
Factors Associated with the COVID-19 Vaccination Status of Higher Education Students: Results of an Online Cross-Sectional Survey at Six Universities in Southwestern Germany

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Vaccine Hesitancy
1.2. Higher Education Students
1.3. Research Questions
- (1)
- How do students in higher education evaluate behavioral and structural measures to prevent SARS-CoV-2 infections in the study environment?
- (2)
- Which factors are associated with the COVID-19 vaccination status of higher education students when they had all been offered vaccination?
2. Materials and Methods
2.1. Study Setting
2.2. Study Population
2.3. Recruitment and Data Collection
2.4. Development of the Standardized Online Student Survey
2.5. Elements of the Standardized Online Student Survey
- Individual variables (socio-demographic and study-related characteristics)
- a.
- Age (numerical variable); categorical variables: gender, affiliation to risk group for developing severe COVID-19 courses [44], SARS-CoV-2 infection, COVID-19 vaccination status, German or other nationality, part-time job while studying, living in a committed relationship, number of household members, presence of health professional within household
- b.
- Big Five personality trait (BFI-10 [51]—five subscales consisting of two items with the range 1–5—low to high each)
- c.
- d.
- Affiliation to and type of HEI (study-related categorical variables: five dummy-coded variables and application-oriented/research-oriented)
- e.
- Faculty/program of study (study-related categorical variable: healthcare university curriculum/non-healthcare university curriculum)
- Perception of SARS-CoV-2 in general [54]
- a.
- Disease perception (scale consisting of two items with the range 1–7—low to high disease perception)
- b.
- Affective risk perception (scale consisting of three items (e.g., worry or thinking about the coronavirus all the time [55]) with the range 1–7—low to high affective risk perception)
- c.
- Perceived adequacy of media coverage (7-point Likert scale with the range from ‘too little media attention’ to ‘media-hype’)
- d.
- Perceived personal susceptibility (7-point Likert scale with the range from ‘not susceptible at all’ to ‘very susceptible’)
- e.
- Expected severity of COVID-19 disease for one’s own (7-point Likert scale with the range from ‘totally harmless’ to ‘extremely dangerous’)
- Attitude toward health and safety measures to prevent SARS-CoV-2 infections in the study environment
- a.
- Attitude toward behavioral preventive measures in the study environment (score consisting of eight items measured on a 5-point Likert scale ranging from 1 ‘not at all suitable’ to 5 ‘very suitable’)
- b.
- Attitude toward structural preventive measures in the study environment (scale consisting of nine items measured on a 5-point Likert scale ranging from 1 ‘not at all suitable’ to 5 ‘very suitable’)
- Impact of COVID-19 on the personal environment
- a.
- Perceived probability to contract COVID-19 in private surroundings (7-point Likert scale with range low to high)
- b.
- Perceived probability to contract COVID-19 in current campus surrounding (7-point Likert scale with range low to high)
- c.
- Readiness to perform SARS-CoV-2 rapid antigen tests (7-point Likert scale with range ‘in no case’ to ‘in any case’)
- d.
- Confirmed SARS-CoV-2 infection (categorical variable: no confirmed infection/confirmed infection)
- e.
- COVID-19 specific reactance (score consisting of four items with range 1–7 low to high reactance) [54]
- f.
- COVID-19 specific resilience (score consisting of four items with range 1–7 low to high resilience) [54]
- g.
- Trust in fellow students to adhere to distance and hygiene rules (7-point Likert scale, each with a range from low to high adherence)
- Variables relating to COVID-19 vaccination
- a.
- Attitude toward COVID-19 vaccination (own health, avoidance of personal disadvantages of the pandemic [54], avoidance of disadvantages of the pandemic for HEIs on 7-point Likert scale with the range ‘do not agree at all’ to ‘fully agree’)
- b.
- COVID-19 vaccination status (categorical variable: not yet vaccinated/vaccinated at least once against COVID-19)
- c.
- 5C psychological antecedents of vaccination (confidence, complacency, constraints, calculation and collective responsibility) [56] in relation to COVID-19 vaccination (five items measured on 7-point Likert scale with range ‘do not agree at all’ to ‘fully agree’)
- d.
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Characteristics of the Participants
3.2. Attitude toward Health and Safety Measures to Prevent SARS-CoV-2 Infections (Research Question 1)
3.3. Univariate Binary Logistic Regression Analysis (Preparation for Answering Research Question 2)
3.4. Multivariate Binary Logistic Regression Analysis (Research Question 2)
4. Discussion
4.1. Variables Not Directly Related to COVID-19
4.2. Perception of SARS-CoV-2 in General and Attitudes toward Health and Safety Measures Implemented to Prevent SARS-CoV-2 Infections in the Study Environment
4.3. Relevance
4.4. Limitations
4.5. Strengths
4.6. Implications and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus disease (COVID-19) pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 25 April 2022).
- Bundesministerium für Gesundheit. Schutz und Prävention [protection and prevention]. Available online: https://www.zusammengegencorona.de/faqs/covid-19/schutz-und-praevention/ (accessed on 4 May 2022).
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.-H.; Jalil, S.M.S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: A systematic review. Hum. Vaccin. Immunother. 2022, 18, 2027160. [Google Scholar] [CrossRef]
- European Medicines Agency. COVID-19 vaccines: Authorised. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/vaccines-covid-19/covid-19-vaccines-authorised#authorised-covid-19-vaccines-section (accessed on 29 June 2022).
- European Centre for Disease Prevention and Control. Facilitating COVID-19 Vaccination Acceptance and Uptake in the EU/EEA. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Facilitating-vaccination-uptake-in-the-EU-EEA.pdf (accessed on 30 June 2022).
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 29 April 2022).
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Baccolini, V.; Renzi, E.; Isonne, C.; Migliara, G.; Massimi, A.; de Vito, C.; Marzuillo, C.; Villari, P. COVID-19 Vaccine Hesitancy among Italian University Students: A Cross-Sectional Survey during the First Months of the Vaccination Campaign. Vaccines 2021, 9, 1292. [Google Scholar] [CrossRef]
- Lo Moro, G.; Cugudda, E.; Bert, F.; Raco, I.; Siliquini, R. Vaccine Hesitancy and Fear of COVID-19 Among Italian Medical Students: A Cross-Sectional Study. J. Community Health 2022, 47, 475–483. [Google Scholar] [CrossRef]
- Montvidas, J.; Basevičiūtė, M.; Burokaitė, K.; Adomaitienė, V.; Lesinskienė, S. COVID-19 Vaccine Hesitancy and Psychosocial Effects of the COVID-19 Pandemic among Health-Science Students of Lithuania—A National Cross-Sectional Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 2870. [Google Scholar] [CrossRef]
- Chamon, Q.; Govindin Ramassamy, K.; Rahis, A.-C.; Guignot, L.; Tzourio, C.; Montagni, I. Persistence of Vaccine Hesitancy and Acceptance of the EU Covid Certificate Among French Students. J. Community Health 2022, 1–8. [Google Scholar] [CrossRef]
- Hilverda, F.; Vollmann, M. The Role of Risk Perception in Students’ COVID-19 Vaccine Uptake: A Longitudinal Study. Vaccines 2021, 10, 22. [Google Scholar] [CrossRef]
- Varol, T.; Schneider, F.; Mesters, I.; Ruiter, R.A.C.; Kok, G.; Hoor, G.A. ten. Facilitating Informed Decision Making: Determinants of University Students’ COVID-19 Vaccine Uptake. Vaccines 2022, 10, 704. [Google Scholar] [CrossRef]
- Tavolacci, M.P.; Dechelotte, P.; Ladner, J. COVID-19 Vaccine Acceptance, Hesitancy, and Resistancy among University Students in France. Vaccines 2021, 9, 654. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; de Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef]
- Norhayati, M.N.; Che Yusof, R.; Azman, Y.M. Systematic Review and Meta-Analysis of COVID-19 Vaccination Acceptance. Front. Med. 2021, 8, 783982. [Google Scholar] [CrossRef]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, J.M.; Pezzuti, T. Vaccination Acceptance Across Cultures: The Roles of Collectivism, Empathy, and Homophily. J. Int. Mark. 2022, 30, 13–27. [Google Scholar] [CrossRef]
- Marzo, R.R.; Ahmad, A.; Islam, M.S.; Essar, M.Y.; Heidler, P.; King, I.; Thiyagarajan, A.; Jermsittiparsert, K.; Songwathana, K.; Younus, D.A.; et al. Perceived COVID-19 vaccine effectiveness, acceptance, and drivers of vaccination decision-making among the general adult population: A global survey of 20 countries. PLoS Negl. Trop. Dis. 2022, 16, e0010103. [Google Scholar] [CrossRef] [PubMed]
- Cocchio, S.; Tremolada, G.; Furlan, P.; Nicoletti, M.; Zabeo, F.; Fonzo, M.; Tonon, M.; Russo, F.; Baldo, V. “Would You Get Vaccinated against COVID-19?” The Picture Emerging from a Study on the Prevalence of SARS-CoV-2 Infection in the General Population of the Veneto Region. Vaccines 2022, 10, 365. [Google Scholar] [CrossRef]
- Sypsa, V.; Roussos, S.; Engeli, V.; Paraskevis, D.; Tsiodras, S.; Hatzakis, A. Trends in COVID-19 Vaccination Intent, Determinants and Reasons for Vaccine Hesitancy: Results from Repeated Cross-Sectional Surveys in the Adult General Population of Greece during November 2020-June 2021. Vaccines 2022, 10, 470. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef]
- Tomietto, M.; Simonetti, V.; Comparcini, D.; Stefanizzi, P.; Cicolini, G. A large cross-sectional survey of COVID-19 vaccination willingness amongst healthcare students and professionals: Reveals generational patterns. J. Adv. Nurs. 2022, 78, 2894–2903. [Google Scholar] [CrossRef]
- Salomoni, M.G.; Di Valerio, Z.; Gabrielli, E.; Montalti, M.; Tedesco, D.; Guaraldi, F.; Gori, D. Hesitant or Not Hesitant? A Systematic Review on Global COVID-19 Vaccine Acceptance in Different Populations. Vaccines 2021, 9, 873. [Google Scholar] [CrossRef]
- Aristovnik, A.; Keržič, D.; Ravšelj, D.; Tomaževič, N.; Umek, L. Impacts of the COVID-19 Pandemic on Life of Higher Education Students: A Global Perspective. Sustainability 2020, 12, 8438. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Belingheri, M.; Ausili, D.; Paladino, M.E.; Luciani, M.; Di Mauro, S.; Riva, M.A. Attitudes towards COVID-19 vaccine and reasons for adherence or not among nursing students. J. Prof. Nurs. 2021, 37, 923–927. [Google Scholar] [CrossRef]
- Gautier, S.; Luyt, D.; Davido, B.; Herr, M.; Cardot, T.; Rousseau, A.; Annane, D.; Delarocque-Astagneau, E.; Josseran, L. Cross-sectional study on COVID-19 vaccine hesitancy and determinants in healthcare students: Interdisciplinary trainings on vaccination are needed. BMC Med. Educ. 2022, 22, 299. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.S.S.; Lee, H.Y.; Leong, J.Z.; Sulaiman, M.M.; Loo, W.F.; Tan, W.W. COVID-19 vaccination acceptance among dental students and dental practitioners: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0267354. [Google Scholar] [CrossRef]
- Marinos, G.; Lamprinos, D.; Georgakopoulos, P.; Patoulis, G.; Vogiatzi, G.; Damaskos, C.; Papaioannou, A.; Sofroni, A.; Pouletidis, T.; Papagiannis, D.; et al. Reported COVID-19 Vaccination Coverage and Associated Factors among Members of Athens Medical Association: Results from a Cross-Sectional Study. Vaccines 2021, 9, 1134. [Google Scholar] [CrossRef]
- Farnell, T.; Skledar Matijevic, A.; Šcukanec Schmidt, N. The Impact of COVID-19 on Higher Education: A Review of Emerging Evidence. Analytical Report; ERIC: Brussels, Belgium, 2021; ISBN 9276213678. [Google Scholar]
- Cullinan, J.; Flannery, D.; Harold, J.; Lyons, S.; Palcic, D. The disconnected: COVID-19 and disparities in access to quality broadband for higher education students. Int. J. Educ. Technol. High. Educ. 2021, 18, 26. [Google Scholar] [CrossRef]
- OECD. The State of Higher Education; OECD Publishing: Paris, France, 2021. [Google Scholar]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Knight, H.; Carlisle, S.; O’Connor, M.; Briggs, L.; Fothergill, L.; Al-Oraibi, A.; Yildirim, M.; Morling, J.R.; Corner, J.; Ball, J.; et al. Impacts of the COVID-19 Pandemic and Self-Isolation on Students and Staff in Higher Education: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 675. [Google Scholar] [CrossRef]
- Donald, W.E.; Jackson, D. Subjective Wellbeing among University Students and Recent Graduates: Evidence from the United Kingdom. Int. J. Environ. Res. Public Health 2022, 19, 6911. [Google Scholar] [CrossRef]
- Savage, M.J.; James, R.; Magistro, D.; Donaldson, J.; Healy, L.C.; Nevill, M.; Hennis, P.J. Mental health and movement behaviour during the COVID-19 pandemic in UK university students: Prospective cohort study. Ment. Health Phys. Act. 2020, 19, 100357. [Google Scholar] [CrossRef]
- Oliveira Carvalho, P.; Hülsdünker, T.; Carson, F. The Impact of the COVID-19 Lockdown on European Students’ Negative Emotional Symptoms: A Systematic Review and Meta-Analysis. Behav. Sci. 2021, 12, 3. [Google Scholar] [CrossRef]
- Mahmud, M.S.; Talukder, M.U.; Rahman, S.M. Does ‘Fear of COVID-19’ trigger future career anxiety? An empirical investigation considering depression from COVID-19 as a mediator. Int. J. Soc. Psychiatry 2021, 67, 35–45. [Google Scholar] [CrossRef]
- Werner, A.M.; Tibubos, A.N.; Mülder, L.M.; Reichel, J.L.; Schäfer, M.; Heller, S.; Pfirrmann, D.; Edelmann, D.; Dietz, P.; Rigotti, T.; et al. The impact of lockdown stress and loneliness during the COVID-19 pandemic on mental health among university students in Germany. Sci. Rep. 2021, 11, 22637. [Google Scholar] [CrossRef]
- Dietz, P.; Reichel, J.L.; Heller, S.; Werner, A.M.; Tibubos, A.N.; Mülder, L.M.; Schäfer, M.; Eisenbarth, L.; Stark, B.; Rigotti, T.; et al. Zehn Thesen zur Situation von Studierenden in Deutschland während der SARS-CoV-2-Pandemie [Ten theses on the situation of higher education students in Germany during the SARS-CoV-2 pandemic]. ASU 2021, 2021, 149–153. [Google Scholar] [CrossRef]
- Baden-Württemberg. Hohe Präsenz- und Impfquoten an den Hochschulen [High attendance and vaccination rates at higher education institutions]. Available online: https://www.baden-wuerttemberg.de/de/service/presse/pressemitteilung/pid/hohe-praesenz-und-impfquoten-an-den-hochschulen/ (accessed on 29 June 2022).
- Landesregierung Baden-Württemberg, Ministerium für Wissenschaft, Forschung und Kunst. Corona-Verordnung Studienbetrieb - CoronaVO Studienbetrieb) [COVID-19 Regulation Study Procedure]. Available online: https://www.baden-wuerttemberg.de/fileadmin/redaktion/dateien/PDF/Coronainfos/210610_CoronaVO_Studienbetrieb_konsolidiert.pdf (accessed on 13 April 2022).
- Robert Koch-Institut. Epidemiologischer Steckbrief zu SARS-CoV-2 und COVID-19 [Epidemiological profile of SARS-CoV-2 and COVID-19]: Risikogruppen für Schwere Verläufe [Risk groups for severe courses]. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=D7ACE9E6FF9AE0E76F31F5E52812B675.internet062?nn=13490888#doc13776792bodyText15 (accessed on 12 May 2022).
- Bundesministerium für Gesundheit. Coronavirus-Pandemie (SARS-CoV-2): Chronik Bisheriger Maßnahmen und Ereignisse [Coronavirus pandemic (SARS-CoV-2): Chronicle of actions and events to date]. Available online: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html (accessed on 13 April 2022).
- Rind, E.; Kimpel, K.; Preiser, C.; Papenfuss, F.; Wagner, A.; Alsyte, K.; Siegel, A.; Klink, A.; Steinhilber, B.; Kauderer, J.; et al. Adjusting working conditions and evaluating the risk of infection during the COVID-19 pandemic in different workplace settings in Germany: A study protocol for an explorative modular mixed methods approach. BMJ Open 2020, 10, e043908. [Google Scholar] [CrossRef]
- Rind, E.; Ehmann, A.; Wagner, A.; Söder, J.; Preiser, C.; Rieger, M.A. Immunization coverage is essential for teaching and learning on campus during the COVID-19 pandemic. Saf. Health Work 2022, 13, S183–S184. [Google Scholar] [CrossRef]
- Stebbins, R.A. Exploratory Research in the Social Sciences; SAGE: Thousand Oaks, CA, USA, 2001; ISBN 9781412984249. [Google Scholar]
- Robert Koch-Institut. 7-Tage-Inzidenzen nach Bundesländern und Kreisen (fixierte Werte) sowie 7-Tage-Inzidenz der Hospitalisierten COVID-19-Fälle Nach Bundesländern (fixierte Werte) [7-day incidences by federal states and counties (fixed values) and 7-day incidence of hospitalised COVID-19 cases by federal states (fixed values)]. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Fallzahlen_Kum_Tab.html (accessed on 10 June 2022).
- UNIPARK. Online Umfrage [online survey]. Available online: https://www.unipark.com/ (accessed on 8 June 2022).
- Rammstedt, B.; Kemper, C.J.; Klein, M.C.; Beierlein, C.; Kovaleva, A. A Short Scale for Assessing the Big Five Dimensions of Personality: 10 Item Big Five Inventory (BFI-10). Methoden Daten Analysen 2013, 7, 2. [Google Scholar] [CrossRef]
- Kemper, C.J.; Beierlein, C.; Bensch, D.; Kovaleva, A.; Rammstedt, B. Allgemeine Bevölkerungsumfrage der Sozialwissenschaften ALLBUS 2006; GESIS—Leibniz Institute for the Social Sciences: Mannheim, Germany, 2006. [Google Scholar]
- Wolter, F.; Mayerl, J.; Andersen, H.; Junkermann, J.; Wieland, T. Überschätzung der Impfquote gegen COVID-19 in Bevölkerungsumfragen: Ergebnisse einer experimentellen Methodenstudie [Overestimation of vaccination coverage against COVID-19 in population surveys: Results of an experimental methods study]. Press release, date of publication: 15 November 2021. Available online: https://osf.io/8kbnd/ (accessed on 28 July 2022).
- WHO Regional Office for Europe. COVID-19 Snapshot MOnitoring (COSMO Standard): Monitoring Knowledge, Risk Perceptions, Preventive Behaviours, and Public Trust in the Current Coronavirus Outbreak—WHO Standard Protocol, Erfurt, Germany. 2020. Available online: https://www.psycharchives.org/en/item/62216bdb-69fa-44e7-92b4-8438b3817341 (accessed on 18 May 2022).
- Betsch, C.; Korn, L.; Burgard, T.; Gaissmaier, W.; Felgendreff, L.; Eitze, S.; Sprengholz, P.; Böhm, R.; Stollorz, V.; Ramharter, M.; et al. The four weeks before lockdown during the COVID-19 pandemic in Germany: A weekly serial cross-sectional survey on risk perceptions, knowledge, public trust and behaviour, 3 to 25 March 2020. Eurosurveillance 2021, 26, 2001900. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Betsch, C.; Wieler, L.; Bosnjak, M.; Ramharter, M.; Stollorz, V.; Omer, S.; Korn, L.; Sprengholz, P.; Felgendreff, L.; Eitze, S.; et al. Germany COVID-19 Snapshot Monitoring (COSMO Germany): Monitoring Knowledge, Risk Perceptions, Preventive Behaviours, and Public Trust in the Current Coronavirus Outbreak in Germany; PsychArchives: Erfurt, Germany, 2020. [Google Scholar]
- Newman, D.A. Missing Data. Organizational Research Methods 2014, 17, 372–411. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE: Los Angeles, CA, USA, 2016. [Google Scholar]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef]
- Harder, T.; Koch, J.; Vygen-Bonnet, S.; Scholz, S.; Pilic, A.; Reda, S.; Wichmann, O. Wie gut schützt die COVID-19-Impfung vor SARS-CoV-2-Infektionen und-Transmission? [How well does COVID-19 vaccination protect against SARS-CoV-2 infection and transmission?]. Epidemiologisches Bulletin 2021, 19, 13–23. [Google Scholar]
- Harder, T.; Koch, J.; Vygen-Bonnet, S.; Külper-Schiek, W.; Pilic, A.; Reda, S.; Scholz, S.; Wichmann, O. Efficacy and effectiveness of COVID-19 vaccines against SARS-CoV-2 infection: Interim results of a living systematic review, 1 January to 14 May 2021. Euro Surveill. 2021, 26. [Google Scholar] [CrossRef]
- Šiđanin, I.; Njegovan, B.R.; Sokolović, B. Students’ Views on Vaccination against COVID-19 Virus and Trust in Media Information about the Vaccine: The Case of Serbia. Vaccines 2021, 9, 1430. [Google Scholar] [CrossRef]
- Mercadante, A.R.; Law, A.V. Will they, or Won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the Health Belief Model. Res. Social Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef]
- Dratva, J.; Wagner, A.; Zysset, A.; Volken, T. To Vaccinate or Not to Vaccinate-This Is the Question among Swiss University Students. Int. J. Environ. Res. Public Health 2021, 18, 9210. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.A.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Environ. Res. Public Health 2021, 18, 2407. [Google Scholar] [CrossRef] [PubMed]
- Sovicova, M.; Zibolenova, J.; Svihrova, V.; Hudeckova, H. Odds Ratio Estimation of Medical Students’ Attitudes towards COVID-19 Vaccination. Int. J. Environ. Res. Public Health 2021, 18, 6815. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Betsch, Cornelia & Team COSMO. Zusammenfassung und Empfehlungen Wellen 48 bis 51 [Summary and recommendations Waves 48 to 51]: Erhebungen vom 27./28.07.2021 bis 07./08.09.2021 [Surveys from 27/28/07/2021 to 07/08/09/2021]. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/summary/48-51/ (accessed on 17 May 2022).
- Savadori, L.; Lauriola, M. Risk perceptions and COVID-19 protective behaviors: A two-wave longitudinal study of epidemic and post-epidemic periods. Social Science & Medicine 2022, 301, 114949. [Google Scholar] [CrossRef]
- Chen, I.-H.; Ahorsu, D.K.; Ko, N.-Y.; Yen, C.-F.; Lin, C.-Y.; Griffiths, M.D.; Pakpour, A.H. Adapting the Motors of Influenza Vaccination Acceptance Scale into the Motors of COVID-19 Vaccination Acceptance Scale: Psychometric evaluation among mainland Chinese university students. Vaccine 2021, 39, 4510–4515. [Google Scholar] [CrossRef]
- Rayani, M.; Rayani, S.; Najafi-Sharjabad, F. COVID-19-related knowledge, risk perception, information seeking, and adherence to preventive behaviors among undergraduate students, southern Iran. Environ. Sci. Pollut. Res. Int. 2021, 28, 59953–59962. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Lawrence, S. Predictors of COVID-19 vaccine hesitancy in Germany: A cross-sectional, population-based study. Postgrad. Med. J. 2022, 0, 1–9. [Google Scholar] [CrossRef]
- Wang, D.; Marmo-Roman, S.; Krase, K.; Phanord, L. Compliance with preventative measures during the COVID-19 pandemic in the USA and Canada: Results from an online survey. Soc. Work Health Care 2021, 60, 240–255. [Google Scholar] [CrossRef]
- Kleitman, S.; Fullerton, D.J.; Zhang, L.M.; Blanchard, M.D.; Lee, J.; Stankov, L.; Thompson, V. To comply or not comply? A latent profile analysis of behaviours and attitudes during the COVID-19 pandemic. PLoS ONE 2021, 16, e0255268. [Google Scholar] [CrossRef]
- Sinclair, R.R.; Probst, T.M.; Watson, G.P.; Bazzoli, A. Caught between Scylla and Charybdis: How economic stressors and occupational risk factors influence workers’ occupational health reactions to COVID-19. Appl. Psychol. 2020. [Google Scholar] [CrossRef]
- Rodríguez-Blázquez, C.; Romay-Barja, M.; Falcón, M.; Ayala, A.; Forjaz, M.J. The COSMO-Spain Survey: Three First Rounds of the WHO Behavioral Insights Tool. Front. Public Health 2021, 9, 678926. [Google Scholar] [CrossRef]
- Rieger, M.A. Neues COVID-19-Impfangebot der Universität [New COVID-19 vaccination offer at the university]: Rundmail des Betriebsärztlichen Dienstes [Circular from the university medical service to all employees and students]. Date of publication: 6 October 2021. Available online: https://uni-tuebingen.de/universitaet/infos-zum-coronavirus/newsfullview-coronavirus/article/neues-covid-19-impfangebot-der-universitaet/ (accessed on 28 July 2022).
- Hamilton, K.; Hagger, M.S. The Vaccination Concerns in COVID-19 Scale (VaCCS): Development and validation. PLoS ONE 2022, 17, e0264784. [Google Scholar] [CrossRef]
- Gregory, M.E.; MacEwan, S.R.; Powell, J.R.; Volney, J.; Kurth, J.D.; Kenah, E.; Panchal, A.R.; McAlearney, A.S. The COVID-19 vaccine concerns scale: Development and validation of a new measure. Hum. Vaccin. Immunother. 2022, 1–7. [Google Scholar] [CrossRef]
- Die Bundesregierung. Corona: Arbeitsschutz, Kurzarbeit, Grundsicherung [Corona: Occupational health and safety, short-time work, basic benefits]. Available online: https://www.bundesregierung.de/breg-de/themen/coronavirus/informationen-fuer-arbeitnehmer-in-der-corona-pandemie-1821408 (accessed on 29 July 2022).
- Robert Koch-Institut. Digitales Impfquotenmonitoring zur COVID-19-Impfung [COVID-19 vaccination digital quota monitoring]. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquoten-Tab.html (accessed on 15 July 2022).
- Elliott, L.; Yang, K. Vaccine Acceptance and Hesitancy among College Students in Nevada: A State-Wide Cross-Sectional Study. Vaccines 2022, 10, 105. [Google Scholar] [CrossRef]
- Peterson, C.J.; Abohelwa, M.; Payne, D.; Mohamed, A.A.; Nugent, K. 2019 Novel Coronavirus Vaccination Among Medical Students. J. Prim. Care Community Health 2021, 12, 21501327211058316. [Google Scholar] [CrossRef] [PubMed]
- Haug, S.; Schnell, R.; Weber, K. Impfbereitschaft mit einem COVID-19-Vakzin und Einflussfaktoren. Ergebnisse einer telefonischen Bevölkerungsbefragung [Vaccination readiness with a COVID-19 vaccine and influencing factors. Results of a telephone population survey]. Gesundheitswesen 2021, 83, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Ambros, M.; Frenkel, M. What Determines COVID-19 Vaccination Rates in Germany? Jahrbücher für Nationalökonomie und Statistik 2022, 242, 149–157. [Google Scholar] [CrossRef]
- Fobiwe, J.P.; Martus, P.; Poole, B.D.; Jensen, J.L.; Joos, S. Influences on Attitudes Regarding COVID-19 Vaccination in Germany. Vaccines 2022, 10, 658. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Specification | n (%) | Valid Percentage * |
|---|---|---|---|
| Age (years) (n = 6259) | Mean (SD) | 24 (4.2) | |
| Median | 23 | ||
| Range | 18–70 | ||
| Gender | Female | n = 4106 (62.6) | 64.8 |
| Male | n = 2226 (34.0) | 35.2 | |
| Divers | n = 49 (0.7) | ||
| Missing | n = 175 (2.7) | ||
| Affiliation to risk group for developing severe COVID-19 courses (pre-existing conditions 1) | Yes | n = 597 (9.1) | 9.4 |
| No | n = 5764 (87.9) | 90.6 | |
| Missing | n = 195 (3.0) | ||
| Confirmed SARS-CoV-2 infection | Yes | n = 312 (4.8) | 5.6 |
| No | n = 5220 (79.6) | 94.4 | |
| Missing | n = 1024 (15.6) | ||
| Received at least one dose of COVID-19 vaccine | Yes | n = 5935 (90.5) | 91.4 |
| No | n = 555 (8.5) | 8.6 | |
| Missing | n = 66 (1.0) | ||
| Nationality | German | n = 6143 (93.7) | 95.2 |
| Other | n = 308 (4.7) | 4.8 | |
| Missing | n = 105 (1.6) | ||
| Part-time job while studying | Yes | n = 2549 (38.9) | 39.5 |
| No | n = 3902 (59.5) | 60.5 | |
| Missing | n = 105 (1.6) | ||
| Living in a committed relationship | Yes | n = 3037 (46.3) | 48.1 |
| No | n = 3277 (50.0) | 51.9 | |
| Missing | n = 242 (3.7) | ||
| Number of household members | Living alone with no other person | n = 657 (10.0) | 10.2 |
| Living with one other person | n = 1691 (25.8) | 26.2 | |
| Living with 3–4 other persons | n = 2854 (43.5) | 44.2 | |
| Living with more than 4 other persons | n = 1256 (19.2) | 19.4 | |
| Missing | n = 98 (1.5) | ||
| Health professional within household | Yes | n = 1502 (22.9) | 23.5 |
| No | n = 4897 (74.7) | 76.5 | |
| Missing | n = 157 (2.4) | ||
| Trait extraversion 2 (n = 6495) | Mean (SD) | 3.17 (1.04) | |
| Trait agreeableness 2 (n = 6494) | Mean (SD) | 3.23 (0.81) | |
| Trait conscientiousness 2 (n = 6494) | Mean (SD) | 3.65 (0.83) | |
| Trait neuroticism 2 (n = 6494) | Mean (SD) | 3.07 (0.98) | |
| Trait openness to experiences 2 (n = 6490) | Mean (SD) | 3.57 (1.02) |
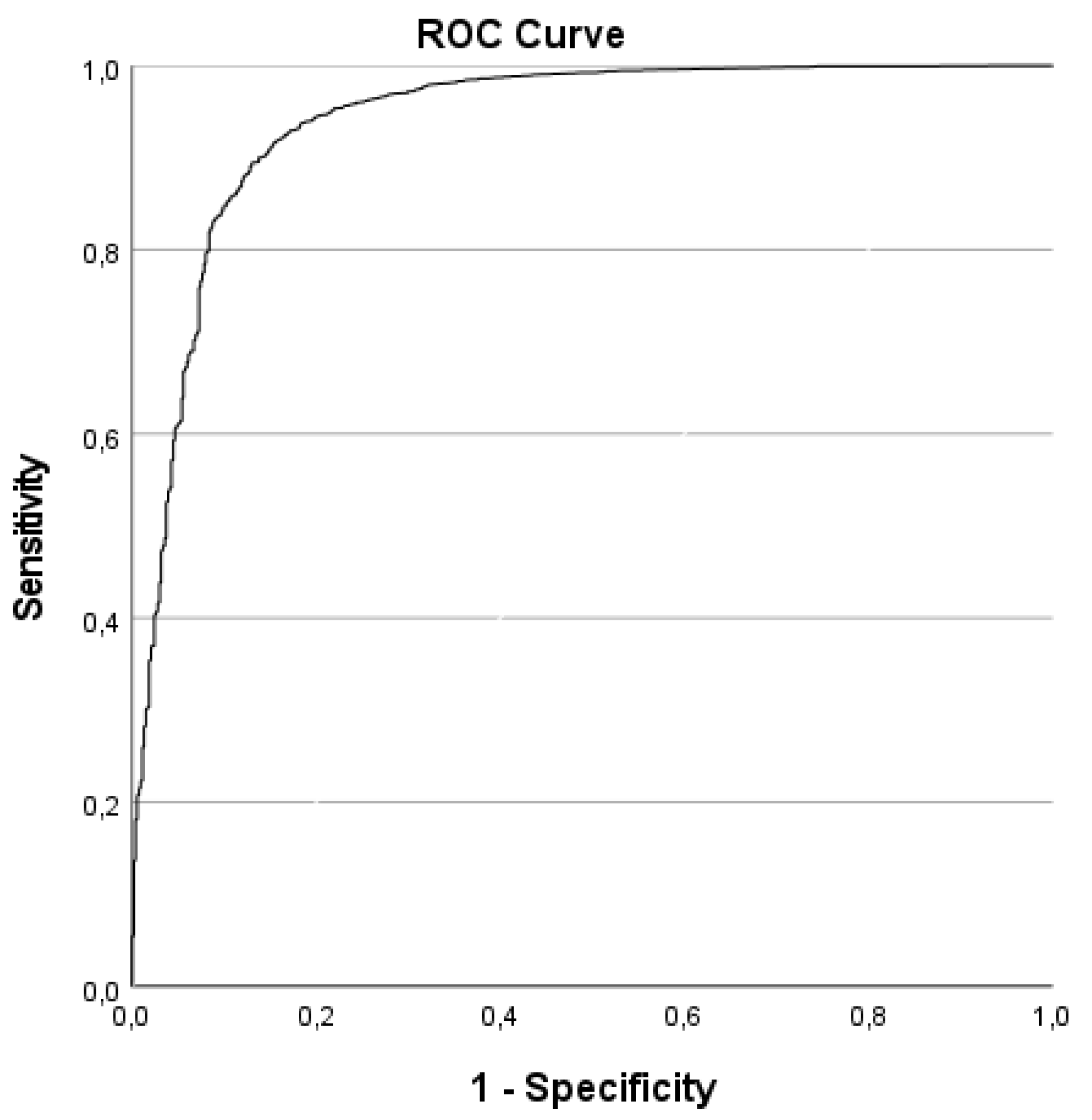
| Variable Group from the Questionnaire (Step) Block | Hosmer and Lemeshow Test | −2 Log Likelihood | Cox & Snell R Square | Nagelkerke Pseudo R2 | Area under the ROC Curve (AUC) | |
|---|---|---|---|---|---|---|
| Control variables: HEI affiliation with five categorical variables with dummy-coding and two social desirability scores [52] | χ2(8) = 2.513 p = 0.961 | 3633.915 | 0.009 | 0.020 | 0.589 | |
 | +(II) Perception of SARS-CoV-2 in general (Affective risk perception, Perception of the outbreak as a media-hype) | χ2(8) = 48.822 p < 0.001 | 2798.381 | 0.130 | 0.297 | 0.831 |
| +(III) Attitude toward health and safety measures to prevent SARS-CoV-2 infections (behavioral and structural preventive measures in the study environment) | χ2(8) = 48.178 p < 0.001 | 2787.634 | 0.132 | 0.300 | 0.833 | |
| +(V) Variables relating to COVID-19 vaccination (own health, COVID-19 vaccine safety, avoidance of disadvantages of the pandemic for HEIs, contribution to the containment of the pandemic) | χ2(8) = 5.424 p = 0.711 | 1698.670 | 0.268 | 0.610 | 0.939 | |
| Explanatory Variables (Factors) * | Regression-Coefficient B | Wald Statistics | p-Value | Adjusted Odds Ratio * (aOR) | 95% Confidence Interval for OR | ||
|---|---|---|---|---|---|---|---|
| Variable Group | Variables (Range: Low to High) | Lower Limit | Upper Limit | ||||
| (II) Perception of SARS-CoV-2 in general 1 | Affective risk perception | 0.161 | 7.101 | 0.008 | 1.175 | 1.044 | 1.323 |
| Perception of the outbreak as a media-hype | −0.174 | 7.997 | 0.005 | 0.840 | 0.744 | 0.948 | |
| (III) Attitude toward health and safety measures to prevent SARS-CoV-2 infections | Attitude toward behavioral preventive measures in the study environment | −0.310 | 4.825 | 0.028 | 0.733 | 0.556 | 0.967 |
| Attitude toward structural preventive measures in the study environment | −0.247 | 3.981 | 0.046 | 0.781 | 0.613 | 0.996 | |
| (V) Variables relating to COVID-19 vaccination | Vaccinating against COVID-19 mainly helps to preserve my health. 1 | 0.270 | 43.230 | <0.001 | 1.310 | 1.209 | 1.420 |
| I am completely confident that vaccination against COVID-19 is safe. 1,2 | 0.505 | 127.923 | <0.001 | 1.656 | 1.518 | 1.808 | |
| Vaccinating against COVID-19 primarily helps higher education to eliminate the disadvantages caused by the pandemic. | 0.150 | 14.582 | <0.001 | 1.161 | 1.076 | 1.254 | |
| I contribute to the containment of the pandemic by vaccinating against COVID-19. 1 | 0.501 | 111.078 | <0.001 | 1.650 | 1.503 | 1.811 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neunhöffer, A.T.; Gibilaro, J.; Wagner, A.; Soeder, J.; Rebholz, B.; Blumenstock, G.; Martus, P.; Rieger, M.A.; Rind, E. Factors Associated with the COVID-19 Vaccination Status of Higher Education Students: Results of an Online Cross-Sectional Survey at Six Universities in Southwestern Germany. Vaccines 2022, 10, 1433. https://doi.org/10.3390/vaccines10091433
Neunhöffer AT, Gibilaro J, Wagner A, Soeder J, Rebholz B, Blumenstock G, Martus P, Rieger MA, Rind E. Factors Associated with the COVID-19 Vaccination Status of Higher Education Students: Results of an Online Cross-Sectional Survey at Six Universities in Southwestern Germany. Vaccines. 2022; 10(9):1433. https://doi.org/10.3390/vaccines10091433
Chicago/Turabian StyleNeunhöffer, Anna T., Jolanda Gibilaro, Anke Wagner, Jana Soeder, Benjamin Rebholz, Gunnar Blumenstock, Peter Martus, Monika A. Rieger, and Esther Rind. 2022. "Factors Associated with the COVID-19 Vaccination Status of Higher Education Students: Results of an Online Cross-Sectional Survey at Six Universities in Southwestern Germany" Vaccines 10, no. 9: 1433. https://doi.org/10.3390/vaccines10091433
APA StyleNeunhöffer, A. T., Gibilaro, J., Wagner, A., Soeder, J., Rebholz, B., Blumenstock, G., Martus, P., Rieger, M. A., & Rind, E. (2022). Factors Associated with the COVID-19 Vaccination Status of Higher Education Students: Results of an Online Cross-Sectional Survey at Six Universities in Southwestern Germany. Vaccines, 10(9), 1433. https://doi.org/10.3390/vaccines10091433