
Acceptance of and Preference for COVID-19 Vaccination in India, the United Kingdom, Germany, Italy, and Spain: An International Cross-Sectional Study

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Respondents
2.3. Data Collection
2.4. Statistical Analysis
2.5. Scenario Analysis and Simulation
3. Results
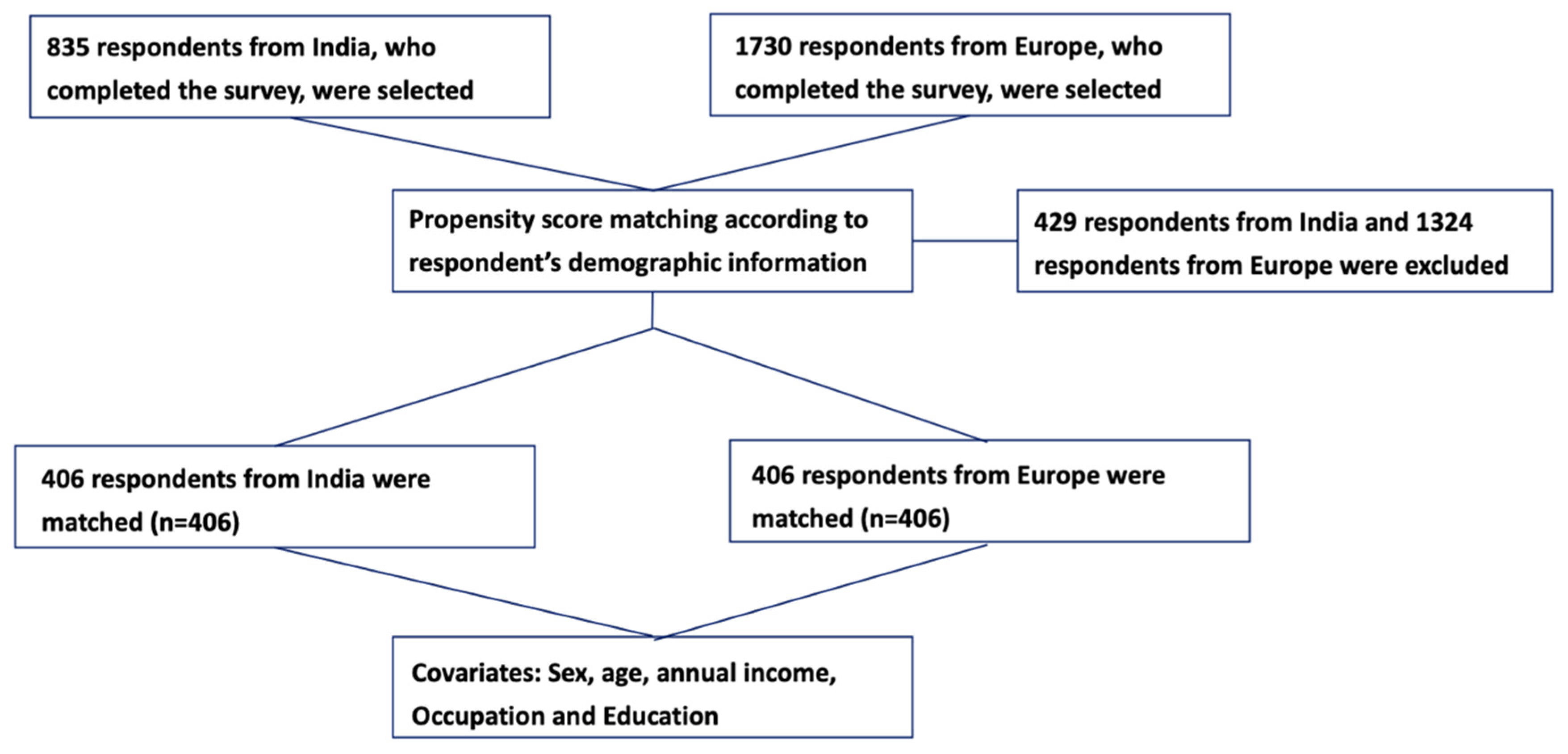
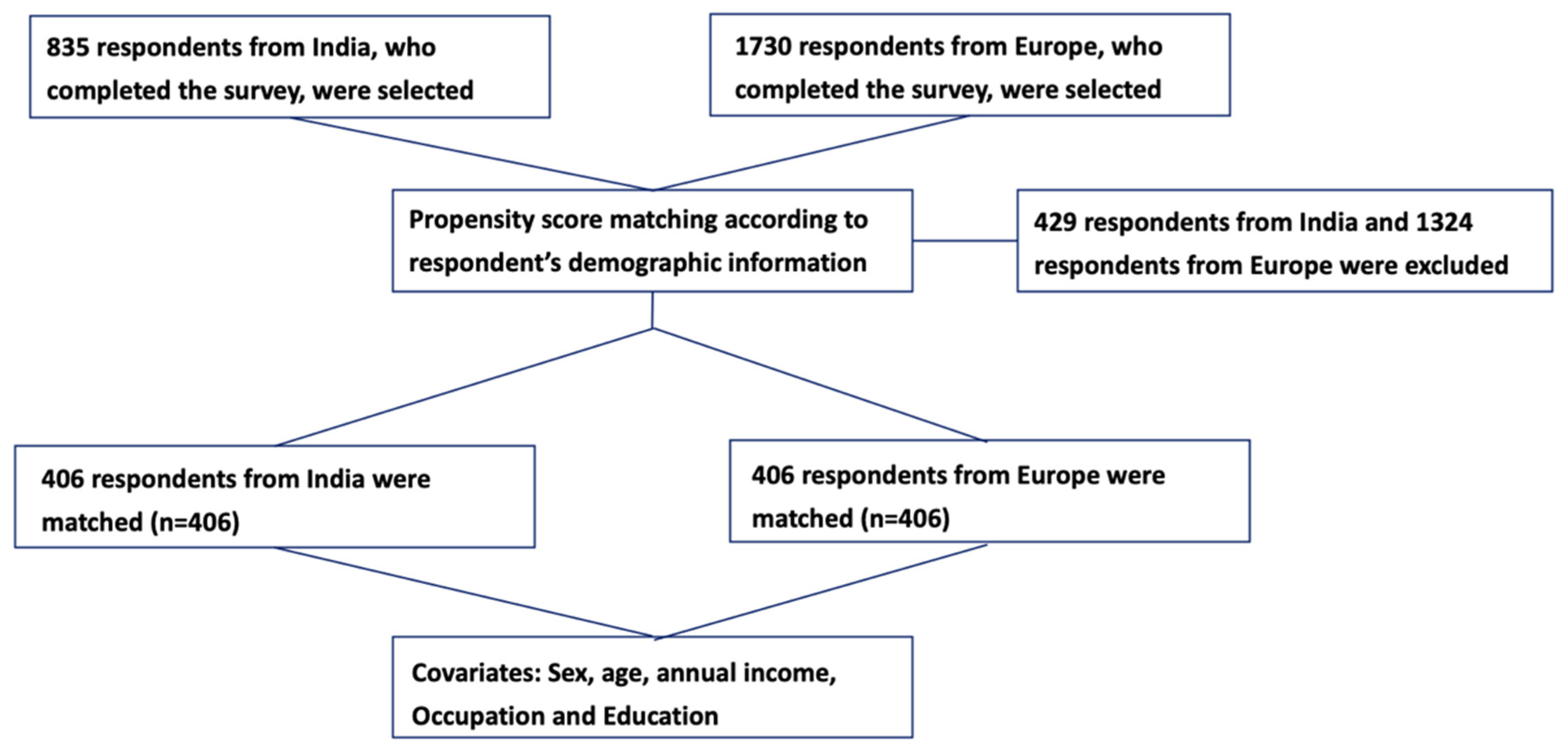
3.1. Respondents’ Characteristics
3.2. General Hesitancy and Participants’ Vaccination History
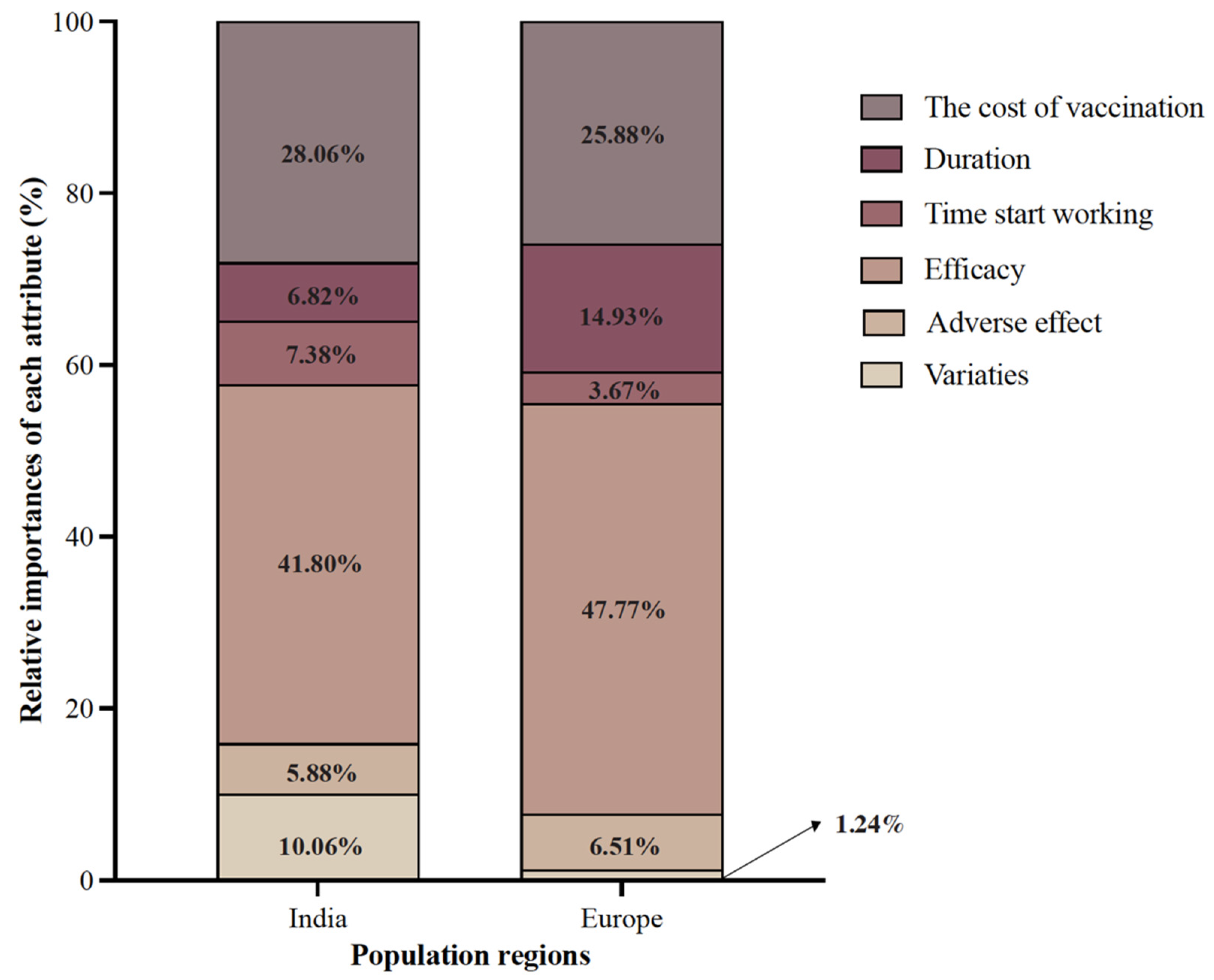
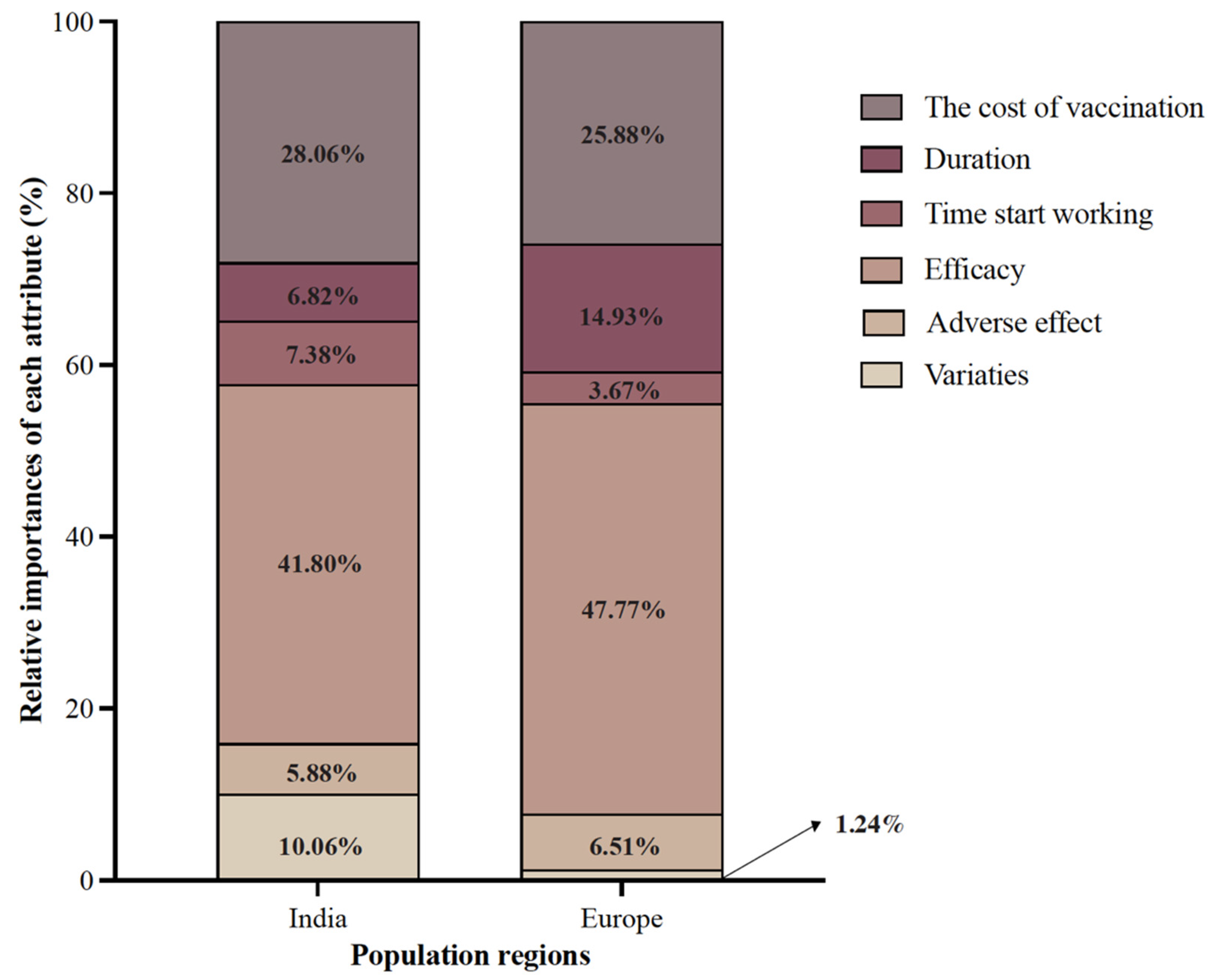
3.3. Post-PSM Vaccine Preference, Attributes, and Level Importance
3.4. Post-PSM Scenario Analysis and Uptake Likelihood Prediction
3.5. Behavioral and Psychological Results
4. Discussion
4.1. The COVID-19 Vaccination Situation in India and Europe
4.2. The Preference for Different COVID-19 Vaccines
4.3. Ensuring Fast Vaccination Is the Key
4.4. Reducing Vaccine Hesitancy
4.5. Ensuring High Efficiency and Safety
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Numbers at a Glance, Coronavirus Disease (COVID-19) Pandemic; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?gclid=CjwKCAjw-e2EBhAhEiwAJI5jg-5O2RcC1w1aEhJ9-mwuRcke3bzpef6-B_dgzyBNOQu6QgwMHffm3BoCIt0QAvD_BwE (accessed on 30 April 2021).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Alexandar, S.; Ravisankar, M.; Kumar, R.S.; Jakkan, K. A comprehensive review on COVID-19 Delta variant. Int. J. Pharmacol. Clin. Res. 2021, 5, 83–85. [Google Scholar]
- Lauring, A.S.; Malani, P.N. Variants of SARS-CoV-2. JAMA 2021, 326, 880. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. 2021. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 1 April 2022).
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing COVID-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Noronha, V.; Abraham, G.; Bondili, S.K.; Rajpurohit, A.; Menon, R.P.; Gattani, S.; Trikha, M.; Tudu, R.; Kota, K.K.; Singh, A.K.; et al. COVID-19 vaccine uptake and vaccine hesitancy in Indian patients with cancer: A questionnaire-based survey. Cancer Res. Stat. Treat. 2021, 4, 211. [Google Scholar]
- Kumar, V.M.; Pandi-Perumal, S.R.; Trakht, I.; Thyagarajan, S.P. Strategy for COVID-19 vaccination in India: The country with the second highest population and number of cases. NPJ Vaccines 2021, 6, 60. [Google Scholar] [CrossRef]
- Rackimuthu, S.; Hasan, M.M.; Bardhan, M.; Essar, M.Y. COVID-19 vaccination strategies and policies in India: The need for further re-evaluation is a pressing priority. Int. J. Health Plan. Manag. 2021, 37, 1847–1850. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Overview of the Implementation of COVID-19 Vaccination Strategies and Deployment Plans in the EU/EEA; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2022; Available online: https://www.ecdc.europa.eu/en/publications-data/overview-implementation-covid-19-vaccination-strategies-and-deployment-plans (accessed on 9 May 2022).
- World Health Organization. Draft Landscape and Tracker of COVID-19 Candidate Vaccines Net; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 14 May 2021).
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2020, 39, 247–254. [Google Scholar] [CrossRef]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- The New York Times. Tracking Coronavirus Vaccinations Around the World. The New York Times, 15 May 2021. Available online: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html(accessed on 14 May 2021).
- World Health Organization. India Situation; World Health Organization: Geneva, Switzerland, 2021. Available online: https://covid19.who.int/region/searo/country/in (accessed on 14 May 2021).
- Umakanthan, S.; Patil, S.; Subramaniam, N.; Sharma, R. COVID-19 Vaccine Hesitancy and Resistance in India Explored through a Population-Based Longitudinal Survey. Vaccines 2021, 9, 1064. [Google Scholar] [CrossRef]
- Sharma, S.; Akhtar, F.; Singh, R.K.; Mehra, S. Understanding the three As (Awareness, Access, and Acceptability) dimensions of vaccine hesitancy in Odisha, India. Clin. Epidemiol. Glob. Health 2019, 8, 399–403. [Google Scholar] [CrossRef] [Green Version]
- Sjölander-Lindqvist, A.; Larsson, S.; Fava, N.; Gillberg, N.; Marcianò, C.; Cinque, S. Communicating about COVID-19 in four Eu-ropean countries: Similarities and differences in national discourses in Germany, Italy, Spain, and Sweden. Front. Commun. 2020, 5, 97. [Google Scholar] [CrossRef]
- Pant, D.; Misra, S.; Nizami, A.-S.; Rehan, M.; Van Leeuwen, R.; Tabacchioni, S.; Goel, R.; Sarma, P.; Bakker, R.; Sharma, N.; et al. Towards the development of a biobased economy in Europe and India. Crit. Rev. Biotechnol. 2019, 39, 779–799. [Google Scholar] [CrossRef]
- Johnson, F.R.; Lancsar, E.; Marshall, D.; Kilambi, V.; Mühlbacher, A.; Regier, D.A.; Bresnahan, B.W.; Kanninen, B.; Bridges, J.F.P. Constructing experimental designs for dis-crete-choice experiments: Report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health 2013, 16, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Bridges, J.F.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.; Johnson, F.R.; Mauskopf, J. Conjoint Analysis Applications in Health—A Checklist: A Report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health 2011, 14, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.L.; Dreyer, N.; Anderson, F.; Towse, A.; Sedrakyan, A.; Normand, S.-L. Prospective observational studies to assess com-parative effectiveness: The ISPOR good research practices task force report. Value Health 2012, 15, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Randolph, J.; Falbe, K.; Manuel, A.K.; Balloun, J.L. A step-by-step guide to propensity score matching in R. Pract. Assess. Res. Eval. 2014, 19, 1–6. [Google Scholar]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc GPMoreira, E.D.; Zerbini, C. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Knoll, M.D.; Wonodi, C. Oxford–AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J. Safety and efficacy of NVX-CoV2373 COVID-19 vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- QUARTZ. India Is the Country Most Willing to Take a COVID-19 Vaccine. 2020. Available online: https://qz.com/1928206/the-countries-most-willing-to-take-a-covid-19-vaccine/ (accessed on 8 July 2021).
- Statista. Cumulative of the Coronavirus (COVID-19) Confirmed, Recovered and Deceased Numbers across India from 29 January 2020 to 10 October 2021. 2021. Available online: https://www.statista.com/statistics/1104054/india-coronavirus-covid-19-daily-confirmed-recovered-death-cases/ (accessed on 15 September 2021).
- The New York Times. Tracking Coronavirus in India: Latest Map and Case Count. The New York Times, 17 May 2021. Available online: https://www.nytimes.com/interactive/2021/world/india-covid-cases.html(accessed on 8 July 2021).
- The BBC News. India vaccination: Does it have enough doses for all adults? The BBC News, 31 December 2021. Available online: https://www.bbc.com/news/world-asia-india-55571793(accessed on 17 May 2022).
- Sharun, K.; Dhama, K. India’s role in COVID-19 vaccine diplomacy. J. Travel Med. 2021, 28, taab064. [Google Scholar] [CrossRef]
- Chakraborty, C.; Agoramoorthy, G. India’s cost-effective COVID-19 vaccine development initiatives. Vaccine 2020, 38, 7883–7884. [Google Scholar] [CrossRef]
- National Public Radio (NPR). India Is the World’s Biggest Vaccine Maker. Yet Only 4% of Indians Are Vaccinated; National Public Radio: Washington, DC, USA, 29 June 2021; Available online: https://www.npr.org/sections/goatsandsoda/2021/06/29/1011022472/india-is-the-worlds-biggest-vaccine-maker-yet-only-4-of-indians-are-vaccinated (accessed on 20 October 2021).
- The Guardian. India: Over 100 million people fail to turn up for second COVID vaccine. The Guardian, 28 October 2021. Available online: https://www.theguardian.com/world/2021/oct/28/india-over-100-million-people-fail-to-turn-up-for-second-covid-vaccine(accessed on 10 November 2021).
- The Hindu. U.S. defends restrictions on export of COVID-19 vaccine raw materials amid India’s request to lift ban. The Hindu, 23 April 2021. Available online: https://www.thehindu.com/news/international/us-defends-restrictions-on-export-of-covid-19-vaccine-raw-materials-amid-indias-request-to-lift-ban/article34391251.ece(accessed on 1 August 2021).
- Burki, T. Global COVID-19 vaccine inequity. Lancet Infect. Dis. 2021, 21, 922–923. [Google Scholar] [CrossRef]
- Brown, G.; Susskind, D. International cooperation during the COVID-19 pandemic. Oxf. Rev. Econ. Policy 2020, 36, S64–S76. [Google Scholar] [CrossRef]
- European Commision. Safe COVID-19 Vaccines for Europeans; European Commision: Brussels, Belgium, 2022; Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/safe-covid-19-vaccines-europeans_en#:~:text=On%2020%20December%20the%20European,vaccine%20authorised%20in%20the%20EU (accessed on 9 May 2022).
- Liu, T.; He, Z.; Huang, J.; Yan, N.; Chen, Q.; Huang, F.; Zhang, Y.; Akinwunmi, O.; Akinwunmi, B.; Zhang, C.; et al. A Comparison of Vaccine Hesitancy of COVID-19 Vaccination in China and the United States. Vaccines 2021, 9, 649. [Google Scholar] [CrossRef]
- Sewell, H.F.; Agius, R.M.; Kendrick, D.; Stewart, M. COVID-19 vaccines: Delivering protective immunity. BMJ 2020, 371, m4838. [Google Scholar] [CrossRef]
- Laura, M.; Julia, E.; Tiffany, L.; Brown Elizabeth, R. Vaccine optimization for Covid-19: Who to vaccinate first. Sci. Adv. 2021, 7, eabf1374. [Google Scholar]
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science 2021, 371, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Lipsitch, M.; Dean, N.E. Understanding COVID-19 vaccine efficacy. Science 2020, 370, 763–765. [Google Scholar] [CrossRef] [PubMed]
- Foy, B.H.; Wahl, B.; Mehta, K.; Shet, A.; Menon, G.I.; Britto, C. Comparing COVID-19 vaccine allocation strategies in India: A mathematical modelling study. Int. J. Infect. Dis. 2020, 103, 431–438. [Google Scholar] [CrossRef]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33, D66–D71. [Google Scholar] [CrossRef]
- Razai, M.; Chaudhry, U.; Doerholt, K.; Bauld, L.; Majeed, A. COVID-19 vaccination hesitancy. BMJ 2021, 373, n1138. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.; Moniz, M.; Gama, A.; Laires, P.; Pedro, A.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Bansal, P.; Raj, A.; Shukla, D.M.; Sunder, N. COVID-19 vaccine preferences in India. Vaccine 2022, 40, 2242–2246. [Google Scholar] [CrossRef]
- Karafillakis, E.; Van Damme, P.; Hendrickx, G.; Larson, H.J. COVID-19 in Europe: New challenges for addressing vaccine hesitancy. Lancet 2022, 399, 699–701. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Cornwall, W. Officials gird for a war on vaccine misinformation. Science 2020, 369, 14–15. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; et al. Strategies for Addressing Vaccine Hesitancy-A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieger, M.O.; Wang, M. Trust in Government Actions during the COVID-19 Crisis. Soc. Indic. Res. 2021, 159, 967–989. [Google Scholar] [CrossRef]
- Han, Q.; Zheng, B.; Cristea, M.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; Kreienkamp, J.; Leander, N.P.; Collaboration, P. Trust in government regarding COVID-19 and its associations with preventive health behaviour and prosocial behaviour during the pandemic: A cross-sectional and longitu-dinal study. Psychol. Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Eskola, J.; Duclos, P.; Schuster, M.; MacDonald, N.E. How to deal with vaccine hesitancy? Vaccine 2015, 33, 4215–4217. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Jensen-Doss, A.; Patel, Z.S.; Casline, E.; Ringle, V.A.M.; Timpano, K.R. Using Mechanical Turk to Study Parents and Children: An Examination of Data Quality and Representativeness. J. Clin. Child Adolesc. Psychol. 2021, 50, 15. [Google Scholar] [CrossRef]
- McCredie, M.N.; Morey, L.C. Who Are the Turkers? A Characterization of MTurk Workers Using the Personality Assessment Inventory. Assessment 2017, 26, 759–766. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Attributes | Attributes Description | Levels |
|---|---|---|
| Vaccine varieties | Different varieties of vaccines developed in different countries | mRNA; adenovirus vector vaccines; inactivated vaccine |
| Adverse effects | The extent of the adverse effect after getting vaccinated | very mild; mild; moderate |
| Efficacy | The efficacy of vaccines that protect the vaccinators from getting infected with COVID-19 | 55%; 65%; 75%; 85%; 95% |
| Time taken for the vaccine to start working | Time taken for the vaccine to start working after getting vaccinated | 5 days; 10 days; 15 days; 20 days |
| The duration of time that the vaccine works | Time taken from when the vaccines start working to their invalidation | 5 months; 10 months; 15 months; 20 months |
| The cost of vaccination | The cost of the whole vaccination process | USD 0; USD 50; USD 100; USD 150; USD 200 |
| Unmatched | Matched 1 | |||||
|---|---|---|---|---|---|---|
| Europe (N = 835) | India (N = 1730) | p-Value | Europe (N = 406) | India (N = 406) | p-Value | |
| Sex (%) | ||||||
| Male | 520 (62.3%) | 1209 (69.9%) | <0.001 | 245 (60.3%) | 240 (59.1%) | 0.77 |
| Female | 314 (37.6%) | 521 (30.1%) | 161 (39.7%) | 166 (40.9%) | ||
| Other | 1 (0.1%) | 0 (0.0%) | ||||
| Age groups (%), years | ||||||
| 18–25 | 213 (25.5%) | 352 (20.3%) | <0.001 | 73 (18.0%) | 78 (19.2%) | 0.46 |
| 26–30 | 181 (21.7%) | 614 (35.5%) | 130 (32.0%) | 128 (31.5%) | ||
| 31–35 | 178 (21.3%) | 427 (24.7%) | 106 (26.1%) | 98 (24.1%) | ||
| 36–40 | 109 (13.1%) | 157 (9.1%) | 53 (13.1%) | 48 (11.8%) | ||
| 41–45 | 77 (9.2%) | 86 (5.0%) | 33 (8.1%) | 31 (7.6%) | ||
| 46–50 | 41 (4.9%) | 46 (2.7%) | 6 (1.5%) | 7 (1.7%) | ||
| 51–55 | 14 (1.7%) | 23 (1.3%) | 4 (1.0%) | 8 (2.0%) | ||
| 56–60 | 13 (1.6%) | 11 (0.6%) | 1 (0.2%) | 7 (1.7%) | ||
| Above 60 | 9 (1.1%) | 14 (0.8%) | 0 (0.0%) | 1 (0.2%) | ||
| Highest educational level (%) | ||||||
| Pre-primary education or primary school education | 4 (0.5%) | 2 (0.1%) | <0.001 | 16 (3.9%) | 16 (3.9%) | 0.58 |
| Middle school education | 13 (1.6%) | 8 (0.5%) | 14 (3.4%) | 9 (2.2%) | ||
| High school education | 216 (25.9%) | 34 (2.0%) | 233 (57.4%) | 225 (55.4%) | ||
| Vocational school education | 58 (6.9%) | 47 (2.7%) | 142 (35.0%) | 156 (38.4%) | ||
| Bachelor’s degree | 328 (39.3%) | 1105 (63.9%) | 1 (0.2%) | 0 (0.0%) | ||
| Master’s degree | 201 (24.1%) | 529 (30.6%) | ||||
| PhD degree | 15 (1.8%) | 5 (0.3%) | ||||
| Occupation (%) | ||||||
| Students | 197 (23.6%) | 48 (2.8%) | <0.001 | 70 (17.2%) | 16 (3.9%) | <0.001 |
| Managers | 89 (10.7%) | 360 (20.8%) | 32 (7.9%) | 97 (23.9%) | ||
| Professionals | 240 (28.7%) | 549 (31.7%) | 148 (36.5%) | 115 (28.3%) | ||
| Technicians and associate professionals | 83 (9.9%) | 348 (20.1%) | 45 (11.1%) | 83 (20.4%) | ||
| Clerical support workers | 30 (3.6%) | 94 (5.4%) | 12 (3.0%) | 16 (3.9%) | ||
| Service and sales workers | 82 (9.8%) | 159 (9.2%) | 48 (11.8%) | 36 (8.9%) | ||
| Skilled agricultural, forestry and fishery workers | 8 (1.0%) | 41 (2.4%) | 2 (0.5%) | 14 (3.4%) | ||
| Craft and related trade workers | 14 (1.7%) | 17 (1.0%) | 7 (1.7%) | 2 (0.5%) | ||
| Plant and machine operators and assemblers | 8 (1.0%) | 11 (0.6%) | 5 (1.2%) | 2 (0.5%) | ||
| Elementary occupations | 17 (2.0%) | 19 (1.1%) | 10 (2.5%) | 4 (1.0%) | ||
| Armed forces occupations | 7 (0.8%) | 1 (0.1%) | 2 (0.5%) | 0 (0.0%) | ||
| Other | 60 (7.2%) | 83 (4.8%) | 25 (6.2%) | 21 (5.2%) | ||
| Annual income (%) | ||||||
| Under USD 10,000 | 173 (22.4%) | 533 (31.1%) | <0.001 | 100 (24.6%) | 100 (24.6%) | 0.99 |
| USD 10,001–20,000 | 173 (22.4%) | 343 (20.0%) | 101 (24.9%) | 96 (23.6%) | ||
| USD 20,001–30,000 | 136 (17.6%) | 254 (14.8%) | 64 (15.8%) | 64 (15.8%) | ||
| USD 30,001–40,000 | 121 (15.6%) | 162 (9.5%) | 67 (16.5%) | 67 (16.5%) | ||
| USD 40,001–50,000 | 72 (9.3%) | 147 (8.6%) | 40 (9.9%) | 40 (9.9%) | ||
| USD 50,001–60,000 | 39 (5.0%) | 133 (7.8%) | 19 (4.7%) | 19 (4.7%) | ||
| USD 60,001–70,000 | 19 (2.5%) | 114 (6.7%) | 9 (2.2%) | 14 (3.4%) | ||
| Above USD 70,000 | 41 (5.3%) | 26 (1.5%) | 6 (1.5%) | 6 (1.5%) | ||
| Acceptance of vaccination 2, mean (SD) | 7.8 (2.9) | 7.4 (2.6) | 0.001 | 7.7 (2.9) | 7.4 (2.5) | 0.054 |
| Acceptance of vaccination under social cues 2, mean (SD) | 7.7 (2.8) | 7.5 (2.5) | 0.14 | 7.6 (2.8) | 7.4 (2.4) | 0.27 |
| Self ever infected with COVID-19 (%) | ||||||
| Yes | 131 (15.7%) | 556 (32.1%) | <0.001 | 68 (16.7%) | 131 (32.3%) | <0.001 |
| No | 699 (83.7%) | 1157 (66.9%) | 336 (82.8%) | 271 (66.7%) | ||
| Not to answer | 5 (0.6%) | 17 (1.0%) | 2 (0.5%) | 4 (1.0%) | ||
| Friend family or community ever infected (%) | ||||||
| Yes | 660 (79.0%) | 1274 (73.6%) | 0.005 | 327 (80.5%) | 317 (78.1%) | 0.68 |
| No | 168 (20.1%) | 447 (25.8%) | 76 (18.7%) | 86 (21.2%) | ||
| Not to answer | 7 (0.8%) | 9 (0.5%) | 3 (0.7%) | 3 (0.7%) | ||
| Marital status (%) | ||||||
| Single | 380 (45.5%) | 550 (31.8%) | <0.001 | 177 (43.6%) | 118 (29.1%) | <0.001 |
| Married | 334 (40.0%) | 1165 (67.3%) | 170 (41.9%) | 283 (69.7%) | ||
| Divorced | 20 (2.4%) | 8 (0.5%) | 9 (2.2%) | 2 (0.5%) | ||
| Other | 95 (11.4%) | 2 (0.1%) | 47 (11.6%) | 1 (0.2%) | ||
| Not to answer | 6 (0.7%) | 5 (0.3%) | 3 (0.7%) | 2 (0.5%) | ||
| Source of information for COVID-19 vaccines (%) | ||||||
| Healthcare provider | 347 (41.6%) | 790 (45.7%) | 0.050 | 178 (43.8%) | 185 (45.6%) | 0.62 |
| CDC or public health department | 247 (29.6%) | 466 (26.9%) | 0.16 | 105 (25.9%) | 114 (28.1%) | 0.48 |
| News reports | 622 (74.5%) | 1127 (65.1%) | <0.001 | 295 (72.7%) | 266 (65.5%) | 0.028 |
| Social media | 364 (43.6%) | 1141 (66.0%) | <0.001 | 176 (43.3%) | 256 (63.1%) | <0.001 |
| Friends or family members | 280 (33.5%) | 856 (49.5%) | <0.001 | 143 (35.2%) | 184 (45.3%) | 0.003 |
| Employers | 59 (7.1%) | 285 (16.5%) | <0.001 | 33 (8.1%) | 55 (13.5%) | 0.013 |
| Pharmaceutical company advertisement | 25 (3.0%) | 120 (6.9%) | <0.001 | 7 (1.7%) | 27 (6.7%) | <0.001 |
| Other | 25 (3.0%) | 3 (0.2%) | <0.001 | 9 (2.2%) | 0 (0.0%) | 0.003 |
| Comparison between India and Europe in Attributes Levels Utility and Odds Ratios | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| India (N = 406) | Europe (N = 406) | ||||||||||
| Attributes | Variable | Coefficient | Std. Error | OR | 95% CI | p-Value | Coefficient | Std. Error | OR | 95% CI | p-Value |
| Varieties | mRNA | Reference 1 | |||||||||
| Adenovirus vector vaccines | 0.080 | 0.028 | 1.058 | 1.000–1.118 | 0.005 | −0.007 | 0.023 | 0.967 | 0.924–1.011 | 0.756 | |
| Inactivated vaccine | −0.103 | 0.029 | 0.881 | 0.833–0.932 | 0.000 | −0.020 | 0.023 | 0.955 | 0.913–0.998 | 0.390 | |
| Adverse effect | very mild | Reference | |||||||||
| mild | 0.055 | 0.029 | 1.061 | 1.002–1.122 | 0.056 | 0.052 | 0.023 | 0.957 | 0.915–1.002 | 0.024 | |
| moderate | −0.052 | 0.029 | 0.953 | 0.901–1.008 | 0.073 | −0.15 | 0.023 | 0.783 | 0.748–0.819 | 0.000 | |
| Efficacy | 55% | Reference | |||||||||
| 65% | −0.211 | 0.041 | 1.142 | 1.055–1.237 | 0.000 | −0.55 | 0.034 | 1.407 | 1.317–1.503 | 0.000 | |
| 75% | −0.042 | 0.046 | 1.353 | 1.237–1.480 | 0.363 | 0.075 | 0.035 | 2.622 | 2.449–2.807 | 0.032 | |
| 85% | 0.181 | 0.040 | 1.690 | 1.562–1.827 | 0.000 | 0.456 | 0.031 | 3.837 | 3.612–4.077 | 0.000 | |
| 95% | 0.415 | 0.044 | 2.137 | 1.961–2.328 | 0.000 | 0.906 | 0.034 | 6.023 | 5.632–6.443 | 0.000 | |
| Time for the vaccine to start working | 5 days | Reference | |||||||||
| 10 days | 0.020 | 0.035 | 0.958 | 0.894–1.027 | 0.578 | −0.071 | 0.028 | 0.871 | 0.824–0.921 | 0.013 | |
| 15 days | −0.011 | 0.035 | 0.929 | 0.868–0.996 | 0.761 | 0.022 | 0.028 | 0.956 | 0.906–1.009 | 0.428 | |
| 20 days | −0.071 | 0.039 | 0.875 | 0.810–0.944 | 0.067 | −0.018 | 0.031 | 0.919 | 0.865–0.976 | 0.563 | |
| The duration of vaccine effectiveness | 5 months | Reference | |||||||||
| 10 months | −0.075 | 0.036 | 0.935 | 0.872–1.003 | 0.037 | −0.089 | 0.028 | 1.275 | 1.206–1.348 | 0.002 | |
| 15 months | 0.049 | 0.037 | 1.059 | 0.984–1.139 | 0.185 | 0.193 | 0.029 | 1.692 | 1.598–1.791 | 0.000 | |
| 20 months | 0.033 | 0.036 | 1.041 | 0.970–1.118 | 0.362 | 0.229 | 0.028 | 1.753 | 1.658–1.852 | 0.000 | |
| The cost of vaccination | USD 0 | Reference | |||||||||
| USD 50 | 0.150 | 0.041 | 0.892 | 0.824–0.966 | 0.000 | 0.192 | 0.032 | 0.674 | 0.633–0.717 | 0.000 | |
| USD 100 | −0.040 | 0.039 | 0.738 | 0.684–0.796 | 0.308 | −0.147 | 0.031 | 0.480 | 0.452–0.510 | 0.000 | |
| USD 150 | −0.130 | 0.043 | 0.674 | 0.619–0.734 | 0.003 | −0.246 | 0.034 | 0.435 | 0.406–0.465 | 0.000 | |
| USD 200 | −0.245 | 0.046 | 0.601 | 0.549–0.658 | 0.000 | −0.386 | 0.037 | 0.378 | 0.351–0.407 | 0.000 | |
| Share of Preference | Base Scenario | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 | Scenario 6 | Scenario 7 | Scenario 8 |
|---|---|---|---|---|---|---|---|---|---|
| INDIA | |||||||||
| Inactivated vaccine | Adenovirus vector vaccines | mRNA | mRNA | Inactivated vaccine | Adenovirus vector vaccines | Adenovirus vector vaccines | Adenovirus vector vaccines | mRNA |
| moderate | very mild | moderate | mild | very mild | mild | very mild | very mild | very mild |
| 55% | 75% | 95% | 95% | 75% | 95% | 65% | 75% | 95% |
| 20 days | 20 days | 20 days | 20 days | 10 days | 20 days | 5 days | 5 days | 5 days |
| 5 months | 5 months | 5 months | 5 months | 5 months | 5 months | 5 months | 5 months | 20 months |
| USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 |
| 3.5% | 4.0% | 13.5% | 13.3% | 3.8% | 16.1% | 7.7% | 7.3% | 30.9% |
| EUROPE | |||||||||
| Adenovirus vector vaccines | Adenovirus vector vaccines | mRNA | mRNA | Inactivated vaccine | Adenovirus vector vaccines | Adenovirus vector vaccines | Adenovirus vector vaccines | Adenovirus vector vaccines |
| moderate | very mild | moderate | mild | very mild | mild | very mild | very mild | very mild |
| 55% | 75% | 95% | 95% | 75% | 95% | 65% | 75% | 95% |
| 20 days | 20 days | 20 days | 20 days | 10 days | 20 days | 5 days | 5 days | 5 days |
| 5 months | 5 months | 5 months | 5 months | 5 months | 5 months | 5 months | 5 months | 20 months |
| USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 | USD 50 |
| 0.7% | 1.5% | 8.1% | 7.1% | 3.1% | 5.1% | 1.8% | 2.5% | 70.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, Y.; He, Z.; Liu, T.; Huang, J.; Zhang, C.J.P.; Akinwunmi, B.; Ming, W.-k. Acceptance of and Preference for COVID-19 Vaccination in India, the United Kingdom, Germany, Italy, and Spain: An International Cross-Sectional Study. Vaccines 2022, 10, 832. https://doi.org/10.3390/vaccines10060832
Dong Y, He Z, Liu T, Huang J, Zhang CJP, Akinwunmi B, Ming W-k. Acceptance of and Preference for COVID-19 Vaccination in India, the United Kingdom, Germany, Italy, and Spain: An International Cross-Sectional Study. Vaccines. 2022; 10(6):832. https://doi.org/10.3390/vaccines10060832
Chicago/Turabian StyleDong, Yanqi, Zonglin He, Taoran Liu, Jian Huang, Casper J. P. Zhang, Babatunde Akinwunmi, and Wai-kit Ming. 2022. "Acceptance of and Preference for COVID-19 Vaccination in India, the United Kingdom, Germany, Italy, and Spain: An International Cross-Sectional Study" Vaccines 10, no. 6: 832. https://doi.org/10.3390/vaccines10060832
APA StyleDong, Y., He, Z., Liu, T., Huang, J., Zhang, C. J. P., Akinwunmi, B., & Ming, W.-k. (2022). Acceptance of and Preference for COVID-19 Vaccination in India, the United Kingdom, Germany, Italy, and Spain: An International Cross-Sectional Study. Vaccines, 10(6), 832. https://doi.org/10.3390/vaccines10060832