
Adverse Mentions, Negative Sentiment, and Emotions in COVID-19 Vaccine Tweets and Their Association with Vaccination Uptake: Global Comparison of 192 Countries


Abstract
:1. Introduction
Objectives
2. Method
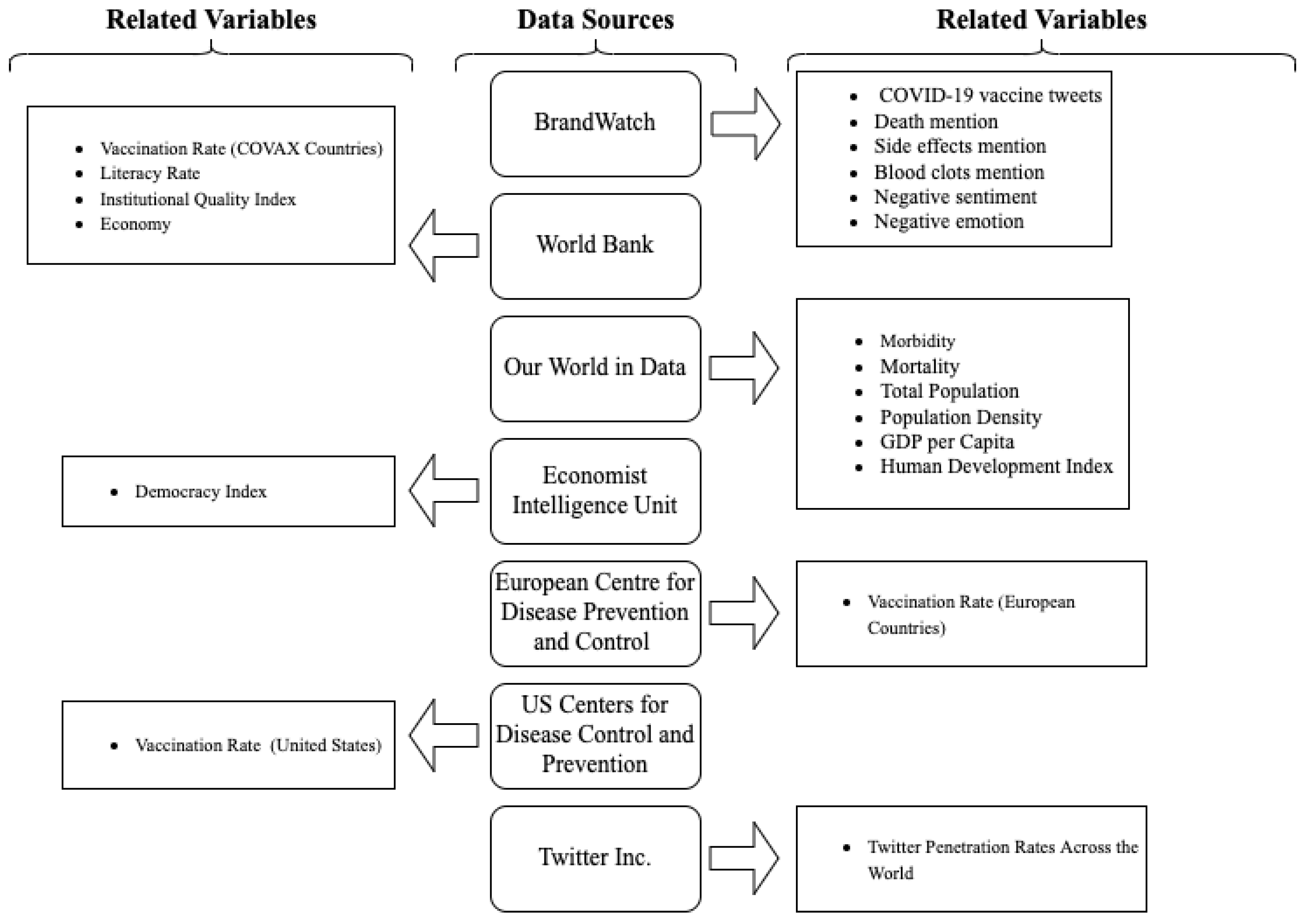
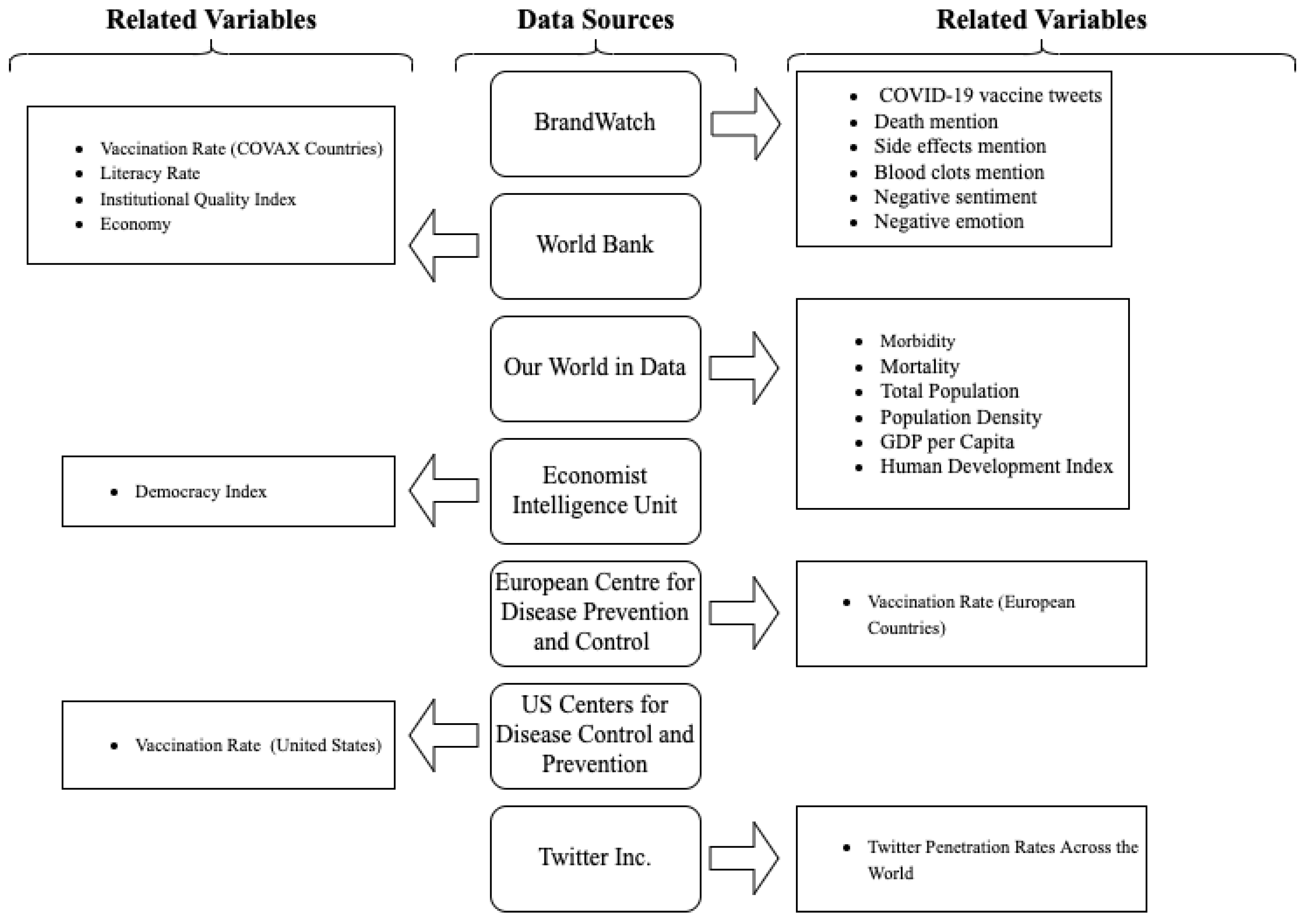
2.1. Data Collection
2.2. Measures
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Basta, N.; Moodie, E. COVID-19 Vaccine Development and Approvals Tracker. 2022. Available online: https://covid19.trackvaccines.org/agency/who (accessed on 21 March 2022).
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Our World Data. 2022. Available online: https://ourworldindata.org/coronavirus (accessed on 21 March 2022).
- WHO. Achieving 70% COVID-19 Immunization Coverage by Mid-2022. Available online: https://www.who.int/news/item/23-12-2021-achieving-70-covid-19-immunization-coverage-by-mid-2022 (accessed on 13 March 2022).
- Cohen, J.; Kupferschmidt, K. Countries Now Scrambling for COVID-19 Vaccines May Soon Have Surpluses to Donate. Sci. Mag. 2021. [Google Scholar] [CrossRef]
- WHO. Vaccine Equity. Available online: https://www.who.int/campaigns/vaccine-equity (accessed on 13 March 2022).
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A Global Database of COVID-19 Vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Rief, W. Fear of Adverse Effects and COVID-19 Vaccine Hesitancy: Recommendations of the Treatment Expectation Expert Group. JAMA Health Forum 2021, 2, e210804. [Google Scholar] [CrossRef]
- Mitchell, A.; Liedke, J. About Four-in-Ten Americans Say Social Media Is an Important Way of Following COVID-19 Vaccine News. Pew Res. Cent. 2021. Available online: https://www.pewresearch.org/fact-tank/2021/08/24/about-four-in-ten-americans-say-social-media-is-an-important-way-of-following-covid-19-vaccine-news (accessed on 21 March 2022).
- Muric, G.; Wu, Y.; Ferrara, E. COVID-19 Vaccine Hesitancy on Social Media: Building a Public Twitter Data Set of Antivaccine Content, Vaccine Misinformation, and Conspiracies. JMIR Public Health Surveill. 2021, 7, e30642. [Google Scholar] [CrossRef]
- Yousefinaghani, S.; Dara, R.; Mubareka, S.; Papadopoulos, A.; Sharif, S. An Analysis of COVID-19 Vaccine Sentiments and Opinions on Twitter. Int. J. Infect. Dis. 2021, 108, 256–262. [Google Scholar] [CrossRef]
- Alshareef, N.; Yunusa, I.; Al-Hanawi, M.K. The Influence of COVID-19 Information Sources on the Attitudes and Practices Toward COVID-19 Among the General Public of Saudi Arabia: Cross-Sectional Online Survey Study. JMIR Public Health Surveill. 2021, 7, e28888. [Google Scholar] [CrossRef]
- Melki, J.; Tamim, H.; Hadid, D.; Makki, M.; El Amine, J.; Hitti, E. Mitigating Infodemics: The Relationship between News Exposure and Trust and Belief in COVID-19 Fake News and Social Media Spreading. PLoS ONE 2021, 16, e0252830. [Google Scholar] [CrossRef]
- Lee, J.J.; Kang, K.-A.; Wang, M.P.; Zhao, S.Z.; Wong, J.Y.H.; O’Connor, S.; Yang, S.C.; Shin, S. Associations Between COVID-19 Misinformation Exposure and Belief With COVID-19 Knowledge and Preventive Behaviors: Cross-Sectional Online Study. J. Med. Internet Res. 2020, 22, e22205. [Google Scholar] [CrossRef]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Ophir, Y.; Walter, D.; Arnon, D.; Lokmanoglu, A.; Tizzoni, M.; Carota, J.; D’Antiga, L.; Nicastro, E. The Framing of COVID-19 in Italian Media and Its Relationship with Community Mobility: A Mixed-Method Approach. J. Health Commun. 2021, 26, 161–173. [Google Scholar] [CrossRef]
- Christakis, N.A.; Fowler, J.H. Social Contagion Theory: Examining Dynamic Social Networks and Human Behavior. Stat. Med. 2013, 32, 556–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouzy, R.; Abi Jaoude, J.; Kraitem, A.; El Alam, M.B.; Karam, B.; Adib, E.; Zarka, J.; Traboulsi, C.; Akl, E.W.; Baddour, K. Coronavirus Goes Viral: Quantifying the COVID-19 Misinformation Epidemic on Twitter. Cureus 2020, 12, e7255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobato, E.J.C.; Powell, M.; Padilla, L.M.K.; Holbrook, C. Factors Predicting Willingness to Share COVID-19 Misinformation. Front. Psychol. 2020, 11, 566108. [Google Scholar] [CrossRef]
- Karami, A.; Zhu, M.; Goldschmidt, B.; Boyajieff, H.R.; Najafabadi, M.M. COVID-19 Vaccine and Social Media in the U.S.: Exploring Emotions and Discussions on Twitter. Vaccines 2021, 9, 1059. [Google Scholar] [CrossRef] [PubMed]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First Month of COVID-19 Vaccine Safety Monitoring—United States, 14 December 2020–13 January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef]
- Neale, T. Reports of Sudden Deaths among Athletes After COVID-19 Vax Are ‘Misinformation.’ tctMD 2022. Available online: https://www.tctmd.com/news/reports-sudden-deaths-among-athletes-after-covid-19-vax-are-misinformation (accessed on 1 April 2022).
- Bond, S. Facebook’s Most Viewed Article In Early 2021 Raised Doubt About COVID Vaccine. NPR. 2021. Available online: https://www.npr.org/2021/08/21/1030038616/facebooks-most-viewed-article-in-early-2021-raised-doubt-about-covid-vaccine (accessed on 1 April 2022).
- US FDA. FDA and CDC Lift Recommended Pause on Johnson & Johnson (Janssen) COVID-19 Vaccine Use Following Thorough Safety Review. Available online: https://www.fda.gov/news-events/press-announcements/fda-and-cdc-lift-recommended-pause-johnson-johnson-janssen-covid-19-vaccine-use-following-thorough (accessed on 9 April 2022).
- Baker, A.T.; Boyd, R.J.; Sarkar, D.; Teijeira-Crespo, A.; Chan, C.K.; Bates, E.; Waraich, K.; Vant, J.; Wilson, E.; Truong, C.D.; et al. ChAdOx1 Interacts with CAR and PF4 with Implications for Thrombosis with Thrombocytopenia Syndrome. Sci. Adv. 2021, 7, eabl8213. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J. Covid: Trigger of Rare Blood Clots with AstraZeneca Jab Found by Scientists. BBC News, 2 December 2021. Available online: https://www.bbc.com/news/health-59418123(accessed on 1 April 2022).
- Jemielniak, D.; Krempovych, Y. An Analysis of AstraZeneca COVID-19 Vaccine Misinformation and Fear Mongering on Twitter. Public Health 2021, 200, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, R.; Mehta, V.; Valkunde, T.; Moustakas, E. Topics, Trends, and Sentiments of Tweets About the COVID-19 Pandemic: Temporal Infoveillance Study. J. Med. Internet Res. 2020, 22, e22624. [Google Scholar] [CrossRef]
- Hung, M.; Lauren, E.; Hon, E.S.; Birmingham, W.C.; Xu, J.; Su, S.; Hon, S.D.; Park, J.; Dang, P.; Lipsky, M.S. Social Network Analysis of COVID-19 Sentiments: Application of Artificial Intelligence. J. Med. Internet Res. 2020, 22, e22590. [Google Scholar] [CrossRef]
- Liu, S.; Liu, J. Public Attitudes toward COVID-19 Vaccines on English-Language Twitter: A Sentiment Analysis. Vaccine 2021, 39, 5499–5505. [Google Scholar] [CrossRef]
- Betsch, C.; Ulshöfer, C.; Renkewitz, F.; Betsch, T. The Influence of Narrative v. Statistical Information on Perceiving Vaccination Risks. Med. Decis. Making 2011, 31, 742–753. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 Vaccine Hesitancy and Related Fears and Anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Chen, J.; Hu, R.; Chen, C.; Zheng, C.; Su, Y.; Zhu, T. Twitter Discussions and Emotions About the COVID-19 Pandemic: Machine Learning Approach. J. Med. Internet Res. 2020, 22, e20550. [Google Scholar] [CrossRef] [PubMed]
- Xi, H.; Zhang, C.; Zhao, Y.; He, S. Public Emotional Diffusion over COVID-19 Related Tweets Posted by Major Public Health Agencies in the United States. Data Intell. 2022, 4, 66–87. [Google Scholar] [CrossRef]
- United Nations Member States. Available online: https://www.un.org/en/about-us/member-states (accessed on 21 March 2022).
- Twitter About Eligibility for Twitter. Ads. Available online: https://business.twitter.com/en/help/ads-policies/campaign-considerations/about-eligibility-for-twitter-ads.html (accessed on 21 March 2022).
- DigitalReportal. Digital 2021 October Global Statshot Report. Available online: https://datareportal.com/reports/digital-2021-october-global-statshot (accessed on 21 March 2022).
- Liu, B. Sentiment Analysis and Opinion Mining. Synth. Lect. Hum. Lang. Technol. 2012, 5, 1–167. [Google Scholar] [CrossRef] [Green Version]
- Bannister, K. Understanding Sentiment Analysis: What It Is & Why It’s Used. Available online: https://www.brandwatch.com/blog/understanding-sentiment-analysis/ (accessed on 1 April 2022).
- Taylor, N. The Data Science Behind Brandwatch’s New Sentiment Analysis. Available online: https://www.brandwatch.com/blog/data-science-behind-brandwatchs-new-sentiment-analysis/ (accessed on 11 April 2022).
- Taylor, N. Get a Deeper Understanding of Consumer Sentiment with Emotion Analysis. Available online: https://www.brandwatch.com/blog/get-a-deeper-understanding-of-consumer-sentiment-with-emotion-analysis/ (accessed on 11 April 2022).
- World Bank. The World Bank|COVID-19 Vaccine Deployment Tracker. Available online: https://covid19vaccinedeploymenttracker.worldbank.org/tracker (accessed on 21 March 2022).
- European Centre for Disease Prevention and Control Sources—Worldwide Data on COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/sources-worldwide-data-covid-19 (accessed on 21 March 2022).
- CDC. COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 21 March 2022).
- The Economist. Intelligence Unit Democracy Index 2020. Available online: https://www.eiu.com/n/campaigns/democracy-index-2020/ (accessed on 21 March 2022).
- de Oliveira, B.R.B.; da Penha Sobral, A.I.G.; Marinho, M.L.M.; Sobral, M.F.F.; de Souza Melo, A.; Duarte, G.B. Determinants of Access to the SARS-CoV-2 Vaccine: A Preliminary Approach. Int. J. Equity Health 2021, 20, 183. [Google Scholar] [CrossRef]
- Roser, M.; Ortiz-Ospina, E. Literacy. Our World Data. 2016. Available online: https://ourworldindata.org/literacy (accessed on 21 March 2022).
- Kaufmann, D.; Kraay, A. WGI-Home. Available online: http://info.worldbank.org/governance/wgi/ (accessed on 21 March 2022).
- WHO. Infodemic. Available online: https://www.who.int/health-topics/infodemic (accessed on 9 April 2022).
- United Nations. Cross-Regional Statement on “Infodemic” in the Context of COVID-19. Available online: https://onu.delegfrance.org/IMG/pdf/cross-regional_statement_on_infodemic_final_with_all_endorsements.pdf (accessed on 9 April 2022).
- Walter, N.; Brooks, J.J.; Saucier, C.J.; Suresh, S. Evaluating the Impact of Attempts to Correct Health Misinformation on Social Media: A Meta-Analysis. Health Commun. 2021, 36, 1776–1784. [Google Scholar] [CrossRef]
- Chou, W.-Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Scheuch, E.K. Cross-National Comparisons Using Aggregated Data: Some Substantive and Methodological Problems. In Comparing Nations: The Use of Quantitative Data in Cross-National Research; Yale University: New Haven, CT, USA, 1966; pp. 131–167. ISBN 978-0-300-00767-1. [Google Scholar]
- Imran, A.S.; Daudpota, S.M.; Kastrati, Z.; Batra, R. Cross-Cultural Polarity and Emotion Detection Using Sentiment Analysis and Deep Learning on COVID-19 Related Tweets. IEEE Access 2020, 8, 181074–181090. [Google Scholar] [CrossRef]
- Hayes, J.L.; Britt, B.C.; Evans, W.; Rush, S.W.; Towery, N.A.; Adamson, A.C. Can Social Media Listening Platforms’ Artificial Intelligence Be Trusted? Examining the Accuracy of Crimson Hexagon’s (Now Brandwatch Consumer Research’s) AI-Driven Analyses. J. Advert. 2020, 1–11. [Google Scholar] [CrossRef]
- Wojcik, S.; Hughes, A. Sizing Up Twitter Users 2019. Available online: https://www.pewresearch.org/internet/2019/04/24/sizing-up-twitter-users/ (accessed on 2 May 2022).

{kind=link}
| Total N = 192 | ||
|---|---|---|
| M (SD) | Min–Max | |
| COVID-19 | ||
| Morbidity (per million) | 59,397 (62,332) | 8.60–260,309.74 |
| Mortality (per million) | 978 (1073) | 3.1–6050.71 |
| Country Characteristics | ||
| GDP per capita | US$18,061 ($19,296) | 661.24–116,935.6 |
| Total population | 40,867,457 (150,016,829) | 10,873–1.44 billion |
| Population density | 301 (1519) | 1.98–19,347.5 |
| Literacy rate | 86% (18%) | 19.10–80.90% |
| Democracy index a | 2.24 (1.08) | 1–4 |
| Institutional quality b | −0.07 (0.91) | −3–1.78 |
| Human development index c | 0.72 (0.15) | 0.39–0.96 |
| Vaccination Rate d | 46.99% (27.77%) | 0.00–99% |
| Low-income countries | 8.01% (9.44%) | 0.00–45% |
| Middle-income countries | 36.8% (23.6%) | 1.00–84% |
| Upper-middle income countries | 48.36% (21.37%) | 8.00–90.29% |
| High-income countries | 72.26% (12.36%) | 38.83–98.99% |
| Vaccine Tweets | Global M (SD) | Top 10 Countries |
|---|---|---|
| COVID19 vaccine tweets per million users | 633.19 (1941.93) | Monaco (20739.44), Canada (9302.41), Ireland (8348.63), United Kingdom (7889.12), United States (5466.66), Maldives (5082.80), Singapore (3347.87), Uruguay (2637.25), Japan (2238.79), Kuwait (2165.87) |
| Death mention | 1.99% (2.77%) | Germany (25.60%), Austria (21.60%), Japan (12.90%), rgw Netherlands (10.68%), Liechtenstein (10.64%), Switzerland (9.43%), Suriname (4.93%), Namibia (4.90%), Swaziland (4.20%), Timor-Leste (4.08%) |
| Side-effects mention | 1.15% (0.79%) | Burundi (4.16%), Comoros (4.00%), Germany (3.47%), Netherland (3.46%), Denmark (3.39%), Slovenia (3.24%), Macedonia (3.24%), Rep. of Congo (3.07%), Japan (2.92%), Thailand (2.95%) |
| Blood clots mention | 0.79% (0.69%) | Equatorial Guinea (3.52%), Serbia (3.39%), Cyprus (3.89%), Swaziland (2.80%), Lesotho (2.47%), Central African Republic (2.39%), Slovenia (2.30%), Montenegro (2.22%), Mauritius (2.13%), Norway (2.08%) |
| Joy | N = 8289 (SD = 56,983) | United States (714,642), United Kingdom (228,668), India (215,465), Canada (155,620), Nigeria (28,166), Australia (25,882), Ireland (16,930), Malaysia (14,676), South Africa (13,547), Kenya (11,726) |
| Fear | N = 2315 (SD = 16,077) | United States (203,800), United Kingdom (63,378), Canada (53,693), India (42,690), Australia (14,856), Nigeria (6319), Ireland (5867), South Africa (5838), Malaysia (4457), Philippines (3552) |
| Sadness | N = 3437 (SD = 25,311) | United States (329,899), India (82,938), United Kingdom (71,629), Canada (60,401), Australia (18,144), Nigeria (11,960), South Africa (10,860), Kenya (7505), Ireland (5510), Malaysia (5008) |
| Anger | N = 1625 (SD = 12,051) | United States (151,662), United Kingdom (55,883), Canada (39,808), India (23,094), Australia (9596), South Africa (4245), Ireland (4010), Nigeria (3047), Kenya (2094), Malaysia (1607) |
| Likelihood of negative sentiment (vs. positive) | 1.90 times (1.33) | Turkey (11.93 times), Burundi (8.73 times), Japan (6.79 times), Dem. Rep. of Congo (6.68 times), Burma (5.18 times), Togo (5.06 times), Central African Republic (4.67 times), Guatemala (4.31 times), Chad (4 times), Cape Verde (4 times) |
| Likelihood of fear/sadness/anger emotions (vs. joy) | 0.70 times (0.33) | Namibia (1.87 times), Australia (1.65 times), Eritrea (1.63 times), Burma (1.60 times), South Africa (1.55 times), Samoa (1.52 times), Swaziland (1.50 times), Iran (1.50 times), Antigua and Barbuda (1.48 times), Iceland (1.36 times) |
| Death Mention | Side-Effect Mentions | Blood Clot Mentions | Negative Sentiment | Fear/ Sadness/Anger | |
|---|---|---|---|---|---|
| r (p) | r (p) | r (p) | r (p) | ||
| Death mention | 0.414 (<0.001) | 0.112 (0.122) | 0.235 (0.001) | 0.182 (0.012) | |
| Side-effect mentions | 0.243 (<0.001) | 0.338 (<0.001) | 0.207 (0.004) | ||
| Blood clot mentions | −0.042 (0.568) | 0.316 (<0.001) | |||
| Negative sentiment | 0.306 (0.001) | ||||
| COVID-19 | |||||
| Morbidity (per million) | 0.186 (<0.001) | 0.224 (0.002) | 0.257 (<0.001) | −0.008 (0.917) | 0.080 (0.280) |
| Mortality (per million) | 0.111 (0.137) | 0.061 (0.417) | 0.159 (0.033) | 0.035 (0.642) | 0.089 (0.236) |
| Country Characteristics | |||||
| GDP per capita | 0.247 (<0.001) | 0.222 (0.002) | 0.168 (0.022) | 0.002 (0.976) | 0.231 (0.002) |
| Total population | 0.043 (0.560) | −0.046 (0.525) | −0.072 (325) | −0.027 (713) | 0.074 (0.313) |
| Population density | −0.003 (0.969) | 0.093 (0.205) | −0.010 (0.891) | 0.056 (0.444) | 0.136 (0.063) |
| Literacy rate | 0.173 (0.018) | 0.132 (0.071) | 0.205 (0.005) | 0.039 (0.592) | 0.274 (<0.001) |
| Democracy index | 0.358 (<0.001) | 0.259 (<0.001) | 0.296 (<0.001) | 0.008 (0.919) | 0.241 (0.002) |
| Institutional quality | 0.340 (<0.001) | 0.243 (<0.001) | 0.226 (0.002) | −0.029 (0.687) | 0.235 (<0.001) |
| Human development index | 0.280 (<0.001) | 0.217 (0.003) | 0.238 (<0.001) | −0.019 (0.796) | 0.259 (<0.001) |
| r (p) | Model I | Model II | Model III | ||||
|---|---|---|---|---|---|---|---|
| COVID-19 | b | SE | b | SE | b | SE | |
| Morbidity | 0.485 (<0.001) | 0.538 *** | 0.000 | −0.126 | 0.000 | −0.053 | 0.000 |
| Mortality | 0.328 (<0.001) | −0.071 | 0.003 | −0.035 | 0.002 | −0.085 | 0.002 |
| Total R2 = 0.24 | R2Change = 0.24 | R2Change = 0.24 | |||||
| Country Characteristics | |||||||
| GDP per capita | 0.642 (<0.001) | 0.025 | 0.000 | 0.073 | 0.000 | ||
| Total population | 0.078 (0.283) | 0.103 * | 0.000 | 0.103 * | 0.000 | ||
| Population density | 0.114 (0.116) | 0.011 | 0.002 | 0.006 | 0.002 * | ||
| Literacy rate | 0.671 (<0.001) | 0.040 | 0.138 | 0.071 | 0.132 | ||
| Democracy index | 0.554 (<0.001) | −0.016 | 20.183 | 0.053 | 2.254 | ||
| Institutional quality | 0.690 (<0.001) | 0.197 | 30.509 | 0.202 | 3.292 | ||
| Human development index | 0.812 (<0.001) | 0.734 *** | 260.490 | 0.682 *** | 25.275 | ||
| R2Change = 0.48 | R2Change = 0.48 | ||||||
| Total R2 = 0.72 | |||||||
| Vaccine Tweets | |||||||
| COVID19 vaccine tweets | 0.070 (0.347) | 0.052 | 0.003 | ||||
| Death mention | 0.387 (0.009) | 0.003 | 0.469 | ||||
| Side-effect mentions | 0.003 (0.971) | −0.156 ** | 1.889 | ||||
| Blood clot mentions | 0.058 (0.428) | −0.042 | 2.050 | ||||
| Negative sentiment | −0.050 (0.945) | −0.022 | 0.248 | ||||
| Fear/sadness/anger | 0.144 (0.049) | −0.105 * | 4.630 | ||||
| R2 Change = 0.05 | |||||||
| Total R2 = 0.77 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jun, J.; Zain, A.; Chen, Y.; Kim, S.-H. Adverse Mentions, Negative Sentiment, and Emotions in COVID-19 Vaccine Tweets and Their Association with Vaccination Uptake: Global Comparison of 192 Countries. Vaccines 2022, 10, 735. https://doi.org/10.3390/vaccines10050735
Jun J, Zain A, Chen Y, Kim S-H. Adverse Mentions, Negative Sentiment, and Emotions in COVID-19 Vaccine Tweets and Their Association with Vaccination Uptake: Global Comparison of 192 Countries. Vaccines. 2022; 10(5):735. https://doi.org/10.3390/vaccines10050735
Chicago/Turabian StyleJun, Jungmi, Ali Zain, Yingying Chen, and Sei-Hill Kim. 2022. "Adverse Mentions, Negative Sentiment, and Emotions in COVID-19 Vaccine Tweets and Their Association with Vaccination Uptake: Global Comparison of 192 Countries" Vaccines 10, no. 5: 735. https://doi.org/10.3390/vaccines10050735
APA StyleJun, J., Zain, A., Chen, Y., & Kim, S.-H. (2022). Adverse Mentions, Negative Sentiment, and Emotions in COVID-19 Vaccine Tweets and Their Association with Vaccination Uptake: Global Comparison of 192 Countries. Vaccines, 10(5), 735. https://doi.org/10.3390/vaccines10050735