus vaccine in Scandinavian women: Interim analysis after 8 years of follow-up. Hum. Vaccines Immunother. 2021, 17, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.R.; Joura, E.A.; Garland, S.M.; Huh, W.K.; Iversen, O.-E.; Kjaer, S.K.; Ferenczy, A.; Kurman, R.J.; Ronnett, B.M.; Stoler, M.H.; et al. Nine-valent HPV vaccine efficacy against related diseases and definitive therapy: Comparison with historic placebo population. Gynecol. Oncol. 2019, 154, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef]
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Ibrahim Khalil, A.; Baussano, I.; Shah, A.S.V.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob. Health 2021, 9, e161–e169. [Google Scholar] [CrossRef]
- Wang, W.; Kothari, S.; Baay, M.; Garland, S.M.; Giuliano, A.R.; Nygård, M.; Velicer, C.; Tota, J.; Sinha, A.; Skufca, J.; et al. Real-world impact and effectiveness assessment of the quadrivalent HPV vaccine: A systematic review of study designs and data sources. Expert Rev. Vaccines 2021, 21, 227–240. [Google Scholar] [CrossRef]
- Weyers, S.; Garland, S.; Cruickshank, M.; Kyrgiou, M.; Arbyn, M. Cervical cancer prevention in transgender men: A review. BJOG: Int. J. Obstet. Gynaecol. 2021, 128, 822–826. [Google Scholar] [CrossRef]
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Damgacioglu, H.; Lin, Y.-Y.; Stier, E.A.; Nyitray, A.G.; Chiao, E.Y.; Nemutlu, G.S.; Chhatwal, J.; et al. Incidence Trends and Burden of Human Papillomavirus-Associated Cancers Among Women in the United States, 2001–2017. JNCI J. Natl. Cancer Inst. 2021, 113, 792–796. [Google Scholar] [CrossRef]
- Arbyn, M.; Xu, L.; Simoens, C.; Martin-Hirsch, P.P. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst Rev. 2018, 5, CD009069. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Populations |
People of any age, from any country, considered at high risk for HPV-related disease, including:∙
| People not in one of the identified high-risk populations |
| Interventions | HPV vaccination | Use of 2vHPV in >50% of vaccinated subjects |
| Comparisons | No vaccine (effectiveness)
Before vaccination programs implemented (impact) | |
| Outcomes | Incidence or prevalence of genital warts or HPV-related precancer or cancer, including:∙
| Patient-reported outcomes (e.g., quality of life, satisfaction) Economic outcomes (e.g., cost-effectiveness, budget impact) Population level incidence/prevalence of Juvenile onset RRP (JoRRP vaccine impact studies) |
| Time | Conference abstracts: 1 January 2018 to present Articles: any time | Conference abstracts published before 2018 |
| Study design | Observational studies using real-world data (e.g., longitudinal survey, medical records, registry) Systematic reviews (for identification of primary studies only) | Randomized trials, including long-term follow-up studies of clinical trial cohorts Decision Analytic and cost-effectiveness modeling/simulation studies Non-systematic reviews Editorials, comments, notes Case studies Clinical practice guidelines |
| Other | English language | Non-English language |
| Author Year | Country | Patient Description | Demonstrated Effect a |
|---|---|---|---|
| Cervical Disease | |||
| Bogani 2020 [24] | Italy | Women undergoing conization for cervical HSIL, 60 months minimum follow-up | 69% in those HPV-free at 6 months to adjust for residual disease. NS in total population. |
| Del Pino 2020 [28] | Spain | Women undergoing conization between January 2013 and July 2018. Mean 22.4 months follow-up | 80% in total population. For those disease-free at 6 months (negative HPV test, negative Pap test, and, if available, a negative biopsy), 100% for HSIL. |
| Ghelardi 2018 [31] | Italy | Women undergoing conization for cervical HSIL/CIN2-3, 36 month median follow-up | 81.2% in analyses adjusting for residual disease. NS without adjustment for residual disease. |
| Kang 2013 [35] | South Korea | Women aged 20–45 years undergoing LEEP for histologically confirmed CIN2-3, 42 month median follow-up, 2 year minimum | 65% in those disease-free at 3 months, b 70% among those with vaccine type lesions before LEEP who were disease-free at 3 months. |
| Petrillo 2020 [43] | Italy | Women undergoing LEEP for CIN1 or greater | 76% for CIN2+. |
| Sand 2020 [44] | Denmark | Women undergoing conization for CIN3 or greater | NS |
| Vulvar Precancer | |||
| Ghelardi 2021 [30] | Italy | Women undergoing surgical treatment for vulvar HSIL | NS overall: 78.5% for disease from incident/reactivated infection. |
| Genital Warts | |||
| Petráš 2015 [42] | Czech Republic | Women aged 16–40 years with prior history of genital warts c | For 4vHPV: 89.0% for certain cases, 74.0% for possible and certain cases. |
| Author Year | Country | Patient Description | Demonstrated Effect a |
|---|---|---|---|
| Effectiveness Studies | |||
| Swedish 2012 [46] | United States | HIV(−) MSM with prior biopsied and treated HGAIN | 58% for recurrent HGAIN at 1 year and 50% at 2 years. Among patients HPV DNA(+) for high-risk genotypes, 60% at 1 year and 53% at 2 years. NS at 3 years for all comparisons. |
| Swedish 2014 [47] | United States | HIV(−) MSM ≥26 y with no anal condyloma history or previously treated, recurrence-free condyloma | 55% in total population. NS for recurrent AGW among patients with history of AGW within the past 5 years. |
| Thompson 2018 [48] | United States | HIV(+) MSM (98%) and transwomen (2%) b | NS against anal precancers among 85% of the population with anal cytology data. |
| Impact Studies of 4vHPV against Anogenital Warts | |||
| Ali 2017 [23] | Australia | Indigenous and non-indigenous MSM attending 39 sexual health clinics c | 36% decline in rate for non-Indigenous. NS for Indigenous between 2004 and 2007 and between 2008 and 2014. |
| Chow 2015 [27] | Australia | MSM aged 16–40 years attending 1 sexual health clinic d | 33% decline overall between 2004 and 2005 and between 2013 and 2014. Variation by age, sexual orientation, and wart location was noted. |
| Donovan 2011 [29] | Australia | MSM attending 8 sexual health clinics d | 28% decline between January and June 2004 and between January and June 2007. |
| Checchi 2019 [25] | United Kingdom | MSM aged 15–24 years attending sexual health clinics participating in national surveillance system d | 79% decline for 15 year olds between 2014 and 2017. NS for other age groups (15–17, 18–20, and 21–24). |
| Lukac 2020 [36] | Canada | MSM aged 14–46 years attending 16 sexual health clinics d | 41% decline between 1991 and 1993 and between 1994 and 1996. NS for earlier birth cohort comparisons. |
| Design and Population | Strength of Evidence b | Study Limitations c | Directness d | Consistency e | Precision f | Publication Bias g |
|---|---|---|---|---|---|---|
| VACCINE EFFECTIVENESS STUDIES | ||||||
| RRP patients h | High | Medium | Direct | Consistent | Imprecise | Low |
| Women with pre-existing anogenital disease | ||||||
| Cervical disease | High | Medium | Direct | Consistent | Precise | Low |
| Vulvar precancer | Medium | Low | Direct | NA i | NA i | Low |
| Genital warts j | Medium | Medium | Direct | NA i | NA i | Low |
| MSM | ||||||
| HIV(–) k | Medium | Medium | Indirect | NA i | NA i | Low |
| HIV(+) l | Low | High | Direct | NA i | NA i | Low |
| Immunosuppressed/ Immunocompromised individuals m | Low | High | Indirect | NA i | NA i | Low |
| VACCINE IMPACT STUDIES | ||||||
| MSM n | Low | High | Direct | Consistent | Precise | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodman, E.; Reuschenbach, M.; Kaminski, A.; Ronnebaum, S. Human Papillomavirus Vaccine Impact and Effectiveness in Six High-Risk Populations: A Systematic Literature Review. Vaccines 2022, 10, 1543. https://doi.org/10.3390/vaccines10091543
Goodman E, Reuschenbach M, Kaminski A, Ronnebaum S. Human Papillomavirus Vaccine Impact and Effectiveness in Six High-Risk Populations: A Systematic Literature Review. Vaccines. 2022; 10(9):1543. https://doi.org/10.3390/vaccines10091543
Chicago/Turabian StyleGoodman, Elizabeth, Miriam Reuschenbach, Allysen Kaminski, and Sarah Ronnebaum. 2022. "Human Papillomavirus Vaccine Impact and Effectiveness in Six High-Risk Populations: A Systematic Literature Review" Vaccines 10, no. 9: 1543. https://doi.org/10.3390/vaccines10091543
APA StyleGoodman, E., Reuschenbach, M., Kaminski, A., & Ronnebaum, S. (2022). Human Papillomavirus Vaccine Impact and Effectiveness in Six High-Risk Populations: A Systematic Literature Review. Vaccines, 10(9), 1543. https://doi.org/10.3390/vaccines10091543