
Patients with Liver Cirrhosis Show High Immunogenicity upon COVID-19 Vaccination but Develop Premature Deterioration of Antibody Titers

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
3.2. Antibody Response and Titer after COVID-19 Vaccination
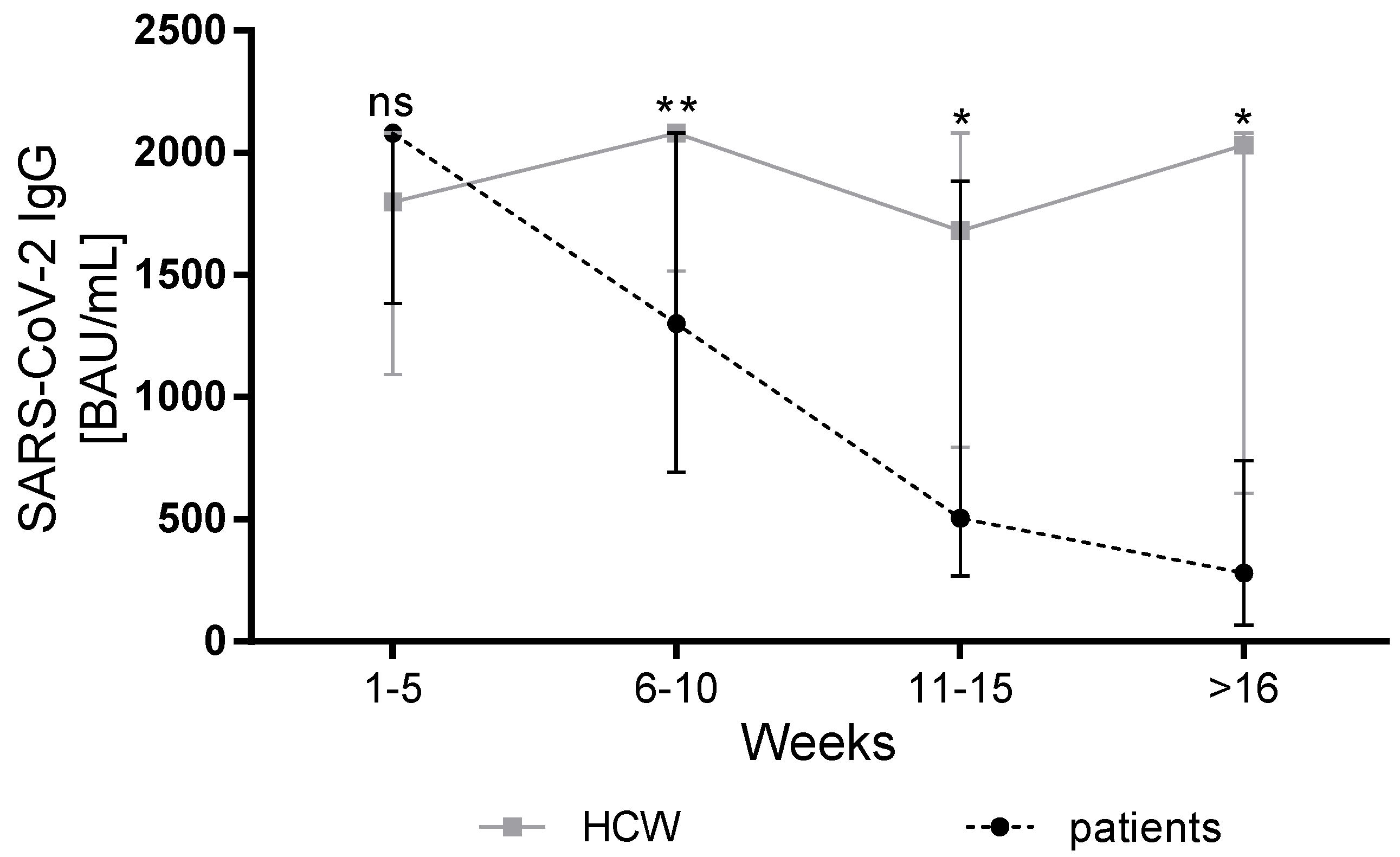
3.3. Course of Antibody Response in Patients with Liver Cirrhosis and HCW
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Gines, P.; Lohse, A.W.; Moon, A.M.; Pose, E.; Trivedi, P.; Barnes, E. SARS-CoV-2 vaccination in patients with liver disease: Responding to the next big question. Lancet Gastroenterol. Hepatol. 2021, 6, 156–158. [Google Scholar] [CrossRef]
- Cornberg, M.; Buti, M.; Eberhardt, C.S.; Grossi, P.A.; Shouval, D. EASL position paper on the use of COVID-19 vaccines in patients with chronic liver diseases, hepatobiliary cancer and liver transplant recipients. J. Hepatol. 2021, 74, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Fix, O.K.; Blumberg, E.A.; Chang, K.M.; Chu, J.; Chung, R.T.; Goacher, E.K.; Hameed, B.; Kaul, D.R.; Kulik, L.M.; Kwok, R.M.; et al. American Association for the Study of Liver Diseases Expert Panel Consensus Statement: Vaccines to Prevent Coronavirus Disease 2019 Infection in Patients with Liver Disease. Hepatology 2021, 74, 1049–1064. [Google Scholar] [CrossRef] [PubMed]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Rashidi-Alavijeh, J.; Frey, A.; Passenberg, M.; Korth, J.; Zmudzinski, J.; Anastasiou, O.E.; Saner, F.H.; Jahn, M.; Lange, C.M.; Willuweit, K. Humoral Response to SARS-Cov-2 Vaccination in Liver Transplant Recipients-A Single-Center Experience. Vaccines 2021, 9, 738. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Alvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [Green Version]
- Piano, S.; Brocca, A.; Mareso, S.; Angeli, P. Infections complicating cirrhosis. Liver Int. 2018, 38 (Suppl. S1), 126–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, J.; Pletcher, M.J.; Lai, J.C.; Consortium, N.C. Outcomes of SARS-CoV-2 Infection in Patients with Chronic Liver Disease and Cirrhosis: A National COVID Cohort Collaborative Study. Gastroenterology 2021, 161, 1487–1501.e5. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, N.; Viveiros, K.; Redd, W.D.; Zhou, J.C.; McCarty, T.R.; Bazarbashi, A.N.; Hathorn, K.E.; Wong, D.; Njie, C.; Shen, L.; et al. Impact of chronic liver disease on outcomes of hospitalized patients with COVID-19: A multicentre United States experience. Liver Int. 2020, 40, 2515–2521. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Belli, L.S.; Duvoux, C.; Cortesi, P.A.; Facchetti, R.; Iacob, S.; Perricone, G.; Radenne, S.; Conti, S.; Patrono, D.; Berlakovich, G.; et al. COVID-19 in liver transplant candidates: Pretransplant and post-transplant outcomes—An ELITA/ELTR multicentre cohort study. Gut 2021, 70, 1914–1924. [Google Scholar] [CrossRef] [PubMed]
- Aggeletopoulou, I.; Davoulou, P.; Konstantakis, C.; Thomopoulos, K.; Triantos, C. Response to hepatitis B vaccination in patients with liver cirrhosis. Rev. Med. Virol. 2017, 27, e1942. [Google Scholar] [CrossRef] [PubMed]
- Harmala, S.; Parisinos, C.A.; Shallcross, L.; O’Brien, A.; Hayward, A. Effectiveness of influenza vaccines in adults with chronic liver disease: A systematic review and meta-analysis. BMJ Open 2019, 9, e031070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCashland, T.M.; Preheim, L.C.; Gentry, M.J. Pneumococcal vaccine response in cirrhosis and liver transplantation. J. Infect. Dis. 2000, 181, 757–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shouval, D. Hepatitis B vaccines. J. Hepatol. 2003, 39 (Suppl. S1), S70–S76. [Google Scholar] [CrossRef]
- Alukal, J.J.; Naqvi, H.A.; Thuluvath, P.J. Vaccination in Chronic Liver Disease: An Update. J. Clin. Exp. Hepatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Adeniji, N.; Latt, N.; Kumar, S.; Bloom, P.P.; Aby, E.S.; Perumalswami, P.; Roytman, M.; Li, M.; Vogel, A.S.; et al. Predictors of Outcomes of COVID-19 in Patients with Chronic Liver Disease: US Multi-center Study. Clin. Gastroenterol. Hepatol. 2021, 19, 1469–1479.e19. [Google Scholar] [CrossRef] [PubMed]
- John, B.V.; Deng, Y.; Scheinberg, A.; Mahmud, N.; Taddei, T.H.; Kaplan, D.; Labrada, M.; Baracco, G.; Dahman, B. Association of BNT162b2 mRNA and mRNA-1273 Vaccines with COVID-19 Infection and Hospitalization Among Patients with Cirrhosis. JAMA Intern. Med. 2021, 181, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hou, Z.; Liu, J.; Gu, Y.; Wu, Y.; Chen, Z.; Ji, J.; Diao, S.; Qiu, Y.; Zou, S.; et al. Safety and immunogenicity of COVID-19 vaccination in patients with non-alcoholic fatty liver disease (CHESS2101): A multicenter study. J. Hepatol. 2021, 75, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Thuluvath, P.J.; Robarts, P.; Chauhan, M. Analysis of antibody responses after COVID-19 vaccination in liver transplant recipients and those with chronic liver diseases. J. Hepatol. 2021, 75, 1434–1439. [Google Scholar] [CrossRef]
- Calleri, A.; Saracco, M.; Pittaluga, F.; Cavallo, R.; Romagnoli, R.; Martini, S. Seroconversion after Coronavirus Disease 2019 Vaccination in Patients Awaiting Liver Transplantation: Fact or Fancy? Liver Transpl. 2021, 28, 180–187. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.; Fong, Y.; Benkeser, D.C.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune Correlates Analysis of the mRNA-1273 COVID-19 Vaccine Efficacy Trial. medRxiv 2021. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Campo, F.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Noia, V.; Di Domenico, E.G.; et al. Antibody Persistence 6 Months Post-Vaccination with BNT162b2 among Health Care Workers. Vaccines 2021, 9, 1125. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, D.; Antonazzo, I.C.; Caci, G.; Vitale, A.; Della Ragione, G.; Romano, M.L.; Borrelli, M.; Schiavone, B.; Polosa, R.; Ferrara, P. Dynamics of antibody response to BNT162b2 mRNA COVID-19 vaccine after 6 months. J. Travel. Med. 2021, 28, taab173. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, D.; Madotto, F.; Conti, S.; Antonazzo, I.C.; Vitale, A.; Della Ragione, G.; Romano, M.L.; Borrelli, M.; Schiavone, B.; Polosa, R.; et al. Response to BNT162b2 mRNA COVID-19 vaccine among healthcare workers in Italy: A 3-month follow-up. Intern. Emerg. Med. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Henry, B.M.; Pighi, L.; De Nitto, S.; Gianfilippi, G.L.; Lippi, G. Three-month analysis of total humoral response to Pfizer BNT162b2 mRNA COVID-19 vaccination in healthcare workers. J. Infect. 2021, 83, e4–e5. [Google Scholar] [CrossRef] [PubMed]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to Covid-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef] [PubMed]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef]
- Gruell, H.; Vanshylla, K.; Tober-Lau, P.; Hillus, D.; Schommers, P.; Lehmann, C.; Kurth, F.; Sander, L.E.; Klein, F. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. Nat. Med. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Irvine, K.M.; Ratnasekera, I.; Powell, E.E.; Hume, D.A. Causes and Consequences of Innate Immune Dysfunction in Cirrhosis. Front. Immunol. 2019, 10, 293. [Google Scholar] [CrossRef]
- Cook, R.T.; Waldschmidt, T.J.; Cook, B.L.; Labrecque, D.R.; McLatchie, K. Loss of the CD5+ and CD45RAhi B cell subsets in alcoholics. Clin. Exp. Immunol. 1996, 103, 304–310. [Google Scholar] [CrossRef]
- Doi, H.; Iyer, T.K.; Carpenter, E.; Li, H.; Chang, K.M.; Vonderheide, R.H.; Kaplan, D.E. Dysfunctional B-cell activation in cirrhosis resulting from hepatitis C infection associated with disappearance of CD27-positive B-cell population. Hepatology 2012, 55, 709–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massonnet, B.; Delwail, A.; Ayrault, J.M.; Chagneau-Derrode, C.; Lecron, J.C.; Silvain, C. Increased immunoglobulin A in alcoholic liver cirrhosis: Exploring the response of B cells to Toll-like receptor 9 activation. Clin. Exp. Immunol. 2009, 158, 115–124. [Google Scholar] [CrossRef]
- Albillos, A.; Hera Ad Ade, L.; Reyes, E.; Monserrat, J.; Munoz, L.; Nieto, M.; Prieto, A.; Sanz, E.; Alvarez-Mon, M. Tumour necrosis factor-alpha expression by activated monocytes and altered T-cell homeostasis in ascitic alcoholic cirrhosis: Amelioration with norfloxacin. J. Hepatol. 2004, 40, 624–631. [Google Scholar] [CrossRef]
- Lario, M.; Munoz, L.; Ubeda, M.; Borrero, M.J.; Martinez, J.; Monserrat, J.; Diaz, D.; Alvarez-Mon, M.; Albillos, A. Defective thymopoiesis and poor peripheral homeostatic replenishment of T-helper cells cause T-cell lymphopenia in cirrhosis. J. Hepatol. 2013, 59, 723–730. [Google Scholar] [CrossRef]
- Yonkers, N.L.; Sieg, S.; Rodriguez, B.; Anthony, D.D. Reduced naive CD4 T cell numbers and impaired induction of CD27 in response to T cell receptor stimulation reflect a state of immune activation in chronic hepatitis C virus infection. J. Infect. Dis. 2011, 203, 635–645. [Google Scholar] [CrossRef] [Green Version]
- Ruether, D.F.; Schaub, G.M.; Duengelhoef, P.M.; Haag, F.; Brehm, T.T.; Fathi, A.; Wehmeyer, M.; Jahnke-Triankowski, J.; Mayer, L.; Hoffmann, A.; et al. SARS-CoV2-specific Humoral and T-cell Immune Response after Second Vaccination in Liver Cirrhosis and Transplant Patients. Clin. Gastroenterol. Hepatol. 2021, 20, 162–172.e9. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, P.; Ponticelli, D.; Aguero, F.; Caci, G.; Vitale, A.; Borrelli, M.; Schiavone, B.; Antonazzo, I.C.; Mantovani, L.G.; Tomaselli, V.; et al. Does smoking have an impact on the immunological response to COVID-19 vaccines? Evidence from the VASCO study and need for further studies. Public Health 2022, 203, 97–99. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Characteristics | Patients n/(%) | HCW n/(%) | p-Value |
|---|---|---|---|
| Total patient number | 110 | 80 | - |
| Sex (male/female) | 50 (50)/55 (50) | 20 (25)/60 (75) | 0.001 |
| Child A/Child B/Child C | 76 (69)/31 (28)/3 (3) | - | |
| SARS-CoV-2 IgG detectability rate | 106 (96) | 79 (99) | 0.40 |
| Median (IQR) | Median (IQR) | ||
| MELD score at first vaccination | 10 (8–13) | - | - |
| Age at first vaccination [years] | 55 (45–61) | 54 (45–59) | 0.19 |
| Time between first and second doses [days] | 42 (35–42) | 44 (22–47) | 0.39 |
| Time between second dose and SARS-CoV-2 Ab detection [days] | 69 (43–106) | 56 (38–90) | 0.20 |
| SARS-CoV-2 IgG (BAU/mL) | 939 (307 to >2080) | 1905 (996.3 to >2080) | 0.0001 |
| Diagnosis | n (%) |
|---|---|
| Alcoholic-induced liver cirrhosis | 35 (32) |
| Primary sclerosing cholangitis | 18 (16) |
| Autoimmune hepatitis | 10 (9) |
| Non-alcoholic steatohepatitis | 9 (8) |
| Primary biliary cholangitis | 8 (7) |
| Cryptogenic liver cirrhosis | 8 (7) |
| Hepatitis C virus-induced liver cirrhosis | 6 (5) |
| Secondary sclerosing cholangitis | 5 (5) |
| Hepatitis B virus-induced liver cirrhosis | 3 (3) |
| Wilson’s disease | 3 (3) |
| Hepatocellular carcinoma | 1 (1) |
| Others 1 | 4 (4) |
| Patients | SARS-CoV-2 IgG (BAU/mL) Median (IQR) | p-Value |
|---|---|---|
| Age | ||
| <60 years (n = 76) | 965 (325.5 to >2080) | 0.96 |
| ≥60 years (n = 34) | 740 (293 to >2080) | |
| MELD score | ||
| <15 (n = 97) | 965 (344.5 to >2080) | 0.15 |
| ≥15 (n = 13) | 570 (128.45–1680) | |
| Child score | ||
| Child A (n = 76) | 968 (362.5 to >2080) | 0.15 |
| Child B (n = 31) | 815 (203 to >2080) | |
| Child C (n = 3) | 203 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willuweit, K.; Frey, A.; Passenberg, M.; Korth, J.; Saka, N.; Anastasiou, O.E.; Möhlendick, B.; Schütte, A.; Schmidt, H.; Rashidi-Alavijeh, J. Patients with Liver Cirrhosis Show High Immunogenicity upon COVID-19 Vaccination but Develop Premature Deterioration of Antibody Titers. Vaccines 2022, 10, 377. https://doi.org/10.3390/vaccines10030377
Willuweit K, Frey A, Passenberg M, Korth J, Saka N, Anastasiou OE, Möhlendick B, Schütte A, Schmidt H, Rashidi-Alavijeh J. Patients with Liver Cirrhosis Show High Immunogenicity upon COVID-19 Vaccination but Develop Premature Deterioration of Antibody Titers. Vaccines. 2022; 10(3):377. https://doi.org/10.3390/vaccines10030377
Chicago/Turabian StyleWilluweit, Katharina, Alexandra Frey, Moritz Passenberg, Johannes Korth, Nissrin Saka, Olympia E. Anastasiou, Birte Möhlendick, Andreas Schütte, Hartmut Schmidt, and Jassin Rashidi-Alavijeh. 2022. "Patients with Liver Cirrhosis Show High Immunogenicity upon COVID-19 Vaccination but Develop Premature Deterioration of Antibody Titers" Vaccines 10, no. 3: 377. https://doi.org/10.3390/vaccines10030377
APA StyleWilluweit, K., Frey, A., Passenberg, M., Korth, J., Saka, N., Anastasiou, O. E., Möhlendick, B., Schütte, A., Schmidt, H., & Rashidi-Alavijeh, J. (2022). Patients with Liver Cirrhosis Show High Immunogenicity upon COVID-19 Vaccination but Develop Premature Deterioration of Antibody Titers. Vaccines, 10(3), 377. https://doi.org/10.3390/vaccines10030377