

Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design and Settings
2.2. Study Area Demographics
2.3. Study Sample Size
2.4. Study Survey Procedure and Instrument
2.5. Ethical Considerations
2.6. Statistical Analysis
3. Results
3.1. Demographic Profile of Respondents
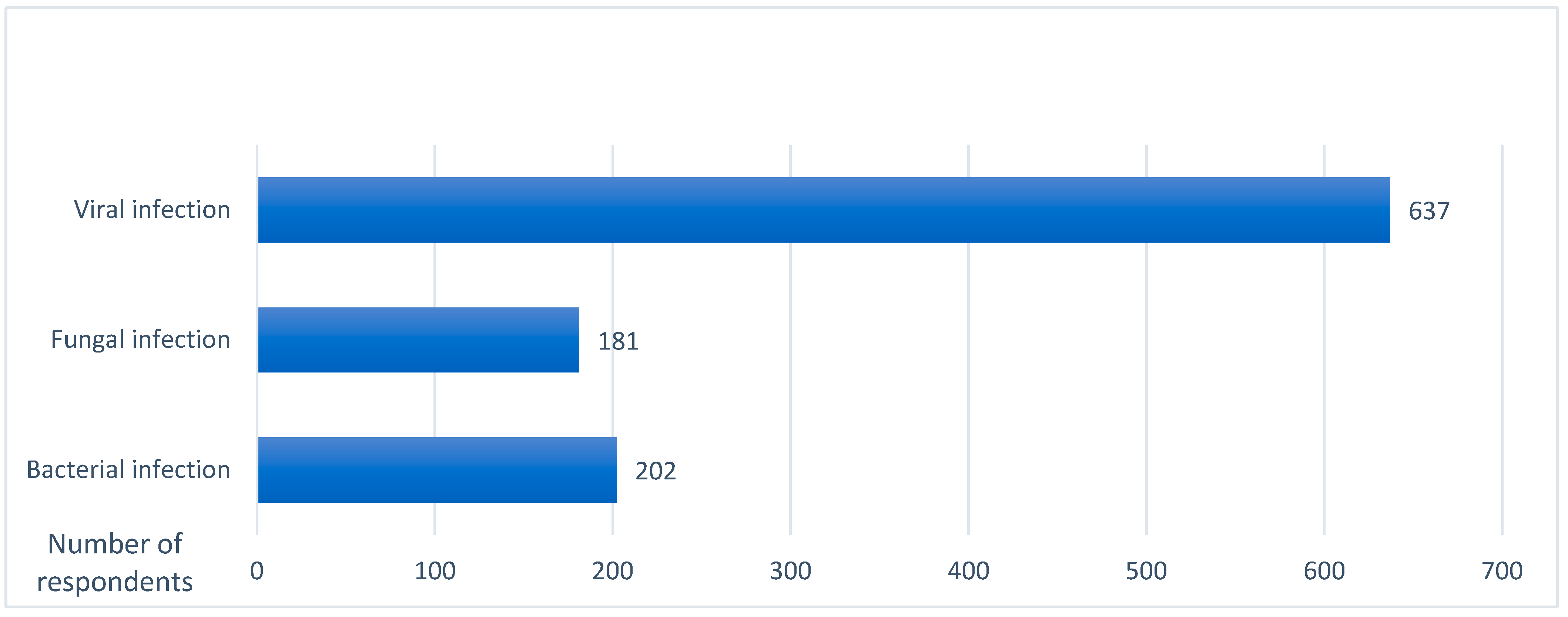
3.2. The Respondents’ Awareness of Monkeypox
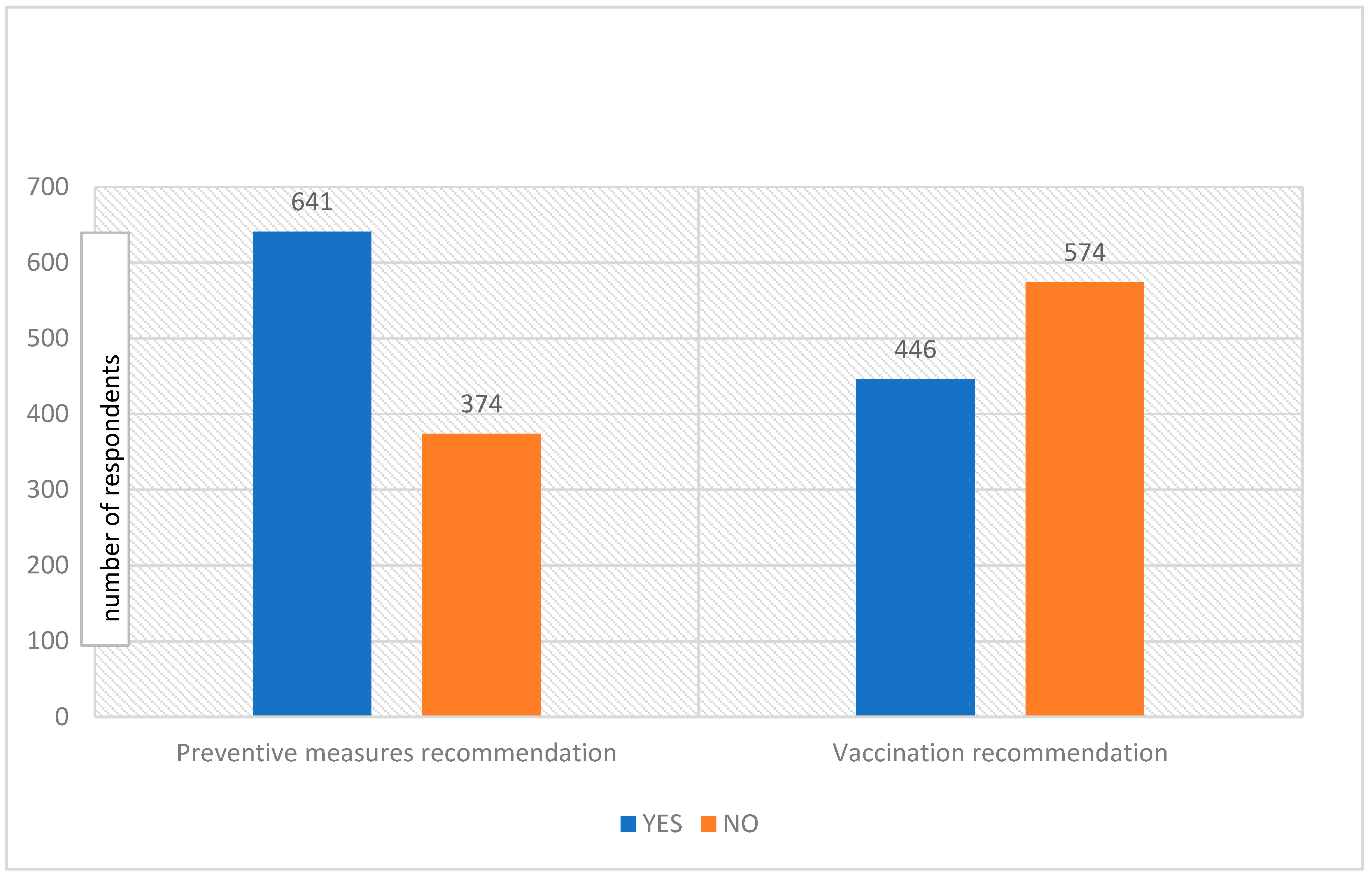
3.3. Preventive and Recommendation Measures
3.4. Perceptions of a Vaccination Campaign against Monkeypox
3.5. Preventive Measures and Recommendations for Monkeypox Vaccination
4. Discussion
4.1. Study Strengths and Limitations
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Monkeypox Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 2 July 2022).
- Centres for Disease Control and Prevention (CDC). About Monkeypox. Available online: https://www.cdc.gov/poxvirus/monkeypox/about.html (accessed on 2 July 2022).
- Moss, B. Poxviridae: The viruses and their replication. In Field’s Virology, 4th ed.; Knipe, D.M., Howley, P.M., Eds.; Lippincott-Raven: Philadelphia, PA, USA, 2001; pp. 2849–2883. [Google Scholar]
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Kugelman, J.R.; Johnston, S.C.; Mulembakani, P.M.; Kisalu, N.; Lee, M.S.; Koroleva, G.; McCarthy, S.E.; Gestole, M.C.; Wolfe, N.D.; Fair, J.N.; et al. Genomic variability of monkeypox virus among humans, Democratic Republic of the Congo. Emerg. Infect. Dis. 2014, 20, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.D.; Melski, J.W.; Graham, M.B.; Regnery, R.L.; Sotir, M.J.; Wegner, M.V. The detection of monkeypox in humans in the Western Hemisphere. N. Engl. J. Med. 2004, 350, 342–350. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON393 (accessed on 23 August 2022).
- Heskin, J.; Belfield, A.; Milne, C.; Brown, N.; Walters, Y.; Scott, C.; Bracchi, M.; Moore, L.S.; Mughal, N.; Rampling, T.; et al. Transmission of monkeypox virus through sexual contact—A novel route of infection. J. Infect. 2022, 85, 334–363. [Google Scholar] [CrossRef] [PubMed]
- Parvin, R.; Ali, A.; Nagy, A.; Zhu, Z.; Zhao, S.; Neuhaus, J.; Paul, A.K.; Hafez, M.; Awad, A.S. Monkeypox virus: A comprehensive review of taxonomy, evolution, epidemiology, diagnosis, prevention, and control regiments so far. Ger. J. Microbiol. 2022, 2, 1–15. [Google Scholar] [CrossRef]
- Magnus, P.V.; Andersen, E.K.; Petersen, K.B.A. Pox-like disease in Cynomolgus Monkeys. Acta Pathol. Microbiol. Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Breman, J.G.; Ruti, K.; Steniowski, M.V. Human monkeypox, 1970–1979. Bull. World Health Organ. 1980, 58, 165–182. [Google Scholar] [PubMed]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by the monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar] [PubMed]
- Centres for Disease Control and Prevention (CDC). Monkeypox- Past U.S. Cases and Outbreaks. Available online: https://www.cdc.gov/poxvirus/monkeypox/outbreak/us-outbreaks.html (accessed on 20 July 2022).
- Centers for Disease Control and Prevention (CDC). 2022 Monkeypox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 24 August 2022).
- United Nations News: Monkeypox was Declared a Global Health Emergency by the World Health Organization. Available online: https://news.un.org/en/story/2022/07/1123152 (accessed on 23 July 2022).
- Meo, S.A.; Jawaid, S.A. Human Monkeypox: Fifty-Two Years based analysis and Updates. Pak. J. Med. Sci. 2022, 38, 1416–1419. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.; Nuara, A.; Buller, R.M.L.; Schultz, D.A. Human monkeypox: An emerging zoonotic disease. Future Microbiol. 2007, 2, 17–34. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.R.; Dolin, R. Vaccinia viruses: Vaccines against smallpox and vectors against infectious diseases and tumors. Expert Rev. Vaccines 2011, 10, 1221–1240. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Pathog. Glob. Health 2020, 114, 68–75. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Archived: WHO Timeline—COVID-19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 23 July 2022).
- Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Value | Frequency | Percentage |
|---|---|---|---|
| Age | 15–20 years | 388 | 38.0 |
| 21–30 years | 558 | 54.7 | |
| 31–40 years | 58 | 5.7 | |
| 41–50 years | 15 | 1.5 | |
| 70 years and above | 1 | 0.1 | |
| Gender | Female | 554 | 54.3 |
| Male | 466 | 45.7 | |
| Educational level | Bachelor’s degree | 608 | 59.6 |
| Elementary | 1 | 0.1 | |
| Master’s degree | 38 | 3.7 | |
| Middle/High school | 341 | 33.4 | |
| Other (Diploma) | 25 | 2.5 | |
| Ph.D./Fellowship | 6 | 0.6 | |
| Region | Central region | 483 | 47.4 |
| Eastern region | 117 | 11.5 | |
| Northern region | 65 | 6.4 | |
| Southern region | 3 | 0.3 | |
| Western region | 352 | 34.5 | |
| Occupation | Governmental job (ex. teachers) | 47 | 4.6 |
| Health practitioner | 33 | 3.2 | |
| Military(police) | 12 | 1.2 | |
| Private sector | 79 | 7.7 | |
| Student | 644 | 63.1 | |
| Unemployed | 205 | 20.1 | |
| Marital status | Divorced | 18 | 1.8 |
| Married | 69 | 6.8 | |
| Single | 932 | 91.4 | |
| Widowed | 1 | 0.1 | |
| Socioeconomic status (monthly) | <3000 SAR | 596 | 58.4 |
| 10,000 or more SAR | 1 | 0.1 | |
| 3000–6000 SAR | 78 | 7.6 | |
| 6000–less than 9000 SAR | 46 | 4.5 | |
| 9000 or more SAR | 81 | 7.9 |
| Statements | Yes (n and (%)) | No (n and (%)) |
|---|---|---|
| Do you believe that monkeypox disease has become a pandemic? | 799 (78.3) | 221 (21.7) |
| Do you know that monkeypox is common in Western and Central Africa? | 798 (78.2) | 222 (21.8) |
| Do you know that monkeypox cases are increasing worldwide? | 692 (67.8) | 328 (32.2) |
| Are monkeypox cases present in Saudi Arabia? | 914 (89.6) | 106 (10.4) |
| Do you know monkeypox is commonly transmitted through direct contact? | 798 (78.2) | 222 (21.8) |
| Do you know monkeypox is easily transmitted from human to human? | 545 (53.4) | 475 (46.6) |
| Do you know that travelling to other countries is the main cause of spreading monkeypox disease? | 693 (67.9) | 327 (32.1) |
| Do you know that monkeypox and smallpox have similar signs and symptoms? | 807 (79.1) | 213 (20.9) |
| Do you know the clinical symptoms of monkeypox disease? | 491 (48.1) | 529 (51.9) |
| Do you know that a skin manifestation (skin rash) is the main symptom of monkeypox disease? | 889 (87.2) | 131 (12.8) |
| Do you know that lymphadenopathy (swollen lymph nodes) is one clinical feature that could be used to differentiate between monkeypox and smallpox? | 585 (57.4) | 435 (42.6) |
| Do you know that the smallpox vaccination protects against the human monkeypox virus? | 728 (71.4) | 292 (28.6) |
| Do you know the complications of monkeypox disease? | 278 (27.3) | 742 (72.7) |
| Frequency | Percentage | |
|---|---|---|
| Bacterial infection | 202 | 19.8 |
| Fungal infection | 181 | 17.7 |
| Viral infection | 637 | 62.5 |
| Questions | Yes (n and (%)) | No (n and (%)) |
|---|---|---|
| Are you afraid of catching monkeypox disease? | 412 (40.4) | 608 (59.6) |
| Are you afraid to visit any family members or friends due to monkeypox disease? | 141 (13.8) | 879 (86.2) |
| Are you afraid to travel to any country due to monkeypox disease? | 399 (39.1) | 621 (60.9) |
| Are you taking more hygienic preventive measures due to monkeypox disease? | 228 (22.4) | 792 (77.6) |
| Recommendations | ||
| Do you recommend that health officials start a vaccination campaign against monkeypox disease? | 446 (43.7) | 574 (56.3) |
| Do you recommend that health officials should take public preventive measures? | 641 (62.8) | 374 (37.2) |
| Variables | Do You Recommend Health Officials to Start a Vaccination Campaign against Monkeypox? | ||
|---|---|---|---|
| Yes (n and (%)) | No (n and (%)) | p-Value | |
| Age | 0.110 | ||
| 15–20 years | 185 (47.7) | 203 (52.3) | |
| 21–30 years | 235 (42.1) | 323 (57.9) | |
| 31–40 years | 20 (34.5) | 38 (55.5) | |
| 41–50 years | 5 (33.3) | 10 (66.7) | |
| 70 years and above | 1 (100.0) | 0 (0.0) | |
| Gender | 0.216 | ||
| Male | 194 (41.6) | 272 (58.4) | |
| Female | 252 (45.5) | 302 (54.5) | |
| Education level | 0.033 | ||
| Bachelor’s | 246 (40.5) | 362 (59.5) | |
| Elementary | 0 (0.0) | 1 (100.0) | |
| Master’s | 16 (42.1) | 22 (57.9) | |
| Middle/High school | 168 (49.3) | 173 (50.7) | |
| Other (Diploma) | 11 (44.0) | 14 (56.0) | |
| Ph.D./Fellowship | 5 (83.3) | 1 (16.7) | |
| Occupation | 0.560 | ||
| Governmental job (ex. teachers) | 21 (44.7) | 26 (55.3) | |
| Health practitioner | 11 (33.3) | 22 (66.7) | |
| Military(police) | 3 (25.0) | 9 (75.0) | |
| Private sector | 32 (40.5) | 47 (59.5) | |
| Student | 290 (45.0) | 354 (55.0) | |
| Unemployed | 89 (43.4) | 116 (56.6) | |
| Socioeconomic status | 0.672 | ||
| <3000 SAR | 262 (44.0) | 334 (56.0) | |
| 10,000 or more SAR | 1 (100) | 0 (0.0) | |
| 3000–6000 SAR | 39 (50.0) | 39 (50.0) | |
| 6000–less than 9000 SAR | 18 (39.1) | 28 (60.9) | |
| 9000 or more SAR | 33 (40.7) | 48 (59.3) | |
| Variables | Do You Recommend that Health Officials Start the Vaccination Campaign against Monkeypox Disease? | ||
|---|---|---|---|
| No (n (%)) | Yes (n (%)) | p-Value | |
| Are you afraid of monkeypox disease? | |||
| No | 423 (69.6) | 185 (30.4) | 0.000 |
| Yes | 151 (36.7) | 261 (63.3) | |
| Are you taking more hygienic preventive measures due to monkeypox disease? | 0.000 | ||
| No | 503 (63.5) | 289 (36.5) | |
| Yes | 71 (31.3) | 157 (68.9) | |
| Are you afraid to visit any family members or friends due to monkeypox disease? | 0.000 | ||
| No | 542 (61.7) | 337 (38.3) | |
| Yes | 32 (22.7) | 109 (77.3) | |
| Are you afraid to travel to any country due to monkeypox disease? | 0.000 | ||
| No | 405 (65.2) | 216 (34.8) | |
| Yes | 169 (42.4) | 230 (57.6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meo, S.A.; Al-Khlaiwi, T.; Aljofan, Z.F.; Alanazi, A.I.; Meo, A.S. Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 1534. https://doi.org/10.3390/vaccines10091534
Meo SA, Al-Khlaiwi T, Aljofan ZF, Alanazi AI, Meo AS. Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study. Vaccines. 2022; 10(9):1534. https://doi.org/10.3390/vaccines10091534
Chicago/Turabian StyleMeo, Sultan Ayoub, Thamir Al-Khlaiwi, Ziyad Fahad Aljofan, Aued Iaed Alanazi, and Anusha Sultan Meo. 2022. "Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study" Vaccines 10, no. 9: 1534. https://doi.org/10.3390/vaccines10091534
APA StyleMeo, S. A., Al-Khlaiwi, T., Aljofan, Z. F., Alanazi, A. I., & Meo, A. S. (2022). Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study. Vaccines, 10(9), 1534. https://doi.org/10.3390/vaccines10091534