
Vaccine-Induced Seroreactivity Impacts the Accuracy of HIV Testing Algorithms in Sub-Saharan Africa: An Exploratory Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Evaluation of HIV Rapid Test Algorithms
2.3. Evaluation of HIV ELISA
2.4. Assessment of HIV Western Blot
2.5. Assessment of Anti-Env Antibody Responses
2.6. Statistical Analysis
3. Results
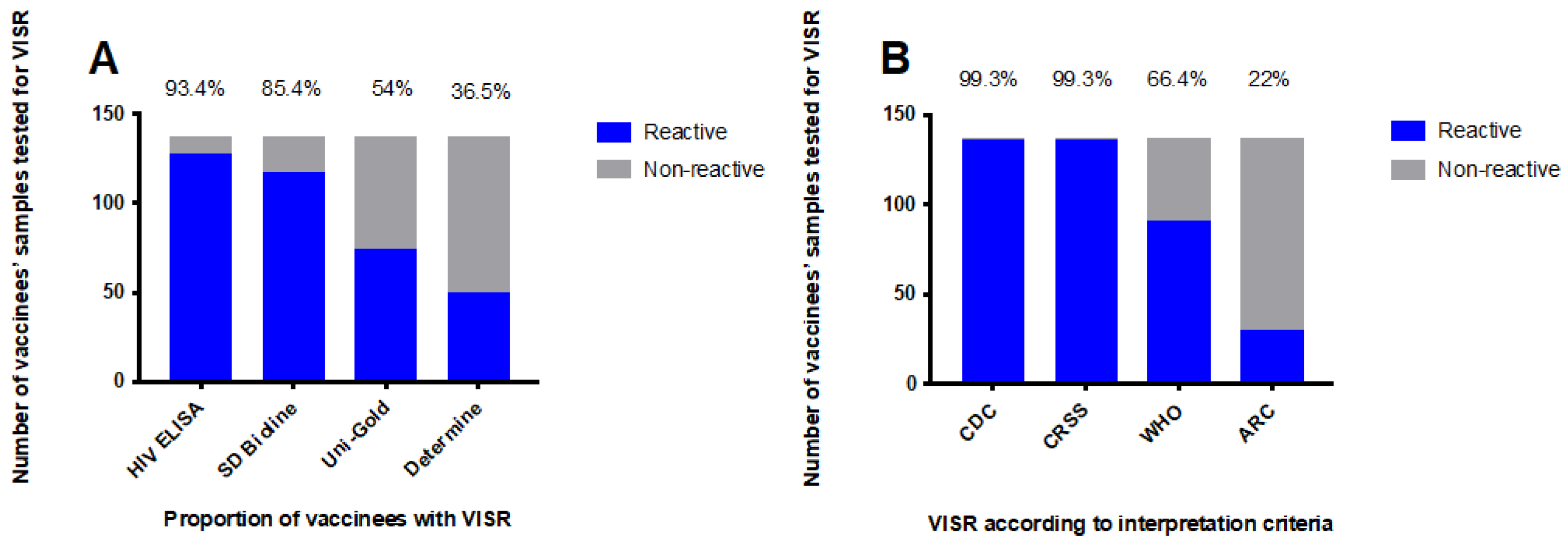
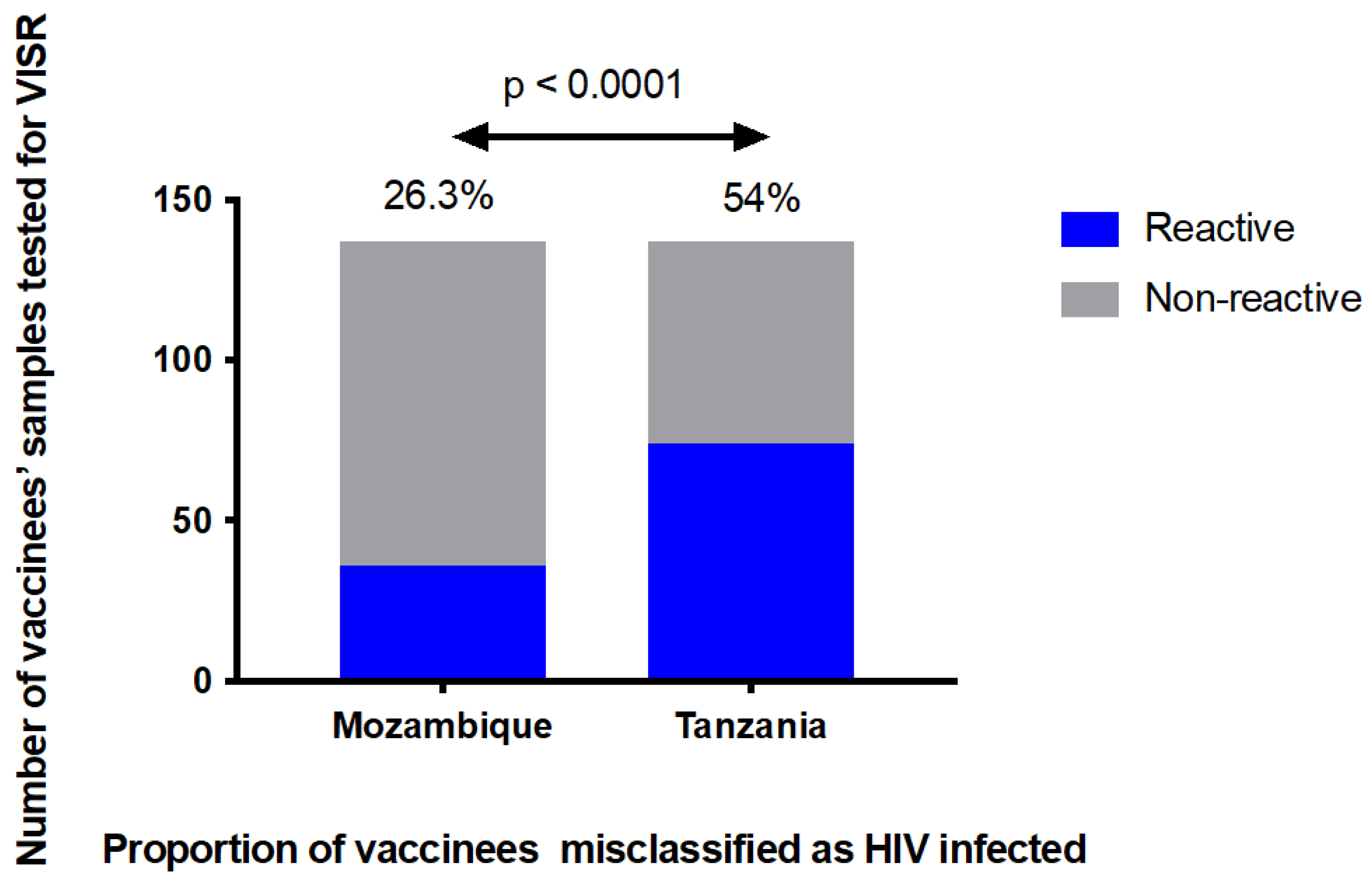
3.1. The HIV Diagnostic Algorithms Misclassified a Large Proportion of HIV-Uninfected Vaccine Recipients
3.2. Antigen Reactivity Patterns as Determined by Western Blot
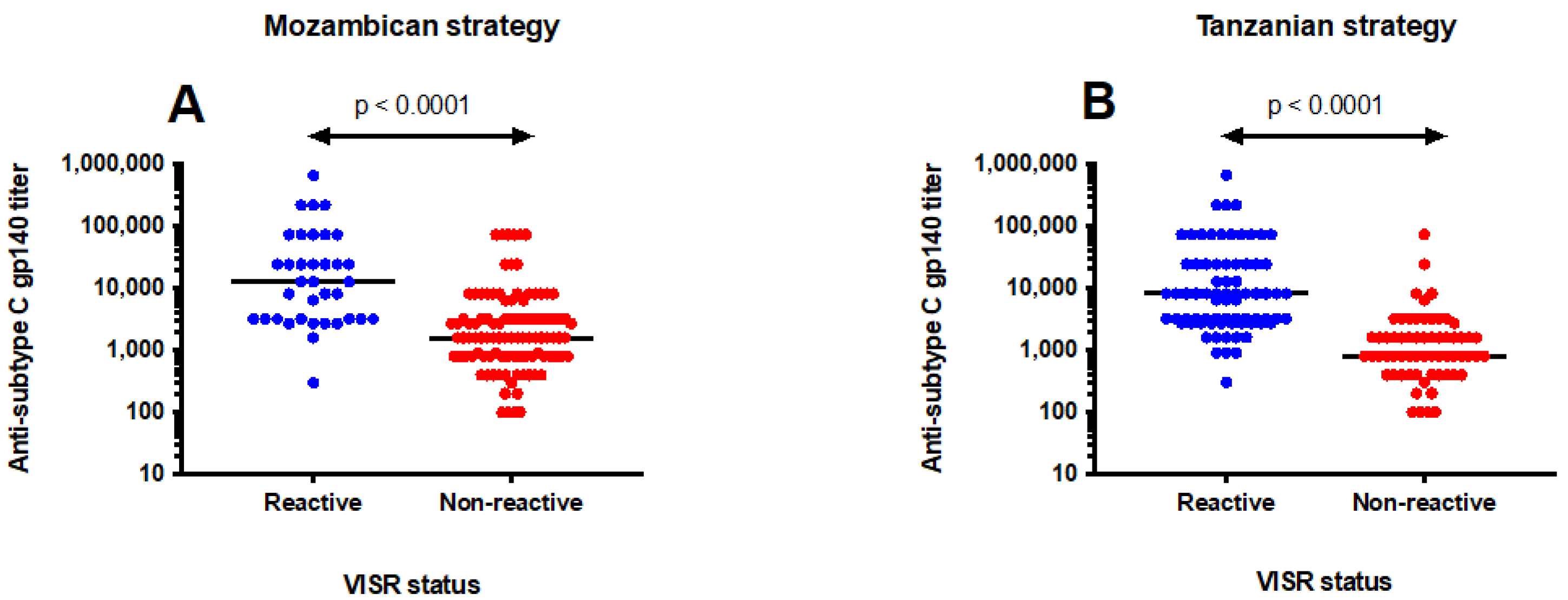
3.3. Antibody Levels Influenced Misclassification of HIV Status
3.4. Vaccinees Received Correct HIV Diagnosis Results Three Years after the Last Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV Statistics; UNAIDS: Geneva, Switzerland, 2021; Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 30 October 2021).
- Fauci, A.S. An HIV Vaccine Is Essential for Ending the HIV/AIDS Pandemic. JAMA 2017, 318, 1535–1536. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Crotty, S. HIV vaccinology: 2021 update. Semin. Immunol. 2021, 51, 101470. [Google Scholar] [CrossRef] [PubMed]
- Rerks-Ngarm, S.; Pitisuttithum, P.; Nitayaphan, S.; Kaewkungwal, J.; Chiu, J.; Paris, R.; Premsri, N.; Namwat, N.; de Souza, M.; Adams, E.; et al. Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N. Engl. J. Med. 2009, 361, 2209–2220. [Google Scholar] [CrossRef] [PubMed]
- Gray, G.E.; Bekker, L.G.; Laher, F.; Malahleha, M.; Allen, M.; Moodie, Z.; Grunenberg, N.; Huang, Y.; Grove, D.; Prigmore, B.; et al. Vaccine Efficacy of ALVAC-HIV and Bivalent Subtype C gp120-MF59 in Adults. N. Engl. J. Med. 2021, 384, 1089–1100. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J. Johnson & Johnson and Global Partners Announce Results from Phase 2b Imbokodo HIV Vaccine Clinical Trial in Young Women in Sub-Saharan Africa. 2021. Available online: https://www.prnewswire.com/news-releases/johnson--johnson-and-global-partners-announce-results-from-phase-2b-imbokodo-hiv-vaccine-clinical-trial-in-young-women-in-sub-saharan-africa-301365918.html (accessed on 27 February 2022).
- Ng’uni, T.; Chasara, C.; Ndhlovu, Z.M. Major Scientific Hurdles in HIV Vaccine Development: Historical Perspective and Future Directions. Front. Immunol. 2020, 11, 590780. [Google Scholar] [CrossRef]
- Voronin, Y.; Zinszner, H.; Karg, C.; Brooks, K.; Coombs, R.; Hural, J.; Holt, R.; Fast, P.; Allen, M.; Busch, M.; et al. HIV vaccine-induced sero-reactivity: A challenge for trial participants, researchers, and physicians. Vaccine 2015, 33, 1243–1249. [Google Scholar] [CrossRef]
- Durier, C.; Desaint, C.; Lelièvre, J.D.; Silbermann, B.; Pialoux, G.; Cuzin, L.; Bonnet, B.; Poizot-Martin, I.; Bouakane, A.; Paul, C.; et al. Long-term safety and vaccine-induced seropositivity in healthy volunteers from HIV vaccine trials. AIDS 2019, 33, 2061–2071. [Google Scholar] [CrossRef]
- Viegas, E.O.; Kroidl, A.; Munseri, P.J.; Missanga, M.; Nilsson, C.; Tembe, N.; Bauer, A.; Joachim, A.; Joseph, S.; Mann, P.; et al. Optimizing the immunogenicity of HIV prime-boost DNA-MVA-rgp140/GLA vaccines in a phase II randomized factorial trial design. PLoS ONE 2018, 13, e0206838. [Google Scholar] [CrossRef]
- Bakari, M.; Aboud, S.; Nilsson, C.; Francis, J.; Buma, D.; Moshiro, C.; Aris, E.A.; Lyamuya, E.F.; Janabi, M.; Godoy-Ramirez, K.; et al. Broad and potent immune responses to a low dose intradermal HIV-1 DNA boosted with HIV-1 recombinant MVA among healthy adults in Tanzania. Vaccine 2011, 29, 8417–8428. [Google Scholar] [CrossRef]
- Joachim, A.; Msafiri, F.; Onkar, S.; Munseri, P.; Aboud, S.; Lyamuya, E.F.; Bakari, M.; Billings, E.; Robb, M.L.; Wahren, B.; et al. Frequent and Durable Anti-HIV Envelope VIV2 IgG Responses Induced by HIV-1 DNA Priming and HIV-MVA Boosting in Healthy Tanzanian Volunteers. Vaccines 2020, 8, 681. [Google Scholar] [CrossRef]
- Nilsson, C.; Godoy-Ramirez, K.; Hejdeman, B.; Bråve, A.; Gudmundsdotter, L.; Hallengärd, D.; Currier, J.R.; Wieczorek, L.; Hasselrot, K.; Earl, P.L.; et al. Broad and potent cellular and humoral immune responses after a second late HIV-modified vaccinia virus ankara vaccination in HIV-DNA-primed and HIV-modified vaccinia virus Ankara-boosted Swedish vaccinees. AIDS Res. Hum. Retrovir. 2014, 30, 299–311. [Google Scholar] [CrossRef]
- World Health Organization. Consolidated Guidelines on HIV Testing Services 2019; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/978-92-4-155058-1 (accessed on 10 October 2021).
- Armstrong-Mensah, E.; Tetteh, A.K.; Choi, S. Utilization of Rapid Diagnostic Testing in sub-Saharan Africa: Challenges and Effects on HIV Prevention. Int. J. MCH AIDS 2021, 10, 1–6. [Google Scholar] [CrossRef]
- Kosack, C.S.; Shanks, L.; Beelaert, G.; Benson, T.; Savane, A.; Ng’ang’a, A.; Andre, B.; Zahinda, J.-P.B.; Fransen, K.; Page, A.-L. HIV misdiagnosis in sub-Saharan Africa: Performance of diagnostic algorithms at six testing sites. J. Int. AIDS Soc. 2017, 20, 21419. [Google Scholar] [CrossRef]
- Penezina, O.; Krueger, N.X.; Rodriguez-Chavez, I.R.; Busch, M.P.; Hural, J.; Kim, J.H.; O’Connell, R.J.; Hunter, E.; Aboud, S.; Higgins, K.; et al. Performance of a redesigned HIV Selectest enzyme-linked immunosorbent assay optimized to minimize vaccine-induced seropositivity in HIV vaccine trial participants. Clin. Vaccine Immunol. 2014, 21, 391–398. [Google Scholar] [CrossRef]
- Munseri, P.J.; Kroidl, A.; Nilsson, C.; Joachim, A.; Geldmacher, C.; Mann, P.; Moshiro, C.; Aboud, S.; Lyamuya, E.; Maboko, L.; et al. Priming with a simplified intradermal HIV-1 DNA vaccine regimen followed by boosting with recombinant HIV-1 MVA vaccine is safe and immunogenic: A phase IIa randomized clinical trial. PLoS ONE 2015, 10, e0119629. [Google Scholar] [CrossRef]
- Nilsson, C.; Hejdeman, B.; Godoy-Ramirez, K.; Tecleab, T.; Scarlatti, G.; Bråve, A.; Earl, P.L.; Stout, R.R.; Robb, M.L.; Shattock, R.J.; et al. HIV-DNA Given with or without Intradermal Electroporation Is Safe and Highly Immunogenic in Healthy Swedish HIV-1 DNA/MVA Vaccinees: A Phase I Randomized Trial. PLoS ONE 2015, 10, e0131748. [Google Scholar] [CrossRef]
- Viegas, E.O.; Tembe, N.; Nilsson, C.; Meggi, B.; Maueia, C.; Augusto, O.; Stout, R.; Scarlatti, G.; Ferrari, G.; Earl, P.L.; et al. Intradermal HIV-1 DNA Immunization Using Needle-Free Zetajet Injection Followed by HIV-Modified Vaccinia Virus Ankara Vaccination Is Safe and Immunogenic in Mozambican Young Adults: A Phase I Randomized Controlled Trial. AIDS Res. Hum. Retrovir. 2018, 34, 193–205. [Google Scholar] [CrossRef]
- World Health Organization. HIV Assays: Laboratory Performance and Other Operational Characteristics, Report 18; WHO: Geneva, Switzerland, 2015; Available online: https://www.who.int/diagnostics_laboratory/publications/15032_hiv_assay_report18.pdf?ua=1 (accessed on 15 September 2021).
- Masciotra, S.; McDougal, J.S.; Feldman, J.; Sprinkle, P.; Wesolowski, L.; Owen, S.M. Evaluation of an alternative HIV diagnostic algorithm using specimens from seroconversion panels and persons with established HIV infections. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2011, 52 (Suppl. S1), S17–S22. [Google Scholar] [CrossRef]
- Joachim, A.; Munseri, P.J.; Nilsson, C.; Bakari, M.; Aboud, S.; Lyamuya, E.F.; Tecleab, T.; Liakina, V.; Scarlatti, G.; Robb, M.L.; et al. Three-Year Durability of Immune Responses Induced by HIV-DNA and HIV-Modified Vaccinia Virus Ankara and Effect of a Late HIV-Modified Vaccinia Virus Ankara Boost in Tanzanian Volunteers. AIDS Res. Hum. Retrovir. 2017, 33, 880–888. [Google Scholar] [CrossRef]
- Pitisuttithum, P.; Marovich, M.A. Prophylactic HIV vaccine: Vaccine regimens in clinical trials and potential challenges. Expert Rev. Vaccines 2020, 19, 133–142. [Google Scholar] [CrossRef]
- Cooper, C.J.; Metch, B.; Dragavon, J.; Coombs, R.W.; Baden, L.R. Vaccine-induced HIV seropositivity/reactivity in noninfected HIV vaccine recipients. JAMA 2010, 304, 275–283. [Google Scholar] [CrossRef]
- Quirk, E.K.; Mogg, R.; Brown, D.D.; Lally, M.A.; Mehrotra, D.V.; DiNubile, M.J.; Robertson, M.N. HIV seroconversion without infection after receipt of adenovirus-vectored HIV type 1 vaccine. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2008, 47, 1593–1599. [Google Scholar] [CrossRef][Green Version]
- Mauk, M.; Song, J.; Bau, H.H.; Gross, R.; Bushman, F.D.; Collman, R.G.; Liu, C. Miniaturized devices for point of care molecular detection of HIV. Lab Chip 2017, 17, 382–394. [Google Scholar] [CrossRef]
- Manoto, S.L.; Lugongolo, M.; Govender, U.; Mthunzi-Kufa, P. Point of Care Diagnostics for HIV in Resource Limited Settings: An Overview. Medicina 2018, 54, 3. [Google Scholar] [CrossRef]
- Iseselo, M.K.; Tarimo, E.A.M.; Sandstrom, E.; Kulane, A. Sexual Behaviours and Practices before and after Phase I/II HIV Vaccine Trial: A Qualitative Study among Volunteers in Dar es Salaam Tanzania. Int. J. Environ. Res. Public Health 2020, 17, 7193. [Google Scholar] [CrossRef]
- Ackers, M.L.; Parekh, B.; Evans, T.G.; Berman, P.; Phillips, S.; Allen, M.; McDougal, J.S. Human immunodeficiency virus (HIV) seropositivity among uninfected HIV vaccine recipients. J. Infect. Dis. 2003, 187, 879–886. [Google Scholar] [CrossRef][Green Version]
- Silbermann, B.; Tod, M.; Desaint, C.; Pialoux, G.; Petitprez, K.; Slama, L.; Poncelet, H.; Moreau, C.; Mazarin, V.; Heshmati, F.; et al. Short communication: Long-term persistence of vaccine-induced HIV seropositivity among healthy volunteers. AIDS Res. Hum. Retrovir. 2008, 24, 1445–1448. [Google Scholar] [CrossRef]
- Kroidl, I.; Clowes, P.; Mwalongo, W.; Maganga, L.; Maboko, L.; Kroidl, A.L.; Geldmacher, C.; Machibya, H.; Hoelscher, M.; Saathoff, E. Low specificity of determine HIV1/2 RDT using whole blood in south west Tanzania. PLoS ONE 2012, 7, e39529. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Organization | HIV-Positive |
|---|---|
| CDC and Association of State and Territorial Public Health Laboratory Directors (ASTPHLD *), 1989 USA | Presence of any two of p24, gp41, gp120/160 bands |
| WHO, 1990 | Presence of two ENV bands with or without GAG or POL |
| CRSS, 1988 USA | Presence of one ENV band with p24 or p31 |
| ARC, 1988 USA | Presence of one band each of GAG, POL, and ENV |
| Diagnostic Assay | Number of Reactive/Number of Tested (%) | ||
|---|---|---|---|
| 1 Month after the Second HIV-MVA Vaccination | 16 Months after the Second HIV-MVA Vaccination | 3 Years after the Second HIV-MVA Vaccination | |
| Alere DetermineTM HIV-1/2 | 12/29 (41.4) | 11/23 (47.8) | 1/20 (5) |
| SD Bioline HIV1/2 | 26/29 (89.7) | 10/23 (43.5) | 6/20 (30) |
| Uni-GoldTM HIV-1/2 | 14/29 (48.3) | 2/23 (8.7) | 0/20 |
| HIV misdiagnosis using Mozambican algorithm | 7/29 (24.1) | 2/23 (8.7) | 0/20 |
| HIV misdiagnosis using Tanzanian algorithm | 14/29 (48.3) | 2/23 (8.7) | 0/20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Msafiri, F.; Manjate, A.; Lindroth, S.; Tembe, N.; Chissumba, R.M.; Cumbane, V.; Jani, I.; Aboud, S.; Lyamuya, E.; Andersson, S.; et al. Vaccine-Induced Seroreactivity Impacts the Accuracy of HIV Testing Algorithms in Sub-Saharan Africa: An Exploratory Study. Vaccines 2022, 10, 1062. https://doi.org/10.3390/vaccines10071062
Msafiri F, Manjate A, Lindroth S, Tembe N, Chissumba RM, Cumbane V, Jani I, Aboud S, Lyamuya E, Andersson S, et al. Vaccine-Induced Seroreactivity Impacts the Accuracy of HIV Testing Algorithms in Sub-Saharan Africa: An Exploratory Study. Vaccines. 2022; 10(7):1062. https://doi.org/10.3390/vaccines10071062
Chicago/Turabian StyleMsafiri, Frank, Alice Manjate, Sarah Lindroth, Nelson Tembe, Raquel Matavele Chissumba, Victoria Cumbane, Ilesh Jani, Said Aboud, Eligius Lyamuya, Sören Andersson, and et al. 2022. "Vaccine-Induced Seroreactivity Impacts the Accuracy of HIV Testing Algorithms in Sub-Saharan Africa: An Exploratory Study" Vaccines 10, no. 7: 1062. https://doi.org/10.3390/vaccines10071062
APA StyleMsafiri, F., Manjate, A., Lindroth, S., Tembe, N., Chissumba, R. M., Cumbane, V., Jani, I., Aboud, S., Lyamuya, E., Andersson, S., & Nilsson, C. (2022). Vaccine-Induced Seroreactivity Impacts the Accuracy of HIV Testing Algorithms in Sub-Saharan Africa: An Exploratory Study. Vaccines, 10(7), 1062. https://doi.org/10.3390/vaccines10071062