
Assessing Community Acceptance of Maternal Immunisation in Rural KwaZulu-Natal, South Africa: A Qualitative Investigation

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis and Interpretation
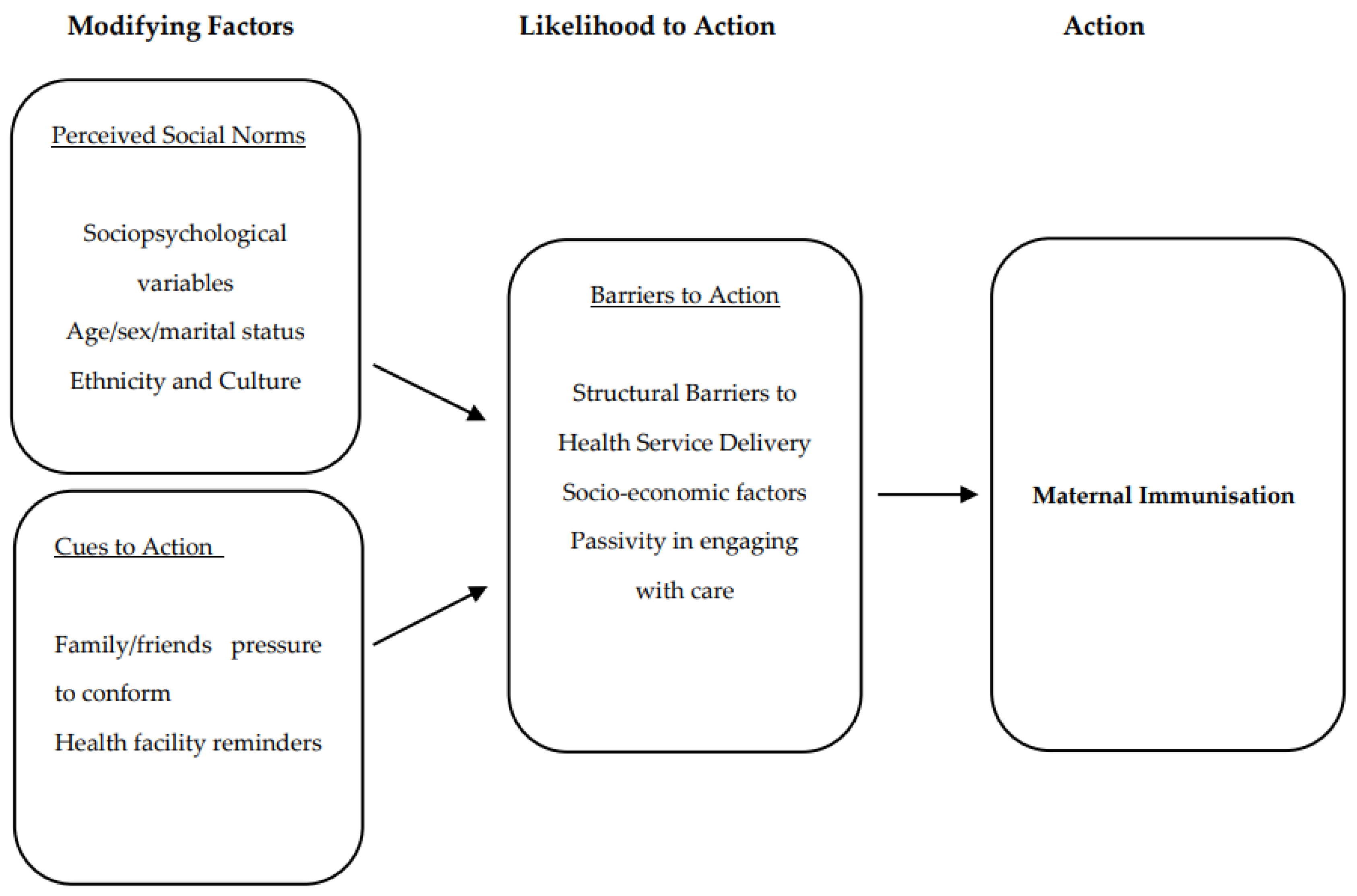
2.3. Theoretical Framework
3. Results
3.1. Modifying Factors
3.1.1. Sociopsychological Variables
“…I don’t know why, but there are others [men] who refuse [to allow] their partners to go to the clinic. Others [some men] don’t like the fact that their partners will be pursued by other men on the road. Others just don’t want to give them money…for transport…”.(Female, 19 years old, PWP-MPU01-060220)
3.1.2. Ethnicity and Culture
“…giving them the rope to wear around their waist. I take that rope and I prepare it using traditional medicines before I give it to the person… So, we offer them means to protect themselves and their pregnancy”.(KII-THP02-15012019)
“…The clinic does not help with anything, how does it protect the baby, you will then find yourself staying at home and not going to the clinic and have faith that your ancestors will protect the baby”.(Pregnant woman, 24 years old, FGD-PWP-HLU01-171219)
“… as I am saying they are (people) who use “isihlambezo” who believe that if they get this… this vaccination will affect the functioning of this “isihlambezo”. But as long as they believe in that thing (isihlambezo) you won’t do anything to them.… she won’t take a thing you are saying…”.(Female Advanced Midwifery healthcare worker, KII-A&MS-MPUK01-13022020)
“…a woman has that belief, saying that no I’m not going anywhere for a period of time… you see, you will find that they do not believe in using the clinic. You see I grew up at home, my mother was not using the clinic, she was that kind of a person. They were using traditional medicines and only that…”.(Mother of pregnant woman, 39 years old, PPW-05-29062020)
3.2. Cues to Action
3.2.1. Family and Friends’ Pressure to Conform
“…In other households you’d find that a pregnant woman may be allowed to go to the clinic maybe for the first day, but when she gets home her mother may change and say neither of my children attends the clinic, in this household we have ancestors…”.(Pregnant woman, 24 years old, FGD-PWP-HLU01-171219)
3.2.2. Health Facility Regulations on Maternal Immunisation
“…I did get it, isn’t it they vaccinated me without knowledge of what the vaccine is or (laughs). What can I say like if they are vaccinating us by force and hey it is the law, isn’t it we are ruled by the law…”.(Mother of pregnant woman, 39 years old, MPW-04-19062020)
3.3. Likelihood of Action
Barriers to Action
“…No, sometimes you come across nurses who have a bad attitude…I was reluctant to ask as to why are we being injected, what are we injecting for on the arm because all of us who were there they gave us that injection”.(Pregnant woman, 34 years old, IMPR-MPW-01-17062020)
“…Eh I think others have the problem of their transportation. For the person to go to the clinic, that can have an impact of ended up not going…”.(Female Antenatal and Maternal healthcare worker, IMPR-A&MS-01-170120)
“…maybe you find (out) that eh, there is no (more) vaccinations at the clinic, probably the vaccination will arrive at some other time…”.(Female Antenatal and Maternal healthcare worker, IMPR-KII-A&MS-01-13022020)
“…It was my first time to get an injection on the arm, I even told them here at home that now when you start clinic you get injection, we were discussing as mothers as to why we are being injected now on the arm…. But I would not have had information as to what they were injecting us for…”.(Female, 34 years old, IMPR-MPW-01-17062020)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Maertens, K.; Orije, M.R.P.; Van Damme, P.; Leuridan, E. Vaccination during pregnancy: Current and possible future recommendations. Eur. J. Pediatr. 2020, 179, 235–242. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Neonatal Tetanus. Regional Committee for the Eastern Mediterranean; World Health Organisation: Geneva, Switzerland, 1982. [Google Scholar]
- Dangor, Z.; Lala, S.G. Maternal vaccination to prevent pertussis in infants. S. Afr. J. Child Health 2016, 10, 146. [Google Scholar] [CrossRef] [Green Version]
- National Department of Health (NDoH). Guidelines for maternity care in South Africa. In A Manual for Clinics, Community Health Centres and District Hospital, 4th ed.; National Department of Health, Republic of South Africa: Pretoria, South Africa, 2015. [Google Scholar]
- WHO/UNICEF. WHO-UNICEF Estimates of DTP3 Coverage. Available online: https://apps.who.int/immunization_monitoring/globalsummary/timeseries/tswucoveragedtp3.html (accessed on 15 September 2021).
- National Department of Health (NDoH). South Africa’s National Strategic Plan for a Campaign on Accelerated Reduction of Maternal and Child Mortality in Africa (CARMMA); National Department of Health: Pretoria, South Africa, 2012.
- National Department of Health (NDoH). South Africa Demographic and Health Survey 2016: Report; National Department of Health (NDoH), Statistics South Africa (Stats SA), South African Medical Research Council (SAMRC), and ICF: Pretoria, South Africa; National Department of Health (NDoH): Rockville, MD, USA, 2016.
- Statistics South Africa (Stats SA). Maternal Health Indicators: Further Analysis of the 1998 and 2016 South Africa Demographic and Health SurveysNational Department of Health (NDoH); Statistics South Africa: Pretoria, South Africa, 2020.
- WHO. Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: Executive Summary. License: CC BY-NC-SA 3.0 IGO ed. Available online: https://apps.who.int/iris/handle/10665/327596 (accessed on 11 October 2021).
- National Department of Health (NDoH). Health on Expanded Programme on Immunisation. 2007. Available online: https://www.gov.za/health-expanded-programme-immunisation-0 (accessed on 28 February 2022).
- Massyn, N.P.Y.; Padarath, A. District Health Barometer; Health Systems Trust: Durban, South Africa, 2019. [Google Scholar]
- Tanser, F.; Hosegood, V.; Benzler, J.; Solarsh, G. New approaches to spatially analyse primary health care usage patterns in rural South Africa. Trop. Med. Int. Health 2001, 6, 826–838. [Google Scholar] [CrossRef] [PubMed]
- Godongwana, M.; Myburgh, N.; Adedini, S.A.; Cutland, C.; Radebe, N. Knowledge and attitudes towards maternal immunization: Perspectives from pregnant and non-pregnant mothers, their partners, mothers, healthcare providers, community and leaders in a selected urban setting in South Africa. Heliyon 2021, 7, e05926. [Google Scholar] [CrossRef] [PubMed]
- Moniz, M.H.; Beigi, R.H. Maternal immunization. Hum. Vaccines Immunother. 2014, 10, 2562–2570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, C.J. A Meta-Analysis of the Effectiveness of Health Belief Model Variables in Predicting Behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 28–35. [Google Scholar] [CrossRef]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, K.T.; Pasch, L.A.; Cornelius, T.; Cirigliano, E. Predicting Participation in Premarital Prevention Programs: The Health Belief Model and Social Norms. Fam. Process 2004, 43, 175–193. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Proce. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Reid, A.E.; Cialdini, R.B.; Aiken, L.S. Social norms and health behavior. In Handbook of Behavioral Medicine: Methods and Applications; Springer Science + Business Media: New York, NY, USA, 2011; pp. 263–274. [Google Scholar]
- Frew, P.M.; Saint-Victor, D.S.; Owens, L.E.; Omer, S.B. Socioecological and message framing factors influencing maternal influenza immunization among minority women. Vaccine 2014, 32, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Kilich, E.; Dada, S.; Francis, M.R.; Tazare, J.; Chico, R.M.; Paterson, P.; Larson, H.J. Factors that influence vaccination decision-making among pregnant women: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0234827. [Google Scholar] [CrossRef] [PubMed]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, A.K.; Fields, R.; McQuestion, M. The future of routine immunization in the developing world: Challenges and opportunities. Glob. Health Sci. Pract. 2014, 2, 381–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mothiba, T.M.; Tladi, F.M. Challenges faced by professional nurses when implementing the Expanded Programme on Immunisation at rural clinics in Capricorn District, Limpopo. Afr. J. Prim. Health Care Fam. Med. 2016, 8, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhwava, L.S.; Morojele, N.; London, L. Psychosocial factors associated with early initiation and frequency of antenatal care (ANC) visits in a rural and urban setting in South Africa: A cross-sectional survey. BMC Pregnancy Childbirth 2016, 16, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chetty, T.; Yapa, H.M.N.; Herbst, C.; Geldsetzer, P.; Naidu, K.K.; De Neve, J.W.; Herbst, K.; Matthews, P.; Pillay, D.; Wyke, S. The MONARCH intervention to enhance the quality of antenatal and postnatal primary health services in rural South Africa: Protocol for a stepped-wedge cluster-randomised controlled trial. BMC Health Serv. Res. 2018, 18, 625. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Study Participants | Number Interviewed Including the Focus Group Discussion | Description |
|---|---|---|
| Pregnant women | 9 | Pregnant women (Primigravida and Multipls) |
| Caregivers/mothers of pregnant women | 7 | Individuals who cared for pregnant women |
| Healthcare workers | 4 | Healthcare personnel specialising in advanced midwifery and as breastfeeding consultants |
| Traditional Healers | 3 | Traditional medicine practitioners |
| Faith healers | 2 | Individuals that were described as anointed for healing either traditional or spiritual |
| Church leaders | 2 | Religious leaders in the church |
| Community Midwife | 1 | Individuals who assist in childbirth within the community. Not registered with the Department of Health |
| Total | 28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chimukuche, R.S.; Ngwenya, N.; Seeley, J.; Nxumalo, P.S.; Nxumalo, Z.P.; Godongwana, M.; Radebe, N.; Myburgh, N.; Adedini, S.A.; Cutland, C. Assessing Community Acceptance of Maternal Immunisation in Rural KwaZulu-Natal, South Africa: A Qualitative Investigation. Vaccines 2022, 10, 415. https://doi.org/10.3390/vaccines10030415
Chimukuche RS, Ngwenya N, Seeley J, Nxumalo PS, Nxumalo ZP, Godongwana M, Radebe N, Myburgh N, Adedini SA, Cutland C. Assessing Community Acceptance of Maternal Immunisation in Rural KwaZulu-Natal, South Africa: A Qualitative Investigation. Vaccines. 2022; 10(3):415. https://doi.org/10.3390/vaccines10030415
Chicago/Turabian StyleChimukuche, Rujeko Samanthia, Nothando Ngwenya, Janet Seeley, Petronella Samukelisiwe Nxumalo, Zama Pinky Nxumalo, Motlatso Godongwana, Nomasonto Radebe, Nellie Myburgh, Sunday A. Adedini, and Clare Cutland. 2022. "Assessing Community Acceptance of Maternal Immunisation in Rural KwaZulu-Natal, South Africa: A Qualitative Investigation" Vaccines 10, no. 3: 415. https://doi.org/10.3390/vaccines10030415
APA StyleChimukuche, R. S., Ngwenya, N., Seeley, J., Nxumalo, P. S., Nxumalo, Z. P., Godongwana, M., Radebe, N., Myburgh, N., Adedini, S. A., & Cutland, C. (2022). Assessing Community Acceptance of Maternal Immunisation in Rural KwaZulu-Natal, South Africa: A Qualitative Investigation. Vaccines, 10(3), 415. https://doi.org/10.3390/vaccines10030415