
Humoral and Cellular Immune Responses of Solid Organ Transplant Patients on Belatacept to Three Doses of mRNA-Based Anti-SARS-CoV-2 Vaccine

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Serological Assays
2.2. Elispot Assay
2.3. Statistical Analyses
3. Results
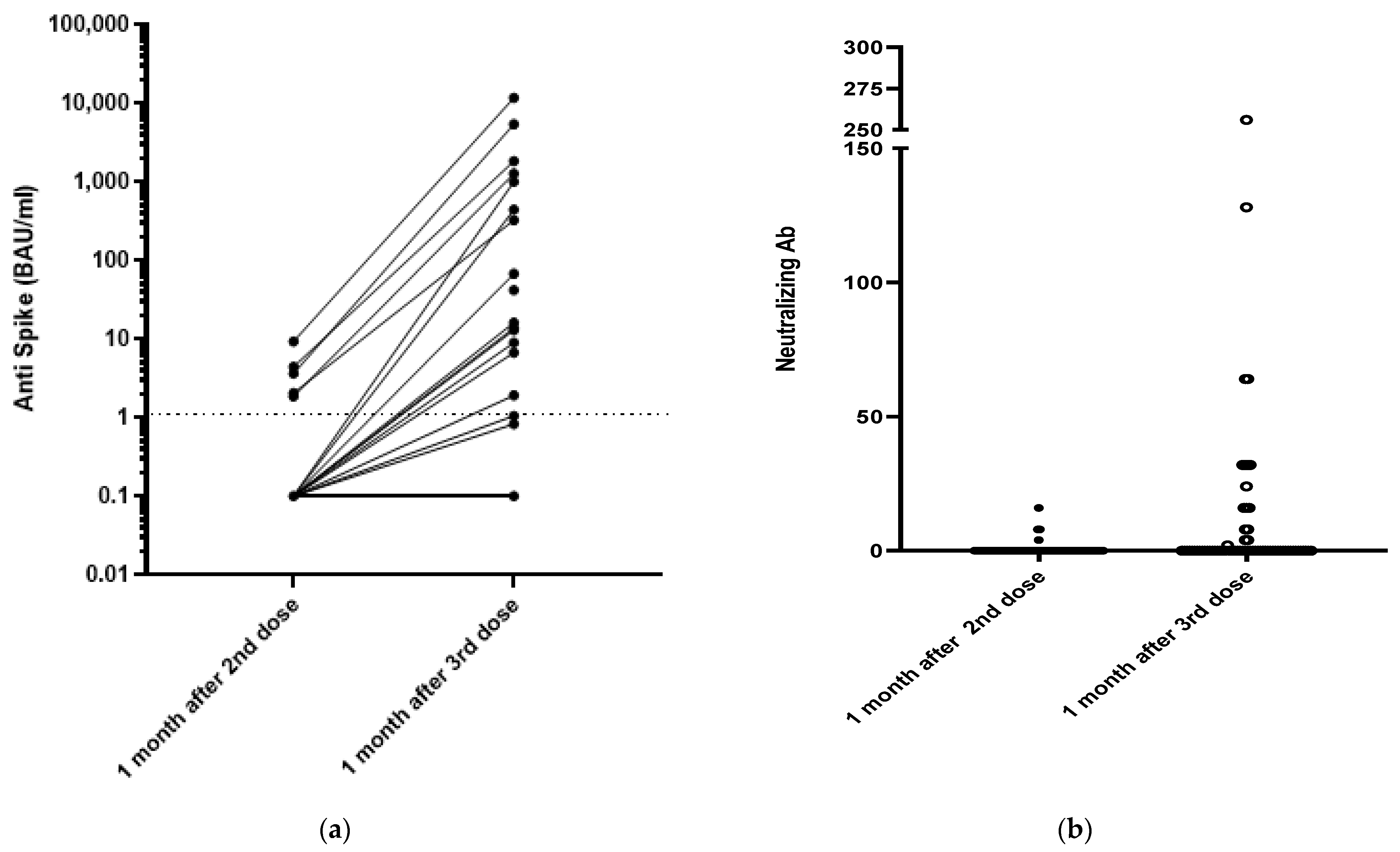
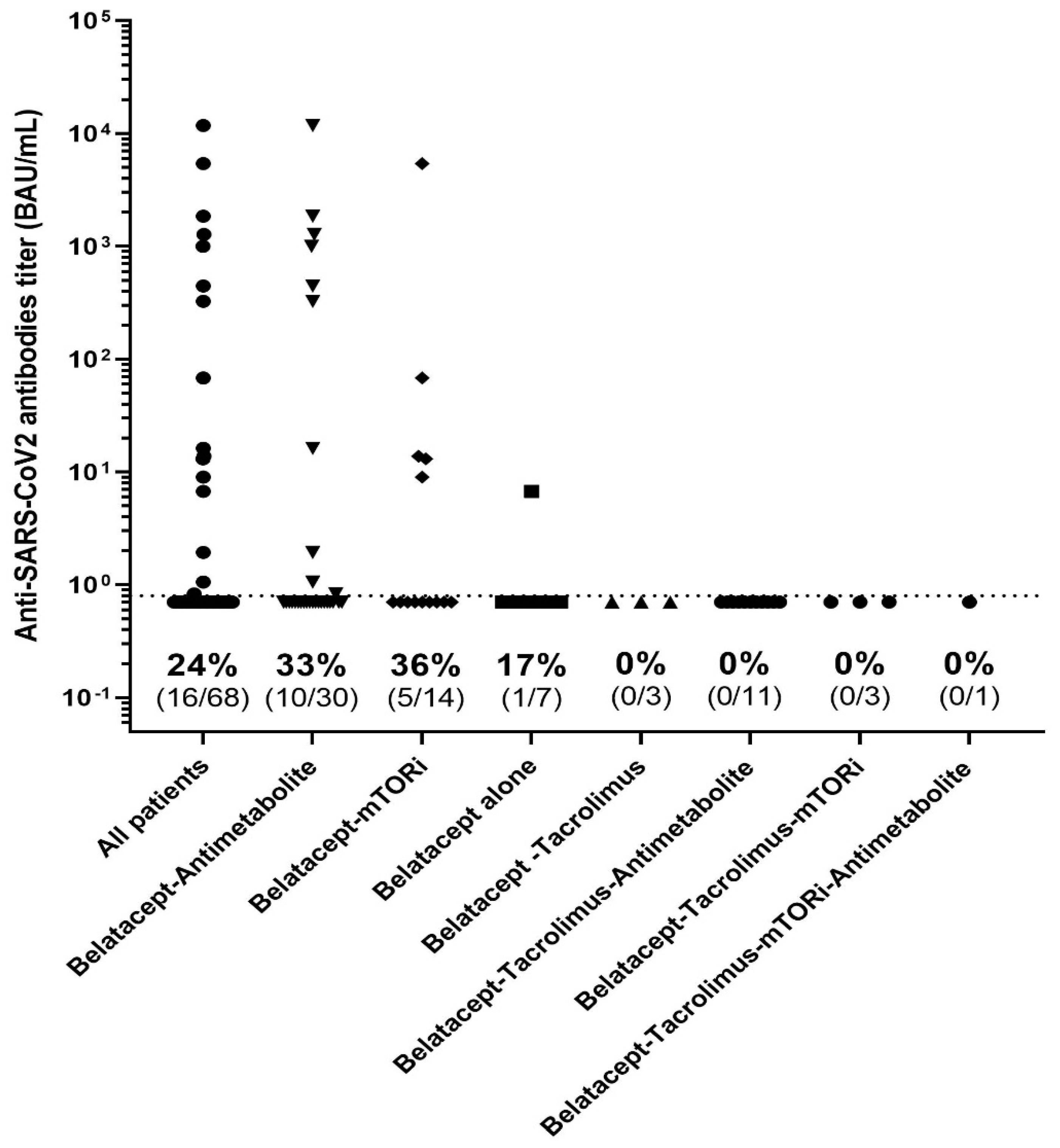
3.1. Humoral Response
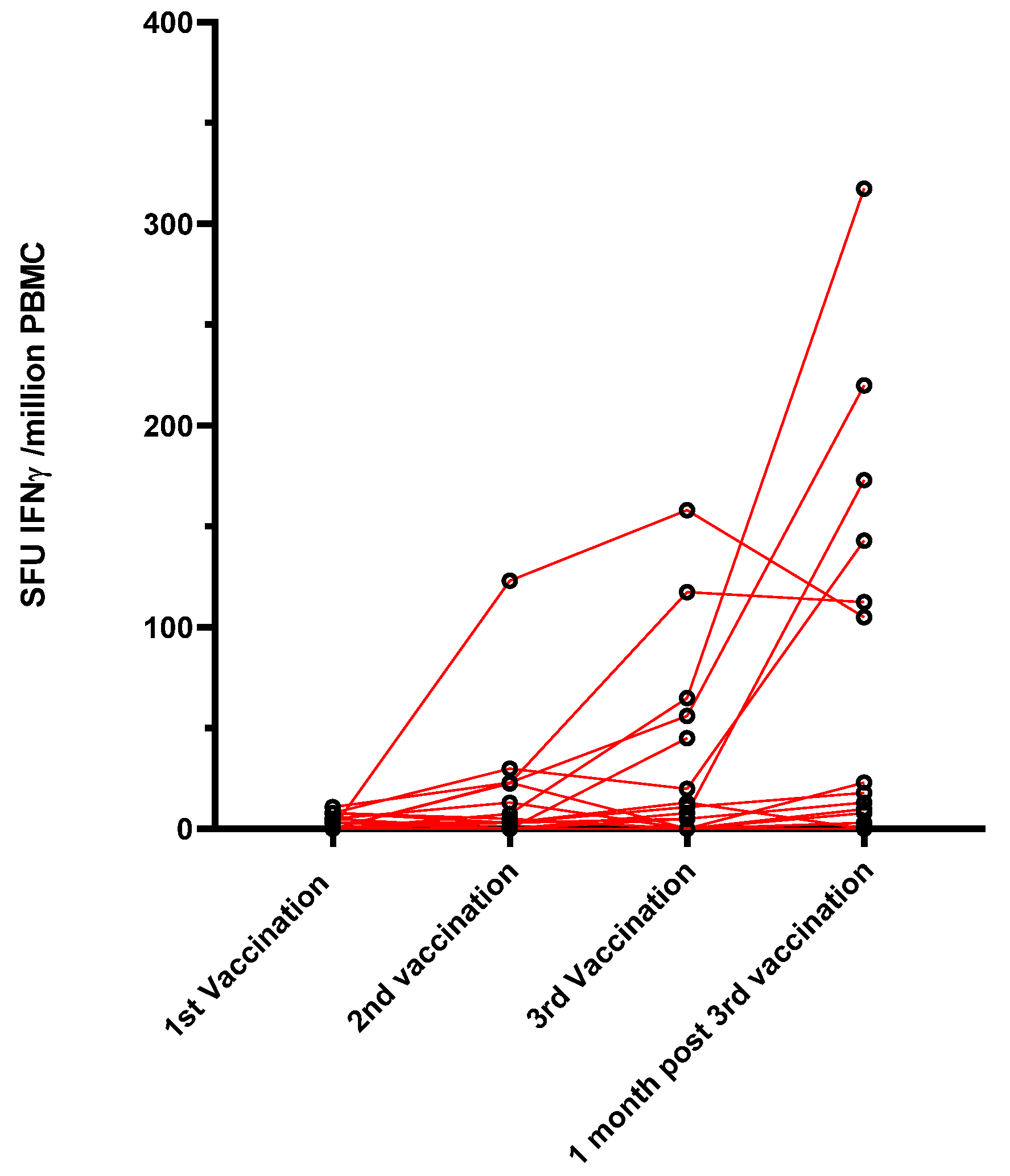
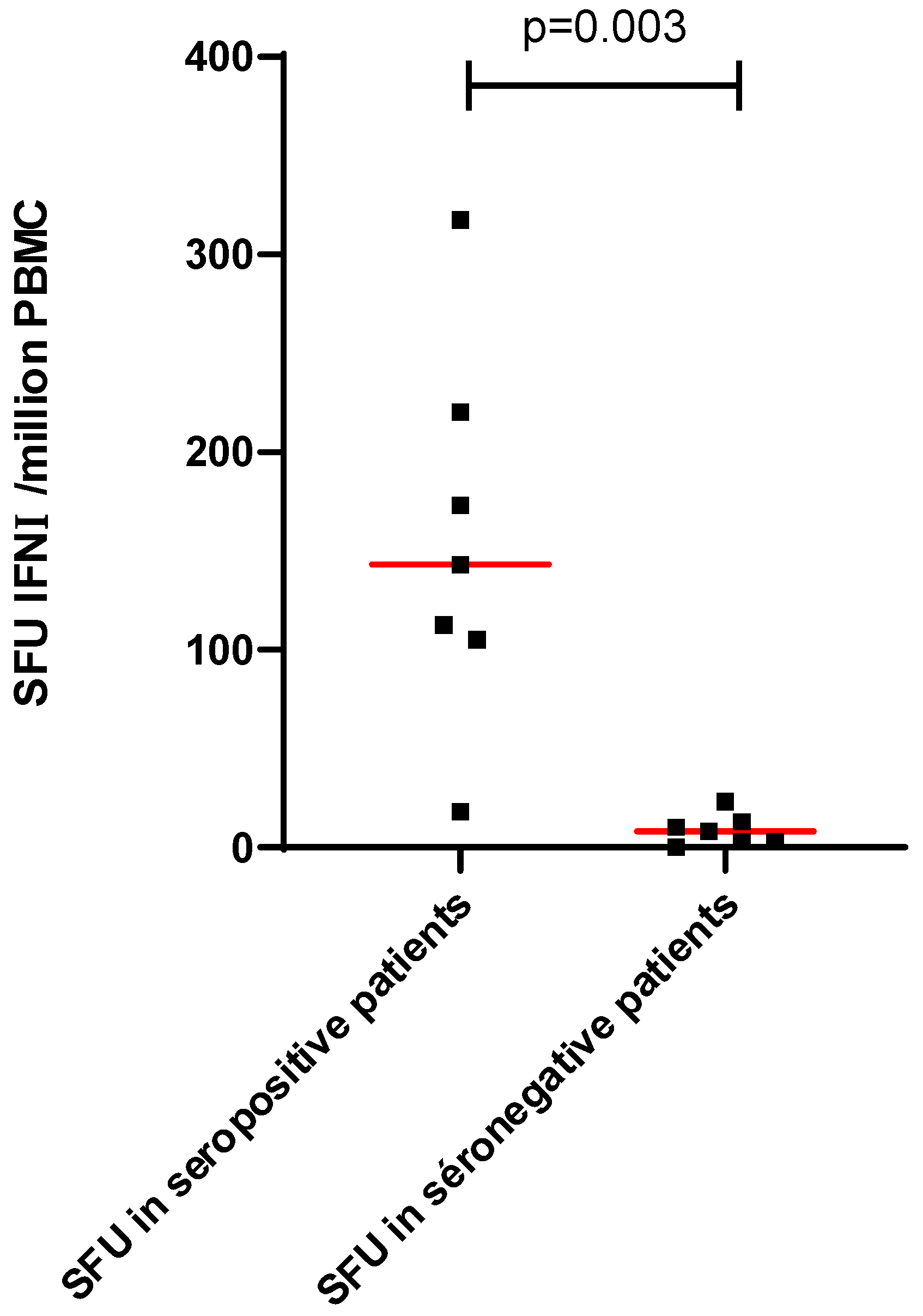
3.2. T-Cell Response
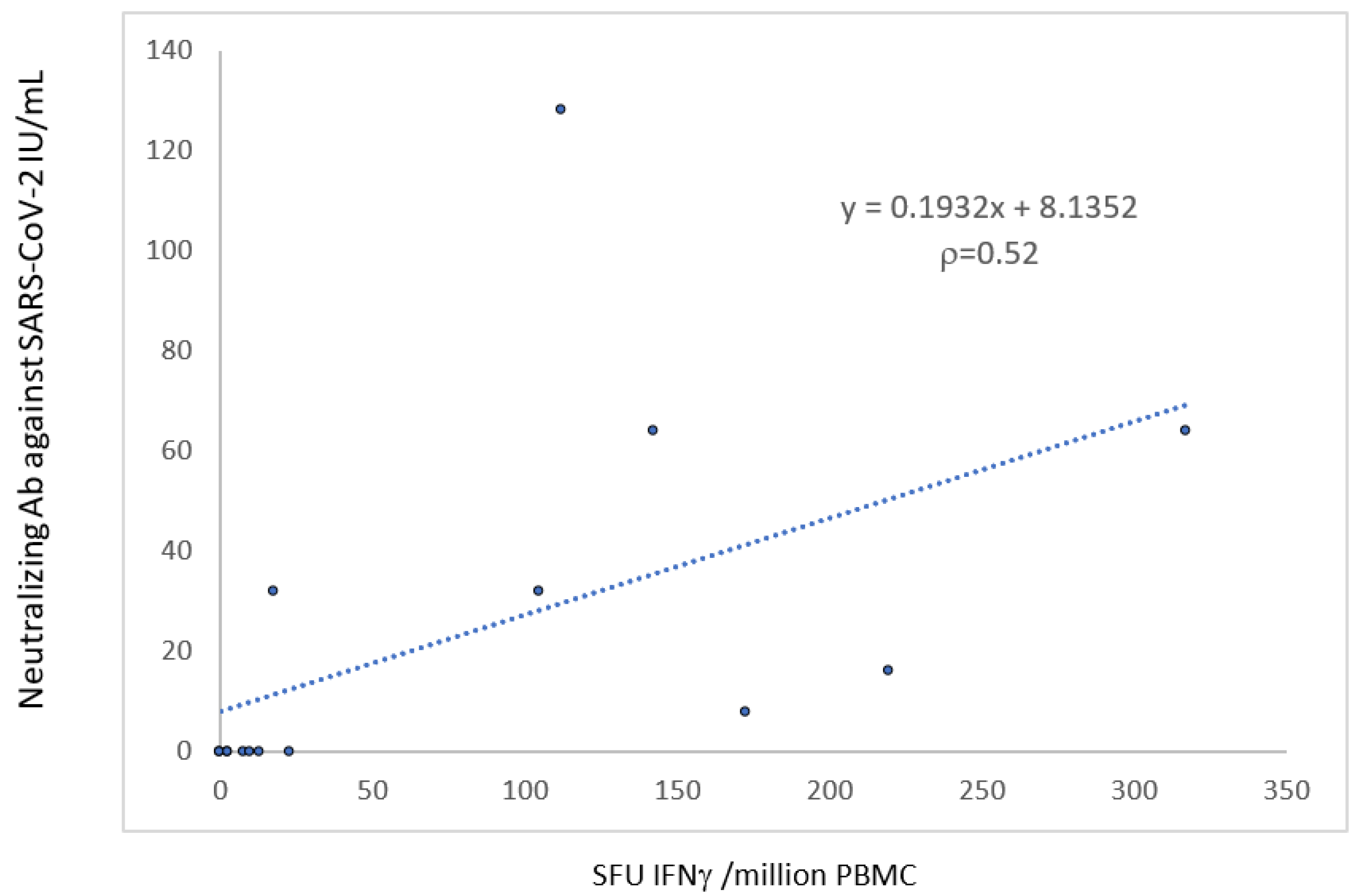
3.3. Factors Associated with an Immune Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kremer, D.; Pieters, T.T.; Verhaar, M.C.; Berger, S.P.; Bakker, S.J.L.; van Zuilen, A.D.; Joles, J.A.; Vernooij, R.W.M.; van Balkom, B.W. A systematic review and meta-analysis of COVID-19 in kidney transplant recipients: Lessons to be learned. Am. J. Transplant. 2021, 21, 3936–3945. [Google Scholar] [CrossRef]
- Marion, O.; Del Bello, A.; Abravanel, F.; Couat, C.; Faguer, S.; Esposito, L.; Hebral, A.L.; Izopet, J.; Kamar, N. Safety and Immunogenicity of Anti-SARS-CoV-2 Messenger RNA Vaccines in Recipients of Solid Organ Transplants. Ann. Intern. Med. 2021, 174, 1336–1338. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.L. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef]
- Del Bello, A.; Abravanel, F.; Marion, O.; Couat, C.; Esposito, L.; Lavayssière, L.; Izopet, J.; Kamar, N. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am. J. Transplant. 2021, 22, 322–323. [Google Scholar] [CrossRef]
- Marion, O.; Del Bello, A.; Abravanel, F.; Faguer, S.; Esposito, L.; Hebral, A.L.; Bellière, J.; Izopet, J.; Kamar, N. Predictive factors for humoral response after 2-doses of anti-SARS-CoV-2 vaccine in solid-organ-transplant patients. Transplant. Direct. 2021, 8, e1248. [Google Scholar] [CrossRef]
- Noble, J.; Jouve, T.; Janbon, B.; Rostaing, L.; Malvezzi, P. Belatacept in kidney transplantation and its limitations. Expert Rev. Clin. Immunol. 2019, 15, 359–367. [Google Scholar] [CrossRef]
- DGS-URGENT N°2021_43—Vaccins Contre la COVID-19: Modalites D’Administrationdes Rappels. Available online: https://www.mesvaccins.net/textes/dgs_urgent_n43_vaccination_modalites_d_administration_des_rappels.pdf (accessed on 23 February 2022).
- Dimeglio, C.; Herin, F.; Martin-Blondel, G.; Miedougé, M.; Izopet, J. Antibody titers and protection against a SARS-CoV-2 infection. J. Infect. 2021, 84, 248–288. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Romieu-Mourez, R.; Couat, C.; Del Bello, A.; Izopet, J. Assessment of 4 Doses of SARS-CoV-2 Messenger RNA–Based Vaccine in Recipients of a Solid Organ Transplant. JAMA Netw. Open 2021, 4, e2136030. [Google Scholar] [CrossRef]
- Ou, M.T.; Boyarsky, B.J.; Chiang, T.P.Y.; Bae, S.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity and Reactogenicity After SARS-CoV-2 mRNA Vaccination in Kidney Transplant Recipients Taking Belatacept. Transplantation 2021, 105, 2119–2123. [Google Scholar] [CrossRef] [PubMed]
- Chavarot, N.; Morel, A.; Leruez-Ville, M.; Villain, E.; Divard, G.; Burger, C.; Serris, A.; Sberro-Soussan, R.; Martinez, F.; Amrouche, L.; et al. Weak antibody response to three doses of mRNA vaccine in kidney transplant recipients treated with belatacept. Am. J. Transplant. 2021, 21, 4043–4051. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.; Langello, A.; Bouchut, W.; Lupo, J.; Lombardo, D.; Rostaing, L. Immune Response Post-SARS-CoV-2 mRNA Vaccination in Kidney Transplant Recipients Receiving Belatacept. Transplantation 2021, 105, e259–e260. [Google Scholar] [CrossRef]
- Cucchiari, D.; Egri, N.; Bodro, M.; Herrera, S.; Del Risco-Zevallos, J.; Casals-Urquiza, J.; Cofan, F.; Moreno, A.; Rovira, J.R.; Banon-Maneus, E.; et al. Cellular and humoral response after MRNA-1273 SARS-CoV-2 vaccine in kidney transplant recipients. Am. J. Transplant. 2021, 21, 2727–2739. [Google Scholar] [CrossRef] [PubMed]
- Herrera, S.; Colmenero, J.; Pascal, M.; Escobedo, M.; Castel, M.A.; Sole-González, E.; Palou, E.; Egri, N.; Ruiz, P.; Mosquera, M.; et al. Cellular and humoral immune response after mRNA-1273 SARS-CoV-2 vaccine in liver and heart transplant recipients. Am. J. Transplant. 2021, 21, 3971–3979. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D. Humoral and cellular immune response and safety of two-dose SARS-CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3980–3989. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Hamzaoui, M.; Lemée, V.; Lamulle, J.; Hanoy, M.; Laurent, C.; Lebourg, L.; Etienne, I.; Lemoine, M.; Le Roy, F.; et al. Antibody and T Cell Response to SARS-CoV-2 Messenger RNA BNT162b2 Vaccine in Kidney Transplant Recipients and Hemodialysis Patients. J. Am. Soc. Nephrol. 2021, 32, 2147–2152. [Google Scholar] [CrossRef]
- Leibler, C.; Thiolat, A.; Hénique, C.; Samson, C.; Pilon, C.; Tamagne, M.; Pirenne, F.; Vingert, B.; Cohen, J.L.; Grimbert, P. Control of Humoral Response in Renal Transplantation by Belatacept Depends on a Direct Effect on B Cells and Impaired T Follicular Helper-B Cell Crosstalk. J. Am. Soc. Nephrol. 2018, 29, 1049–1062. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 COVID-19 vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Gallo, E.; Abbasciano, I.; Mingozzi, S.; Lavacca, A.; Presta, R.; Bruno, S.; Deambrosis, I.; Barreca, A.; Romagnoli, R.; Mella, A.; et al. Prevention of acute rejection after rescue with Belatacept by association of low-dose Tacrolimus maintenance in medically complex kidney transplant recipients with early or late graft dysfunction. PLoS ONE 2020, 15, e0240335. [Google Scholar] [CrossRef]
- Bruminhent, J.; Setthaudom, C.; Chaumdee, P.; Boongird, S.; Kiertiburanakul, S.; Malathum, K.; Nongnuch, A.; Phuphuakrat, A.; Jirasiritham, S.; Janphram, C.; et al. The Ramathibodi Transplant Infectious Diseases (RTID) Study Group. SARS-CoV-2-specific humoral and cell-mediated immune responses after immunization with inactivated COVID-19 vaccine in kidney transplant recipients (CVIM 1 study). Am. J. Transplant. 2021. online ahead of print. [Google Scholar]
- Tylicki, L.; Alicja Debska-Slizie, A.; Muchlado, M.; Ślizień, Z.; Gołębiewska, J.; Dąbrowska, M.; Biedunkiewicz, B. Boosting Humoral Immunity from mRNA COVID-19 Vaccines in Kidney Transplant Recipients. Vaccines 2022, 10, 56. [Google Scholar] [CrossRef] [PubMed]
- RONAPREVE (Casirivimab-Imdevimab) (Prophylaxie Pré-Exposition de L’Infection à SARS-CoV-2). Available online: https://www.has-sante.fr/jcms/p_3281544/fr/ronapreve-casirivimab-imdevimab-prophylaxie-pre-exposition-de-l-infection-a-sars-cov-2 (accessed on 23 February 2022).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Responders (N = 16) | Non-Responders (N = 52) | p-Value | |
|---|---|---|---|
| Sex ratio (M/F) | 4.3 (13/3) | 2.3 (36/16) | 0.53 |
| Age (years, mean ± SEM) | 55 ± 3 | 63 ± 2 | 0.02 |
| Type of organ transplant, n (%) Kidney Heart | |||
| 16 (100) | 46 (88) | 0.32 | |
| - | 6 (12) | ||
| History of rejection in the year preceding vaccination, n (%) | 0 (0) | 5 (10) | 0.33 |
| Time between vaccine and transplantation (months, mean ± SEM) | 132 ± 24 | 80 ± 12 | 0.01 |
| No induction therapy, n (%) Induction therapy, n (%) Anti-IL2 receptor Thymoglobulin | 5 (31) | 22 (42) | 0.56 |
| 11 (69) | 30 (58) | ||
| 8 (73) | 17 (57) | ||
| 3 (27) | 13 (43) | ||
| Type of immunosuppressive regimen, n (%) Tacrolimus Antimetabolite Mycophenolic acid Azathioprine mTOR inhibitors Steroids | |||
| 0 (0) | 18 (35) | <0.01 | |
| 10 (63) | 32 (61) | 1 | |
| 9 | 31 | ||
| 1 | 1 | ||
| 5 (31) | 13 (25) | 0.75 | |
| 13 (81) | 48 (92) | 0.34 | |
| Neutrophil count (/mm3, mean ± SEM) | 5250 ± 509 | 6009 ± 474 | 0.55 |
| Lymphocyte count (/mm3, mean ± SEM) | 1850 ± 215 | 1201 ± 90 | <0.01 |
| CD4+ T-cell count (/mm3, mean ± SEM) | n = 13 | n = 32 | <0.001 |
| 671 ± 61 | 325 ± 33 | ||
| CD8+ T-cell count (/mm3, mean ± SEM) | n = 13 | n = 32 | 0.10 |
| 634 ± 135 | 351 ± 37 | ||
| CD19+ T-cell count (/mm3, mean ± SEM) | n = 13 | n = 33 | 0.03 |
| 120 ± 27 | 93 ± 30 | ||
| NK cell count (/mm3, mean ± SEM) | n = 13 | n = 33 | 0.53 |
| 284 ± 52 | 233 ± 29 | ||
| eGFR (mL/min/1.73 m2) Kidney transplant eGFR Non-kidney transplant eGFR | 63 ± 7 | 42 ± 3 | 0.02 |
| 63 ± 7 | 41 ± 3 | 0.01 | |
| - | 53 ± 12 | - | |
| Positive anti-SARSCoV2 antibodies before vaccination | 0 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abravanel, F.; Marion, O.; Del Bello, A.; Beunon, T.; Romieu-Mourez, R.; Couat, C.; Pucelle, M.; Staes, L.; Guitard, J.; Esposito, L.; et al. Humoral and Cellular Immune Responses of Solid Organ Transplant Patients on Belatacept to Three Doses of mRNA-Based Anti-SARS-CoV-2 Vaccine. Vaccines 2022, 10, 354. https://doi.org/10.3390/vaccines10030354
Abravanel F, Marion O, Del Bello A, Beunon T, Romieu-Mourez R, Couat C, Pucelle M, Staes L, Guitard J, Esposito L, et al. Humoral and Cellular Immune Responses of Solid Organ Transplant Patients on Belatacept to Three Doses of mRNA-Based Anti-SARS-CoV-2 Vaccine. Vaccines. 2022; 10(3):354. https://doi.org/10.3390/vaccines10030354
Chicago/Turabian StyleAbravanel, Florence, Olivier Marion, Arnaud Del Bello, Thomas Beunon, Raphaelle Romieu-Mourez, Chloé Couat, Mélanie Pucelle, Laetitia Staes, Joelle Guitard, Laure Esposito, and et al. 2022. "Humoral and Cellular Immune Responses of Solid Organ Transplant Patients on Belatacept to Three Doses of mRNA-Based Anti-SARS-CoV-2 Vaccine" Vaccines 10, no. 3: 354. https://doi.org/10.3390/vaccines10030354
APA StyleAbravanel, F., Marion, O., Del Bello, A., Beunon, T., Romieu-Mourez, R., Couat, C., Pucelle, M., Staes, L., Guitard, J., Esposito, L., Faguer, S., Kamar, N., & Izopet, J. (2022). Humoral and Cellular Immune Responses of Solid Organ Transplant Patients on Belatacept to Three Doses of mRNA-Based Anti-SARS-CoV-2 Vaccine. Vaccines, 10(3), 354. https://doi.org/10.3390/vaccines10030354