
Sociodemographic Predictors Associated with the Willingness to Get Vaccinated against COVID-19 in Peru: A Cross-Sectional Survey

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Population
2.2. Variables
2.3. Procedures
2.4. Data Analysis
2.5. Ethical Aspects
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval & Informed Consent
Appendix A
- 1.
- Gender:
- □
- Male
- □
- Female
- 2.
- Age: _____ years
- 3.
- Education:
- □
- Primary school
- □
- High school
- □
- Technical degree
- □
- University degree
- □
- Postgraduate
- 4.
- Civil status:
- □
- Single
- □
- Married
- □
- Divorced
- □
- Other, specify: _____
- 5.
- Department you live in Peru:
- □
- Amazonas
- □
- Ancash
- □
- Apurimac
- □
- Arequipa
- □
- Ayacucho
- □
- Cajamarca
- □
- Callao
- □
- Cusco
- □
- Huancavelica
- □
- Huanuco
- □
- Ica
- □
- Junin
- □
- La Libertad
- □
- Lambayeque
- □
- Lima
- □
- Loreto
- □
- Madre de Dios
- □
- Moquegua
- □
- Pasco
- □
- Piura
- □
- Puno
- □
- San Martin
- □
- Tacna
- □
- Tumbes
- □
- Ucayali
- 6.
- Do you work in healthcare?
- □
- Yes
- □
- No
- 7.
- Do you have a chronic illness (diabetes, hypertension, asthma, pulmonary fibrosis, cancer)?
- □
- Yes
- □
- No
- 8.
- How many people live in your home? _____
- 9.
- Have you been sick with COVID-19?
- □
- Yes, confirmed
- □
- Yes, but not yet confirmed
- □
- No
- □
- Don’t know
- 10.
- Family or friends got infected with COVID-19?
- □
- Yes, confirmed
- □
- Yes, but not yet confirmed
- □
- No
- □
- Don’t know
- 11.
- What is your current work situation?
- □
- Employed (questions below appear if this option is selected)
- I.
- Are you working from home?
- □
- Yes
- □
- No
- II.
- Have your work hours been reduced due to the current COVID-19 pandemic?
- □
- Yes
- □
- No
- III.
- Are you worried about losing your job in the next 6 months due to the COVID-19 pandemic?
- □
- Yes
- □
- No
- □
- Unemployed (the next question appears if this option is selected)
- I.
- Is your unemployment a result of the COVID-19 pandemic?
- □
- Yes
- □
- No
- □
- Retired
- □
- Student
- 12.
- Have you been vaccinated against the flu virus (influenza or pneumococcus) in the last few months?
- □
- Yes
- □
- No
- □
- Don’t know
- 13.
- Do you plan to get vaccinated against the flu?
- □
- Yes
- □
- No
- □
- Don’t know
- 14.
- Do you plan to get vaccinated against COVID-19?
- □
- Yes (questions below appear if this option is selected)
- I.
- What is the main reason to get vaccinated?
- □
- Protect my health
- □
- Protect my family members
- II.
- If you had to choose the country of origin of the vaccine, which one would you select?
- □
- China
- □
- Germany
- □
- England
- □
- United States
- □
- Switzerland
- □
- India
- □
- Peru
- □
- Other: _____
- □
- No
- □
- Don’t know
- 15.
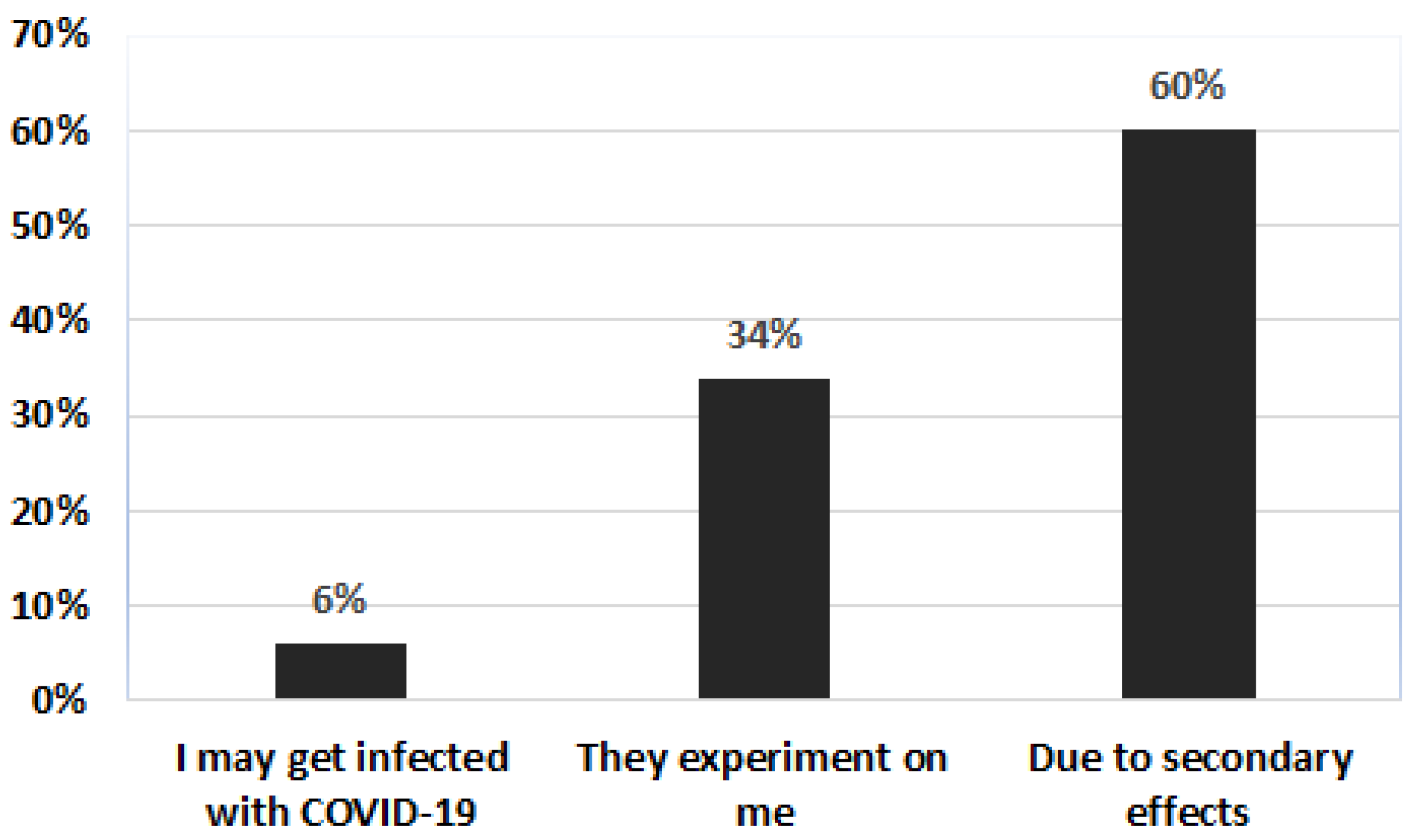
- Do you have any fear of receiving the COVID-19 vaccine?
- □
- Yes (question below appears if this option is selected)
- I.
- Why?
- □
- It can cause me some damage (secondary effect)
- □
- I can get sick from COVID-19
- □
- They are experimenting with me
- □
- No
- □
- Don’t knowKnowledge about COVID-19
- 16.
- Are you aware of the novel coronavirus/COVID-19 pandemic?
- □
- Yes
- □
- No → (this explanation pops up if this option is selected) There is a pandemic of respiratory disease caused by a novel (new) coronavirus. The disease has been named “coronavirus disease 2019” or COVID-19. Although the virus was first identified in Wuhan, Hubei Province, China, it has now spread across the globe with millions of infections and deaths.
- □
- Don’t know → (this explanation pops up if this option is selected) There is a pandemic of respiratory disease caused by a novel (new) coronavirus. The disease has been named “coronavirus disease 2019” or COVID-19. Although the virus was first identified in Wuhan, Hubei Province, China, it has now spread across the globe with millions of infections and deaths.
- 17.
- How did you learn about the novel coronavirus/COVID-19 pandemic?
- □
- Television
- □
- Newspapers/magazines
- □
- Websites
- □
- Family/friends
- □
- Healthcare professionals (For example: doctors, nurses, pharmacists or other health professionals)
- □
- Health officials (For example: Ministry of Health, Centers for Disease Control and Prevention, National Institute of Health)
- □
- Social media
- 18.
- How would you rate your knowledge level on novel coronavirus/COVID-19?
- □
- Very poor
- □
- Poor
- □
- Average
- □
- Good
- □
- Very good
- 19.
- Which of the following statements is correct about the definition of novel coronavirus/COVID-19?
- □
- The novel coronavirus/COVID-19 is a respiratory disease caused by a viral infection.
- □
- Displayed symptoms usually include respiratory symptoms accompanied by fever, but novel coronavirus/COVID-19 is not contagious
- □
- The novel coronavirus/COVID-19 can progress to a severe illness but never leads to death
- □
- Don’t know
- 20.
- Which of the following statements is correct about transmission route of novel coronavirus/COVID-19?
- □
- Novel coronavirus/COVID-19 is transmitted through coughing or sneezing.
- □
- Novel coronavirus/COVID-19 is not transmitted by close contact with people.
- □
- Don’t know
- 21.
- Which of the following are effective preventative measures for yourself and/or others against the novel coronavirus/COVID-19?
| Yes | No | Don’t Know | |
| Hand-washing | |||
| Avoiding touching your eyes, nose and mouth with unwashed hands | |||
| Using disinfectants | |||
| Staying home when you are sick | |||
| Taking herbal supplements | |||
| Covering your cough or sneeze | |||
| Eating a balanced diet | |||
| Avoiding close contact with someone who is sick | |||
| Using vitamin supplements | |||
| Using caution when opening mail | |||
| Avoiding eating meat | |||
| Exercising regularly | |||
| Wearing a face mask | |||
| Using hand sanitizer | |||
| Using drugs | |||
| Social/physical distancing | |||
| Using homeopathic remedies |
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- González-Bustamante, B. Evolution and early government responses to COVID-19 in South America. World Dev. 2021, 137, 105180. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Cao, Q.; Qin, L.; Wang, X.; Cheng, Z.; Pan, A.; Dai, J.; Sun, Q.; Zhao, F.; Qu, J.; et al. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China. J. Infect. 2020, 80, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID-19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef]
- Rojas Román, B.; Moscoso, S.; Chung, S.A.; Limpias Terceros, B.; Álvarez-Risco, A.; Yáñez, J.A. Tratamiento de la COVID-19 en Perú y Bolivia y los riesgos de la automedicación. Rev. Cuba. Farm. 2020, 53, 1–20. [Google Scholar]
- Yáñez, J.A.; Alvarez-Risco, A.; Delgado-Zegarra, J. Covid-19 in Peru: From supervised walks for children to the first case of Kawasaki-like syndrome. BMJ 2020, 369, m2418. [Google Scholar] [CrossRef]
- Alvarez-Risco, A.; Mejia, C.R.; Delgado-Zegarra, J.; Del-Aguila-Arcentales, S.; Arce-Esquivel, A.A.; Valladares-Garrido, M.J.; Rosas del Portal, M.; Villegas, L.F.; Curioso, W.H.; Sekar, M.C.; et al. The Peru Approach against the COVID-19 Infodemic: Insights and Strategies. Am. J. Trop. Med. Hyg. 2020, 103, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Risco, A.; Arellano, E.Z.; Valerio, E.M.; Acosta, N.M.; Tarazona, Z.S. Pharmaceutical care campaign as a strategy for implementation of pharmaceutical services: Experience Peru. Pharm. Care Esp. 2013, 15, 35–37. [Google Scholar]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S. Prescription errors as a barrier to pharmaceutical care in public health facilities: Experience Peru. Pharm. Care Esp. 2015, 17, 725–731. [Google Scholar]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Diaz-Risco, S. Pharmacovigilance as a tool for sustainable development of healthcare in Peru. Pharmacovigil. Rev. 2018, 10, 4–6. [Google Scholar]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Rosen, M.A.; García-Ibarra, V.; Maycotte-Felkel, S.; Martínez-Toro, G.M. Expectations and interests of university students in covid-19 times about sustainable development goals: Evidence from Colombia, Ecuador, Mexico, and Peru. Sustainability 2021, 13, 3306. [Google Scholar] [CrossRef]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Stevenson, J.G. Pharmacists and mass communication for implementing pharmaceutical care. Am. J. Pharm. Benefits 2015, 7, e125–e126. [Google Scholar]
- Alvarez-Risco, A.; Quiroz-Delgado, D.; Del-Aguila-Arcentales, S. Pharmaceutical care in hypertension patients in a peruvian hospital. Indian J. Public Health Res. Dev. 2016, 7, 183–188. [Google Scholar] [CrossRef]
- Alvarez-Risco, A.; Turpo-Cama, A.; Ortiz-Palomino, L.; Gongora-Amaut, N.; Del-Aguila-Arcentales, S. Barriers to the implementation of pharmaceutical care in pharmacies in Cusco, Peru. Pharm. Care Esp. 2016, 18, 194–205. [Google Scholar]
- Enciso-Zarate, A.; Guzmán-Oviedo, J.; Sánchez-Cardona, F.; Martínez-Rohenes, D.; Rodríguez-Palomino, J.C.; Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Diaz-Risco, S. Evaluation of contamination by cytotoxic agents in Colombian hospitals. Pharm. Care Esp. 2016, 18, 241–250. [Google Scholar]
- Mejía-Acosta, N.; Alvarez-Risco, A.; Solís-Tarazona, Z.; Matos-Valerio, E.; Zegarra-Arellano, E.; Del-Aguila-Arcentales, S. Adverse drug reactions reported as a result of the implementation of pharmaceutical care in the Institutional Pharmacy DIGEMID-Ministry of Health. Pharm. Care Esp. 2016, 18, 67–74. [Google Scholar]
- Gonzales-Tamayo, L.; Arevalo-Oropeza, M.; Yáñez, J.A. COVID-19 Physician Deaths in Peru: A Result of an Underfunded and Fragmented Healthcare System. Available online: https://ssrn.com/abstract=3676849 (accessed on 1 November 2021).
- Mejia, C.R.; Ticona, D.; Rodriguez-Alarcon, J.F.; Campos-Urbina, A.M.; Garayar-Peceros, H.; Catay-Medina, J.B.; Porta-Quinto, T.; Garay-Rios, L.; Ignacio-Quinte, C.; Guevara-Sosa, S. Percepción de las medidas de salud pública en Perú para frenar el avance de la COVID-19. Rev. Cuba Investig. Bioméd. 2021, 40, e737. [Google Scholar]
- Yáñez, J.A.; Afshar Jahanshahi, A.; Alvarez-Risco, A.; Li, J.; Zhang, S.X. Anxiety, Distress, and Turnover Intention of Healthcare Workers in Peru by Their Distance to the Epicenter during the COVID-19 Crisis. Am. J. Trop. Med. Hyg. 2020, 103, 1614–1620. [Google Scholar] [CrossRef]
- Yan, J.; Kim, S.; Zhang, S.X.; Foo, M.-D.; Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Yáñez, J.A. Hospitality Workers’ COVID-19 Risk Perception and Depression: A Contingent Model Based on Transactional Theory of Stress Model. Int. J. Hosp. Manag. 2021, 95, 102935. [Google Scholar] [CrossRef]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Yanez, J.A. Opportunity for eHealth due to COVID-19 Outbreak: Case of Peru. Am. J. Trop. Med. Hyg. 2020. Available online: https://ssrn.com/abstract=3741715 (accessed on 1 November 2021). [CrossRef]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Yáñez, J.A.; Rosen, M.A.; Mejia, C.R. Influence of Technostress on Academic Performance of University Medicine Students in Peru during the COVID-19 Pandemic. Sustainability 2021, 13, 8949. [Google Scholar] [CrossRef]
- Yáñez, J.A.; Chung, S.A.; Inga-Berrospi, F.; Mejia, C.R. Demographic and Geographic COVID-19 Death Risk Factors in Peru. A Nationwide Analysis. EClinicalMedicine 2020. Available online: https://ssrn.com/abstract=3648543 (accessed on 1 November 2021). [CrossRef]
- Yáñez, J.A.; Alvarez-Risco, A.; Delgado-Zegarra, J. Rapid Response: Does Peru Really Have That High Number of COVID-19 Confirmed Cases? The Deception of Combining RT-PCR and Rapid Test Results. Available online: https://www.bmj.com/content/369/bmj.m2518/rr-4 (accessed on 1 July 2020).
- Yáñez, J.A.; Alvarez-Risco, A.; Delgado-Zegarra, J. Rapid Response: Clearing the Path for COVID-19 in Peru? The Decision of Supervised Walks for Children and Adolescents. Available online: https://www.bmj.com/content/369/bmj.m1918/rr-9 (accessed on 3 June 2020).
- Salathé, M.; Althaus, C.L.; Neher, R.; Stringhini, S.; Hodcroft, E.; Fellay, J.; Zwahlen, M.; Senti, G.; Battegay, M.; Wilder-Smith, A.; et al. COVID-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation. Swiss Med Wkly. 2020, 150, 1112. [Google Scholar] [CrossRef]
- MacIntyre, C.R. Case isolation, contact tracing, and physical distancing are pillars of COVID-19 pandemic control, not optional choices. Lancet Infect. Dis. 2020, 20, 1105–1106. [Google Scholar] [CrossRef]
- VanderWeele, T.J. Challenges Estimating Total Lives Lost in COVID-19 Decisions: Consideration of Mortality Related to Unemployment, Social Isolation, and Depression. JAMA 2020, 324, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Chen, J.; Afshar Jahanshahi, A.; Alvarez-Risco, A.; Dai, H.; Li, J.; Patty-Tito, R.M. Succumbing to the COVID-19 Pandemic—Healthcare Workers Not Satisfied and Intend to Leave Their Jobs. Int. J. Ment. Health Addict. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, S.X.; Jahanshahi, A.A.; Alvarez-Risco, A.; Dai, H.; Li, J.; Ibarra, V.G. Belief in a COVID-19 conspiracy theory as a predictor of mental health and well-being of health care workers in Ecuador: Cross-sectional survey study. JMIR Public Health Surveill. 2020, 6, e20737. [Google Scholar] [CrossRef]
- Bernard, R.; Bowsher, G.; Sullivan, R.; Gibson-Fall, F. Disinformation and Epidemics: Anticipating the Next Phase of Biowarfare. Health Secur. 2020, 19, 3–12. [Google Scholar] [CrossRef]
- Stolle, L.B.; Nalamasu, R.; Pergolizzi, J.V.; Varrassi, G.; Magnusson, P.; LeQuang, J.; Breve, F. Fact vs. Fallacy: The Anti-Vaccine Discussion Reloaded. Adv. Ther. 2020, 37, 4481–4490. [Google Scholar] [CrossRef]
- Burki, T. The online anti-vaccine movement in the age of COVID-19. Lancet Digit. Health 2020, 2, e504–e505. [Google Scholar] [CrossRef]
- Matias, T.; Dominski, F.H.; Marks, D.F. Human needs in COVID-19 isolation. J. Health Psychol. 2020, 25, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Quispe-Cañari, J.F.; Fidel-Rosales, E.; Manrique, D.; Mascaro-Zan, J.; Huamán-Castillón, K.M.; Chamorro-Espinoza, S.E.; Garayar-Peceros, H.; Ponce-López, V.L.; Sifuentes-Rosales, J.; Alvarez-Risco, A.; et al. Self-medication practices during the COVID-19 pandemic among the adult population in Peru: A cross-sectional survey. Saudi Pharm. J. 2021, 29, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yáñez, J.A.; Chung, S.A.; Román, B.R.; Hernández-Yépez, P.J.; Garcia-Solorzano, F.O.; Del-Aguila-Arcentales, S.; Inga-Berrospi, F.; Mejia, C.R.; Alvarez-Risco, A. Chapter 14-Prescription, over-the-counter (OTC), herbal, and other treatments and preventive uses for COVID-19. In Environmental and Health Management of Novel Coronavirus Disease (COVID-19); Hadi Dehghani, M., Karri, R.R., Roy, S., Eds.; Academic Press: London, UK, 2021; pp. 379–416. [Google Scholar]
- Lim, X.Y.; Teh, B.P.; Tan, T.Y.C. Medicinal Plants in COVID-19: Potential and Limitations. Front. Pharmacol. 2021, 12, 611408. [Google Scholar] [CrossRef]
- Villena-Tejada, M.; Vera-Ferchau, I.; Cardona-Rivero, A.; Zamalloa-Cornejo, R.; Quispe-Florez, M.; Frisancho-Triveño, Z.; Abarca-Meléndez, R.C.; Alvarez-Sucari, S.G.; Mejia, C.R.; Yañez, J.A. Use of medicinal plants for COVID-19 prevention and respiratory symptom treatment during the pandemic in Cusco, Peru: A cross-sectional survey. PLoS ONE 2021, 16, e0257165. [Google Scholar] [CrossRef]
- Pomeranz, J.L.; Schwid, A.R. Governmental actions to address COVID-19 misinformation. J. Public Health Policy 2021, 42, 201–210. [Google Scholar] [CrossRef]
- Kolluri, N.L.; Murthy, D. CoVerifi: A COVID-19 news verification system. Online Soc. Netw. Media 2021, 22, 100123. [Google Scholar] [CrossRef]
- Alvarez-Risco, A.; Del-Aguila-Arcentales, S.; Yanez, J.A. Telemedicine in Peru as a Result of the COVID-19 Pandemic: Perspective from a Country with Limited Internet Access. Am. J. Trop. Med. Hyg. 2021, 105, 6–11. [Google Scholar] [CrossRef] [PubMed]
- MINSA. Resolución Ministerial N° 686-2020-MINSA-Norma Técnica de Salud para la Investigación y Desarrollo de Vacunas contra Enfermedades Infecciosas; Ministerio de Salud: Lima, Peru, 2020. [Google Scholar]
- MINSA. Resolución Ministerial N° 848-2020-MINSA-Plan Nacional de Vacunación contra la COVID-19; Ministerio de Salud: Lima, Peru, 2020. [Google Scholar]
- MINSA. Covid-19: Conoce Aquí el Cronograma de Vacunación para Personas de 12 Años a Más. Available online: https://elperuano.pe/noticia/124671-covid-19-conoce-aqui-el-cronograma-de-vacunacion-para-personas-de-12-anos-a-mas/ (accessed on 25 November 2021).
- PCM. Campaña Nacional de Vacunación contra la COVID-19. Available online: https://www.gob.pe/institucion/pcm/campa%C3%B1as/3451-campana-nacional-de-vacunacion-contra-la-covid-19 (accessed on 25 November 2021).
- MINSA. Resolución Ministerial N° 023-2021-MINSA-CENARES se Encargue de Ejecutar el Acuerdo de Compraventa con la Empresa Sinopharm; Ministerio de Salud: Lima, Peru, 2021. [Google Scholar]
- MINSA. Resolución Ministerial N° 078-2021-MINSA-CENARES Gestionar, Implementar y Ejecutar el Contrato de Compraventa con la Empresa Astrazeneca; Ministerio de Salud: Lima, Peru, 2021. [Google Scholar]
- MINSA. Resolución Ministerial N° 209-2021-MINSA-Ejecutar el Acuerdo de Fabricación y Suministro Suscrito con la Empresa Pfizer S.A.; Ministerio de Salud: Lima, Peru, 2021. [Google Scholar]
- MINSA. Resolución Ministerial N° 443-2021-MINSA-Encargar a CENARES en el Marco de Acuerdo de Compromisos Gestione Autorización Sanitaria; Ministerio de Salud: Lima, Peru, 2021. [Google Scholar]
- MINSA. Coronavirus: Vacunas contra la COVID-19 en el Perú. Available online: https://www.gob.pe/11571-coronavirus-vacunas-contra-la-covid-19-en-el-peru (accessed on 23 November 2021).
- RPP. Digemid Otorga Registro Sanitario Condicional a Vacuna de Pfizer Contra la COVID-19. Available online: https://rpp.pe/peru/actualidad/coronavirus-en-peru-digemid-otorga-registro-sanitario-condicional-a-vacuna-de-pfizer-contra-la-covid-19-noticia-1318775?ref=rpp (accessed on 23 November 2021).
- CenadIM. La DIGEMID Otorga Autorización Excepcional para la Importación y Uso de la Vacuna COVID 19 AstraZeneca (ChAdOx1-S [recombinant]). Available online: https://bvcenadim.digemid.minsa.gob.pe/noticias/422-la-digemid-otorga-autorizacion-excepcional-para-la-importacion-y-uso-de-la-vacuna-covid-19-astrazeneca-chadox1-s-recombinant (accessed on 23 November 2021).
- DIGEMID. Ministerio de Salud Autorizó el Registro Sanitario Condicional de la Vacuna contra la COVID-19 de la Farmacéutica Johnson & Johnson. Available online: https://www.digemid.minsa.gob.pe/noticias/2021/07/ID=1912/ministerio-de-salud-autorizo-el-registro-sanitario-condicional-de-la-vacuna-contra-la-covid-19-de-la-farmaceutica-johnson-johnson (accessed on 23 November 2021).
- DIGEMID. Digemid del Ministerio de Salud Otorga Registro Sanitario Condicional a la Vacuna contra la COVID-19 de Sinopharm. Available online: https://www.digemid.minsa.gob.pe/noticias/2021/08/ID=2478/digemid-otorga-registro-sanitario-condicional-a-la-vacuna-contra-la-covid-19-de-sinopharm (accessed on 23 November 2021).
- MINSA. Resolución Ministerial N° 161-2021-MINSA-Modificar el Rubro “Fases de Vacunación” del Plan Nacional de Vacunación contra la COVID-19; Ministerio de Salud: Lima, Peru, 2021. [Google Scholar]
- MINSA. Resolución Ministerial N° 139-2021-MINSA-Conformación de un Equipo Consultivo de Alto Nivel; Ministerio de Salud: Lima, Peru, 2021. [Google Scholar]
- Lope, P.C.; Carracedo, S.; Romani, F. The regulation of COVID-19 clinical trials in Peru. Rev. Peru Med. Exp. Salud Publica 2021, 38, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, G. Vacuna-gate escalates in Peru. Lancet Infect. Dis. 2021, 21, 463. [Google Scholar] [CrossRef]
- Mayta-Tristán, P.; Aparco, J.P. Use of experimental vaccine outside of clinical trial: The “Vacunagate” case. Rev. Peru Med. Exp. Salud Publica 2021, 38, 203–205. [Google Scholar] [CrossRef]
- Mayta-Tovalino, F.; Munive-Degregori, A.; Mendoza, R.; Alvitez-Temoche, D. Vacunagate scandal and its possible impact on the vaccination against COVID-19 of health professionals in Peru. J. Int. Oral Health 2021, 13, 310–311. [Google Scholar] [CrossRef]
- Chauvin, L. Peruvian COVID-19 vaccine scandal spreads. Lancet 2021, 397, 783. [Google Scholar] [CrossRef]
- Collave Garcia, Y. ‘Vacunagate’ ¿Cómo Afecta a la Ciencia Peruana el Escándalo de las Vacunas Extra de Sinopharm? Available online: https://elcomercio.pe/tecnologia/ciencias/vacunagate-como-afecta-el-escandalo-de-las-vacunas-extra-de-sinopharm-a-la-ciencia-peruana-noticia/ (accessed on 24 November 2021).
- Cabezas-Sanchez, C.; Hurtado-Roca, Y.; Suárez-Moreno, V. Peru to punish bending of clinical-trial rules. Nature 2021, 595, 650. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodes-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Baltekian, D.; Roser, M. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 1 November 2021).
- Institute of Global Health Innovation. Covid-19: Global Attitudes towards a COVID-19 Vaccine; Covid Data Hub. Available online: https://www.imperial.ac.uk/media/imperial-college/institute-of-global-health-innolvation/GlobalVaccineInsights_ICL-YouGov-Covid-19-Behaviour-Tracker_20210520_v2.pdf (accessed on 1 November 2021).
- OCU. Encuesta OCU: Los Españoles y la Vacuna. Available online: https://www.ocu.org/salud/medicamentos/noticias/encuesta-vacuna-covid (accessed on 1 November 2021).
- Faasse, K.; Newby, J. Public Perceptions of COVID-19 in Australia: Perceived Risk, Knowledge, Health-Protective Behaviors, and Vaccine Intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef] [PubMed]
- Volkman, J.E.; Hokeness, K.L.; Morse, C.R.; Viens, A.; Dickie, A. Information source’s influence on vaccine perceptions: An exploration into perceptions of knowledge, risk and safety. J. Commun. Healthc. 2021, 14, 50–60. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef]
- Gutiérrez-Zevallos, J.D.; Espíritu-Martínez, L.B. COVID-19: Vaccination in a developing country. J. Public Health 2021, 43, e362–e363. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Aiken, L.R. Three Coefficients for Analyzing the Reliability and Validity of Ratings. Educ. Psychol. Meas. 1985, 45, 131–142. [Google Scholar] [CrossRef]
- Naderifar, M.; Goli, H.; Ghaljaei, F. Snowball Sampling: A Purposeful Method of Sampling in Qualitative Research. Strides Dev. Med. Educ. 2017, 14, e67670. [Google Scholar] [CrossRef] [Green Version]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Costa Aponte, F. Resultados Definitivos de los Censos Nacionales 2017; INEI: Lima, Peru, 2018. [Google Scholar]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Seale, H.; Heywood, A.E.; Leask, J.; Sheel, M.; Durrheim, D.N.; Bolsewicz, K.; Kaur, R. Examining Australian public perceptions and behaviors towards a future COVID-19 vaccine. BMC Infect. Dis. 2021, 21, 120. [Google Scholar] [CrossRef]
- Al-Ayyadhi, N.; Ramadan, M.M.; Al-Tayar, E.; Al-Mathkouri, R.; Al-Awadhi, S. Determinants of Hesitancy Towards COVID-19 Vaccines in State of Kuwait: An Exploratory Internet-Based Survey. Risk Manag. Healthc. Policy 2021, 14, 4967–4981. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, R.; Nguse, T.M.; Habte, B.M.; Fentie, A.M.; Gebretekle, G.B. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS ONE 2021, 16, e0261125. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.A.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, Q.; Silver Tarimo, C.; Wang, M.; Gu, J.; Wei, W.; Ma, M.; Zhao, L.; Mu, Z.; Miao, Y. COVID-19 Vaccine Hesitancy Among Chinese Population: A Large-Scale National Study. Front. Immunol. 2021, 12, 781161. [Google Scholar] [CrossRef] [PubMed]
- Kanyanda, S.; Markhof, Y.; Wollburg, P.; Zezza, A. Acceptance of COVID-19 vaccines in sub-Saharan Africa: Evidence from six national phone surveys. BMJ Open 2021, 11, e055159. [Google Scholar] [CrossRef]
- Altulahi, N.; AlNujaim, S.; Alabdulqader, A.; Alkharashi, A.; AlMalki, A.; AlSiari, F.; Bashawri, Y.; Alsubaie, S.; AlShahrani, D.; AlGoraini, Y. Willingness, beliefs, and barriers regarding the COVID-19 vaccine in Saudi Arabia: A multiregional cross-sectional study. BMC Fam. Pract. 2021, 22, 247. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, M.V.; Kummerfeld, E.; MacDonald, A., III; Vinogradov, S. Willingness to vaccinate against SARS-CoV-2: The role of reasoning biases and conspiracist ideation. Vaccine 2021, in press. [Google Scholar] [CrossRef]
- Zein, S.; Abdallah, S.B.; Al-Smadi, A.; Gammoh, O.; Al-Awaida, W.J.; Al-Zein, H.J. Factors associated with the unwillingness of Jordanians, Palestinians and Syrians to be vaccinated against COVID-19. PLoS Negl. Trop. Dis. 2021, 15, e0009957. [Google Scholar] [CrossRef]
- Caycho-Rodríguez, T.; Carbajal-León, C.; Vivanco-Vidal, A.; Saroli-Araníbar, D. Intention to vaccinate against COVID-19 in Peruvian older adults. Rev. Esp. Geriatr. Gerontol. 2021, 56, 245–246. [Google Scholar] [CrossRef]
- Herrera-Añazco, P.; Uyen-Cateriano, A.; Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Toro-Huamanchumo, C.J.; Rodríguez-Morales, A.J.; Hernández, A.V.; Benites-Zapata, V.A. Prevalencia y factores asociados a la intención de vacunarse contra la COVID-19 en el Perú. Rev. Peru. Med. Exp. Salud Publica 2021, 38, 381–390. [Google Scholar] [CrossRef]
- Corrales, C.; Alberto, J.M. Percepciones de la Aceptación de la Vacuna contra el COVID-19 en Personas Que Acuden a un Mercado Popular en Arequipa 2021; Universidad Nacional de San Agustín de Arequipa: Arequipa, Peru, 2021. [Google Scholar]
- Caycho-Rodríguez, T.; Tomás, J.M.; Carbajal-León, C.; Vilca, L.W.; Reyes-Bossio, M.; Intimayta-Escalante, C.; Vivanco-Vidal, A.; Saroli-Araníbar, D.; Esteban, R.F.C.; White, M. Sociodemographic and Psychological Predictors of Intention to Receive a COVID-19 Vaccine in Elderly Peruvians. Trends Psychol. 2021, 21, 1–18. [Google Scholar] [CrossRef]
- Serpa Barrientos, A.; Tito-Huamani, P.L.; Soria Qui Jaite, J.J.; Pena Tomas, B.G.; Geraldo Campos, L.A. Attitude towards COVID-19 Vaccination in the Peruvian Population. J. Res. Med. Dent. Sci. 2021, 9, 1–10. [Google Scholar]
- Alabdulla, M.; Reagu, S.M.; Al-Khal, A.; Elzain, M.; Jones, R.M. COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir. Viruses 2021, 15, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Sanche, S.; Lin, Y.T.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg Infect Dis. 2020, 26, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Ditekemena, J.D.; Nkamba, D.M.; Mutwadi, A.; Mavoko, H.M.; Siewe Fodjo, J.N.; Luhata, C.; Obimpeh, M.; Van Hees, S.; Nachega, J.B.; Colebunders, R. COVID-19 Vaccine Acceptance in the Democratic Republic of Congo: A Cross-Sectional Survey. Vaccines 2021, 9, 153. [Google Scholar] [CrossRef]
- Kuter, B.J.; Browne, S.; Momplaisir, F.M.; Feemster, K.A.; Shen, A.K.; Green-McKenzie, J.; Faig, W.; Offit, P.A. Perspectives on the receipt of a COVID-19 vaccine: A survey of employees in two large hospitals in Philadelphia. Vaccine 2021, 39, 1693–1700. [Google Scholar] [CrossRef] [PubMed]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef] [PubMed]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and Vaccine Hesitancy: A Challenge the United States Must Overcome. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef] [PubMed]
- Casapia, J.P. Crisis por el Coronavirus Aumentó las Desigualdades en el Perú, Banco Mundial. 2021. Available online: https://www.bancomundial.org/es/news/press-release/2020/09/08/crisis-por-el-coronavirus-aumento-las-desigualdades-en-el-peru (accessed on 1 November 2021).
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association Between Vaccine Refusal and Vaccine-Preventable Diseases in the United States: A Review of Measles and Pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MINSA. Vacunación COVID-19-Perú. Available online: https://www.minsa.gob.pe/reunis/data/vacunas-covid19.asp (accessed on 21 December 2021).
- MINSA. Covid-19: Desde Este Viernes 10 de Diciembre Será Obligatorio el Carné de Vacunación. Available online: https://elperuano.pe/noticia/135041-covid-19-desde-este-viernes-10-de-diciembre-sera-obligatorio-el-carnet-de-vacunacion (accessed on 21 December 2021).
- Gestión. COVID: ¿Se Llegará al 80% de Cobertura de Población Vacunada Antes de Culminar el 2021? Available online: https://gestion.pe/peru/resumen-del-ano-2021-covid-19-peru-llegara-al-80-de-la-cobertura-poblacion-vacunada-antes-de-culminar-el-2021-minsa-nndc-noticia/ (accessed on 21 December 2021).

{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency | Percentage/Interquartile Range |
|---|---|---|
| Gender | ||
| Male | 748 | 42.1% |
| Female | 1028 | 57.9% |
| Age (years of age) a | 24 | 20–28 |
| Level of education | ||
| High school or lower | 145 | 8.2% |
| Technical | 241 | 13.6% |
| University | 1199 | 67.5% |
| Postgraduate | 191 | 10.8% |
| Household size a | 4 | 3–5 |
| Healthcare worker | ||
| No | 1589 | 89.5% |
| Yes | 187 | 10.5% |
| With a chronic disease | ||
| No | 1428 | 80.4% |
| Yes | 348 | 19.6% |
| Got infected with COVID-19? | ||
| No | 1085 | 61.1% |
| Yes (confirmed with a test) | 244 | 13.7% |
| Yes (without a test) | 112 | 6.3% |
| I don’t know/it is possible | 335 | 18.9% |
| Family or friends got infected with COVID-19? | ||
| No | 805 | 45.3% |
| Yes (confirmed with a test) | 657 | 37.0% |
| Yes (without a test) | 156 | 8.8% |
| I don’t know/it is possible | 158 | 8.9% |
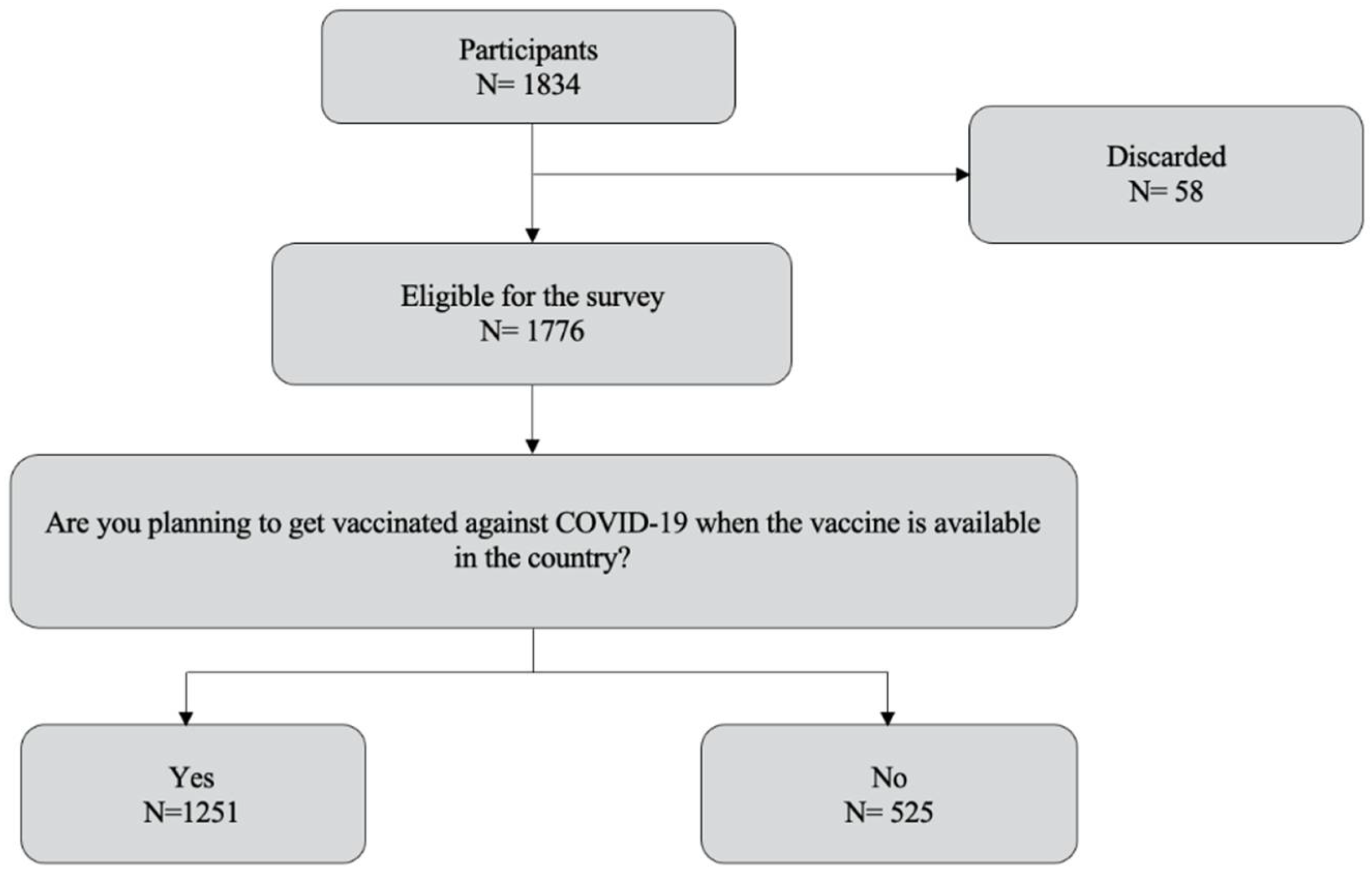
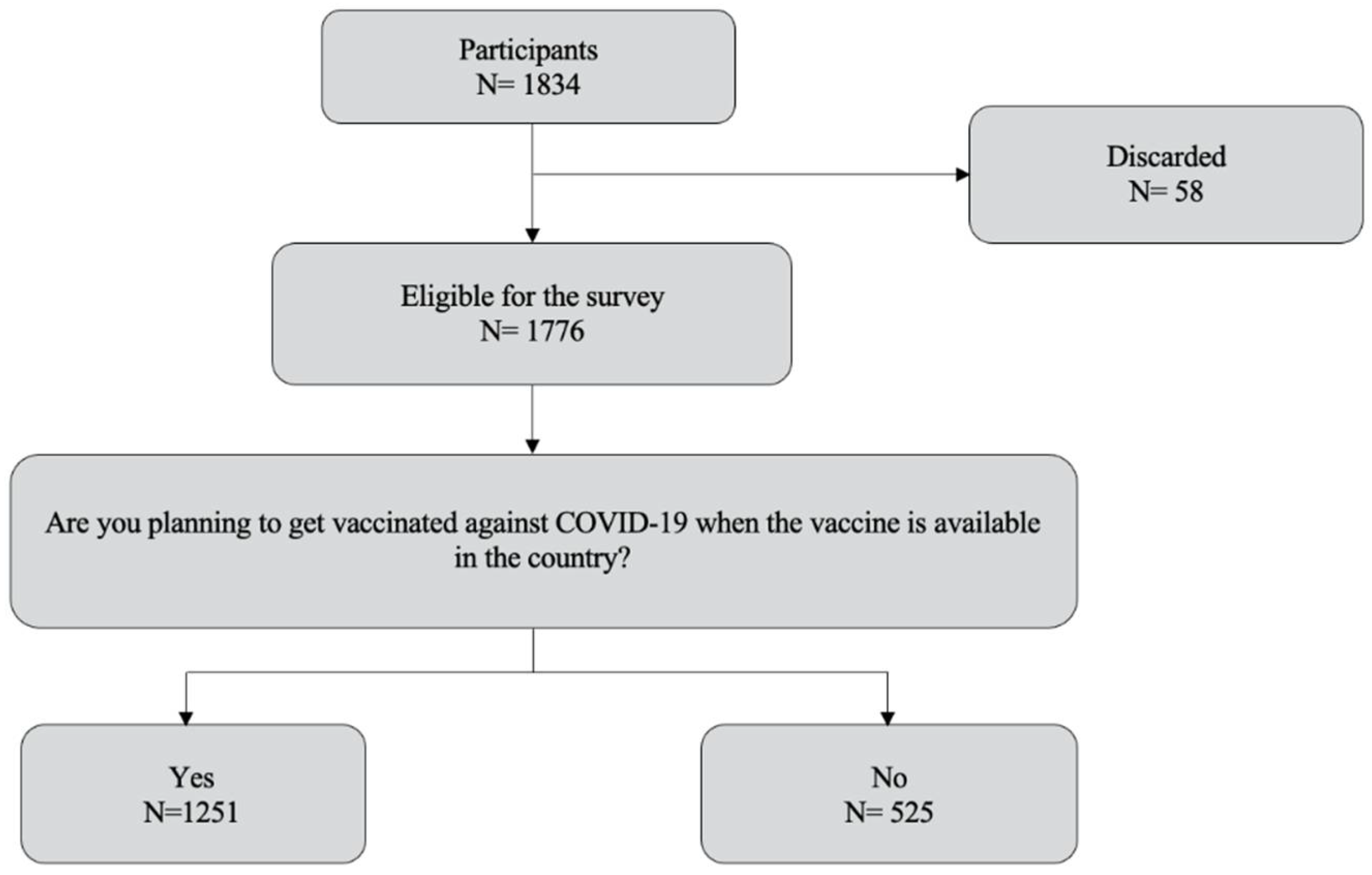
| Will you get vaccinated against COVID-19? | ||
| No | 179 | 10.1% |
| Yes | 1251 | 70.4% |
| I don’t know yet. | 346 | 19.5% |
| Variable | Will You Get Vaccinated? | p-Value | ||
|---|---|---|---|---|
| No | Yes | I Don’t Know | ||
| Gender | ||||
| Male | 72 (9.6%) | 539 (72.1%) | 137 (18.3%) | 0.439 |
| Female | 107 (10.4%) | 712 (69.3%) | 209 (20.3%) | |
| Age (years of age) a | 29 (21–42) | 24 (20–37) | 23 (20–39) | 0.021 |
| Level of education | ||||
| High school or lower | 16 (11.0%) | 89 (61.4%) | 40 (27.6%) | <0.001 |
| Technical | 20 (8.3%) | 175 (72.6%) | 46 (19.1%) | |
| University | 107 (8.9%) | 856 (71.4%) | 236 (19.7%) | |
| Postgraduate | 36 (18.9%) | 131 (68.6%) | 24 (12.5%) | |
| Household size a | 4 (3–5) | 4 (3–5) | 4 (3–5) | 0.456 |
| Healthcare worker | ||||
| No | 167 (10.5%) | 1096 (69.0%) | 326 (20.5%) | <0.001 |
| Yes | 12 (6.4%) | 155 (82.9%) | 20 (10.7%) | |
| With a chronic disease | ||||
| No | 152 (10.6%) | 988 (69.2%) | 288 (20.2%) | 0.058 |
| Yes | 27 (7.8%) | 263 (75.6%) | 58 (16.6%) | |
| Got infected with COVID-19? | ||||
| No | 113 (10.4%) | 798 (73.6%) | 174 (16.0%) | <0.001 |
| Yes (confirmed with a test) | 17 (7.0%) | 169 (69.3%) | 58 (23.7%) | |
| Yes (without a test) | 12 (10.7%) | 85 (75.9%) | 15 (13.4%) | |
| I don’t know/it is possible | 37 (11.0%) | 199 (59.4%) | 99 (29.6%) | |
| Family or friends got infected with COVID-19? | ||||
| No | 81 (10.1%) | 588 (73.0%) | 136 (16.9%) | 0.003 |
| Yes (confirmed with a test) | 66 (10.0%) | 457 (69.6%) | 134 (20.4%) | |
| Yes (without a test) | 17 (10.9%) | 113 (72.4%) | 26 (16.7%) | |
| I don’t know/it is possible | 15 (9.5%) | 93 (58.9%) | 50 (31.6%) | |
| Variable | aPR (95% Confidence Internal) p-Value | |
|---|---|---|
| Bivariate Analysis | Multivariate Analysis | |
| Female | 1.10 (0.95–1.27) 0.186 | Did not use the model |
| Age (years of age) | 1.00 (0.99–1.01) 0.459 | Did not use the model |
| Level of education | ||
| High school or lower | Ref. | Ref. |
| Technical | 0.71 (0.49–1.01) 0.062 | 0.72 (0.49–1.04) 0.077 |
| University | 0.74 (0.60–0.92) 0.007 | 0.75 (0.61–0.92) 0.005 |
| Postgraduate | 0.81 (0.55–1.21) 0.312 | 0.93 (0.63–1.37) 0.724 |
| Household size | 1.00 (0.96–1.05) 0.965 | Did not use the model |
| Healthcare worker | 0.55 (0.41–0.74) <0.001 | 0.59 (0.44–0.80) 0.001 |
| With a chronic disease | 0.79 (0.58–1.09) 0.148 | Did not use the model |
| Got infected with COVID-19? | ||
| No | Ref. | Ref. |
| Yes (confirmed with a test) | 1.16 (0.93–1.45) 0.179 | 1.15 (0.89–1.49) 0.289 |
| Yes (without a test) | 0.91 (0.62–1.34) 0.640 | 0.88 (0.56–1.39) 0.595 |
| I don’t know/it is possible | 1.53 (1.23–1.91) <0.001 | 1.40 (1.09–1.81) 0.008 |
| Family or friends got infected with COVID-19? | ||
| No | Ref. | Ref. |
| Yes (confirmed with a test) | 1.13 (0.92–1.39) 0.256 | 1.04 (0.82–1.32) 0.744 |
| Yes (without a test) | 1.02 (0.72–1.46) 0.902 | 0.96 (0.65–1.41) 0.827 |
| I don’t know/it is possible | 1.53 (1.09–2.15) 0.015 | 1.22 (0.83–1.78) 0.310 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vizcardo, D.; Salvador, L.F.; Nole-Vara, A.; Dávila, K.P.; Alvarez-Risco, A.; Yáñez, J.A.; Mejia, C.R. Sociodemographic Predictors Associated with the Willingness to Get Vaccinated against COVID-19 in Peru: A Cross-Sectional Survey. Vaccines 2022, 10, 48. https://doi.org/10.3390/vaccines10010048
Vizcardo D, Salvador LF, Nole-Vara A, Dávila KP, Alvarez-Risco A, Yáñez JA, Mejia CR. Sociodemographic Predictors Associated with the Willingness to Get Vaccinated against COVID-19 in Peru: A Cross-Sectional Survey. Vaccines. 2022; 10(1):48. https://doi.org/10.3390/vaccines10010048
Chicago/Turabian StyleVizcardo, David, Linder Figueroa Salvador, Arian Nole-Vara, Karen Pizarro Dávila, Aldo Alvarez-Risco, Jaime A. Yáñez, and Christian R. Mejia. 2022. "Sociodemographic Predictors Associated with the Willingness to Get Vaccinated against COVID-19 in Peru: A Cross-Sectional Survey" Vaccines 10, no. 1: 48. https://doi.org/10.3390/vaccines10010048
APA StyleVizcardo, D., Salvador, L. F., Nole-Vara, A., Dávila, K. P., Alvarez-Risco, A., Yáñez, J. A., & Mejia, C. R. (2022). Sociodemographic Predictors Associated with the Willingness to Get Vaccinated against COVID-19 in Peru: A Cross-Sectional Survey. Vaccines, 10(1), 48. https://doi.org/10.3390/vaccines10010048