
Factors Associated with Adverse Reactions to BNT162b2 COVID-19 Vaccine in a Cohort of 3969 Hospital Workers

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Source and Variables
2.3. Analyses
2.4. Ethical Considerations
3. Results
3.1. Description of the Sample
3.2. Specific Adverse Reactions
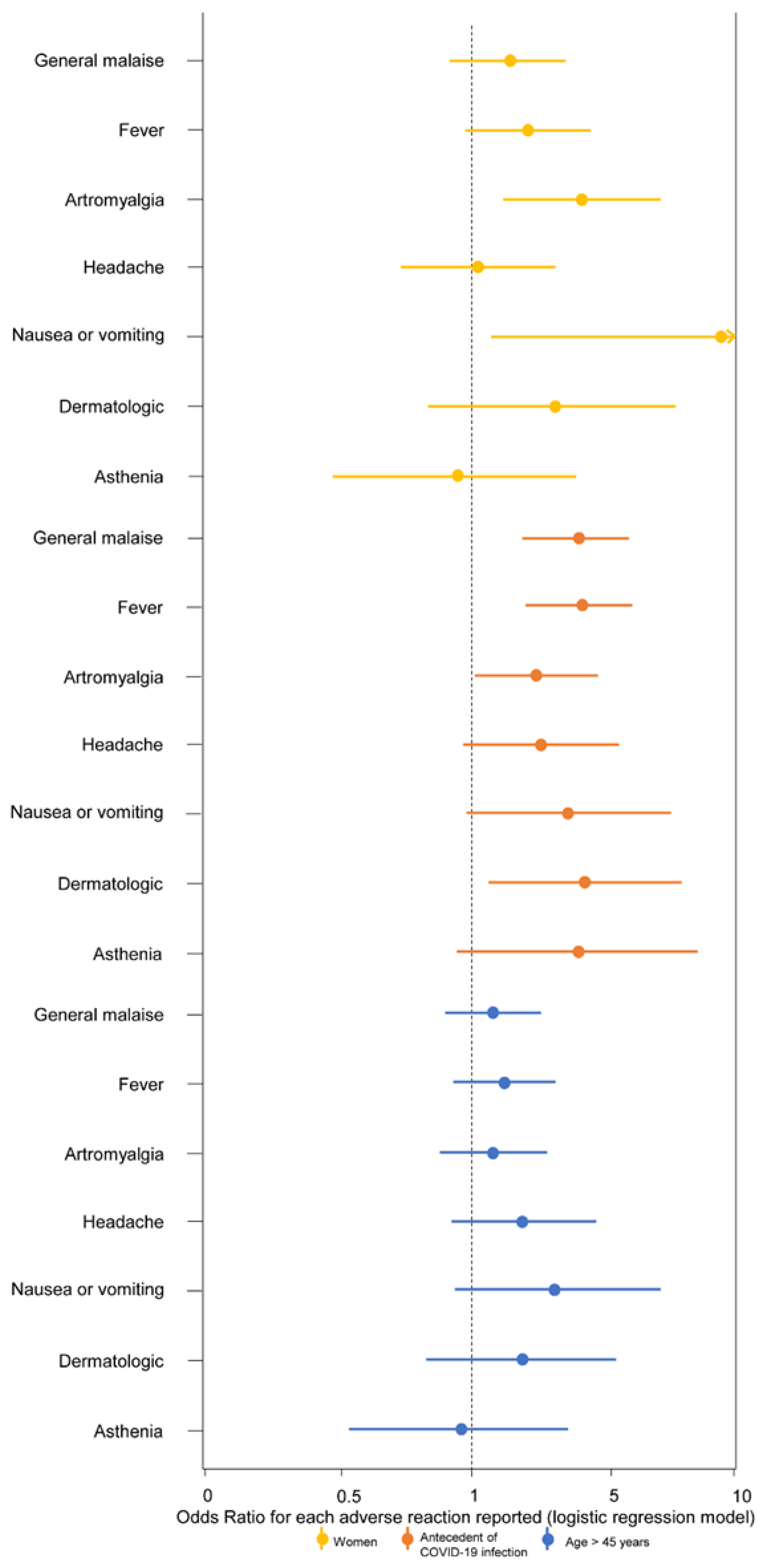
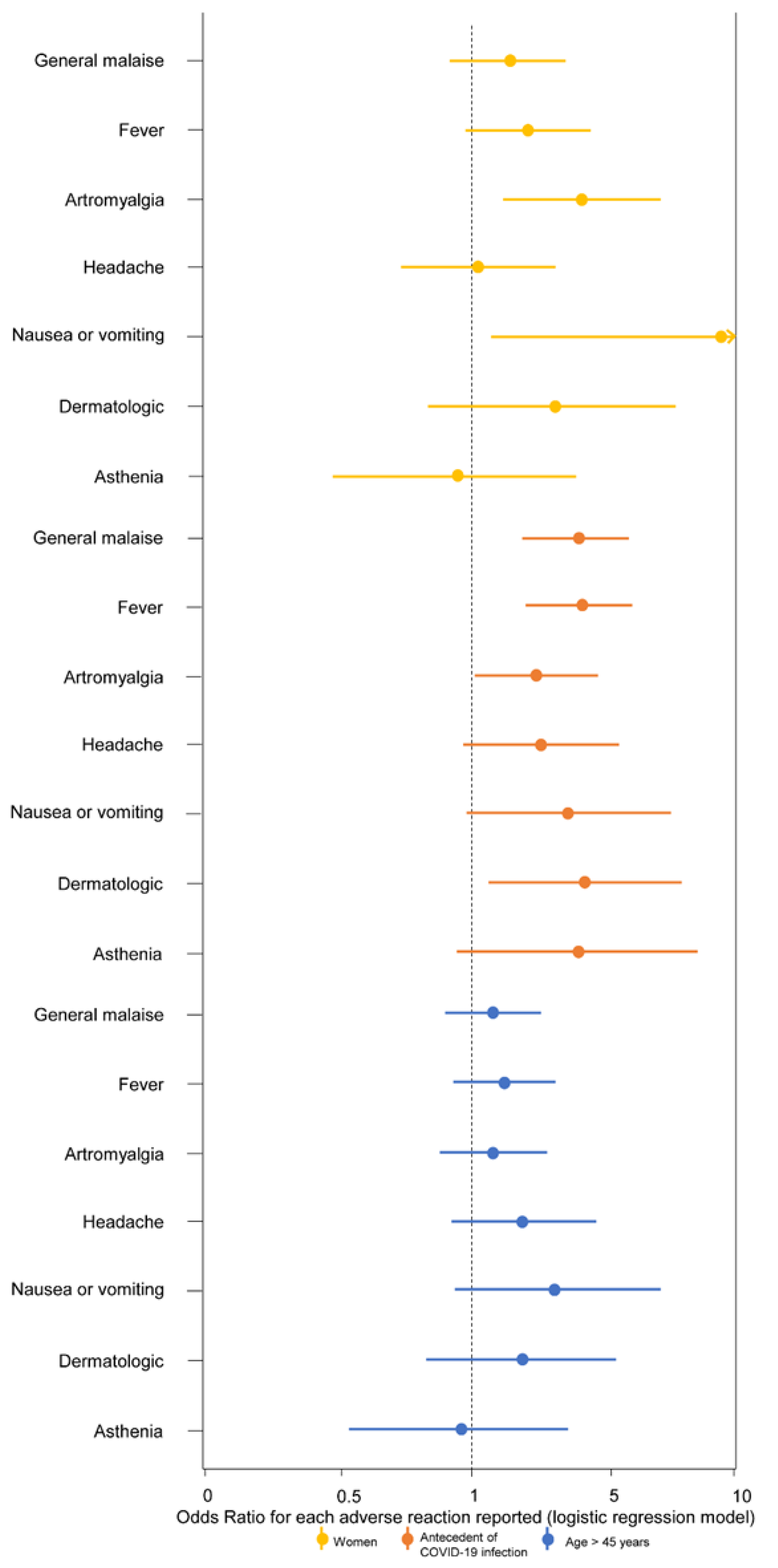
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forni, G.; Mantovani, A.; COVID-19 Commission of Accademia Nazionale dei Lincei, Rome. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Dema, B.; Reyes-Sandoval, A. COVID-19 vaccines: Breaking record times to first-in-human trials. NPJ Vaccines 2020, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Sakong, J.; Jo, S.; Kim, M.; Baek, K. Adverse Effects on Work and Daily Life Interference among Healthcare Workers after the First and Second ChAdOx1 and BNT162b2 COVID-19 Vaccine Doses. Vaccines 2021, 9, 926. [Google Scholar] [CrossRef] [PubMed]
- Modenese, A.; Paduano, S.; Bargellini, A.; Bellucci, R.; Marchetti, S.; Bruno, F.; Grazioli, P.; Vivoli, R.; Gobba, F. Neutralizing Anti-SARS-CoV-2 Antibody Titer and Reported Adverse Effects, in a Sample of Italian Nursing Home Personnel after Two Doses of the BNT162b2 Vaccine Administered Four Weeks Apart. Vaccines 2021, 9, 652. [Google Scholar] [CrossRef] [PubMed]
- Coggins, S.A.A.; Laing, E.D.; Olsen, C.H.; Goguet, E.; Moser, M.; Jackson-Thompson, B.M.; Samuels, E.C.; Pollett, S.D.; Tribble, D.R.; Davies, J.; et al. Adverse effects and antibody titers in response to the BNT162b2 mRNA COVID-19 vaccine in a prospective study of healthcare workers. medRxiv 2021. [Google Scholar] [CrossRef]
- Spanish Ministry of Health. Estrategia de Vacunación COVID-19 en España [Vaccination Strategy for COVID-19 in Spain]. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/vacunaCovid19.html (accessed on 18 October 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Tau, N.; Yahav, D.; Shepshelovich, D. Vaccine safety—Is the SARS-CoV-2 vaccine any different? Hum. Vaccin. Immunother. 2021, 17, 1322–1325. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [PubMed]
- European Medicines Agency. Comirnaty. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (accessed on 18 October 2021).
- Hajiabdolbaghi, M.; Jam, S.; SeyedAlinaghi, S.; Jafari, S.; Badie, B.M.; Sabzvari, D. Adverse reactions of trivalent influenza vaccine in HIV-infected individuals. Acta Med. Iran. 2010, 48, 95–100. [Google Scholar] [PubMed]
- Hurley, D.; Griffin, C.; Young, M.; Scott, D.A.; Pride, M.W.; Scully, I.L.; Ginis, J.; Severs, J.; Jansen, K.U.; Gruber, W.C.; et al. Safety, Tolerability, and Immunogenicity of a 20-Valent Pneumococcal Conjugate Vaccine (PCV20) in Adults 60 to 64 Years of Age. Clin. Infect. Dis. 2021, 73, e1489–e1497. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.C.; Li, Y.H.; Guan, X.H.; Hou, L.H.; Wang, W.J.; Li, J.X.; Wu, S.P.; Wang, B.S.; Wang, Z.; Wang, L.; et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Nakayama, T. Causal relationship between immunological responses and adverse reactions following vaccination. Vaccine 2019, 37, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística [National Institute of Statistics]. Available online: https://www.ine.es/index.htm (accessed on 9 December 2021).



{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 3969) | Adverse Reaction (n = 182) | No Adverse Reaction (n = 3781) | p-Value 1 |
|---|---|---|---|---|
| n (%)/x (s) | n (%)/x (s) | n (%)/x (s) | ||
| Age | 46.4 (13.9) | 48.0 (11.8) | 46.3 (14.0) | 0.118 |
| Sex | 0.027 * | |||
| Women | 2902 (73.1) | 146 (80.2) | 2751 (72.8) | |
| Men | 1066 (26.9) | 36 (19.8) | 1030 (27.2) | |
| Professional category 2 | 0.010 * | |||
| Physician | 496 (13.7) | 10 (5.9) | 485 (14.1) | 0.003 * |
| Healthcare training resident | 166 (4.6) | 4 (2.4) | 161 (4.7) | 0.174 |
| Nurse | 834 (23.0) | 42 (24.9) | 791 (22.9) | 0.486 |
| Auxiliary nurse | 663 (18.3) | 33 (19.5) | 630 (18.3) | 0.604 |
| Warden | 303 (8.4) | 19 (11.2) | 283 (8.2) | 0.142 |
| Pregraduate student | 49 (1.4) | 3 (1.8) | 46 (1.3) | 0.393 |
| Other healthcare worker | 300 (8.3) | 12 (7.1) | 288 (8.4) | 0.610 |
| Administrative worker | 242 (6.7) | 21 (11.8) | 221 (6.2) | 0.002 * |
| Other non-healthcare worker | 567 (15.7) | 25 (14.8) | 542 (15.7) | 0.822 |
| Unknown | 349 (8.8) | 13 (7.1) | 334 (8.8) | - |
| Vaccination regimen | <0.001 * | |||
| Double-dosed (completed) | 3913 (98.7) | 170 (93.4) | 3743 (99.0) | |
| Single-dosed 3 | 50 (1.3) | 12 (6.6) | 38 (1.0) | |
| Antecedent of COVID-19 infection 4 | 567 (14.3) | 50 (27.6) | 517 (13.7) | <0.001 * |
| Infection before vaccine | 452 (11.4) | 41 (22.5) | 410 (10.8) | <0.001 * |
| Infection during vaccine | 58 (1.5) | 5 (2.7) | 53 (1.4) | 0.126 |
| Infection after vaccine | 59 (1.5) | 4 (2.2) | 54 (1.4) | 0.275 |
| Hospitalization | 7 (0.2) | 2 (4.0) | 5 (1.0) | 0.124 |
| Serology tests | 1.000 | |||
| Positive IgG after vaccine | 1399 (99.6) | 68 (100.0) | 1331 (99.6) | |
| Negative IgG after vaccine | 6 (0.4) | 0 (0.0) | 6 (0.4) | |
| Unknown | 2564 (64.6) | 114 (62.6) | 2444 (54.3) |
| Adverse Reaction | Total (n) | % of the Total Number of Patients Who Reported Adverse Reactions (n = 182) | % of the Total Sample of Hospital Workers (n = 3969) |
|---|---|---|---|
| General malaise | 95 | 52.2% | 2.4% |
| Fever | 92 | 50.6% | 2.3% |
| Arthromyalgia | 80 | 44.0% | 2.0% |
| Headache | 47 | 25.8% | 1.2% |
| Nausea or vomiting | 26 | 14.3% | 0.7% |
| Dermatologic adverse reactions | 26 | 14.3% | 0.7% |
| Diarrhea | 17 | 9.3% | 0.4% |
| Asthenia | 17 | 9.3% | 0.4% |
| Painful adenopathy | 12 | 6.6% | 0.3% |
| Non-severe neurological symptoms | 12 | 6.6% | 0.3% |
| Neurovegetative symptoms | 12 | 6.6% | 0.3% |
| Catarrhal symptoms | 6 | 3.3% | 0.2% |
| Dyspnea | 5 | 2.7% | 0.1% |
| Vertigo | 4 | 2.2% | 0.1% |
| Variable | Crude Odds Ratio (95% CI) | Adjusted Odds Ratio (95% CI) | p-Value 1 |
|---|---|---|---|
| Sex (women) | 1.52 (1.05–2.20) | 1.51 (1.03–2.20) | 0.033 |
| Age (per year) | 1.01 (1.00–1.01) | 1.01 (1.00–1.01) | 0.108 |
| Vaccination regimen (single-dosed) | 6.95 (3.57–13.55) | 4.92 (2.45–9.89) | <0.001 |
| Antecedent of COVID-19 infection | 2.40 (1.71–3.37) | 2.09 (1.47–2.98) | <0.001 |
| Professional category (physicians) | 0.40 (0.21–0.73) | 0.41 (0.21–0.80) | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Izquierdo, M.; Soler-Iborte, E.; de Rojas, J.P.; Pegalajar-García, M.D.; Gil-Villalba, A.; Ruiz-Villaverde, R.; Valero-Ubierna, M.d.C. Factors Associated with Adverse Reactions to BNT162b2 COVID-19 Vaccine in a Cohort of 3969 Hospital Workers. Vaccines 2022, 10, 15. https://doi.org/10.3390/vaccines10010015
Rivera-Izquierdo M, Soler-Iborte E, de Rojas JP, Pegalajar-García MD, Gil-Villalba A, Ruiz-Villaverde R, Valero-Ubierna MdC. Factors Associated with Adverse Reactions to BNT162b2 COVID-19 Vaccine in a Cohort of 3969 Hospital Workers. Vaccines. 2022; 10(1):15. https://doi.org/10.3390/vaccines10010015
Chicago/Turabian StyleRivera-Izquierdo, Mario, Eva Soler-Iborte, Javier Pérez de Rojas, María Dolores Pegalajar-García, Ana Gil-Villalba, Ricardo Ruiz-Villaverde, and María del Carmen Valero-Ubierna. 2022. "Factors Associated with Adverse Reactions to BNT162b2 COVID-19 Vaccine in a Cohort of 3969 Hospital Workers" Vaccines 10, no. 1: 15. https://doi.org/10.3390/vaccines10010015
APA StyleRivera-Izquierdo, M., Soler-Iborte, E., de Rojas, J. P., Pegalajar-García, M. D., Gil-Villalba, A., Ruiz-Villaverde, R., & Valero-Ubierna, M. d. C. (2022). Factors Associated with Adverse Reactions to BNT162b2 COVID-19 Vaccine in a Cohort of 3969 Hospital Workers. Vaccines, 10(1), 15. https://doi.org/10.3390/vaccines10010015