
Persistence of Immunity in Adults after 1, 5 and 10 Years with Recombinant Hepatitis B Vaccine in Beijing in 2010–2020

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Participants
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Demography and Hepatitis B Virus Serological Test Results of Participants
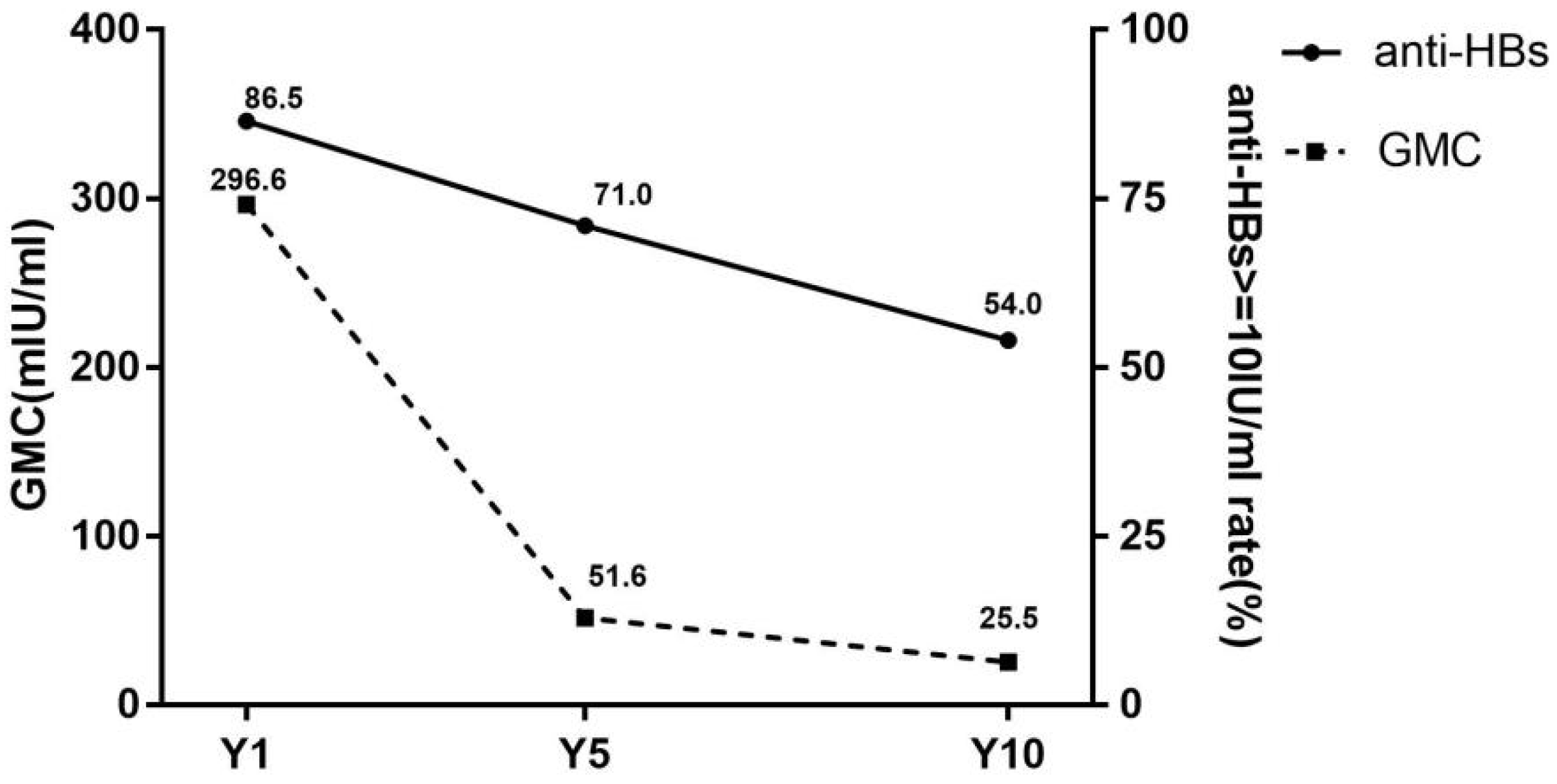
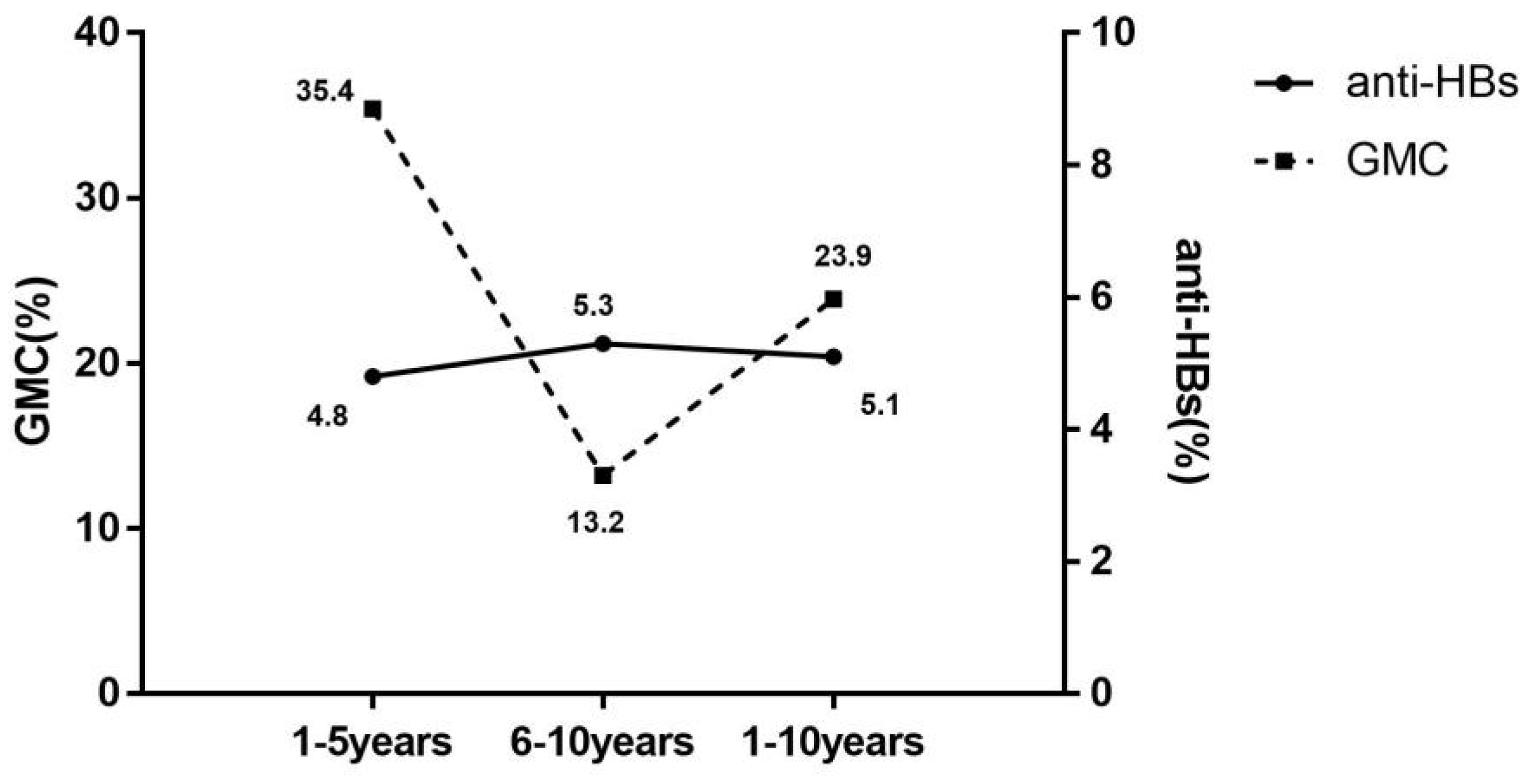
3.2. Immune Persistence
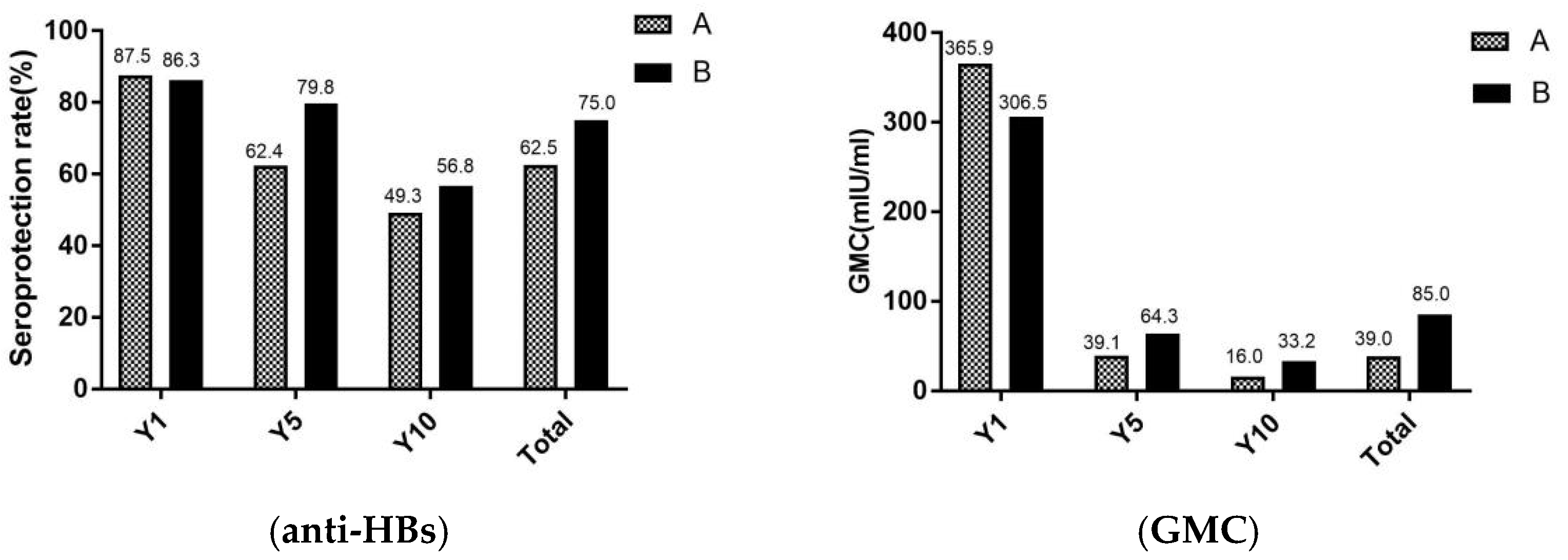
3.3. Effectiveness of Immunization against Hepatitis B of Adults in Different Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liang, T.J. Hepatitis B: The virus and disease. Hepatology 2009, 49, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Trépo, C.; Chan, H.L.; Lok, A. Hepatitis B virus infection. Lancet 2014, 384, 2053–2063. [Google Scholar] [CrossRef]
- Chinese Society of Infectious Diseases, Chinese Medical Association; Chinese Society of Hepatology, Chinese Medical Association. The guidelines of prevention and treatment for chronic hepatitis B (2019 version). Zhonghua Gan Zang Bing Za Zhi 2019, 27, 938–961. (In Chinese) [Google Scholar]
- World Health Organization. Global Hepatitis Report. 2017. Available online: https://www.who.int/publications/i/item/global-hepatitis-report-2017 (accessed on 27 November 2021).
- Guan, Z.Q.; Dong, Z.H.; Wang, Q.H.; Cao, D.X.; Fang, Y.Y.; Liu, H.T.; Iloeje, U.H. Cost of chronic hepatitis B infection in China. J. Clin. Gastroenterol. 2004, 38, S175–S178. [Google Scholar]
- Marshall, H.; Nolan, T.; Díez Domingo, J.; Rombo, L.; Sokal, E.M.; Marès, J.; Casanovas, J.M.; Kuriyakose, S.; Leyssen, M.; Jacquet, J.M. Long-term (5-year) antibody persistence following two- and three-dose regimens of a combined hepatitis A and B vaccine in children aged 1–11 years. Vaccine 2010, 28, 4411–4415. [Google Scholar] [CrossRef]
- Ren, W.; Ren, J.; Wu, Z.; Shen, L.; Shan, H.; Dai, X.; Li, J.; Liu, Y.; Qiu, Y.; Yao, J.; et al. Long-term persistence of anti-HBs after hepatitis B vaccination among isolated anti-HBc positive adults in China: 8-years results. Hum. Vaccin. Immunother. 2020, 16, 687–692. [Google Scholar] [CrossRef]
- Zhou, Y.H.; Wu, C.; Zhuang, H. Vaccination against hepatitis B: The Chinese experience. Chin. Med. J. (Engl.) 2009, 122, 98–102. [Google Scholar]
- Cui, F.; Shen, L.; Li, L.; Wang, H.; Wang, F.; Bi, S.; Liu, J.; Zhang, G.; Wang, F.; Zheng, H. Prevention of Chronic Hepatitis B after 3 Decades of Escalating Vaccination Policy, China. Emerg. Infect Dis. 2017, 23, 765–772. [Google Scholar] [CrossRef]
- Liang, X.; Bi, S.; Yang, W.; Wang, L.; Cui, G.; Cui, F.; Zhang, Y.; Liu, J.; Gong, X.; Chen, Y.; et al. Epidemiological serosurvey of hepatitis B in China--declining HBV prevalence due to hepatitis B vaccination. Vaccine 2009, 27, 6550–6557. [Google Scholar] [CrossRef]
- Wu, Z.; Bao, H.; Yao, J.; Chen, Y.; Lu, S.; Li, J.; Jiang, Z.G.; Ren, J.J.; Xu, K.J.; Ruan, B.; et al. Suitable hepatitis B vaccine for adult immunization in China: A systematic review and meta-analysis. Hum. Vaccin. Immunother. 2019, 15, 220–227. [Google Scholar] [CrossRef]
- Cui, F.Q.; Chinese Prevention Medicine Association, National Immunization Program, Chinese Center for Disease Control Prevention. Technical guide for adult hepatitis B immunization in China. Zhonghua Liu Xing Bing Xue Za Zhi 2011, 32, 1199–1203. (In Chinese) [Google Scholar] [PubMed]
- Wu, Q.; Zhuang, G.H.; Wang, X.L.; Wang, L.R.; Li, N.; Zhang, M. Antibody levels and immune memory 23 years after primary plasma-derived hepatitis B vaccination: Results of a randomized placebo-controlled trial cohort from China where endemicity is high. Vaccine 2011, 29, 2302–2307. [Google Scholar] [CrossRef]
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Zanis, C.; Thompson, G.; Rea, L.; Toomey, M.; Townshend-Bulson, L.; Rudolph, K.; Bulkow, L.; et al. Antibody Levels and Protection After Hepatitis B Vaccine: Results of a 30-Year Follow-up Study and Response to a Booster Dose. J. Infect. Dis. 2016, 214, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, P.; Dionne, M.; Leroux-Roels, G.; Van Der Meeren, O.; Di Paolo, E.; Salaun, B.; Surya Kiran, P.; Folschweiller, N. Persistence of HBsAg-specific antibodies and immune memory two to three decades after hepatitis B vaccination in adults. J. Viral Hepat. 2019, 26, 1066–1075. [Google Scholar] [CrossRef] [PubMed]
- McMahon, B.J.; Dentinger, C.M.; Bruden, D.; Zanis, C.; Peters, H.; Hurlburt, D.; Bulkow, L.; Fiore, A.E.; Bell, B.P.; Hennessy, T.W. Antibody levels and protection after hepatitis B vaccine: Results of a 22-year follow-up study and response to a booster dose. J. Infect. Dis. 2009, 200, 1390–1396. [Google Scholar] [CrossRef]
- Zhao, X.Y.; Gao, P.; Wang, H.; Wang, L.; Wu, J. Anti-HBs level in 15 years after vaccination in adults and newborns. Basic Clin. Med. 2017, 37, 808–811. (In Chinese) [Google Scholar]
- Wu, W.L.; Yan, B.Y.; Lyu, J.J.; Liu, J.Y.; Feng, Y.; Chen, S.Y.; Zhou, L.B.; Liang, X.F.; Cui, F.Q.; Wang, F.Z.; et al. Antibody persistence following primary vaccination with hepatitis B vaccine among normal and high-responder adults: A 5-year follow-up study. Zhonghua Yu Fang Yi Xue Za Zhi 2016, 50, 484–490. (In Chinese) [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Acute hepatitis B among children and adolescents--United States, 1990–2002. MMWR Morb. Mortal. Wkly. Rep. 2004, 53, 1015–1018. [Google Scholar]
- Ayerbe, M.C.; Pérez-Rivilla, A.; ICOVAHB group. Assessment of long-term efficacy of hepatitis B vaccine. Eur. J. Epidemiol. 2001, 17, 150–156. [Google Scholar] [CrossRef]
- Feng, Y.; Lv, J.J.; Cao, C.Z.; Meng, X.; Liang, X.F.; Wang, F.Z.; Xv, A.Q.; Yan, B.Y.; Zhang, L. Antibody persistence following primary vaccination with hepatitis B vaccine among normal and high-response adults: A 9-year follow-up study. Prev. Med. Trib. 2021, 27, 401–405. (In Chinese) [Google Scholar]
- Ghorbani, G.A.; Alavian, S.M.; Ghadimi, H.R. Long term effects of one or two doses of hepatitis B vaccine in adults after five years. Pak. J. Biol. Sci. 2008, 11, 660–663. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wang, Z.Z.; Gao, Y.H.; Wang, P.; Wei, L.; Xie, C.P.; Yang, Z.X.; Lan, J.; Fang, Z.L.; Zeng, Y.; Yan, L.; et al. Comparison of immunogenicity between hepatitis B vaccines with different dosages and schedules among healthy young adults in China: A 2-year follow-up study. Hum. Vaccin. Immunother. 2018, 14, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Lv, J.; Liu, J.; Yan, B.; Feng, Y.; Xu, A.; Zhang, L. Persistence of immune memory among adults with normal and high antibody response to primary hepatitis B vaccination: Results from a five-year follow-up study in China. Hum. Vaccin. Immunother. 2018, 14, 2485–2490. [Google Scholar] [CrossRef] [PubMed]
- Katoonizadeh, A.; Sharafkhah, M.; Ostovaneh, M.R.; Norouzi, A.; Khoshbakht, N.; Mohamadkhani, A.; Eslami, L.; Gharravi, A.; Shayanrad, A.; Khoshnia, M.; et al. Immune responses to hepatitis B immunization 10–18 years after primary vaccination: A population-based cohort study. J. Viral Hepatol. 2016, 23, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, P.; Leroux-Roels, G.; Crasta, P.; Messier, M.; Jacquet, J.M.; Van Herck, K. Antibody persistence and immune memory in adults, 15 years after a three-dose schedule of a combined hepatitis A and B vaccine. J. Med. Virol. 2012, 84, 11–17. [Google Scholar] [CrossRef]
- Yuen, M.F.; Lim, W.L.; Chan, A.O.; Wong, D.K.; Sum, S.S.; Lai, C.L. 18-year follow-up study of a prospective randomized trial of hepatitis B vaccinations without booster doses in children. Clin. Gastroenterol. Hepatol. 2004, 2, 941–945. [Google Scholar]
- Coppola, N.; Corvino, A.R.; De Pascalis, S.; Signoriello, G.; Di Fiore, E.; Nienhaus, A.; Sagnelli, E.; Lamberti, M. The long-term immunogenicity of recombinant hepatitis B virus (HBV) vaccine: Contribution of universal HBV vaccination in Italy. BMC Infect Dis. 2015, 15, 149. [Google Scholar] [CrossRef]
- Wan, Y.M.; Wang, F.Z.; Zhang, G.M.; Cui, F.Q. Risk and disease burden of adult hepatitis B infection. Chin. J. Vaccines Immun. 2019, 25, 611–616. (In Chinese) [Google Scholar]
- Koc, Ö.; Van Damme, P.; Busschots, D.; Bielen, R.; Forier, A.; Nevens, F.; Robaeys, G. Acute hepatitis B notification rates in Flanders, Belgium, 2009 to 2017. Eur. Surveill. 2019, 24, 1900064. [Google Scholar] [CrossRef]
- Chaves, S.S.; Fischer, G.; Groeger, J.; Patel, P.R.; Thompson, N.D.; Teshale, E.H.; Stevenson, K.; Yano, V.M.; Armstrong, G.L.; Samandari, T.; et al. Persistence of long-term immunity to hepatitis B among adolescents immunized at birth. Vaccine 2012, 30, 1644–1649. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | n | HBsAg ≥ 0.05 IU/mL | Anti-HBs ≥ 10 IU/mL | Anti-HBc ≥ 1.00 S/CO | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Y1 | 200 | 0 | 0 | 173 | 86.5 | 2 | 1.0 |
| Gender | |||||||
| Male | 78 | 0 | 0 | 63 | 80.8 | 1 | 1.3 |
| female | 122 | 0 | 0 | 110 | 90.2 | 1 | 0.8 |
| age (95%CI) | 47.1 (45.3, 49.0) | - | 46.4 (43.5, 48.9) | 36.5 (36.0, 37.0) | |||
| Y5 | 200 | 0 | 0 | 142 | 71.0 | 6 | 3.0 |
| Gender | |||||||
| Male | 85 | 0 | 0 | 59 | 69.4 | 5 | 5.9 |
| female | 115 | 0 | 0 | 83 | 72.2 | 1 | 0.9 |
| age (95%CI) | 54.7 (52.6, 56.8) | - | 54.0 (51.2, 56.8) | 64.5 (61.0, 68.0) | |||
| Y10 | 200 | 0 | 0 | 108 | 54.0 | 7 | 3.5 |
| Gender | |||||||
| Male | 90 | 0 | 0 | 43 | 47.8 | 5 | 5.6 |
| female | 110 | 0 | 0 | 65 | 59.1 | 2 | 1.8 |
| age (95%CI) | 56.5 (55.1, 57.8) | - | 55.8 (54.0, 57.7) | 54.5 (53.0, 56.0) | |||
| Total | 600 | 0 | 0 | 423 | 70.5 | 15 | 2.5 |
| Gender | |||||||
| Male | 253 | 0 | 0 | 165 | 65.2 | 11 | 6.7 |
| female | 347 | 0 | 0 | 258 | 72.3 | 4 | 1.6 |
| age (95%CI) | 52.8 (51.6, 53.8) | - | 50.9 (49.7, 52.3) | 57.7 (50.8, 64.3) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, S.; Ge, S.; Zhang, Z.; Ma, J.; Jiao, Y.; Li, Q.; Liang, Y.; Li, S. Persistence of Immunity in Adults after 1, 5 and 10 Years with Recombinant Hepatitis B Vaccine in Beijing in 2010–2020. Vaccines 2022, 10, 181. https://doi.org/10.3390/vaccines10020181
Shen S, Ge S, Zhang Z, Ma J, Jiao Y, Li Q, Liang Y, Li S. Persistence of Immunity in Adults after 1, 5 and 10 Years with Recombinant Hepatitis B Vaccine in Beijing in 2010–2020. Vaccines. 2022; 10(2):181. https://doi.org/10.3390/vaccines10020181
Chicago/Turabian StyleShen, Sijia, Shen Ge, Zheng Zhang, Jianxin Ma, Yang Jiao, Qian Li, Yan Liang, and Shuming Li. 2022. "Persistence of Immunity in Adults after 1, 5 and 10 Years with Recombinant Hepatitis B Vaccine in Beijing in 2010–2020" Vaccines 10, no. 2: 181. https://doi.org/10.3390/vaccines10020181
APA StyleShen, S., Ge, S., Zhang, Z., Ma, J., Jiao, Y., Li, Q., Liang, Y., & Li, S. (2022). Persistence of Immunity in Adults after 1, 5 and 10 Years with Recombinant Hepatitis B Vaccine in Beijing in 2010–2020. Vaccines, 10(2), 181. https://doi.org/10.3390/vaccines10020181