
Evaluation and Validation of the Roche Elecsys SARS-CoV-2 Antigen Electro-Chemiluminescent Immunoassay in a Southeast Asian Region



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Materials and Methods
2.3. Statistical Analysis
3. Results
3.1. Performance Evaluation
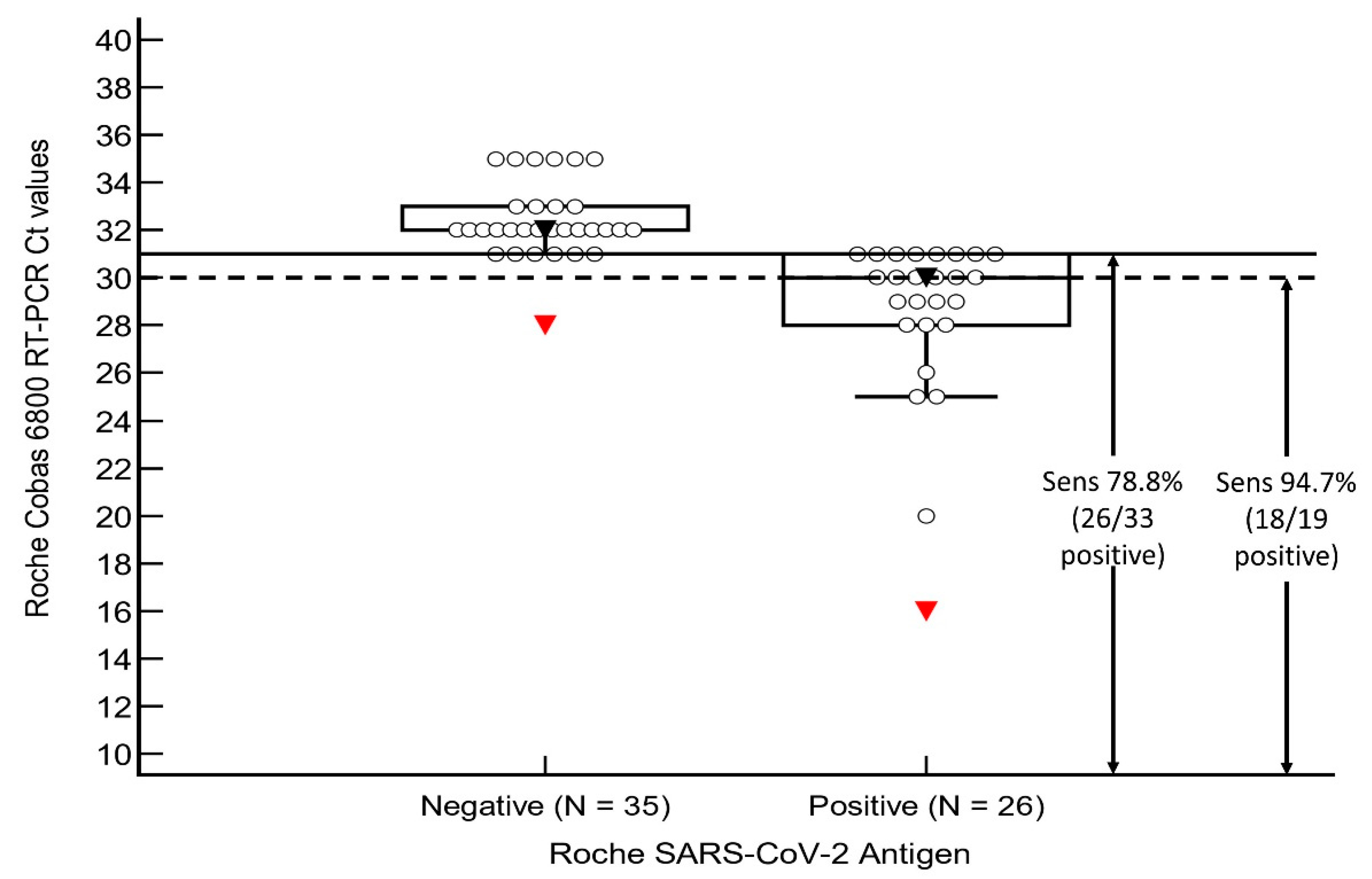
3.2. Sensitivity and Specificity Analysis
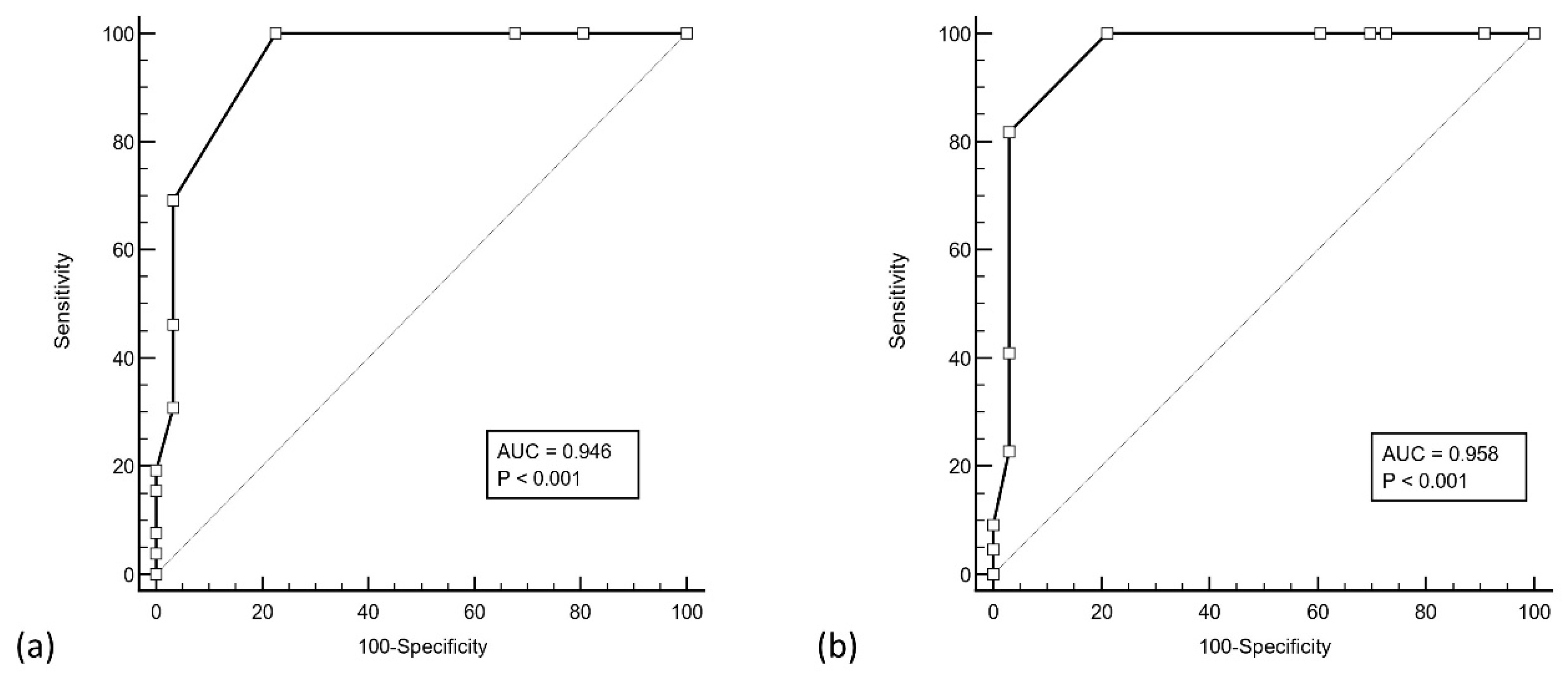
3.3. ROC Analysis
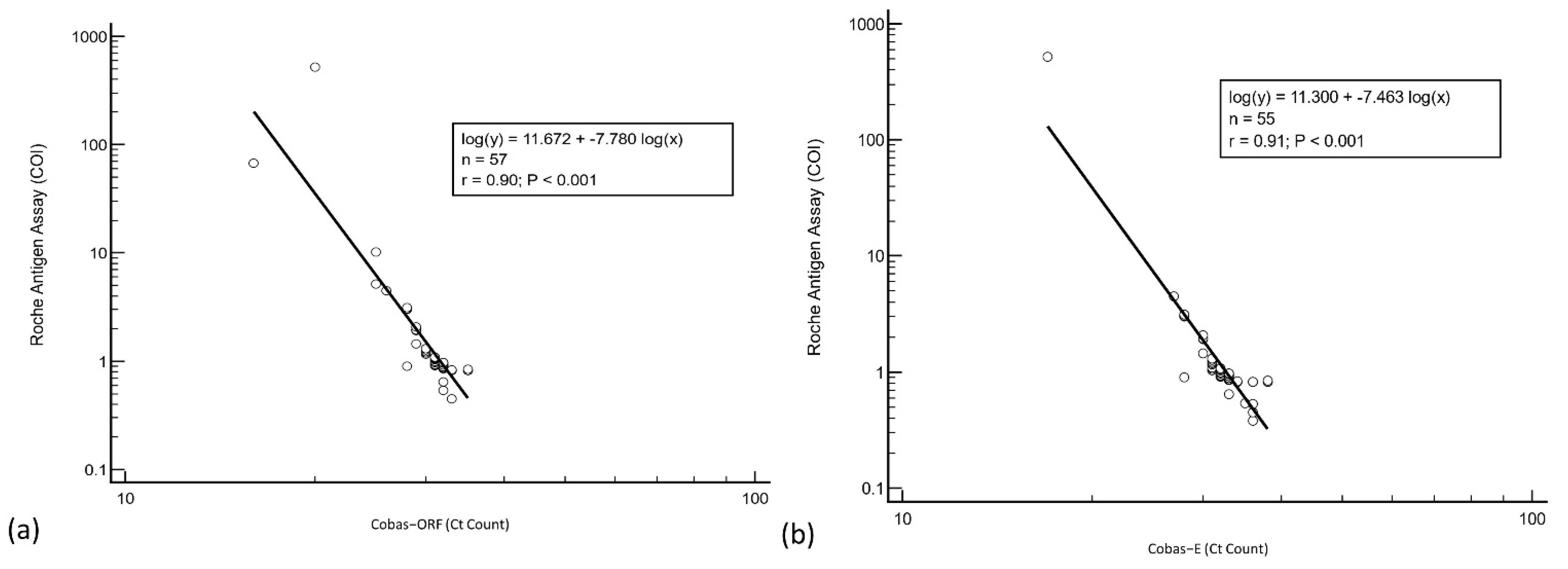
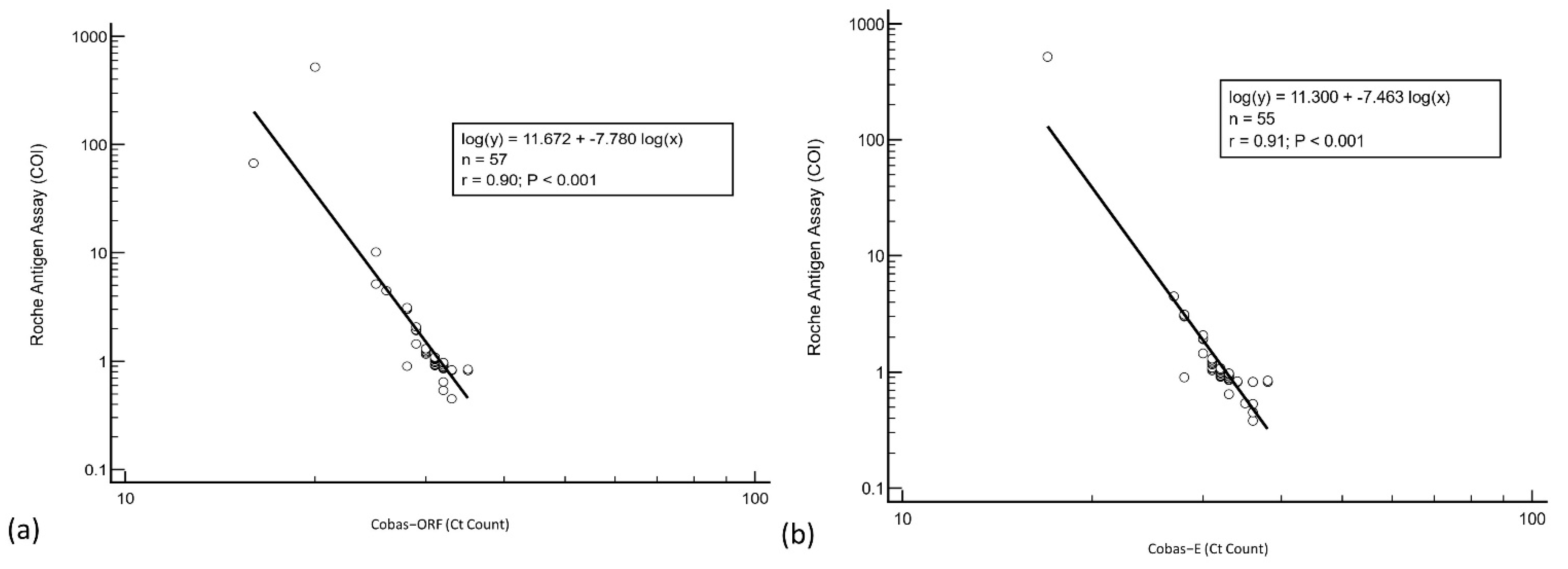
3.4. Regression Analysis
3.5. Validation Group Analysis
4. Discussion
- The sensitivity of the Roche antigen assay can be improved when used in patients with high viral loads; sensitivity exceeds 90% in cases with Ct ≤ 30;
- The antigen assay has a good agreement with the RT-PCR Ct values;
- The antigen assay is most sensitive in the first week after the first positive RT-PCR.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RT-PCR | Reverse transcription–polymerase chain reaction |
| LFIA | Lateral flow immunoassay |
| CI | Confidence interval |
| Ct | Cycle threshold |
| COI | Cut-off index |
| ROC | Receiver Operating Characteristic |
| AUC | Area Under Curve |
References
- World Health Organization. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Interim Guidance. 19 March 2020. Available online: https://www.who.int/publications/i/item/10665-331501 (accessed on 5 January 2022).
- Norz, D.; Grunwald, M.; Olearo, F.; Fischer, N.; Aepfelbacher, M.; Pfefferle, S.; Lutgehetmann, M. Evaluation of a fully automated high-throughput SARS-CoV-2 multiplex qPCR assay with built-in screening functionality for del-HV69/70- and N501Y variants such as B.1.1.7. J. Clin. Virol. 2021, 141, 104894. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Interim Guidance for Antigen Testing for SARS-CoV-2. Updated 14 June 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html (accessed on 4 January 2022).
- Centers for Disease Control and Prevention. SARS-CoV-2 Antigen Testing in Long Term Care Facilities, Considerations for Use in Nursing Homes and Other Long-Term Care Facilities. Updated 7 January 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/nursing-homes-antigen-testing.html (accessed on 4 January 2022).
- World Health Organization. WHO Emergency Use Listing for In Vitro Diagnostics (IVDs) Detecting SARS-CoV-2. Available online: https://extranet.who.int/pqweb/sites/default/files/documents/211125_EUL_SARS-CoV-2_products_list.pdf (accessed on 25 January 2022).
- Anais, S.; Anantharajah, A.; Bodeus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J. Clin. Virol. 2020, 129, 104455. [Google Scholar]
- Lanser, L.; Bellmann-Weiler, R.; Ottl, K.W.; Huber, L.; Griesmacher, A.; Theurl, I.; Weiss, G. Evaluating the clinical utility and sensitivity of SARS-CoV-2 antigen testing in relation to RT-PCR Ct values. Infection 2021, 49, 555–557. [Google Scholar] [CrossRef] [PubMed]
- Olearo, F.; Norz, D.; Heinrich, F.; Sutter, J.P.; Roedl, K.; Schultze, A.; Wiesch, J.S.Z.; Platon, B.; Oestereich, L.; Kreuels, B.; et al. Handling and accuracy of four rapid antigen tests for the diagnosis of SARS-CoV-2 compared to RT-qPCR. J. Clin. Virol. 2021, 137, 104782. [Google Scholar] [CrossRef] [PubMed]
- Merino-Amador, P.; Gonzalez-Donapetry, P.; Dominguez-Fernandez, M.; Gonzalez-Romo, F.; Sanchez-Castellano, M.A.; Seoane-Estevez, A.; Delgado-Iribarren, A.; Garcia, J.; Bou, G.; Cuenca-Estrella, M.; et al. Clinitest rapid COVID-19 antigen test for the diagnosis of SARS-CoV-2 infection: A multicenter evaluation study. J. Clin. Virol. 2021, 143, 104961. [Google Scholar] [CrossRef] [PubMed]
- Linares, M.; Perez-Tanoira, R.; Carrero, A.; Romanyk, J.; Perez-Garcia, F.; Gomez-Herruz, P.; Arroyo, T.; Cuadros, J. Panbio antigen rapid test is reliable to diagnose SARS-CoV-2 infection in the first 7 days after the onset of symptoms. J. Clin. Virol. 2020, 133, 104659. [Google Scholar] [CrossRef] [PubMed]
- US Food & Drug Administration. QIAreach SARS-CoV-2 Antigen Test—Letter of Authorization. 5 August 2021. Available online: https://www.fda.gov/media/151380/download (accessed on 5 January 2022).
- Clinical and Laboratory Standards Institute. EP12-A2: User protocol for evaluation of qualitative test performance. In Approved Guideline, 2nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Zhang, Z.; Bi, Q.; Fang, S.; Wei, L.; Wang, X.; He, J.; Wu, Y.; Liu, X.; Gao, W.; Zhang, R.; et al. Insight into the practical performance of RT-PCR testing for SARS-CoV-2 using serological data: A cohort study. Lancet Microbe 2021, 2, e79–e87. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Mina, M.; Parker, R.; Larremore, D.B. Rethinking COVID-19 test sensitivity—A strategy for containment. N. Engl. J. Med. 2020, 383, e120. [Google Scholar] [CrossRef]
- Hirotsu, Y.; Maejima, M.; Shibusawa, M.; Nagakubo, Y.; Hosaka, K.; Amemiya, K.; Sueki, H.; Hayakawa, M.; Mochizuki, H.; Tsutsui, T.; et al. Comparison of automated SARS-CoV-2 antigen test for COVID-19 infection with quantitative RT-PCR using 313 nasopharyngeal swabs, including from seven serially followed patients. Int. J. Infect. Dis. 2020, 99, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Osterman, A.; Iglhaut, M.; Lehner, A.; Spath, P.; Stern, M.; Autenrieth, H.; Muenchhoff, M.; Graf, A.; Krebs, S.; Blum, H.; et al. Comparison of four commercial, automated antigen tests to detect SARS-CoV-2 variants of concern. Med. Microbiol. Immunol. 2021, 210, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Hauser, F.; Sprinzl, M.F.; Dreis, K.J.; Renzaho, A.; Youhanen, S.; Kremer, W.M.; Podlech, J.; Galle, P.R.; Lackner, K.J.; Rossmann, H.; et al. Evaluation of a laboratory-based high-throughput SARS-CoV-2 antigen assay for non-COVID-19 patient screening at hospital admission. Med. Microbiol. Immunol. 2021, 210, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Blitz, L.T.A.; Klausner, J.D. A real-world comparison of SARS-CoV-2 rapid antigen testing versus PCR testing in Florida. J. Clin. Microbiol. 2021, 59, e0110721. [Google Scholar]
- Yokota, I.; Sakurazawa, T.; Sugita, J.; Iwasaki, S.; Yasuda, K.; Yamashita, N.; Fujisawa, S.; Nishida, M.; Konno, S.; Teshima, T. Performance of qualitative and quantitative antigen tests for SARS-CoV-2 using saliva. Infect. Dis. Rep. 2021, 13, 69. [Google Scholar] [CrossRef] [PubMed]
- Fourati, S.; Soulier, A.; Gourgeon, A.; Khouider, S.; Langlois, C.; Galbin, A.; Bouter, A.L.; Rodriguez, C.; Joanny, M.; Dublineau, A.; et al. Performance of a high-throughput, automated enzyme immunoassay for the detection of SARS-CoV-2 antigen, including in viral “variants of concern”: Implications for clinical use. J. Clin. Virol. 2021, 146, 105048. [Google Scholar] [CrossRef] [PubMed]
- Nomoto, H.; Yamamoto, K.; Yamada, G.; Suzuki, M.; Kinoshita, N.; Takasaki, J.; Moriya, A.; Maeda, K.; Kimura, M.; Ohmagari, N. Time-course evaluation of the quantitative antigen test for severe acute respiratory syndrome coronavirus 2: The potential contribution to alleviating isolation of COVID-19 patients. J. Infect. Chemother. 2021, 27, 1669–1673. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, C.S.; Phua, S.K.; Hoo, S.P.; Jiang, B.; Aw, T.-C. Evaluation and Validation of the Roche Elecsys SARS-CoV-2 Antigen Electro-Chemiluminescent Immunoassay in a Southeast Asian Region. Vaccines 2022, 10, 198. https://doi.org/10.3390/vaccines10020198
Lau CS, Phua SK, Hoo SP, Jiang B, Aw T-C. Evaluation and Validation of the Roche Elecsys SARS-CoV-2 Antigen Electro-Chemiluminescent Immunoassay in a Southeast Asian Region. Vaccines. 2022; 10(2):198. https://doi.org/10.3390/vaccines10020198
Chicago/Turabian StyleLau, Chin Shern, Soon Kieng Phua, See Ping Hoo, Boran Jiang, and Tar-Choon Aw. 2022. "Evaluation and Validation of the Roche Elecsys SARS-CoV-2 Antigen Electro-Chemiluminescent Immunoassay in a Southeast Asian Region" Vaccines 10, no. 2: 198. https://doi.org/10.3390/vaccines10020198
APA StyleLau, C. S., Phua, S. K., Hoo, S. P., Jiang, B., & Aw, T.-C. (2022). Evaluation and Validation of the Roche Elecsys SARS-CoV-2 Antigen Electro-Chemiluminescent Immunoassay in a Southeast Asian Region. Vaccines, 10(2), 198. https://doi.org/10.3390/vaccines10020198