
Drivers of Routine and Outbreak Vaccination Uptake in the Western Democratic Republic of Congo: An Exploratory Study in Ten Health Zones

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Sites and Populations
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Study Population
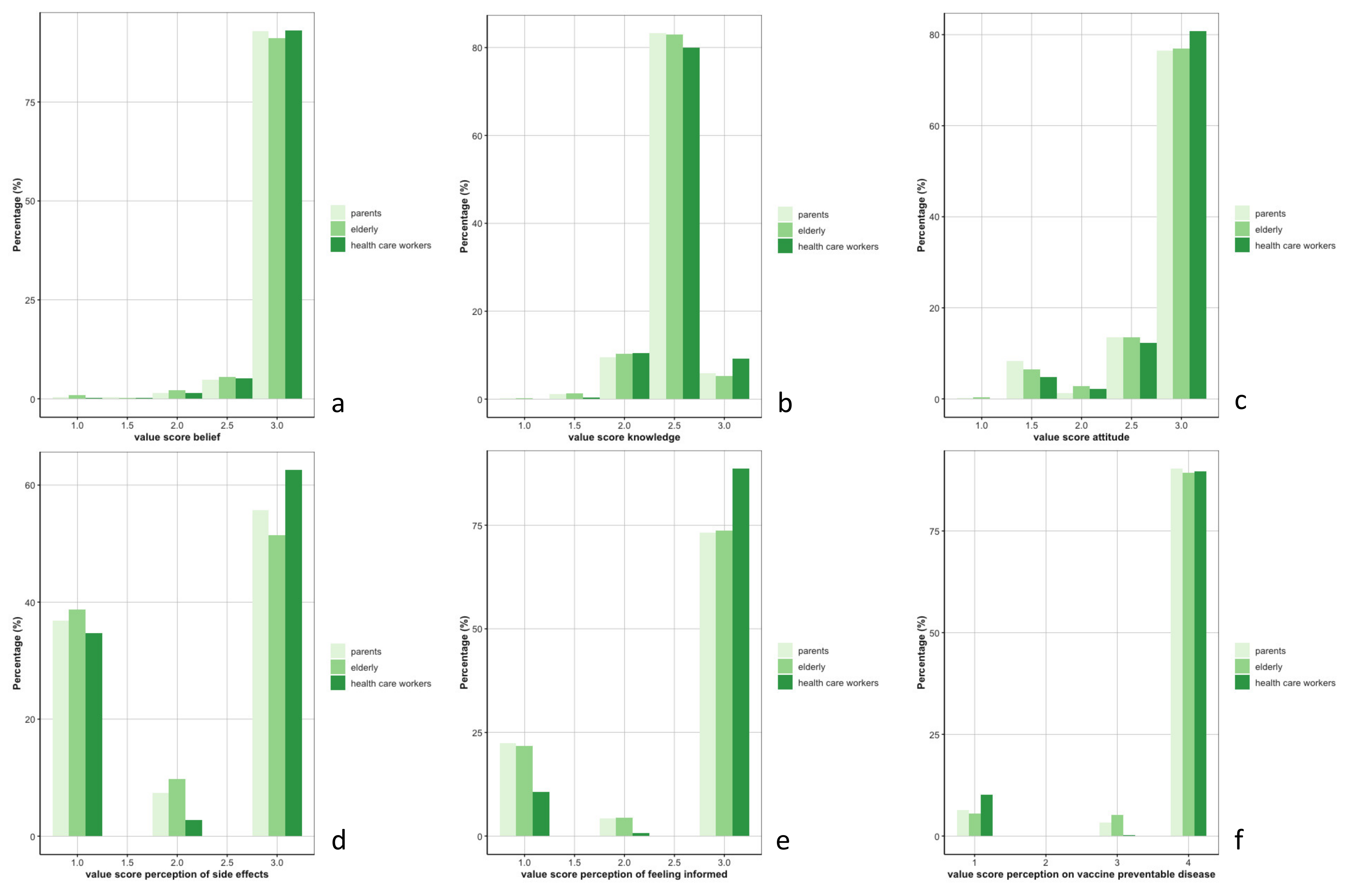
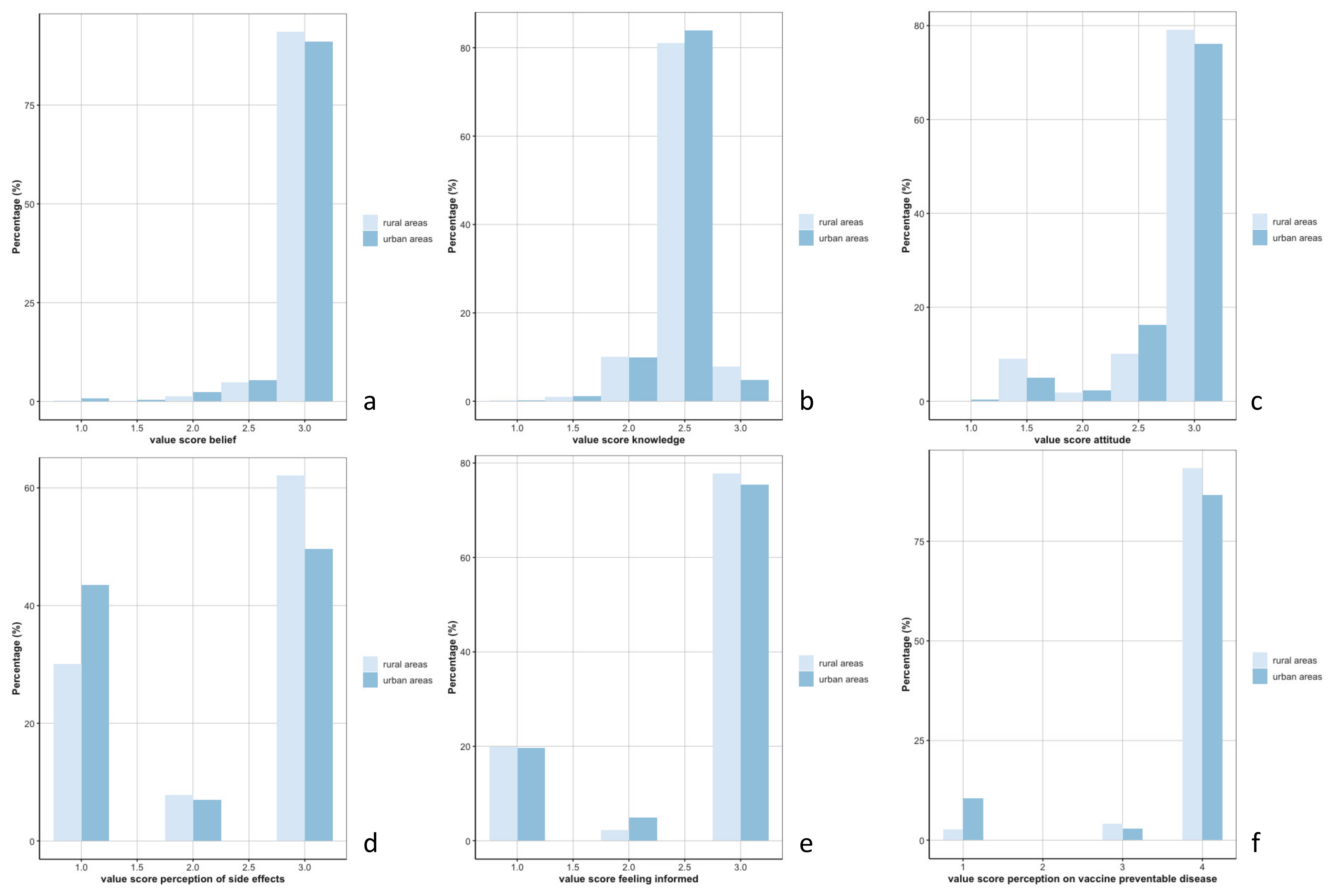
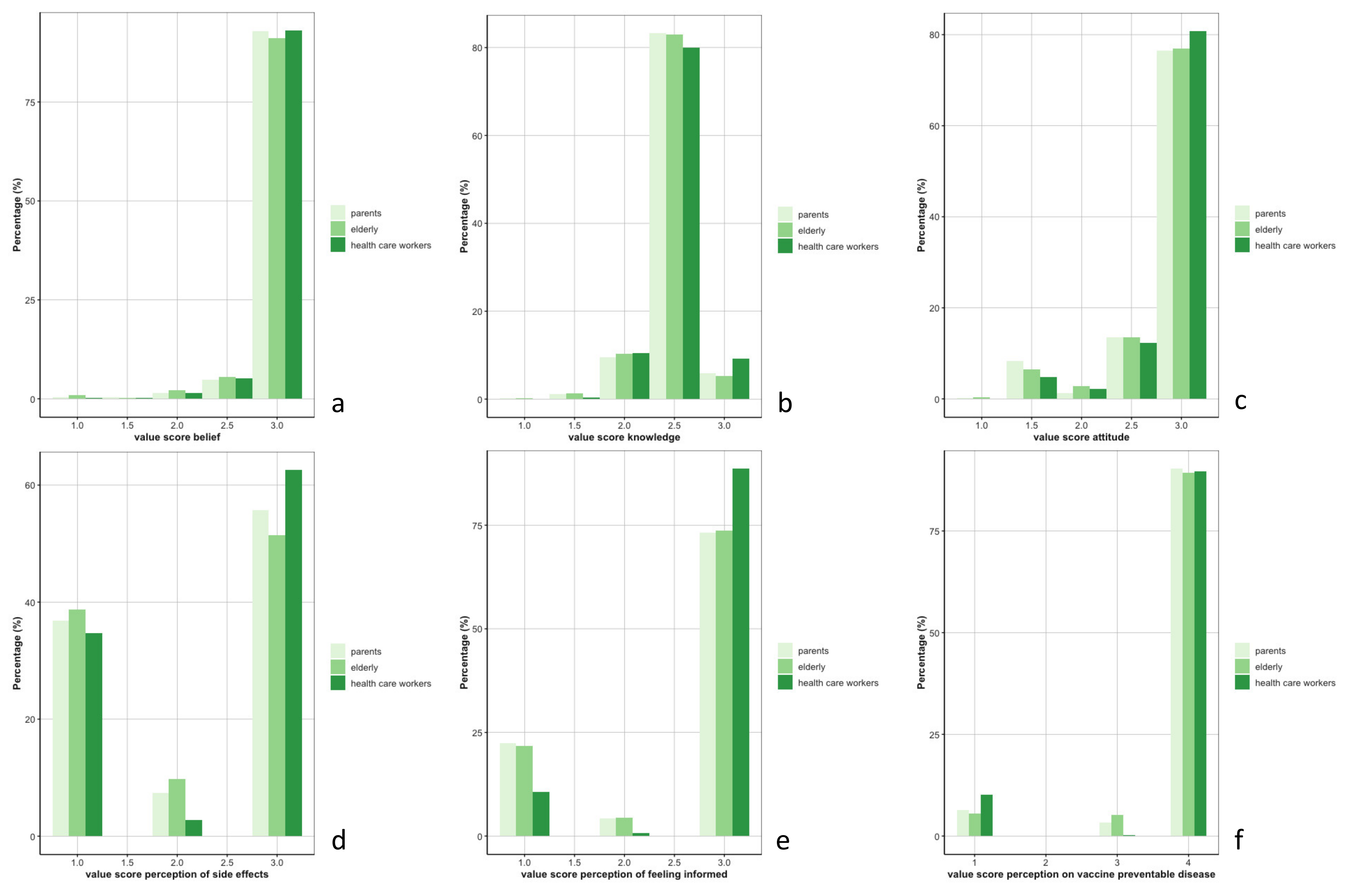
3.2. Analysis of the KAP Concepts
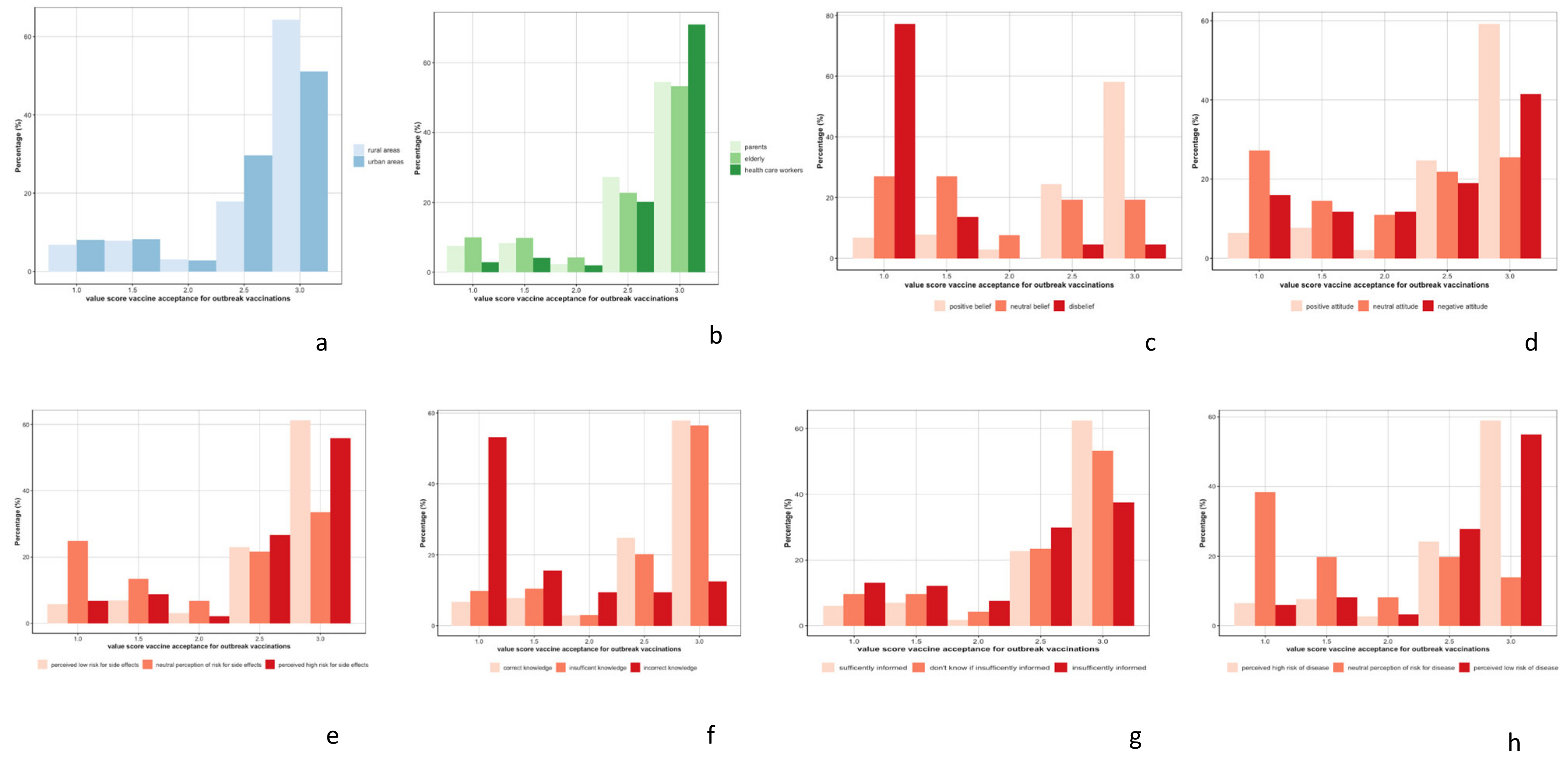
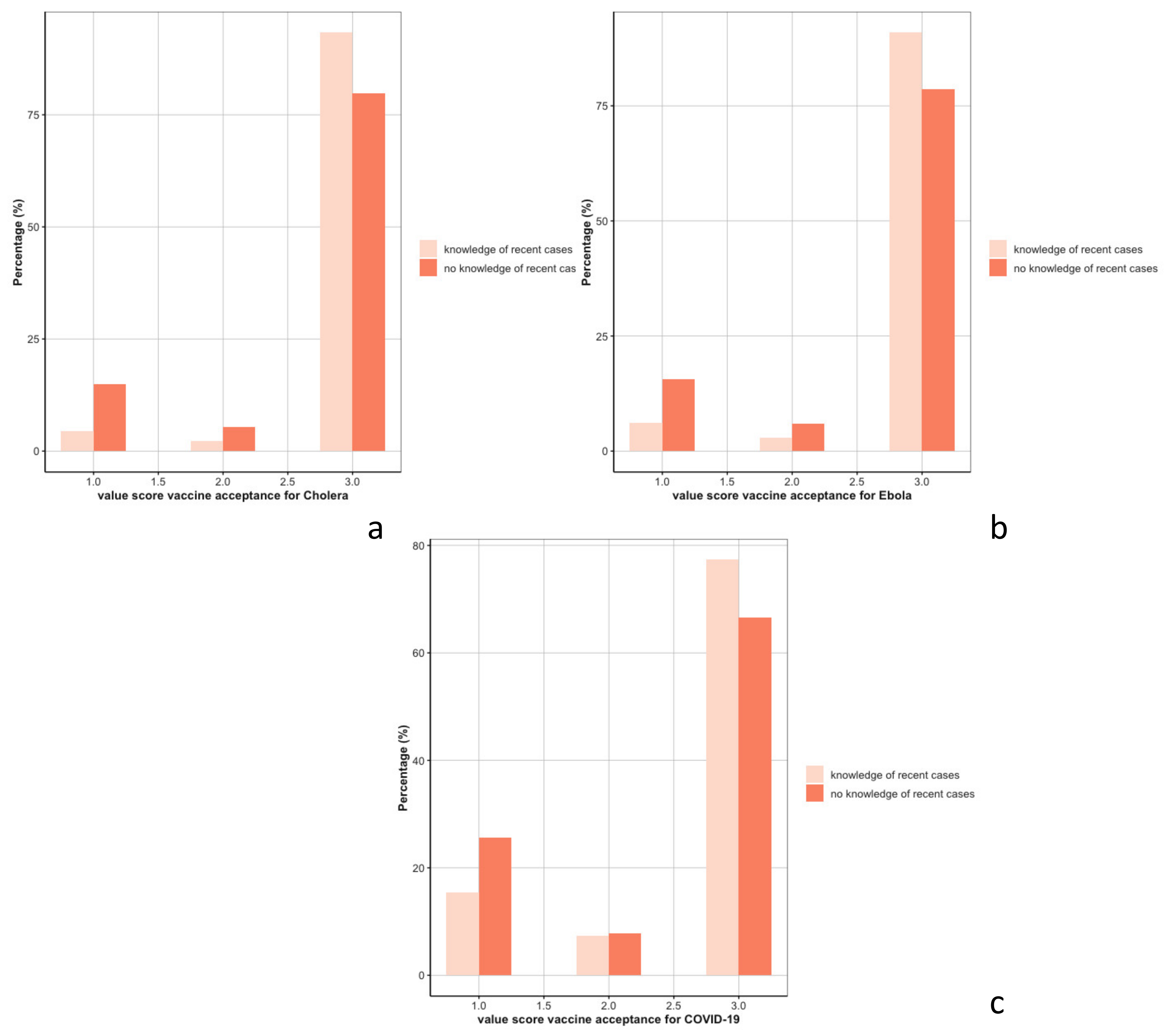
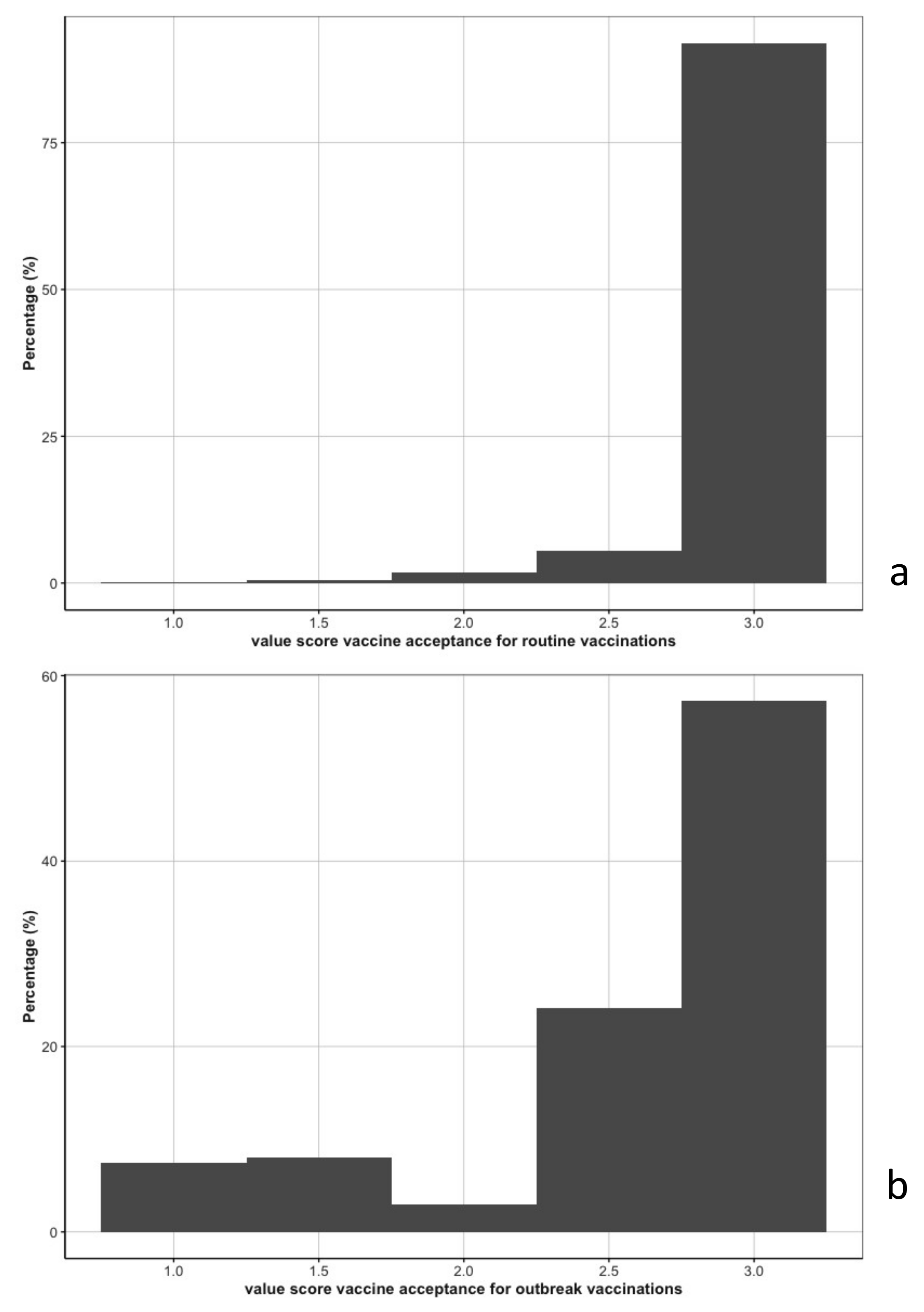
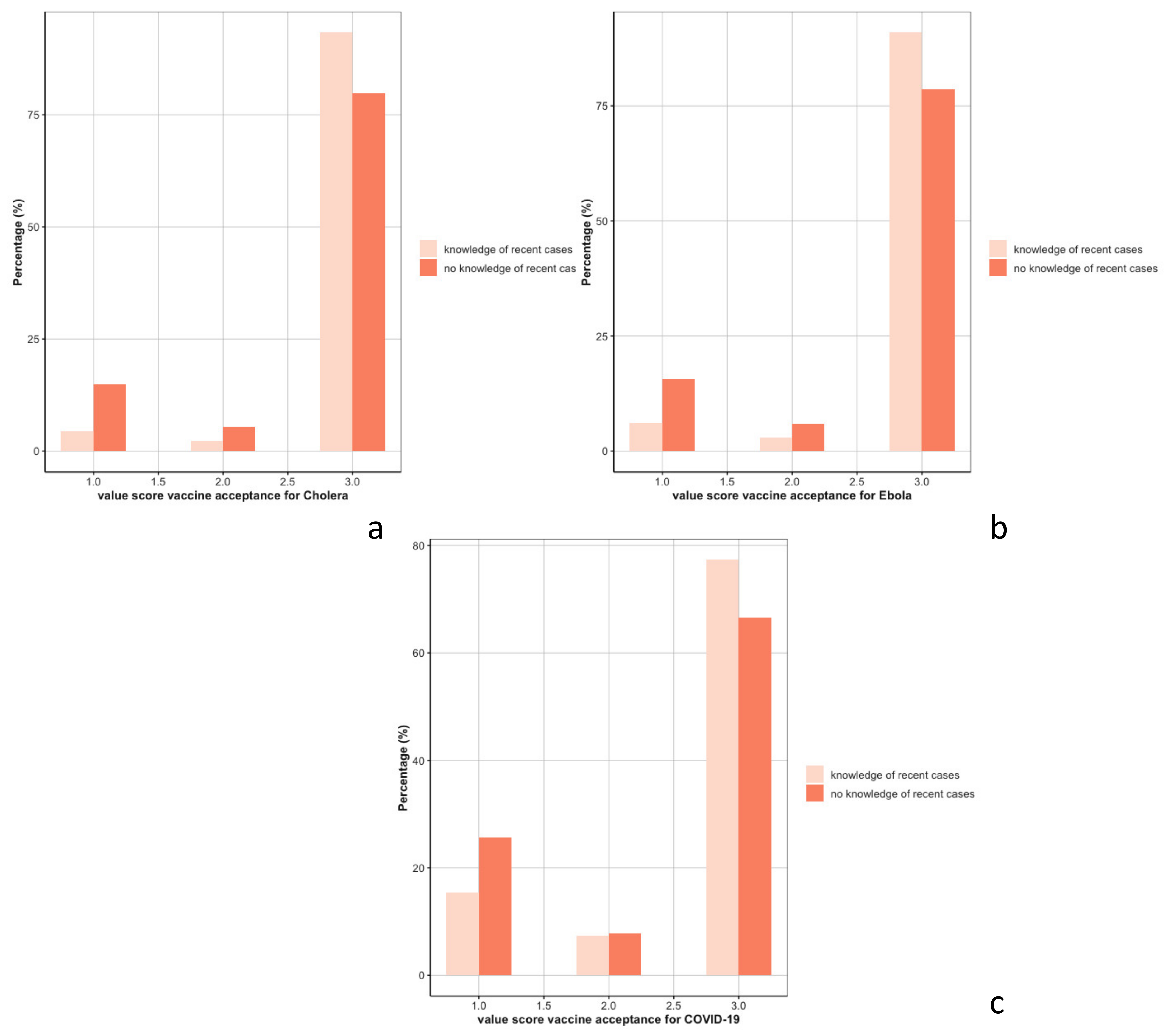
3.3. Vaccine Acceptance
3.4. Supply Chain Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Plotkin, S.A. Vaccine: Past present, future. Nat. Med. 2005, 11, S5–S11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. In Vaccine Hesitancy; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Abbas, K.; Procter, S.R.; van Zandvoort, K.; Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; Flasche, S.; et al. Routine childhood immunisation during the COVID-19 pandemic in Africa: A benefit–risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob. Health 2020, 8, e1264–e1272. [Google Scholar] [CrossRef]
- Buonsenso, D.; Cinicola, B.; Kallon, M.N.; Iodice, F. Child Healthcare and Immunizations in Sub-Saharan Africa During the COVID-19 Pandemic. Front. Pediatr. 2020, 8, 517. [Google Scholar] [CrossRef] [PubMed]
- Chandir, S.; Siddiqi, D.A.; Setayesh, H.; Khan, A.J. Impact of COVID-19 lockdown on routine immunisation in Karachi, Pakistan. Lancet Glob. Health 2020, 8, e1118–e1120. [Google Scholar] [CrossRef]
- Chandir, S.; Siddiqi, D.A.; Mehmood, M.; Setayesh, H.; Siddique, M.; Mirza, A.; Soundardjee, R.; Dharma, V.K.; Shah, M.T.; Abdullah, S.; et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: An analysis of provincial electronic immunization registry data. Vaccine 2020, 38, 7146–7155. [Google Scholar] [CrossRef]
- Roberts, L. Why measles deaths are surging—And coronavirus could make it worse. Nature 2020, 580, 446–447. [Google Scholar] [CrossRef]
- Ogundele, O.A.; Omotoso, A.A.; Fagbemi, A.T. COVID-19 outbreak: A potential threat to routine vaccination programme activities in Nigeria. Hum. Vaccines Immunother. 2021, 17, 661–663. [Google Scholar] [CrossRef]
- Siedner, M.J.; Kraemer, J.D.; Meyer, M.J.; Harling, G.; Mngomezulu, T.; Gabela, P.; Dlamini, S.; Gareta, D.; Majozi, N.; Ngwenya, N.; et al. Access to primary healthcare during lockdown measures for COVID-19 in rural South Africa: An interrupted time series analysis. BMJ Open 2020, 10, e043763. [Google Scholar] [CrossRef]
- Suwantika, A.A.; Boersma, C.; Postma, M.J. The potential impact of COVID-19 pandemic on the immunization performance in Indonesia. Expert Rev. Vaccines 2020, 19, 687–690. [Google Scholar] [CrossRef]
- Dodd, R.H.; Pickles, K.; Nickel, B.; Cvejic, E.; Ayre, J.; Batcup, C.; Bonner, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Concerns and motivations about COVID-19 vaccination. Lancet Infect. Dis. 2021, 21, 161–163. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Matsungo, T.M.; Chopera, P. Effect of the COVID-19-induced lockdown on nutrition, health and lifestyle patterns among adults in Zimbabwe. BMJ Nutr. Prev. Health 2020, 3, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Saso, A.; Skirrow, H.; Kampmann, B. Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network. Vaccines 2020, 8, 556. [Google Scholar] [CrossRef]
- Shet, A.; Carr, K.; Danovaro-Holliday, M.C.; Sodha, S.V.; Prosperi, C.; Wunderlich, J.; Wonodi, C.; Reynolds, H.W.; Mirza, I.; Gacic-Dobo, M.; et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: Evidence of disruption and recovery from 170 countries and territories. Lancet Glob. Health 2022, 10, e186–e194. [Google Scholar] [CrossRef]
- Dyer, O. DRC faces new Ebola outbreak, COVID-19, and measles all at once. BMJ 2020, 369, m2219. [Google Scholar] [CrossRef]
- Michel-Kabamba, N.; Christophe-Luhata, L.; Ngatu, N.R.; Othepa, C.; Bertin-Lora, M.; Arsene-Kabwaya, M.; Bateyi, S.H.; Hoff, N.A.; Leon-Kabamba, N.; Muzembo, B.A.; et al. Impact of Eastern Congo Ebola Outbreak on Child Health Services Delivery: Decline of Routine Child Immunization and Need for Vaccine Supplementation. Res. Sq. 2019. [Google Scholar] [CrossRef]
- Hategeka, C.; Carter, S.E.; Chenge, F.M.; Katanga, E.N.; Lurton, G.; Mayaka, S.M.-N.; Mwamba, D.K.; van Kleef, E.; Vanlerberghe, V.; Grépin, K.A. Impact of the COVID-19 pandemic and response on the utilisation of health services in public facilities during the first wave in Kinshasa, the Democratic Republic of the Congo. BMJ Glob. Health 2021, 6, e005955. [Google Scholar] [CrossRef]
- Ditekemena, J.D.; Nkamba, D.M.; Mutwadi, A.; Mavoko, H.M.; Siewe Fodjo, J.N.; Luhata, C.; Obimpeh, M.; Van Hees, S.; Nachega, J.B.; Colebunders, R. COVID-19 Vaccine Acceptance in the Democratic Republic of Congo: A Cross-Sectional Survey. Vaccines 2021, 9, 153. [Google Scholar] [CrossRef]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- World Health Organization. Training for Mid-Level Managers: The EPI Coverage Survey; WHO Expanded Programme on Immunization: Geneva, Switzerland, 1991. [Google Scholar]
- Gilkey, M.B.; Magnus, B.E.; Reiter, P.L.; McRee, A.-L.; Dempsey, A.F.; Brewer, N.T. The Vaccination Confidence Scale: A brief measure of parents’ vaccination beliefs. Vaccine 2014, 32, 6259–6265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilkey, M.B.; Reiter, P.L.; Magnus, B.E.; McRee, A.-L.; Dempsey, A.F.; Brewer, N.T. Validation of the Vaccination Confidence Scale: A Brief Measure to Identify Parents at Risk for Refusing Adolescent Vaccines. Acad. Pediatr. 2016, 16, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.A.; de Melker, H.E.; Timmermans, D.R.; Mollema, L. Informed decision making in the context of childhood immunization. Patient Educ. Couns. 2017, 100, 2339–2345. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [Green Version]
- Faye, S.L.B.; Krumkamp, R.; Doumbia, S.; Tounkara, M.; Strauss, R.; Ouedraogo, H.G.; Sagna, T.; Barry, A.M.; Mbawah, A.K.; Doumbia, C.O.; et al. Factors influencing hesitancy towards adult and child COVID-19 vaccines in rural and urban West Africa: A cross-sectional study. BMJ Open 2022, 12, e059138. [Google Scholar] [CrossRef]
- Pugliese-Garcia, M.; Heyerdahl, L.W.; Mwamba, C.; Nkwemu, S.; Chilengi, R.; Demolis, R.; Guillermet, E.; Sharma, A. Factors influencing vaccine acceptance and hesitancy in three informal settlements in Lusaka, Zambia. Vaccine 2018, 36, 5617–5624. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Kumar, D.; Chandra, R.; Mathur, M.; Samdariya, S.; Kapoor, N. Vaccine hesitancy: Understanding better to address better. Isr. J. Health Policy Res. 2016, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Wiysonge, C.S.; Uthman, O.A.; Ndumbe, P.M.; Hussey, G.D. Individual and Contextual Factors Associated with Low Childhood Immunisation Coverage in Sub-Saharan Africa: A Multilevel Analysis. PLoS ONE 2012, 7, e37905. [Google Scholar] [CrossRef] [Green Version]
- Mwamba, G.N.; Yoloyolo, N.; Masembe, Y.; Nsambu, M.N.; Nzuzi, C.; Tshekoya, P.; Dah, B.; Kaya, G. Vaccination coverage and factors influencing routine vaccination status in 12 high risk health zones in the Province of Kinshasa City, Democratic Republic of Congo (DRC), 2015. Pan Afr. Med. J. 2017, 27 (Suppl. 3), 7. [Google Scholar] [CrossRef] [PubMed]
- Venturas, C.; Umeh, K. Health professional feedback on HPV vaccination roll-out in a developing country. Vaccine 2017, 35, 1886–1891. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.L.; McCloskey, L.; Mwale, M.; Mwananyanda, L.; Murray, K.; Herman, A.R.; Thea, D.M.; MacLeod, W.B.; Gill, C.J. “When you are injected, the baby is protected”: Assessing the acceptability of a maternal Tdap vaccine based on mothers’ knowledge, attitudes, and beliefs of pertussis and vaccinations in Lusaka, Zambia. Vaccine 2018, 36, 3048–3053. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Jacoby, J.; Matell, M.S. Three-Point Likert Scales Are Good Enough. J. Mark. Res. 1971, 8, 495. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, D.R.; Hulbert, J. Are Three-Point Scales Always Good Enough? J. Mark. Res. 1972, 9, 444–446. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | All Participants | |
|---|---|---|
| (n = 2751) | ||
| Health zones | n (%) | |
| Boko | 280 (10) | |
| Boma | 249 (9) | |
| Kenge | 226 (8) | |
| Kikwit nord | 306 (11) | |
| Limete | 260 (9) | |
| Lusanga | 276 (10) | |
| Masi Manimba | 296 (11) | |
| Matadi | 413 (15) | |
| Mbanza Ngungu | 231 (8) | |
| Nsele | 214 (8) | |
| Gender | n (%) | |
| Female | 1792 (65) | |
| Male | 959 (35) | |
| Participant group | n (%) | Age (in years) (median, IQR) |
| Health care workers | 546 (20) | 41 (33–51) |
| Parents of children < 5 years old | 1165 (42) | 30 (25–37) |
| Elderly (≥55 years) | 1040 (38) | 59 (57–65) |
| Educational level | n (%) | |
| None | 225 (8) | |
| Primary school | 581 (21) | |
| Secondary school | 1282 (47) | |
| University | 625 (23) | |
| Other | 25 (1) | |
| Don’t know | 9 (<1) | |
| Refused to respond | 4 (<1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peckeu-Abboud, L.; Mangoni, P.; Chammam, K.; Kwete, P.; Mutombo Lupola, P.; Vanlerberghe, V.; Yango, J.; Meudec, M.; Ifufa, C.; van der Sande, M.A.B.; et al. Drivers of Routine and Outbreak Vaccination Uptake in the Western Democratic Republic of Congo: An Exploratory Study in Ten Health Zones. Vaccines 2022, 10, 1066. https://doi.org/10.3390/vaccines10071066
Peckeu-Abboud L, Mangoni P, Chammam K, Kwete P, Mutombo Lupola P, Vanlerberghe V, Yango J, Meudec M, Ifufa C, van der Sande MAB, et al. Drivers of Routine and Outbreak Vaccination Uptake in the Western Democratic Republic of Congo: An Exploratory Study in Ten Health Zones. Vaccines. 2022; 10(7):1066. https://doi.org/10.3390/vaccines10071066
Chicago/Turabian StylePeckeu-Abboud, Laurene, Patrick Mangoni, Kaouther Chammam, Papy Kwete, Patrick Mutombo Lupola, Veerle Vanlerberghe, Jepsy Yango, Marie Meudec, Christian Ifufa, Marianne A. B. van der Sande, and et al. 2022. "Drivers of Routine and Outbreak Vaccination Uptake in the Western Democratic Republic of Congo: An Exploratory Study in Ten Health Zones" Vaccines 10, no. 7: 1066. https://doi.org/10.3390/vaccines10071066
APA StylePeckeu-Abboud, L., Mangoni, P., Chammam, K., Kwete, P., Mutombo Lupola, P., Vanlerberghe, V., Yango, J., Meudec, M., Ifufa, C., van der Sande, M. A. B., Madinga Ntwan, J., & Mbala, P. (2022). Drivers of Routine and Outbreak Vaccination Uptake in the Western Democratic Republic of Congo: An Exploratory Study in Ten Health Zones. Vaccines, 10(7), 1066. https://doi.org/10.3390/vaccines10071066