
Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors

 , , ,
, , , 
Abstract
:1. Introduction
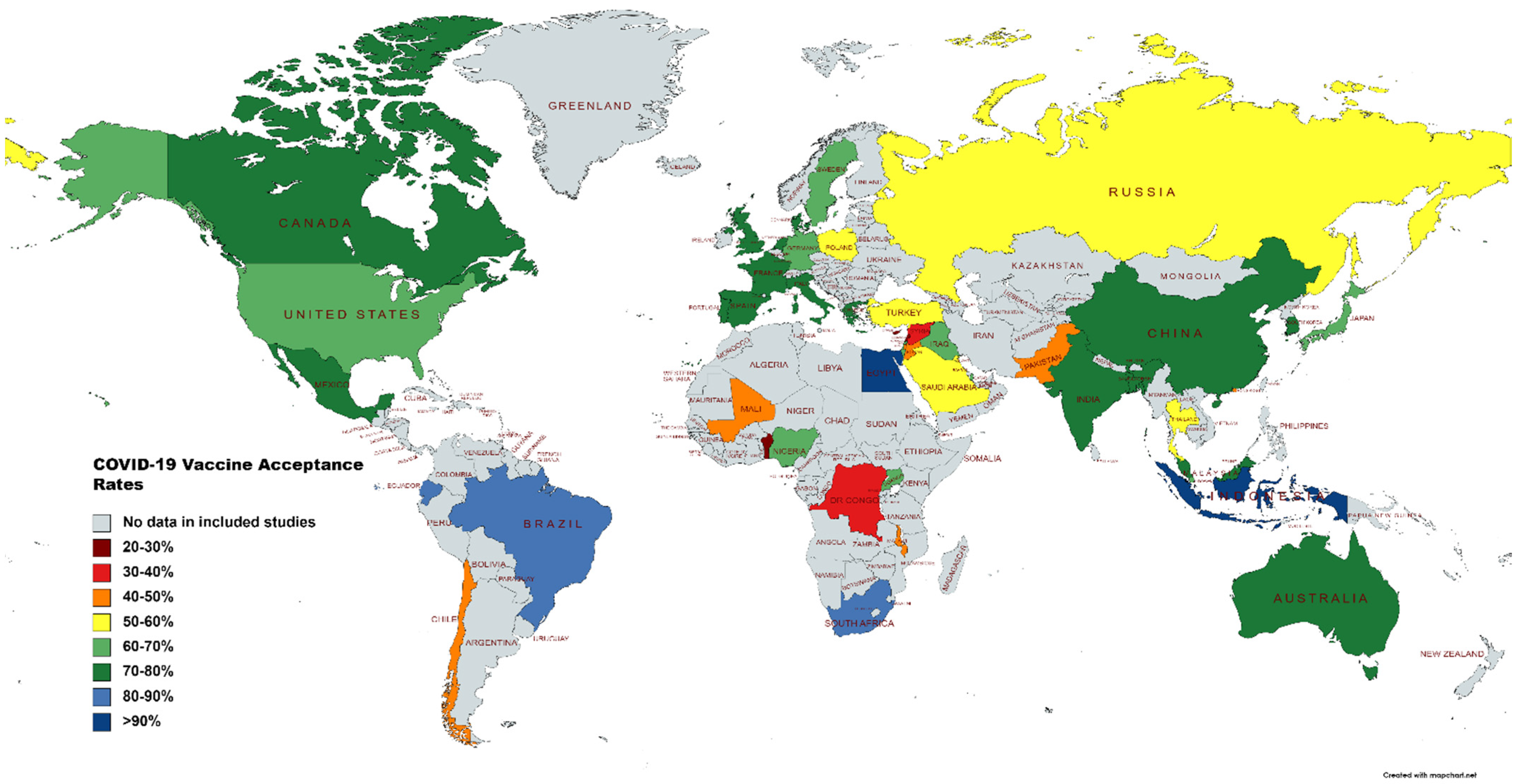
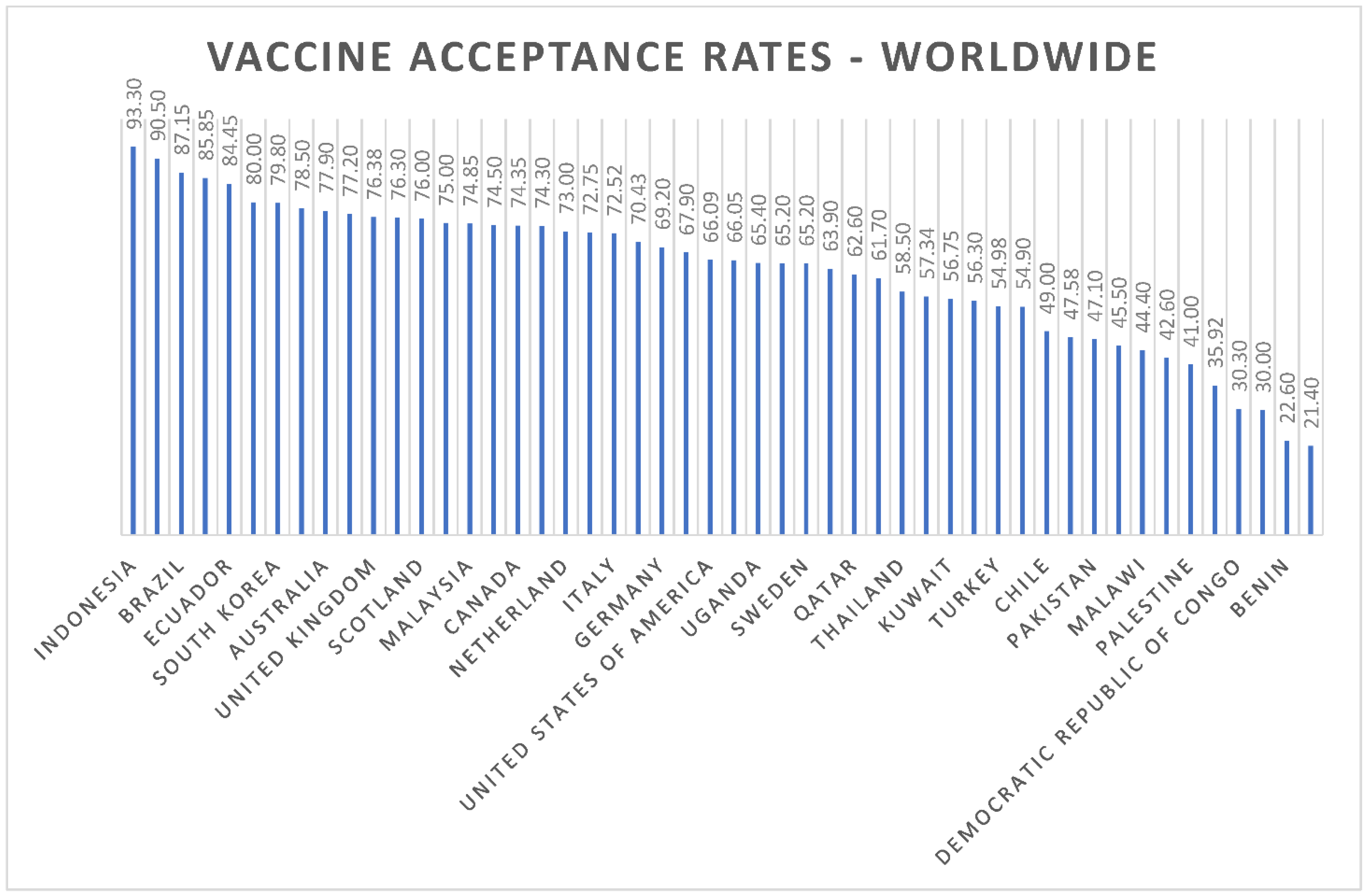
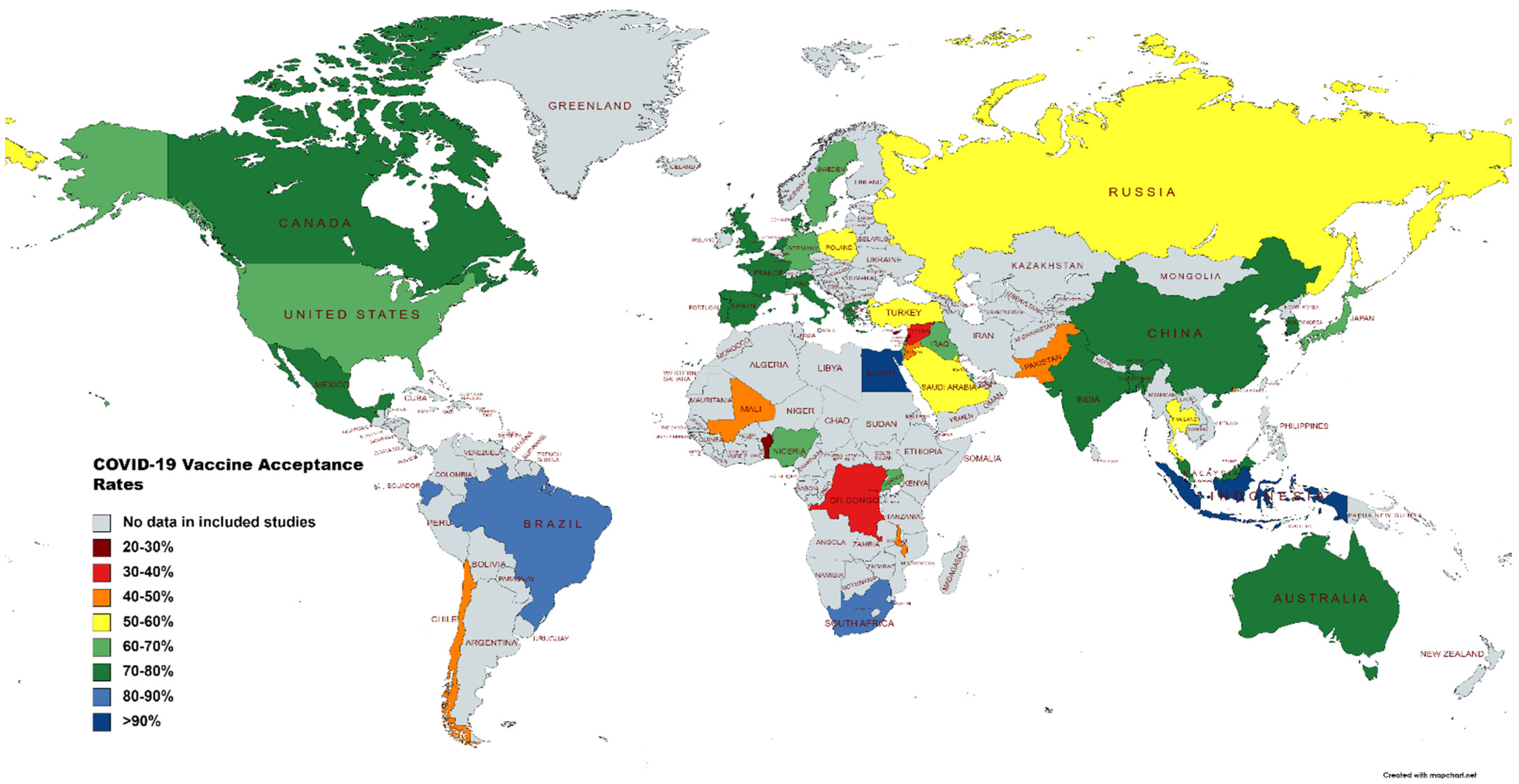
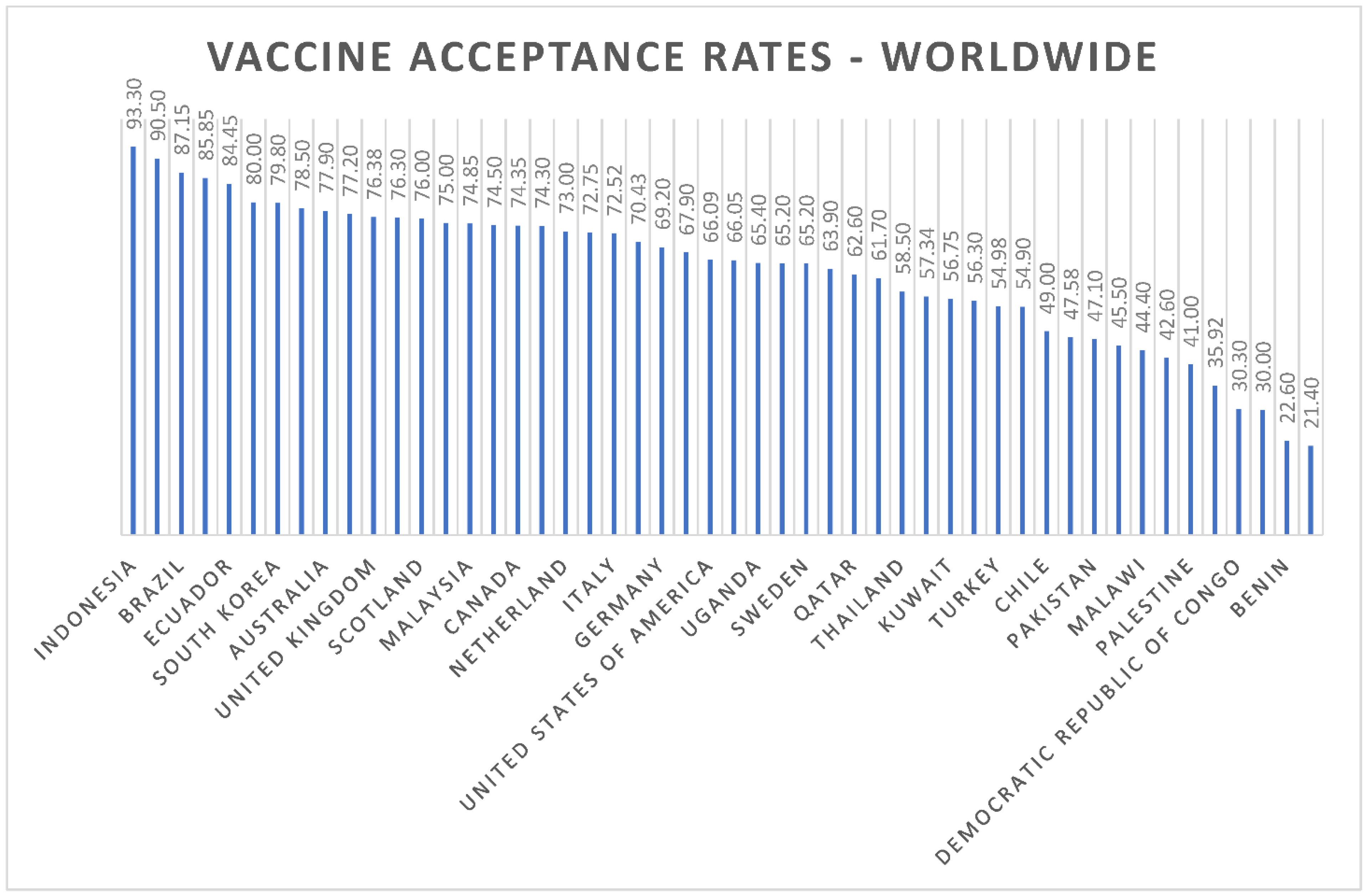
- How do the COVID-19 vaccine-acceptance rates differ among different countries?
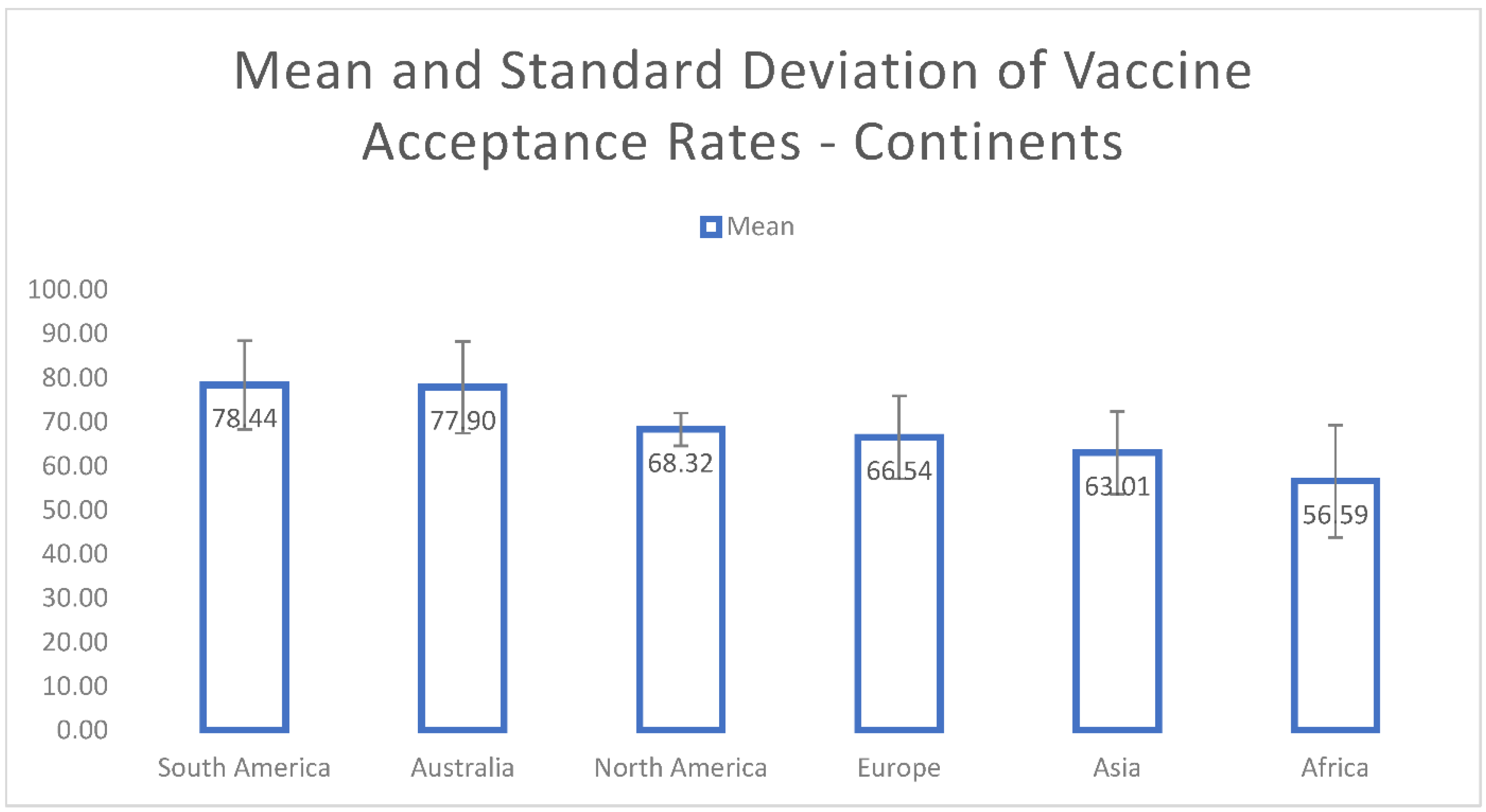
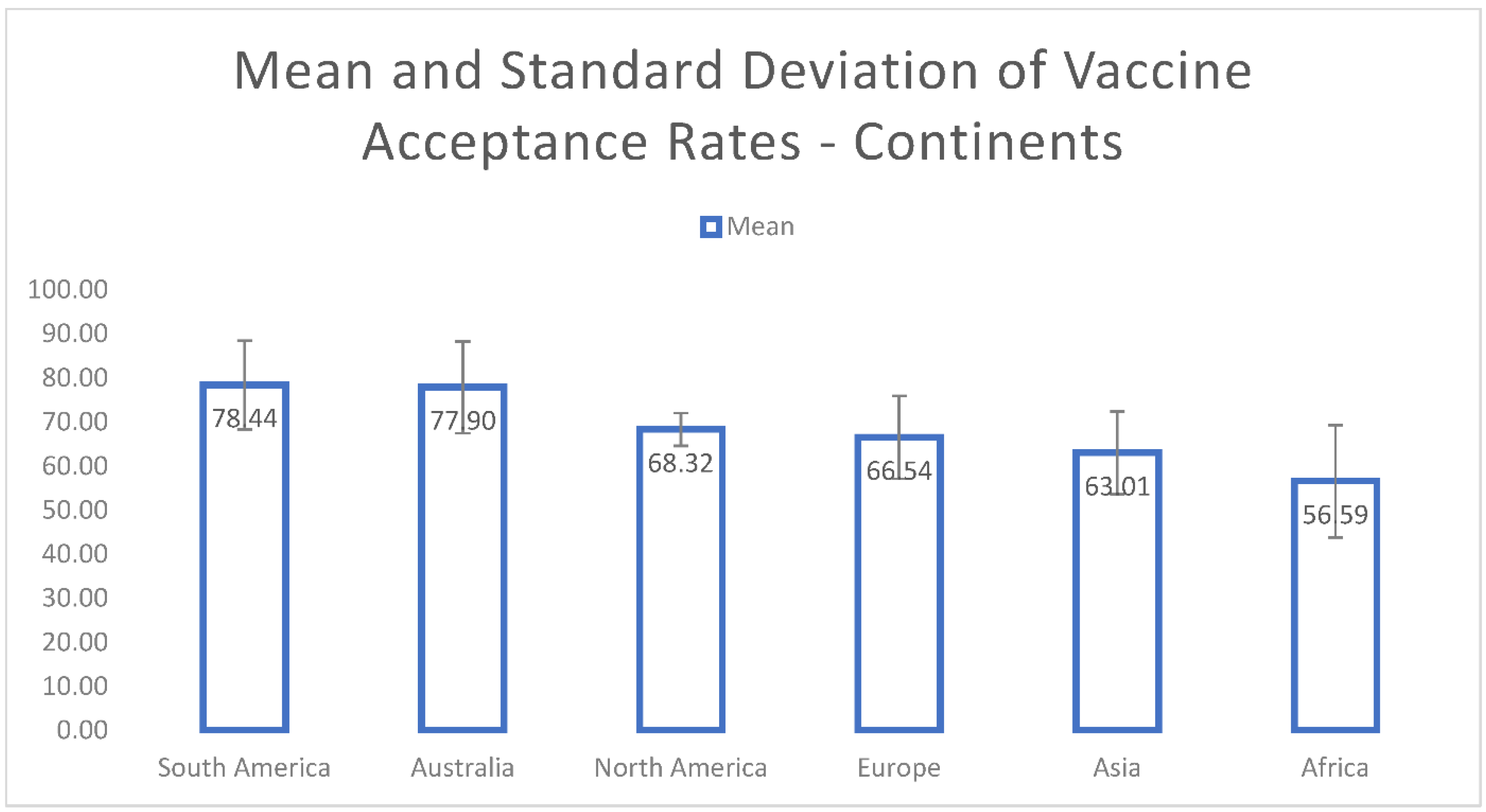
- How do the COVID-19 vaccine-acceptance rates differ among different continents?
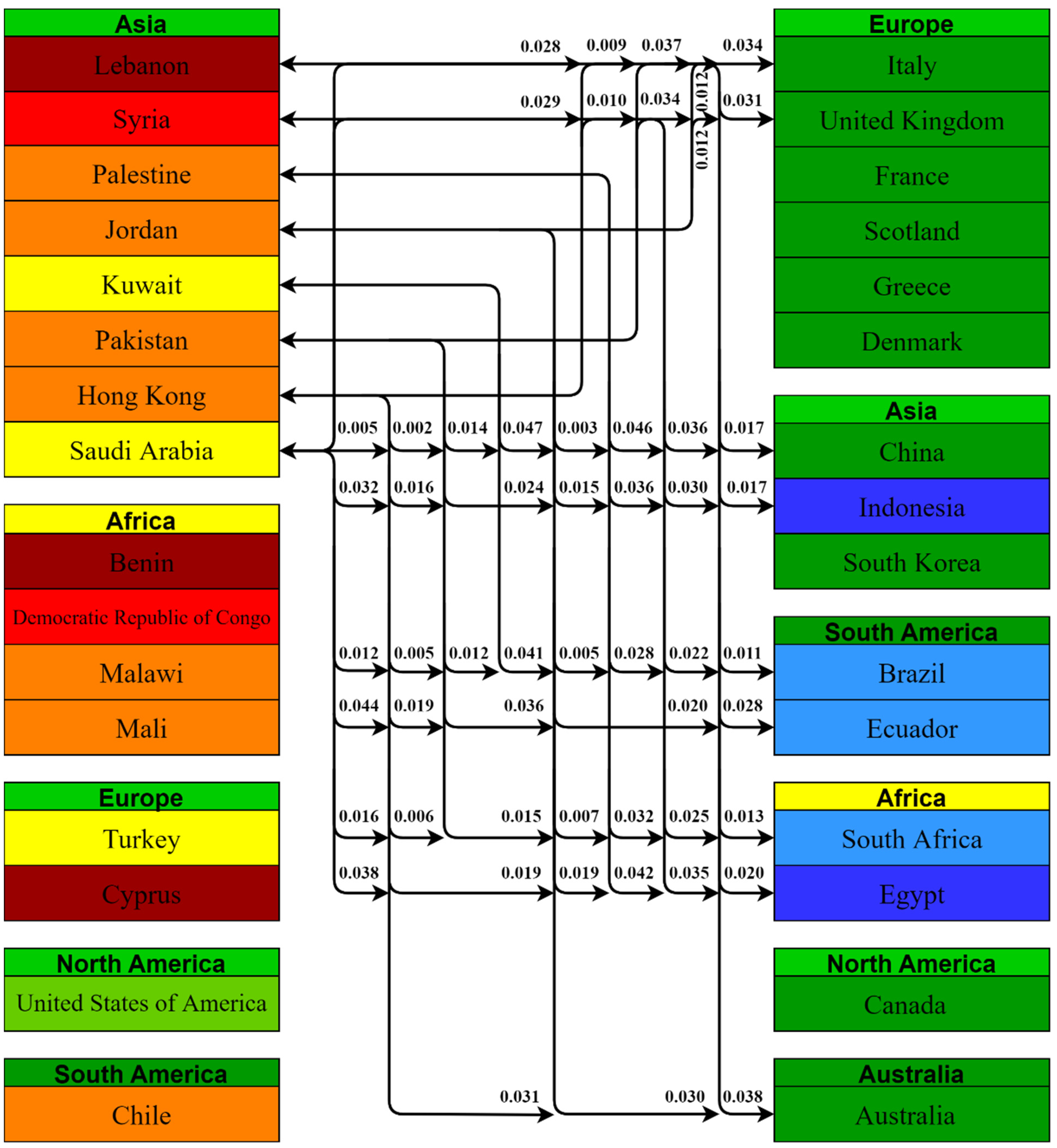
- What social and behavioral factors are responsible for country-level differences in COVID-19 vaccine-acceptance rates?
- A systematic and comparative study about the variations in COVID-19 vaccine-acceptance rates across different countries and continents.
- Statistical analysis of the reported COVID-19 vaccine-acceptance rates.
- Determination of associated social and behavioral factors in relation to COVID-19 vaccine acceptance and vaccine hesitancy.
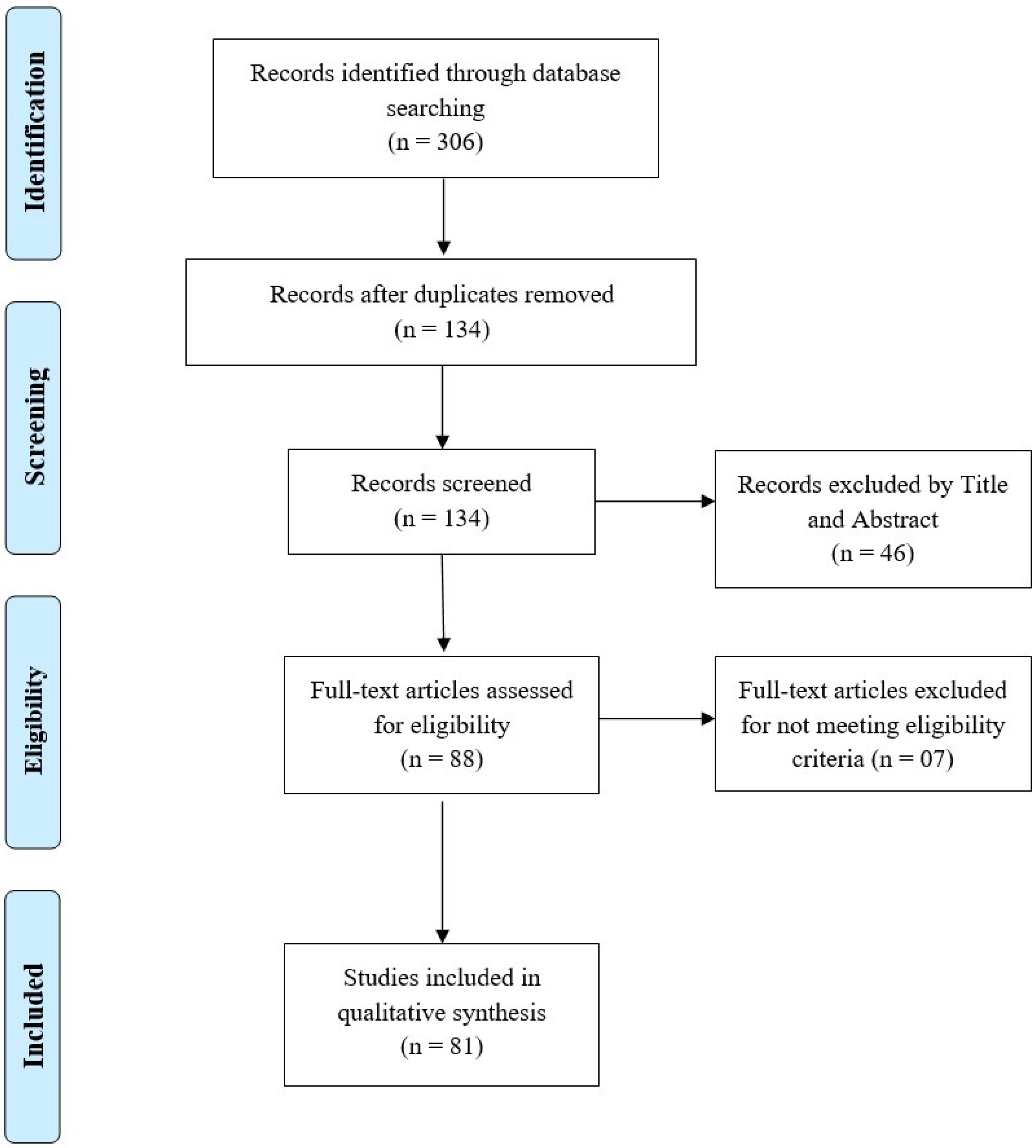
2. Materials and Methods
2.1. Information Sources and Search Strategy
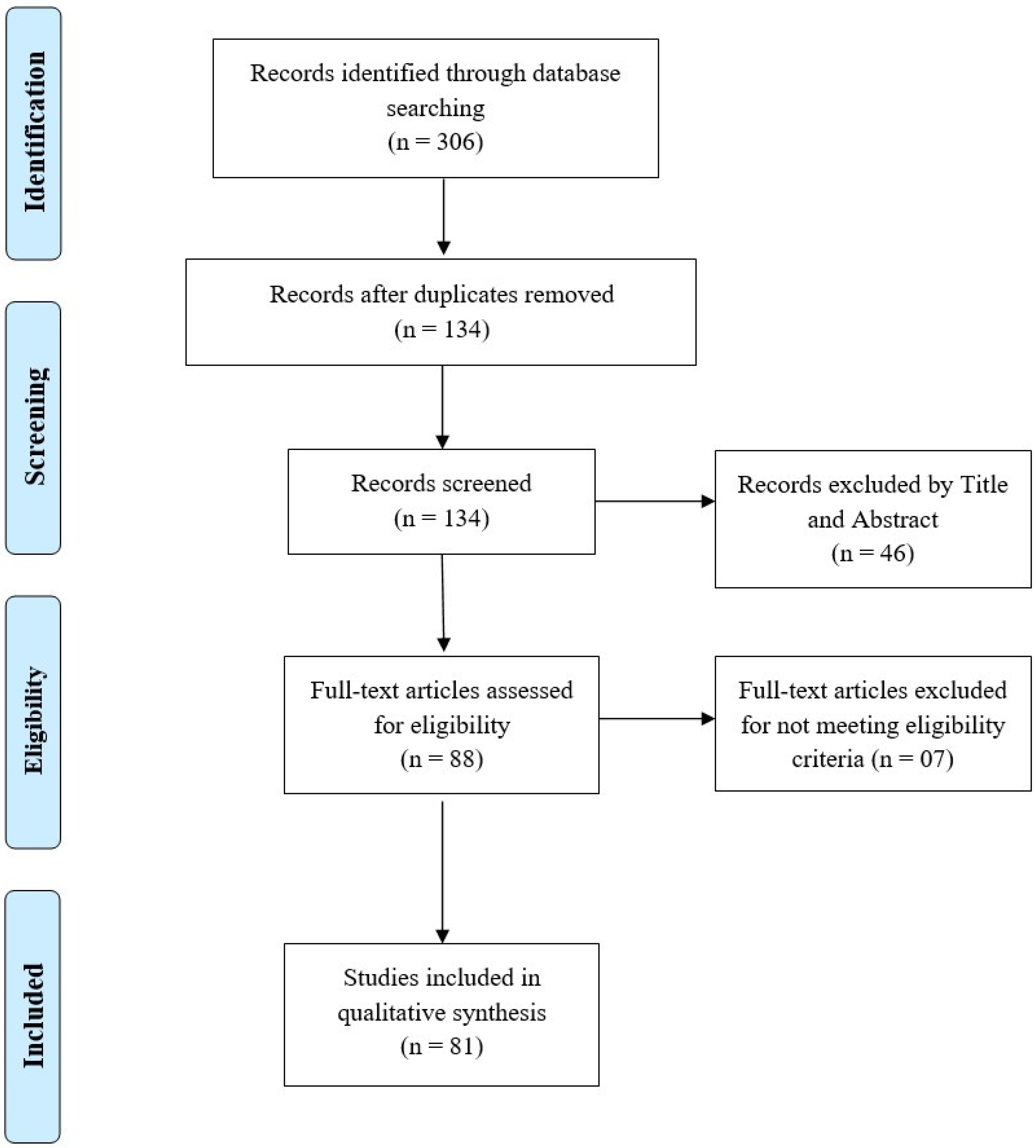
2.2. Study Selection
2.3. Eligibility Criteria
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Papers Included
3.2. Rates of COVID-19 Vaccine Acceptance
3.3. Demographic Factors Influencing COVID-19 Vaccine-Acceptance Rates
3.3.1. North America
3.3.2. South America
3.3.3. Europe
3.3.4. Australia
3.3.5. Asia
3.3.6. Africa
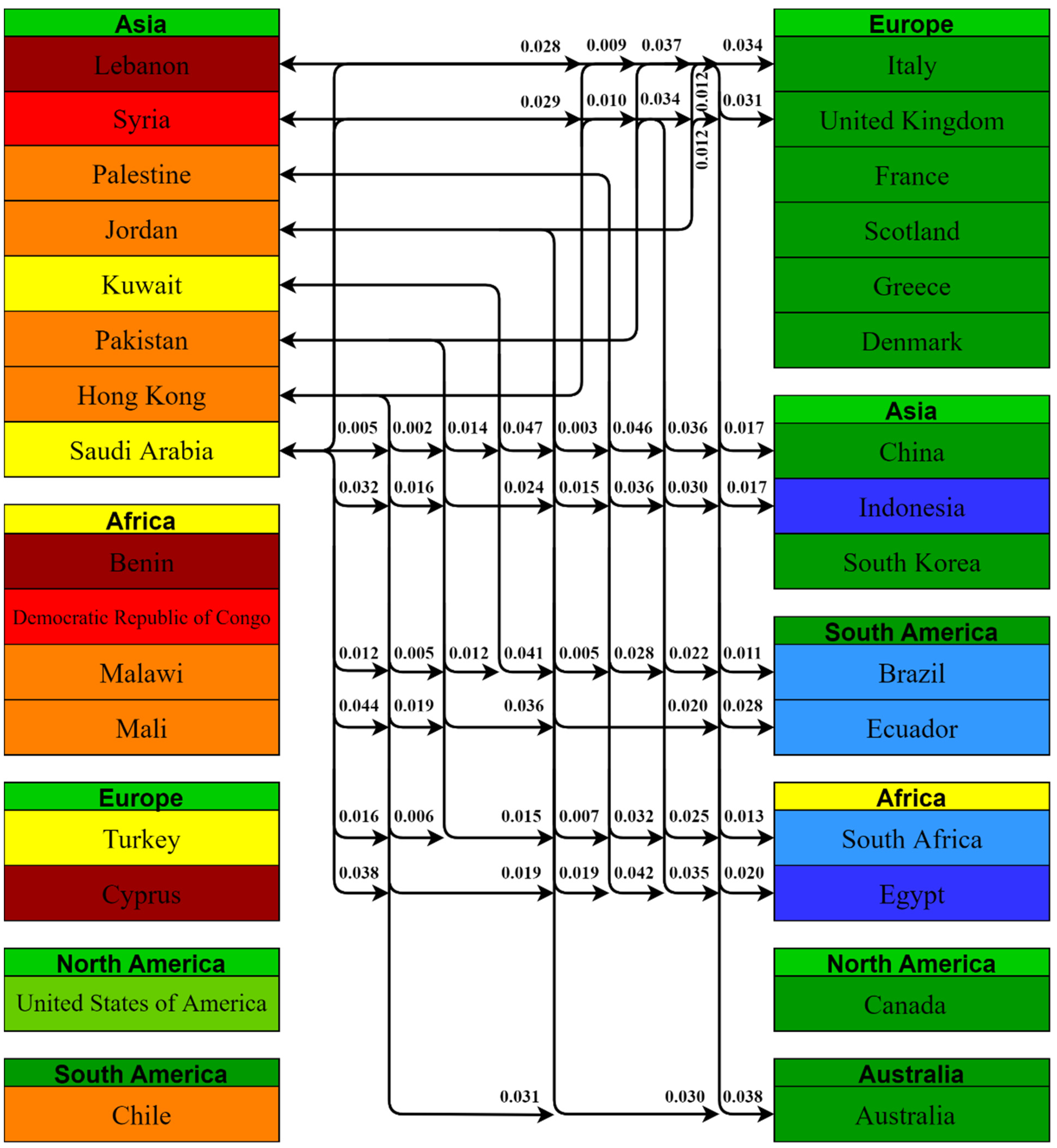
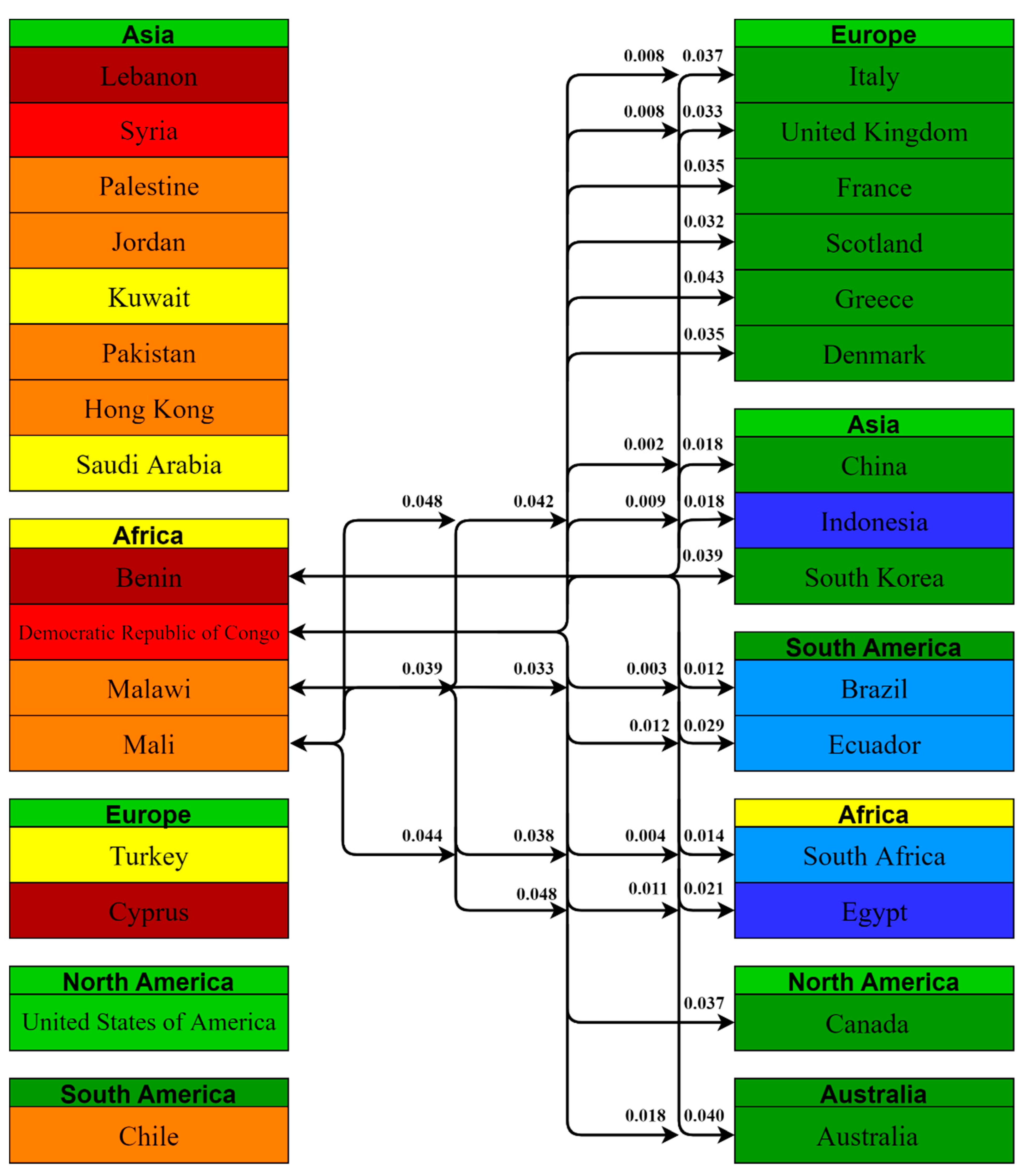
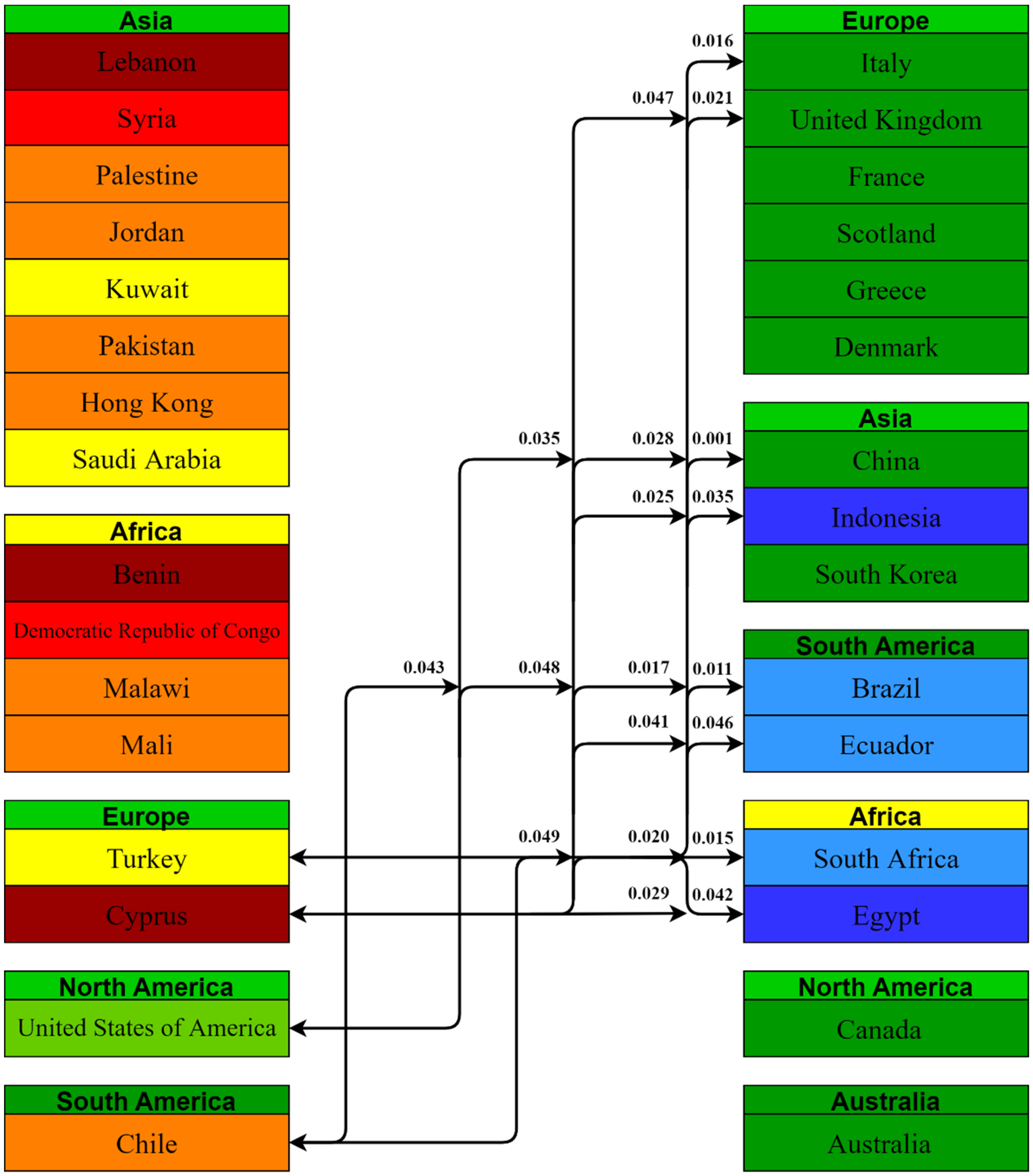
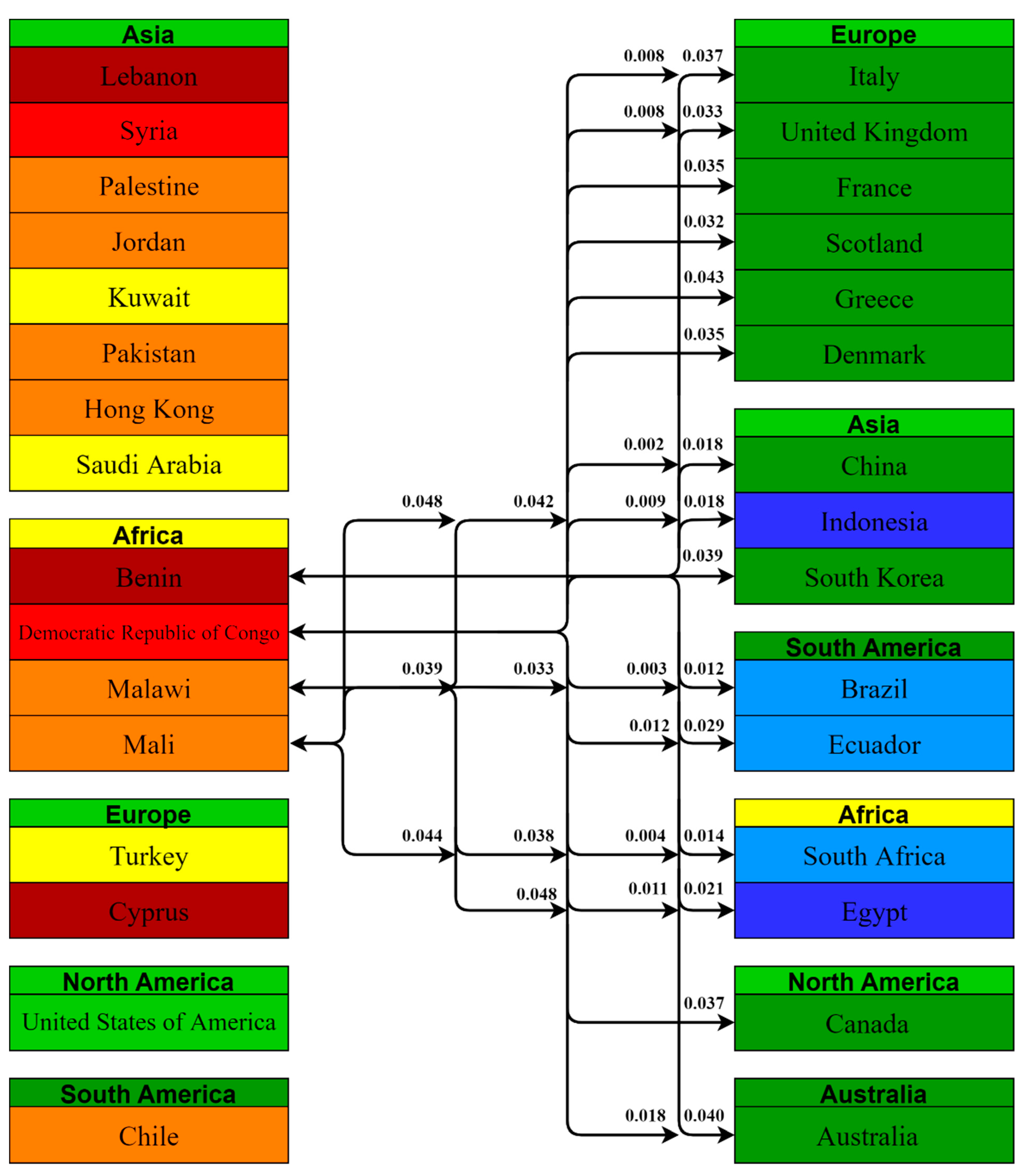
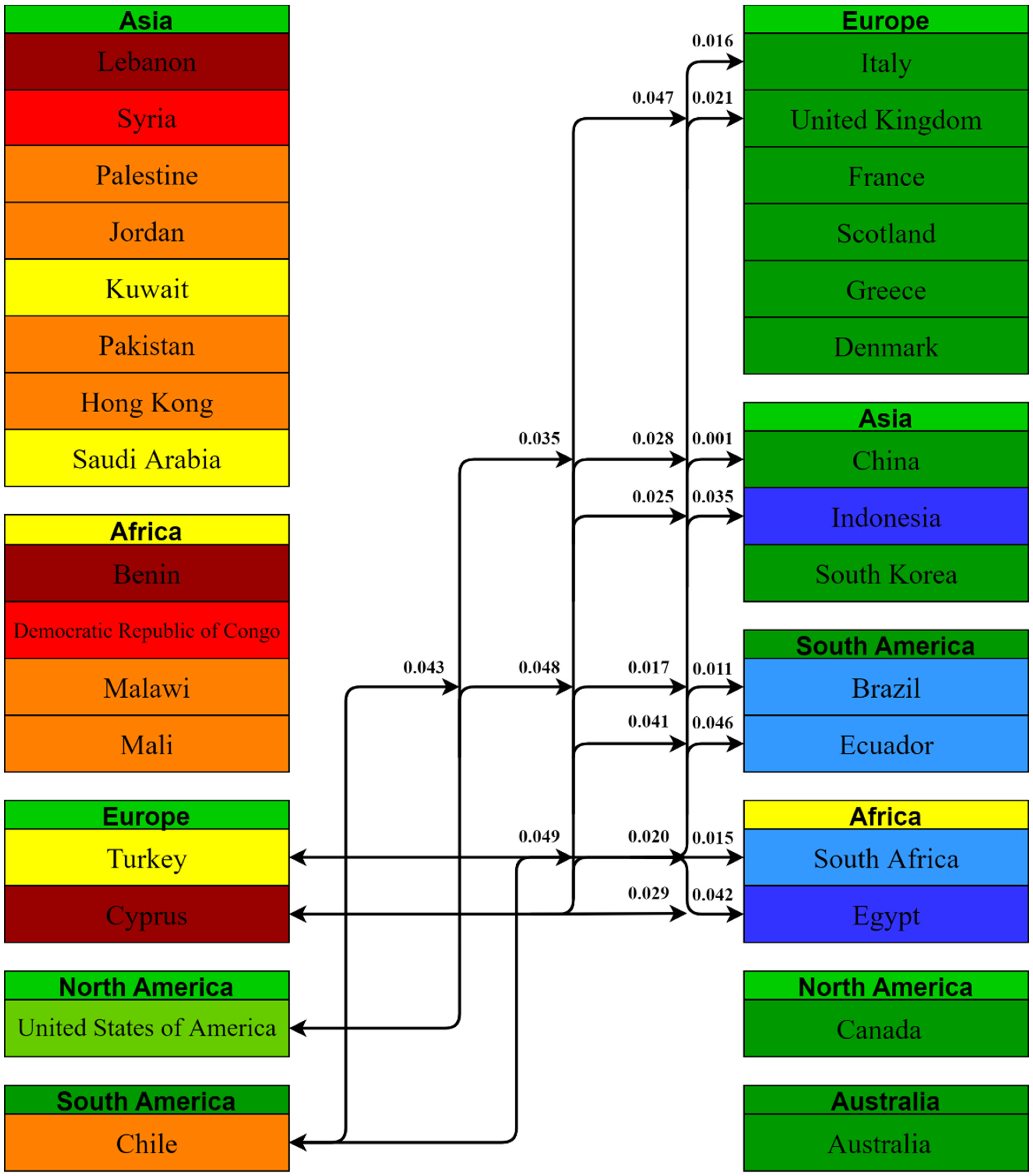
3.4. Comparisons between Countries
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pišot, S.; Milovanović, I.; Šimunič, B.; Gentile, A.; Bosnar, K.; Prot, F.; Bianco, A.; Lo Coco, G.; Bartoluci, S.; Katović, D.; et al. Maintaining everyday life praxis in the time of COVID-19 pandemic measures (ELP-COVID-19 survey). Eur. J. Public Health 2020, 30, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Lades, L.K.; Laffan, K.; Daly, M.; Delaney, L. Daily emotional well-being during the COVID-19 pandemic. Br. J. Health Psychol. 2020, 25, 902–911. [Google Scholar] [CrossRef]
- Patrick, S.W.; Henkhaus, L.E.; Zickafoose, J.S.; Lovell, K.; Halvorson, A.; Loch, S.; Letterie, M.; Davis, M.M. Well-being of parents and children during the COVID-19 pandemic: A national survey. Pediatrics 2020, 146, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Aslam, F.; Awan, T.M.; Syed, J.H.; Kashif, A.; Parveen, M. Sentiments and emotions evoked by news headlines of coronavirus disease (COVID-19) outbreak. Hum. Soc. Sci. Commun. 2020, 7, 1–9. [Google Scholar] [CrossRef]
- Dariya, B.; Nagaraju, G.P. Understanding novel COVID-19: Its impact on organ failure and risk assessment for diabetic and cancer patients. Cytokine Growth Factor Rev. 2020, 53, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Lake, M.A. What we know so far: COVID-19 current clinical knowledge and research. Clin. Med. 2020, 20, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dey, S.K.; Rahman, M.M.; Siddiqi, U.R.; Howlader, A. Analyzing the epidemiological outbreak of COVID-19: A visual exploratory data analysis approach. J. Med. Virol. 2020, 92, 632–638. [Google Scholar] [CrossRef]
- Koh, D. COVID-19 lockdowns throughout the world. Occup. Med. 2020, 70, 322. [Google Scholar] [CrossRef]
- Fathollahi-Fard, A.M.; Ahmadi, A.; Karimi, B. Multi-Objective Optimization of Home Healthcare with Working-Time Balancing and Care Continuity. Sustainability 2021, 13, 12431. [Google Scholar] [CrossRef]
- Fathollahi-Fard, A.M.; Hajiaghaei-Keshteli, M.; Tavakkoli-Moghaddam, R.; Smith, N.R. Bi-level programming for home health care supply chain considering outsourcing. J. Ind. Inf. Integr. 2021, 25, 100246. [Google Scholar] [CrossRef]
- Al-Quteimat, O.M.; Amer, A.M. The impact of the COVID-19 pandemic on cancer patients. Am. J. Clin. Oncol. 2020, 43, 452–455. [Google Scholar] [CrossRef]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Shafaghi, A.H.; Talabazar, F.R.; Koşar, A.; Ghorbani, M. On the effect of the respiratory droplet generation condition on COVID-19 transmission. Fluids 2020, 5, 113. [Google Scholar] [CrossRef]
- Deprest, J.; Choolani, M.; Chervenak, F.; Farmer, D.; Lagrou, K.; Lopriore, E.; McCullough, L.; Olutoye, O.; Simpson, L.; Van Mieghem, T.; et al. Fetal diagnosis and therapy during the COVID-19 pandemic: Guidance on behalf of the international fetal medicine and surgery society. Fetal Diagn. Ther. 2020, 47, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Caparros-Gonzalez, R.A.; Ganho-Ávila, A.; Torre-Luque, A.d.l. The COVID-19 Pandemic Can Impact Perinatal Mental Health and the Health of the Offspring; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2020. [Google Scholar]
- Sade, S.; Sheiner, E.; Wainstock, T.; Hermon, N.; Yaniv Salem, S.; Kosef, T.; Lanxner Battat, T.; Oron, S.; Pariente, G. Risk for depressive symptoms among hospitalized women in high-risk pregnancy units during the COVID-19 pandemic. J. Clin. Med. 2020, 9, 2449. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Hompes, T.; Foulon, V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: A call for action. Int. J. Gynecol. Obstet. 2020, 151, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Barone Gibbs, B.; Kline, C.E.; Stoner, L. COVID-19 impact on behaviors across the 24-h day in children and adolescents: Physical activity, sedentary behavior, and sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef]
- Xue, A.; Oros, V.; Marca-Ghaemmaghami, P.L.; Scholkmann, F.; Righini-Grunder, F.; Natalucci, G.; Karen, T.; Bassler, D.; Restin, T. New parents experienced lower parenting self-efficacy during the COVID-19 pandemic lockdown. Children 2021, 8, 79. [Google Scholar] [CrossRef]
- Chang, C.-L.; McAleer, M.; Wong, W.-K. Risk and Financial Management of COVID-19 in Business, Economics and Finance; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2020. [Google Scholar]
- Singer, D.R. Health policy and technology challenges in responding to the COVID-19 pandemic. Health Policy Technol. 2020, 9, 123. [Google Scholar] [CrossRef]
- Angrup, A.; Kanaujia, R.; Ray, P.; Biswal, M. Healthcare facilities in low-and middle-income countries affected by COVID-19: Time to upgrade basic infection control and prevention practices. Indian J. Med. Microb. 2020, 38, 139–143. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Chatzittofis, A.; Karanikola, M.; Michailidou, K.; Constantinidou, A. Impact of the COVID-19 Pandemic on the Mental Health of Healthcare Workers. Int. J. Environ. Res. Public Health 2021, 18, 1435. [Google Scholar] [CrossRef]
- Andreadakis, Z.; Kumar, A.; Román, R.G.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar]
- Graham, B.S. Rapid COVID-19 vaccine development. Science 2020, 368, 945–946. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhao, S.; Ou, J.; Zhang, J.; Lan, W.; Guan, W.; Wu, X.; Yan, Y.; Zhao, W.; Wu, J.; et al. COVID-19: Vaccine Development Updates. Front. Immunol. 2020, 11, 3435. [Google Scholar] [CrossRef]
- Yan, Y.; Pang, Y.; Lyu, Z.; Wang, R.; Wu, X.; You, C.; Zhao, H.; Manickam, S.; Lester, E.; Wu, T.; et al. The COVID-19 vaccines: Recent development, challenges and prospects. Vaccines 2021, 9, 349. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Dowling, W.E.; Román, R.G.; Chaudhari, A.; Gurry, C.; Le, T.T.; Tollefson, S.; Clark, C.E.; Bernasconi, V.; Kristiansen, P.A. Status report on COVID-19 vaccines development. Curr. Infect. Dis. Rep. 2021, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Prüβ, B.M. Current state of the first COVID-19 vaccines. Vaccines 2021, 9, 30. [Google Scholar] [CrossRef]
- Mannan, D.K.A.; Farhana, K.M. Knowledge, attitude and acceptance of a COVID-19 vaccine: A global cross-sectional study. Int. Res. J. Bus. Soc. Sci. 2020, 6, 1–23. [Google Scholar] [CrossRef]
- Feleszko, W.; Lewulis, P.; Czarnecki, A. Waszkiewicz Flattening the curve of COVID-19 vaccine rejection—An international overview. Vaccines 2021, 9, 44. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Bono, S.A.; Faria de Moura Villela, E.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors Affecting COVID-19 Vaccine Acceptance: An International Survey among Low-and Middle-Income Countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Wake, A.D. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: Vaccination Refusal Could Prolong the War of This Pandemic A Systematic Review. Risk Manag. Healthc. Policy 2021, 14, 2609–2623. [Google Scholar] [CrossRef] [PubMed]
- Selçuk, A.A. A guide for systematic reviews: PRISMA. Turk. Arch. Otorhinolaryngol. 2019, 57, 57. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, Y.; Long, S.; Fu, X.; Zhang, X.; Zhao, S.; Xiu, S.; Wang, X.; Lu, B.; Jin, H. Non-EPI Vaccine Hesitancy among Chinese Adults: A Cross-Sectional Study. Vaccines 2021, 9, 772. [Google Scholar] [CrossRef]
- Xu, B.; Gao, X.; Zhang, X.; Hu, Y.; Yang, H.; Zhou, Y.-H. Real-World Acceptance of COVID-19 Vaccines among Healthcare Workers in Perinatal Medicine in China. Vaccines 2021, 9, 704. [Google Scholar] [CrossRef]
- Liu, R.; Zhang, Y.; Nicholas, S.; Leng, A.; Maitland, E.; Wang, J. COVID-19 Vaccination Willingness among Chinese Adults under the Free Vaccination Policy. Vaccines 2021, 9, 292. [Google Scholar] [CrossRef] [PubMed]
- Gan, L.; Chen, Y.; Hu, P.; Wu, D.; Zhu, Y.; Tan, J.; Li, Y.; Zhang, D. Willingness to receive SARS-CoV-2 vaccination and associated factors among Chinese adults: A cross sectional survey. Int. J. Environ. Res. Public Health 2021, 18, 1993. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.N.; Zhang, T.; Peng, X.Q.; Ge, J.J.; Gu, H.; You, H. Vaccine Acceptance and Its Influencing Factors: An Online Cross-Sectional Study among International College Students Studying in China. Vaccines 2021, 9, 585. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, X.; Cao, M.; Xiang, T.; Zhang, J.; Wang, P.; Dai, H. Will Healthcare Workers Accept a COVID-19 Vaccine When It Becomes Available? A Cross-Sectional Study in China. Front. Public Health 2021, 9, 609. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Wang, R.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Liu, M.; Liu, J. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: A multi-center cross-sectional study based on health belief model. Hum. Vaccines Immunother. 2021, 17, 1–10. [Google Scholar] [CrossRef]
- Chen, M.; Li, Y.; Chen, J.; Wen, Z.; Feng, F.; Zou, H.; Fu, C.; Chen, L.; Shu, Y.; Sun, C. An online survey of the attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum. Vaccines Immunother. 2021, 17, 2279–2288. [Google Scholar] [CrossRef]
- Han, K.; Francis, M.R.; Zhang, R.; Wang, Q.; Xia, A.; Lu, L.; Yang, B.; Hou, Z. Confidence, Acceptance and Willingness to Pay for the COVID-19 Vaccine among Migrants in Shanghai, China: A Cross-Sectional Study. Vaccines 2021, 9, 443. [Google Scholar] [CrossRef]
- Fayed, A.A.; Al Shahrani, A.S.; Almanea, L.T.; Alsweed, N.I.; Almarzoug, L.M.; Almuwallad, R.I.; Almugren, W.F. Willingness to Receive the COVID-19 and Seasonal Influenza Vaccines among the Saudi Population and Vaccine Uptake during the Initial Stage of the National Vaccination Campaign: A Cross-Sectional Survey. Vaccines 2021, 9, 765. [Google Scholar] [CrossRef]
- Qattan, A.M.N.; Alshareef, N.; Alsharqi, O.; al Rahahleh, N.; Chirwa, G.C.; Al-Hanawi, K.M. Acceptability of a COVID-19 Vaccine Among Healthcare Workers in the Kingdom of Saudi Arabia. Front. Med. 2021, 8, 83. [Google Scholar] [CrossRef]
- Alfageeh, E.I.; Alshareef, N.; Angawi, K.; Alhazmi, F.; Chirwa, G.C. Acceptability of a COVID-19 Vaccine among the Saudi Population. Vaccines 2021, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, S.M.; Dehom, S.; Almutairi, D.; Alnasser, B.S.; Alsaif, B.; Alabdrabalnabi, A.A.; Bin Rahmah, A.; Alshahrani, M.S.; El-Metwally, A.; Al-Khateeb, B.F.; et al. Acceptability of COVID-19 vaccination in Saudi Arabia: A cross-sectional study using a web-based survey. Hum. Vaccines Immunother. 2021, 17, 3338–3347. [Google Scholar] [CrossRef]
- Awadhi, E.A.; Zein, D.; Mallallah, F.; Haider, N.B.; Hossain, A. Monitoring COVID-19 Vaccine Acceptance in Kuwait During the Pandemic: Results from a National Serial Study. Risk Manag. Healthc. Policy 2021, 14, 1413–1429. [Google Scholar] [CrossRef] [PubMed]
- Alqudeimat, Y.; Alenezi, D.; AlHajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A.H. Acceptance of a COVID-19 vaccine and its related determinants among the general adult population in Kuwait. Med. Princ. Pract. 2021, 30, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: A study in Jordan and Kuwait among other Arab countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Al-Qerem, W.A.; Jarab, A.S. COVID-19 Vaccination Acceptance and Its Associated Factors Among a Middle Eastern Population. Front. Public Health 2021, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef]
- Yan, E.; Lai, D.W.; Lee, V.W. Predictors of Intention to Vaccinate against COVID-19 in the General Public in Hong Kong: Findings from a Population-Based, Cross-Sectional Survey. Vaccines 2021, 9, 696. [Google Scholar] [CrossRef] [PubMed]
- Luk, T.T.; Zhao, S.; Wu, Y.; Wong, J.Y.-h.; Wang, M.P.; Lam, T.H. Prevalence and determinants of SARS-CoV-2 vaccine hesitancy in Hong Kong: A population-based survey. Vaccine 2021, 39, 3602–3607. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Acceptance of a COVID-19 Vaccine in Japan during the COVID-19 Pandemic. Vaccines 2021, 9, 210. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Katsuyama, H. Willingness to receive COVID-19 vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, F.A.; Ahmad, B.; Khalid, M.D.; Fazal, A.; Javaid, M.M.; Butt, Q.D. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum. Vaccines Immunother. 2021, 17, 3365–3370. [Google Scholar] [CrossRef] [PubMed]
- Arshad, M.S.; Hussain, I.; Mahmood, T.; Hayat, K.; Majeed, A.; Imran, I.; Saeed, H.; Iqbal, M.O.; Uzair, M.; Ashraf, W.; et al. A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability, Preference, and Willingness to Pay among the General Population of Pakistan. Vaccines 2021, 9, 720. [Google Scholar] [CrossRef] [PubMed]
- Al-Mulla, R.; Abu-Madi, M.; Talafha, Q.M.; Tayyem, R.F.; Abdallah, A.M. COVID-19 Vaccine Hesitancy in a Representative Education Sector Population in Qatar. Vaccines 2021, 9, 665. [Google Scholar] [CrossRef] [PubMed]
- Abedin, M.; Islam, M.A.; Rahman, F.N.; Reza, H.M.; Hossain, M.Z.; Hossain, M.A.; Arefin, A.; Hossain, A. Willingness to vaccinate against COVID-19 among Bangladeshi adults: Understanding the strategies to optimize vaccination coverage. PLoS ONE 2021, 16, e0250495. [Google Scholar] [CrossRef]
- Al Halabi, C.K.; Obeid, S.; Sacre, H.; Akel, M.; Hallit, R.; Salameh, P.; Hallit, S. Attitudes of Lebanese adults regarding COVID-19 vaccination. BMC Public Health 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the acceptance of COVID-19 vaccine among healthcare workers and general population using health belief model. J. Eval. Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef]
- Mohamad, O.; Zamlout, A.; AlKhoury, N.; Mazloum, A.; Alsalkini, M.; Shaaban, R. Factors associated with the intention of Syrian adult population to accept COVID19 vaccination: A cross-sectional study. BMC Public Health 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Rabi, R.; Maraqa, B.; Nazzal, Z.; Zink, T. Factors affecting nurses’ intention to accept the COVID-9 vaccine: A cross-sectional study. Public Health Nurs. 2021, 38, 781–788. [Google Scholar] [CrossRef]
- Zigron, A.; Dror, A.A.; Morozov, N.; Shani, T.; Haj Khalil, T.; Eisenbach, N.; Rayan, D.; Daoud, A.; Kablan, F.; Sela, E.; et al. COVID-19 vaccine acceptance among dental professionals based on employment status during the pandemic. Front. Med. 2021, 8, 13. [Google Scholar] [CrossRef]
- Lin, Y.L.; Hu, Z.J.; Zhao, Q.J.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental acceptability of COVID-19 vaccination for children under the age of 18 years: Cross-sectional online survey. Jmir Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: A web-based national survey. J. Multidiscip. Healthc. 2020, 13, 1657. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Fedele, F.; Aria, M.; Esposito, V.; Micillo, M.; Cecere, G.; Spano, M.; De Marco, G. COVID-19 vaccine hesitancy: A survey in a population highly compliant to common vaccinations. Hum. Vaccines Immunother. 2021, 17, 1–7. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV-2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef]
- Del Riccio, M.; Boccalini, S.; Rigon, L.; Biamonte, M.A.; Albora, G.; Giorgetti, D.; Bonanni, P.; Bechini, A. Factors Influencing SARS-CoV-2 Vaccine Acceptance and Hesitancy in a Population-Based Sample in Italy. Vaccines 2021, 9, 633. [Google Scholar] [CrossRef]
- Trabucco Aurilio, M.; Mennini, F.S.; Gazzillo, S.; Massini, L.; Bolcato, M.; Feola, A.; Ferrari, C.; Coppeta, L. Intention to be vaccinated for COVID-19 among Italian nurses during the pandemic. Vaccines 2021, 9, 500. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, F.; Montalti, M.; Di Valerio, Z.; Mannucci, E.; Nreu, B.; Monami, M.; Gori, D. Rate and Predictors of Hesitancy toward SARS-CoV-2 Vaccine among Type 2 Diabetic Patients: Results from an Italian Survey. Vaccines 2021, 9, 460. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Pelullo, C.P.; della Polla, G.; Pavia, M.; Angelillo, I.F. Exploring the willingness to accept SARS-CoV-2 vaccine in a University population in Southern Italy, September to November 2020. Vaccines 2021, 9, 275. [Google Scholar] [CrossRef] [PubMed]
- İkiışık, H.; Sezerol, M.A.; Taşçı, Y.; Maral, I. COVID-19 Vaccine Hesitancy: A Community-Based Research in Turkey. Int. J. Clin. Pract. 2021, 75, e14336. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 vaccine acceptance of healthcare providers in a tertiary Pediatric hospital. Hum. Vaccines Immunother. 2021, 17, 1–5. [Google Scholar] [CrossRef]
- Yurttas, B.; Poyraz, B.C.; Sut, N.; Ozdede, A.; Oztas, M.; Uğurlu, S.; Tabak, F.; Hamuryudan, V.; Seyahi, E. Willingness to get the COVID-19 vaccine among patients with rheumatic diseases, healthcare workers and general population in Turkey: A web-based survey. Rheumatol. Int. 2021, 41, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Flowers, P.; McLeod, J.; Young, D.; Rollins, L. Social patterning and stability of intention to accept a COVID-19 vaccine in Scotland: Will those most at risk accept a vaccine? Vaccines 2021, 9, 17. [Google Scholar] [CrossRef]
- Fakonti, G.; Kyprianidou, M.; Toumbis, G.; Giannakou, K. Attitudes and Acceptance of COVID-19 Vaccination Among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front. Public Health 2021, 9, 481. [Google Scholar] [CrossRef]
- Papagiannis, D.; Rachiotis, G.; Malli, F.; Papathanasiou, I.V.; Kotsiou, O.; Fradelos, E.C.; Giannakopoulos, K.; Gourgoulianis, K.I. Acceptability of COVID-19 Vaccination among Greek Health Professionals. Vaccines 2021, 9, 200. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, E210–E221. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once We Have It, Will We Use It? A European Survey on Willingness to Be Vaccinated against COVID-19; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 50, 1–15. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 50, 1–3. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.K.; Alleaume, C.; Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Beck, F.; Legleye, S.; et al. The French public’s attitudes to a future COVID-19 vaccine: The politicization of a public health issue. Soc. Sci. Med. 2020, 265, 113414. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Alicandro, G.; Scarpino, V. Attitudes towards influenza vaccine and a potential COVID-19 vaccine in Italy and differences across occupational groups, September 2020. Med. Lav. 2020, 111, 445. [Google Scholar]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Waters, A.R.; Kepka, D.; Ramsay, J.M.; Mann, K.; Vaca Lopez, P.L.; Anderson, J.S.; Ou, J.Y.; Kaddas, H.K.; Palmer, A.; Ray, N.; et al. COVID-19 Vaccine Hesitancy Among Adolescent and Young Adult Cancer Survivors. JNCI Can. Spectr. 2021, 5, pkab049. [Google Scholar] [CrossRef]
- Mascarenhas, A.K.; Lucia, V.C.; Kelekar, A.; Afonso, N.M. Dental students’ attitudes and hesitancy toward COVID-19 vaccine. J. Dent. Educ. 2021, 85, 1504–1510. [Google Scholar] [CrossRef]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.N.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine A Survey of US Adults. Ann. Int. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EclinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J. A proactive approach for managing COVID-19: The importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV-2. Front. Psychol. 2020, 11, 2890. [Google Scholar] [CrossRef]
- Seale, H.; Heywood, A.E.; Leask, J.; Sheel, M.; Durrheim, D.N.; Bolsewicz, K.; Kaur, R. Examining Australian public perceptions and behaviors towards a future COVID-19 vaccine. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.-A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2021, 21, e110. [Google Scholar] [CrossRef]
- Adeniyi, O.V.; Stead, D.; Singata-Madliki, M.; Batting, J.; Wright, M.; Jelliman, E.; Abrahams, S.; Parrish, A. Acceptance of COVID-19 Vaccine among the Healthcare Workers in the Eastern Cape, South Africa: A Cross Sectional Study. Vaccines 2021, 9, 666. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of vaccination against COVID-19 among healthcare workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103. [Google Scholar] [CrossRef]
- Cerda, A.A.; Garcia, L.Y. Hesitation and Refusal Factors in Individuals’ Decision-Making Processes Regarding a Coronavirus Disease 2019 Vaccination. Front. Public Health 2021, 9, 1–14. [Google Scholar] [CrossRef]
- Sarasty, O.; Carpio, C.E.; Hudson, D.; Guerrero-Ochoa, P.A.; Borja, I. The demand for a COVID-19 vaccine in Ecuador. Vaccine 2020, 38, 8090–8098. [Google Scholar] [CrossRef]
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4464. [Google Scholar] [CrossRef]
- Cyranoski, D. What China’s speedy COVID vaccine deployment means for the pandemic. Nature 2020, 586, 343–345. [Google Scholar] [CrossRef]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1338–1339. [Google Scholar] [CrossRef]
- Burgess, R.A.; Osborne, R.H.; Yongabi, K.A.; Greenhalgh, T.; Gurdasani, D.; Kang, G.; Falade, A.G.; Odone, A.; Busse, R.; Martin-Moreno, J.M.; et al. The COVID-19 vaccines rush: Participatory community engagement matters more than ever. Lancet 2021, 397, 8–10. [Google Scholar] [CrossRef]
- Schoch-Spana, M.; Brunson, E.K.; Long, R.; Ruth, A.; Ravi, S.J.; Trotochaud, M.; Borio, L.; Brewer, J.; Buccina, J.; Connell, N.; et al. The public’s role in COVID-19 vaccination: Human-centered recommendations to enhance pandemic vaccine awareness, access, and acceptance in the United States. Vaccine 2021, 39, 6004–6012. [Google Scholar] [CrossRef]
- Demuyakor, J.; Nyatuame, I.N.; Obiri, S. Unmasking COVID-19 Vaccine Infodemic in the Social Media. Online J. Commun. Media Technol. 2021, 11, e202119. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Continent | Year | Authors | Number of Participants | Type of Participant Population | Country | COVID-19 Vaccine-Acceptance Rate (%) | Associated Factors |
|---|---|---|---|---|---|---|---|
| Asia, Africa, Europe, North America, South America | 2021 | Lazarus et al. [34] | 13,426 | General Population | Brazil, Canada, China, Ecuador, France, Germany, Italy, India, Mexico, Nigeria, Poland, Russia, Singapore, South Africa, South Korea, Spain, Sweden, United Kingdom and United States | 85.36%, 68.74%, 88.62%, 71.93%, 58.89%, 68.42%, 70.79%, 74.53%, 76.25%, 65.22%, 56.31%, 54.85%, 67.94%, 81.58%, 79.79%, 74.33%, 65.23%, 71.48%, 75.42%, respectively. | AF: Trust in government institutions and employers’ advice played major roles in enhancing vaccine-acceptance levels. HF: Men were less likely to accept a vaccine and individuals with lower income demonstrated vaccine hesitancy. |
| Asia, Africa, South America | 2021 | Bono et al. [35] | 10,183 | General population | Brazil, Malaysia, Thailand, Bangladesh, Democratic Republic of Congo, Benin, Uganda, Malawi and Mali | 94.2%, 78.6%, 87.3%, 89.6%, 59.4%, 48.4%%, 88.8%, 61.7%, 74.5%, respectively. | AF: Social, medical and behavioral factors including knowledge relating to COVID-19, income, age, gender and chronic diseases were linked to vaccine-acceptance rates. HF: Perceived vaccine threats were linked to vaccine hesitancy. |
| Asia | 2021 | Wang et al. [39] | 7381 | Adults (Above 18 years) | China | 75.3% | AF: Adults who had previously received the influenza vaccine, individuals who were older, were nonmedical personnel and had high educational levels demonstrated high vaccine acceptance. HF: Vaccine hesitancy due to the fear of side effects. |
| 2021 | Xu et al. [40] | 1051 | Adults (Healthcare workers) | China | 86.2% | AF: Accepted the vaccine after studying scientific literature and being encouraged by family members, friends, colleagues, experts and news media. HF: Request by employers and concern for vaccine safety was associated with vaccine hesitance. | |
| 2021 | Liu et al. [41] | 2377 | Adults | China | 82.25% | AF: Older age, medical insurance and vaccine safety for both paid and free vaccines. Factors relating high income, perceived benefits of vaccine were responsible for vaccine acceptance. HF: Young age, low educational levels and concerns about vaccine safety and side effects led towards vaccine hesitancy. | |
| 2021 | Gan et al. [42] | 1009 | Adults (General Population) | China | 60.40% | AF: Middle aged people with higher education, those with a past influenza vaccination history and perceived effectiveness of the COVID-19 vaccine resulted in vaccine acceptance. HF: Lower education levels, different occupations and lack of influenza vaccination resulted in vaccine hesitancy. | |
| 2021 | Walker et al. [43] | 330 | College Students | China | 36.4% | AF: Perceived vaccine benefits resulted in vaccine acceptance. HF: Vaccine hesitancy among international college students was due to perception of barriers, lack of knowledge, place of residence and program of study. | |
| 2021 | Sun et al. [44] | 505 | Healthcare Workers | China | 76.63% | AF: Understanding the benefits of the vaccine, perceived risks of COVID-19, living with elderly individuals and history of influenza vaccination resulted in vaccine acceptance. HF: Major contributors to vaccine hesitancy were perceptions about vaccine safety, effectiveness and concerns relating to rapid mutation of the virus. | |
| 2021 | Tao et al. [45] | 1392 | Pregnant Women | China | 77.4% | AF: High level of perceived susceptibility of COVID-19, significant vaccine information, high level of perceived vaccine benefits, living in western region and young age resulted in vaccine acceptance. HF: Low level of education, older age, and perceived risks of vaccine side effects led to vaccine hesitancy. | |
| 2021 | Chen et al. [46] | 3195 | Adults | China | 83.8% | AF: Belief that the vaccine would be beneficial to health and enhanced trust in government institutions and health experts resulted in vaccine acceptance. HF: Lack of confidence, risks associated with vaccine and awareness frequency was the main contributors affecting the intention of receiving the COVID-19 vaccine. | |
| 2021 | Han et al. [47] | 2126 | Migrant population | Shanghai, China | 89.1% | AF: Higher acceptance rates were demonstrated by younger individuals, families with three to four members, and those with higher education and income. HF: Vaccine hesitancy contributors included lack of information and confidence and willingness to pay for the vaccine. | |
| 2021 | Fayed et al. [48] | 980 | Adults (General Population) | Saudi Arabia | 59.5% | AF: Demographic characteristics and the willingness to be vaccinated against the seasonal influenza. HF: Lack of trust in government institutions and perceived risks about vaccine side effects and safety. | |
| 2021 | Qattan et al. [49] | 673 | Healthcare Workers | Saudi Arabia | 50.52% | AF: Being a male healthcare worker, perceiving an elevated risk of infection and adhering to the compulsory vaccination requirement were contributors for high vaccine-acceptance rates. HF: Young age, female gender, and HCWs residing in the south showed vaccine hesitancy. | |
| 2021 | Alfageeh et al. [50] | 2137 | Adults | Saudi Arabia | 48% | AF: Individuals residing in the southern region, past influenza vaccination, perceived risks of contracting the coronavirus and belief in mandatory vaccination were responsible for vaccine acceptance. HF: Social and behavioral factors pertaining to vaccine safety, history of vaccine refusal, attitudes towards seasonal influenza vaccination made up for the vaccine hesitancy. | |
| 2021 | Alshahrani et al. [51] | Not reported | General population | Saudi Arabia | 64% | AF: Factors associated with vaccine acceptance included vaccine information and awareness, perceptions towards vaccine effectiveness and previous uptake of influenza vaccine. HF: Misinformation relating to the side effects of the vaccine increased vaccine hesitancy. | |
| 2021 | AlAwadhi et al. [52] | 7241 | Adults | Kuwait | 67% | AF: Increased agreement with containment policies, high confidence in medical professionals and high awareness regarding the benefits of the vaccine increased acceptance rates. HF: Behavioral and social factors such as having low confidence in doctors, perceived fear and worries were evaluated to the reasons behind vaccine hesitancy. | |
| 2021 | Alqudeimat Y et al. [53] | 2368 | Adults (above 21 years) | Kuwait | 53.1% | AF: Past influenza vaccination history, male gender, and increased perceptions about the benefits of the vaccine improved acceptance rates. HF: Safety concerns regarding the vaccine and lack of influenza vaccine history increased vaccine hesitancy chances. | |
| 2021 | Al-Sanafi et al. [54] | 1019 | Adults (Healthcare workers) | Kuwait | 83.3% | AF: High levels of trust and confidence in government institutions and health systems resulted in high vaccine-acceptance rates. HF: Vaccine hesitancy was linked to social and behavioral factors such as conspiracy theories, gender and lower educational levels. | |
| 2021 | Sallam et al. [55] | 771; 2173 | Adults (General Population) | Kuwait, Jordan | 23.6%; 28.4% | HF: Vaccine conspiracy beliefs such as injection of microchips and vaccine administration leading to infertility. Vaccine hesitancy related to exposure to social-media platforms displaying negative information. | |
| 2021 | Qerem and Jarab [56] | 1144 | Adults (General Population) | Jordan | 36.8% | HF: High refusal and hesitancy were due to concern regarding use of vaccines and lack of trust. | |
| 2021 | El-Elimat et al. [57] | 3100 | Adults (General population) | Jordan | 62.6% | AF: Males and who took the influenza vaccine before demonstrated vaccine acceptance. Moreover, willingness to pay, and perceived benefits of the vaccine helped in increasing the acceptance rates. HF: Social and behavioral factors including female gender, lack of influenza vaccine history, less knowledge regarding vaccine safety and conspiracy theories behind the COVID-19 virus. | |
| 2021 | Yan et al. [58] | 1255 | Adults (General population) | Hong Kong | 42% | AF: Vaccine acceptance associated with male gender, witnessing of previous pandemics, and government influence. HF: Individuals who were female, older aged and with lower educational levels were more likely to show hesitancy towards the vaccine. | |
| 2021 | Luk et al. [59] | 1501 | Adults | Hong Kong | 45.3% | AF: Older people and individuals with chronic diseases demonstrated vaccine acceptance. HF: The most prevalent vaccine hesitancy factors included vaccine safety concerns, younger adults, those with chronic diseases and smokers. Furthermore, social factors comprised of inadequate knowledge and decelerated perceived risk of danger of not getting vaccinated. | |
| 2021 | Kwok et al. [60] | 1205 | Adults (Nurses) | Hong Kong | 63.00% | AF: Younger age, more confidence in HCWs and past influenza vaccination history resulted in vaccine acceptance. HF: Lack of influenza vaccination, older individuals and less educational levels were responsible for vaccine hesitancy. | |
| 2021 | Machida et al. [61] | 2956 | General Population | Japan | 62.1% | AF: Men who were aged 65 and above demonstrated vaccine acceptance. Individuals, who were married, were suffering from chronic diseases and had high educational levels exhibited high vaccine acceptance. HF: Psychological factors such as perceived side effects of vaccine and social factors including lower income groups, and adults aged 20–49 were hesitant to receive the COVID-19 vaccine. | |
| 2021 | Yoda and Katsuyama [62] | 1100 | Adults (General Population) | Japan | 65.7% | AF: Willingness to be vaccinated was associated with social factors such as older age groups, rural residences and individuals with underlying medical conditions. HF: Vaccine hesitancy was related to male gender. | |
| 2021 | Chaudhary et al. [63] | 423 | General population | Pakistan | 53% | AF: Healthy individuals with high income and educational backgrounds were more willing to get vaccinated. HF: Social and behavioral factors including lack of knowledge, perceptions of vaccine risks and perception of vaccine safety encapsulated the factors for low vaccine-acceptance rates. | |
| 2021 | Arshad et al. [64] | 2158 | Adults (General Population) | Pakistan | 41.2% | AF: Willingness to pay for the vaccine developed by Sino Pharm resulted in vaccine acceptance. HF: Conspiracy beliefs strongly associated with vaccine rejection. | |
| 2021 | Mulla et al. [65] | 462 | Adults | Qatar | 62.6% | AF: Social and behavioral factors including gender, having a postgraduate degree, government ruling on making vaccinations mandatory for travel and safety concerns. HF: Concerns regarding the rushed pace of development of a vaccine and its side effects, and the emergence of new variants of the coronavirus were responsible for vaccine hesitancy. | |
| 2021 | Abedin et al. [66] | 3646 | Adults | Bangladesh | 74.6% | AF: Trust in health safety regulations and high confidence in country’s health system resulted in vaccine acceptance. HF: Vaccine hesitancy resulted in social factors such as low educational levels, health and clinical related factors including chronic diseases. | |
| 2021 | Al Halabi et al. [67] | 579 | Adults | Lebanon | 21.4% | HF: Mainly females, married participants and those who had a general vaccine hesitancy comprised of the high percentage of people exhibiting low willingness to receive the vaccine. | |
| 2021 | Al-Metwali et al. [68] | 1680 | Healthcare workers, general population and health college students | Iraq | 61.7% | AF: HCWs and individuals who had received the influenza vaccination in the past were more willing to get vaccinated. HF: Concerns with storage, perceived benefits, perceived barriers and less awareness about vaccination formed the basis for the factors leading to vaccine hesitancy. | |
| 2021 | Mohamad et al. [69] | 3402 | Adults | Syria | 35.92% | HF: Factors including gender, age, not having children, rural residence, smoking and perceived risks of vaccine side effects and low educational levels were responsible for the poor vaccine-acceptance rate. | |
| 2021 | Rabi et al. [70] | 639 | Nurses | Palestine | 41% | HF: Lack of knowledge pertaining to the vaccine, age, perceived risk of side effects and preference to natural immunity comprised of social and behavioral factors responsible for low vaccine-acceptance rate. | |
| 2021 | Zigron et al. [71] | 506 | Adults (Dentists and dental residents) | Israel | 85% | AF: Increase in unemployment rate led towards enhanced vaccine acceptance. HF: Decreased unemployment rate resulted in less willingness to inoculate with the vaccine. | |
| 2020 | Lin et al. [72] | 3541 | Adults (General Population) | China | 83.50% | AF: The willingness to pay for the vaccine was influenced by socio-economic factors, such as preference of domestic made vaccine over foreign produced. HF: Lack of health belief models with effective health promotion strategies resulted in vaccine hesitancy. | |
| 2020 | Wang et al. [73] | 2058 | Adults | China | 91.30% | AF: Being male, married, perceiving a high risk of infection, valuing a doctor’s recommendation, believing in the efficacy of the vaccine or being vaccinated for influenza in the past season. HF: Female gender, lack of influenza vaccination in the past, less perceived risks of COVID-19 and being married resulted in vaccine hesitancy. | |
| 2020 | Zhang et al. [74] | 1052 | Children below 18 years of age | China | 72.60% | AF: Support from a family member, perceived behavioral control related to positive attitude from parents towards vaccinating their children. HF: Higher exposure to negative content regarding the vaccine was associated with parental rejection of the vaccine for their children. | |
| 2020 | Wang et al. [75] | 806 | Adult nurses | Hong Kong | 40% | HF: Lack of trust in government institutions and less intention to accept influenza vaccination in the past resulted in COVID-19 vaccine hesitancy. | |
| 2020 | Harapan et al. [76] | 1359 | Adults | Indonesia | 93.30% | AF: Exposure to COVID-19 information, being a HCW and increased perceived risk of infection resulted in COVID-19 vaccine acceptance. HF: Lower perceived risks about COVID-19 among retired/older individuals and lack of knowledge about the benefits of the vaccine resulted in vaccine hesitancy. | |
| 2020 | Al Mohaitheif and Badhi [77] | 992 | N/A | Saudi Arabia | 64.70% | AF: Older individuals, individuals who are married, having high educational levels, and employed in government sector resulted in vaccine acceptance. HF: Lack of confidence and perceived risks of vaccine side effects demonstrated vaccine hesitancy. | |
| 2020 | Dror et al. [78] | 388 | Doctors, general population, nurses | Israel | 78.1%, 75%, 61.1% | AF: Having a child, acceptance of recent most influenza vaccine, or being in the healthcare profession increased vaccine acceptance. HF: Not caring about the harmful effects of COVID-19 resulted in vaccine hesitancy. | |
| 2020 | Wong et al. [79] | 1159 | Adults (General Population) | Malaysia | 94.30% | AF: The willingness to pay for the vaccine was influenced by no affordability barriers as well as by socio-economic factors, such as higher education levels, professional and managerial occupations and higher incomes. | |
| Europe | 2021 | Fedele et al. [80] | Not reported | Population of parents | Italy | 27% | HF: Safety concerns in 76% parents. Females, lower education level and younger age were associated with non-adherence to vaccination. |
| 2021 | Di Gennaro et al. [81] | 1723 | Healthcare workers | Italy | 67% | AF: Perceived benefits about the health belief models and health promotion strategies resulted in vaccine acceptance. HF: Lack of trust in vaccine safety, inadequate information regarding vaccine and misinformation on social media encapsulated as the main social and behavioral contributors for vaccine hesitancy. | |
| 2021 | Riccio et al. [82] | 7605 | Adults (General Population | Italy | 81.9% | AF: COVID-19 vaccine acceptance was associated with female gender, trust in institutions and personal beliefs about the benefits of getting vaccination. HF: Unemployed individuals and those with a lack of influenza vaccination history demonstrated vaccine hesitancy. | |
| 2021 | Aurilio et al. [83] | 531 | Adults (Nurses) | Italy | 91.5% | AF: Female sex and confidence in vaccine efficacy were related to vaccine acceptance. HF: Poor understanding about the need to vaccinate, lack of confidence in vaccines and low educational levels resulted in vaccine hesitancy. | |
| 2021 | Guaraldi et al. [84] | 1176 | Adults (Type 2 Diabetes Mellitus patients) | Italy | 85.8% | AF: Social and behavioral factors such as older age, male gender, high educational development and influenza vaccination history were evaluated to be associated with vaccine acceptance. HF: Having experienced adverse effects from past vaccinations resulted in vaccine hesitancy. | |
| 2021 | Guiseppe et al. [85] | 481 | Adults | Italy | 84.1% | AF: Perceived risks of getting COVID-19 were prevalent in females, younger individuals and those who believed that COVID-19 is a severe disease. HF: Being male, being unmarried and less perceived benefits of getting vaccinated resulted in vaccine hesitancy. | |
| 2021 | Ikiisik et al. [86] | 384 | General Population | Turkey | 51.6% | AF: Perceived benefits of getting vaccinated and high trust in HCWs demonstrated vaccine acceptance. HF: Perception of vaccine risks and younger age were observed to be the main contributors for vaccine hesitancy. | |
| 2021 | Yigit et al. [87] | 343 | Healthcare Workers | Turkey | 50% | AF: Men demonstrated high vaccine acceptance. Individuals who were employed and older people exhibited vaccine acceptance. HF: The younger the age, the higher the vaccine hesitancy was reported. | |
| 2021 | Yurttas et al. [88] | 732 patients with rheumatic diseases, 763 general public and 320 healthcare providers | Patients with rheumatic diseases, general population and healthcare providers. | Turkey | 29.2% (patients with rheumatic diseases), 34.6% (general population), 52.5% (healthcare providers) | HF: Unknown scientific results, perceived vaccine side effects and lack of trust in government institutions were major factors for the low vaccine-acceptance rates. | |
| 2021 | Williams et al. [89] | 3436 (1st survey); 2016 (2nd survey) | Adults (General Population) | Scotland | 74%, (1st survey); 78% (2nd survey) | AF: Participants of white ethnicity, and individuals with high income levels and high education levels resulted in vaccine acceptance. HF: Black. Asian and minority ethnic groups with lower income and educational levels demonstrated vaccine hesitancy. | |
| 2021 | Fakonti et al. [90] | 437 | Nurses and Midwives | Cyprus | 30% | HF: Fear of side effects, female gender, younger age, lack of history of influenza vaccination and working in private sector resulted in vaccine hesitancy. | |
| 2021 | Papagiannis et al. [91] | 340 | Health Professionals | Greece | 78.5% | AF: Less fear of vaccine side effects and adequate information received from Greek public health authorities effected vaccine-acceptance rate. High vaccination coverage and absence of fear over vaccine safety were also responsible for high vaccine acceptance. | |
| 2021 | Schwarzinger et al. [92] | 1942 | Adults (working population) | France | 71.2% | HF: Vaccine refusal was associated with low educational level, chronic diseases, female gender, age and lower perceived severity of COVID-19. | |
| 2021 | Gagneux-Brunon et al. [93] | 2047 | Adults (Healthcare workers) | France | 76.90% | AF: Older age, male gender, and perceived fear about COVID-19 increased vaccine-acceptance rates. HF: Hesitancy to the vaccine relating with female gender, being a nurse or suffering from a chronic medical condition. | |
| 2021 | Sherman et al. [94] | 1500 | Adults (General Population) | UK | 64.00% | AF: Positive beliefs and attitudes for the COVID-19 vaccine were associated with vaccine acceptance. HF: General lack of knowledge in the vaccine and belief in side effects was related to vaccine hesitancy. | |
| 2020 | Neumann-Bohme et al. [95] | 1000 | Adults | Denmark, UK, Portugal, Netherland, Germany, France, Italy | 80%, 79%, 75%, 73%, 70%, 62%, 77.30% | AF: Men above 55 years with high perceived risks about getting COVID-19 and benefits of vaccination resulted in vaccine acceptance. HF: Vaccine hesitancy dependent on female gender, younger age, and a lack of trust in a vaccine prepared very quickly. | |
| 2020 | Freeman et al. [96] | 5114 | Adults (General population) | UK | 71.70% | AF: Age, gender, ethnicity income and region matched with vaccine acceptance. HF: Vaccine hesitancy associated with negative beliefs including mistrust, conspiracy theories and negative support of doctors. | |
| 2020 | Bell et al. [97] | 1252 | Adults (General Population) | UK | 89.10% | AF: Protection of own self and family members, high trust in vaccines, scientific literature and HCWs, to stay safe to look after children and the need for stopping social distancing resulted in vaccine acceptance. HF: Race, ethnicity and low-income households most prominently related to vaccine hesitancy. Also relating to vaccine rejection was mistrust in a rapidly developed vaccine. | |
| 2020 | Salali and Uysal [98] | 1088; 3936 | Adults | UK, Turkey | 83%; 77% | AF: Willingness of participants to get vaccinated against the virus and high levels of education helped enhance vaccine acceptance. HF: Less public health campaigns demonstrated vaccine hesitancy. | |
| 2020 | Detoc et al. [99] | 3259 | Adults | France | 77.60% | AF: Older age, male gender, perceived risks about getting infected with the coronavirus and being a HCW increased vaccine acceptance. HF: Younger age, female gender, anxiety and misconceptions about COVID-19 and associated risk factors with the vaccine resulted in vaccine hesitancy. | |
| 2020 | Ward et al. [100] | 5018 | Adults (General Population) | France | 76% | AF: Older individuals, men and individuals with high educational levels accepted the vaccine. HF: Believing that a vaccine produced quickly would be unsafe resulted in vaccine hesitancy. | |
| 2020 | La Vecchia et al. [101] | 1055 | Aged 15–85 years (General Population) | Italy | 53.70% | AF: Older age, occupation and willingness to be vaccinated against influenza were related to the intention to be vaccinated against COVID-19. HF: Vaccine mistrust, less qualified individuals and those with lower educational levels demonstrated vaccine hesitancy. | |
| 2020 | Barello et al. [102] | 735 | Adults (University Students) | Italy | 86.10% | AF: High levels of trust in health promotion strategies and government institutions increased vaccine acceptance. Students having high levels of education demonstrated high vaccine acceptance. HF: Fears of vaccine safety and side effects resulted in vaccine hesitancy. | |
| North America | 2021 | Waters et al. [103] | 342 | Adolescents and young adults (15–39 years) | United States | 63% | AF: Male gender and those having high educational backgrounds resulted in vaccine acceptance. HF: Female gender and individuals with a high school education or less, reported high vaccine hesitancy. |
| 2021 | Mascarenhas et al. [104] | 248 | Dental students | United States | 56% | HF: Lack of trust in public health experts, perceived risks of vaccine side effects were major contributors affecting the vaccine-acceptance rate. | |
| 2021 | Viswanath et al. [105] | 1012 | Adults | United States | 65% | HF: Vaccine hesitancy was based on risks associated with the COVID-19 vaccine, exposure to social-media platforms and ethnicity along with less education levels. | |
| 2020 | Pogue et al. [106] | 316 | General Population | United States | 68% | HF: Efficacy, length of testing and perceived vaccine side effects lead towards vaccine hesitancy. | |
| 2020 | Fisher et al. [107] | 1003 | Adults | United States | 56.90% | HF: Younger age, black race, low education attainment and lack of information resulted in vaccine hesitancy. | |
| 2020 | Malik et al. [108] | 672 | Adults (General Population) | United States | 67.00% | AF: Males, older adults, Asians, individuals with high educational levels were more willing to accept the vaccine. HF: Females, young adults, racial ethnic groups and those having less education demonstrated vaccine hesitancy. | |
| 2020 | Reiter et al. [109] | 2006 | Adults (General Population) | United States | 68.50% | AF: Willingness to be vaccinated was related to healthcare provider’s advice, political understanding, and knowledge about vaccine harms. | |
| 2020 | Taylor et al. [110] | 1902; 1772 | Adults (General Population) | Canada, United States | 80.0%; 75.0% | HF: Vaccine rejection was strongly influenced by mistrust of vaccine benefits and by worries about unforeseen future effects, concerns about commercial profiteering from pharmaceutical companies, and preferences for natural immunity. | |
| Australia | 2021 | Seale et al. [111] | 1420 | Adults (18 years and above) | Australia | 80% | AF: Females, individuals aged 70 years and above, individuals with private health insurance and those suffering from chronic diseases demonstrated vaccine acceptance. Family support greatly increased vaccine acceptance. HF: Males and individuals having age between 18 to 29 years demonstrated vaccine hesitancy. |
| 2021 | Rhodes et al. [112] | 2018 | Adults (Parents and Guardians) | Australia | 75.80% | AF: Women, men and generally people with higher socioeconomic status were related for vaccine acceptance. HF: Vaccine hesitancy was associated with a younger age, educational level and knowledge about the COVID-19 vaccine. | |
| Africa | 2021 | Adeniyi et al. [113] | 1308 | Adults (healthcare workers) | South Africa | 90.1% | AF: Social factors including high levels of education were associated with vaccine-acceptance rates. |
| 2021 | Saeid et al. [114] | 2133 | Medical Students | Egypt | 90.5% | AF: Female students, students in medicine and physiotherapy and students who had high income and socioeconomic status demonstrated high vaccine acceptance. HF: Inadequate information relating to vaccine effects and insufficient information of the vaccine itself led to vaccine hesitancy. | |
| 2020 | Nzaji et al. [115] | 613 | Adults (healthcare workers) | Democratic Republic of Congo | 27.70% | AF: Male HCWs, particularly doctors and having a positive attitude towards COVID-19 vaccine resulted in vaccine acceptance. HF: Misinformation about vaccine safety and side effects on social networks were responsible for vaccine hesitancy. | |
| South America | 2021 | Cerda and Gracia [116] | 370 | General population | Chile | 49% | HF: Perceived side effects including immunity and less awareness by the government authorities about vaccine benefits were evaluated as reasons for vaccine hesitancy. |
| 2020 | Sarasty et al. [117] | 1050 | Adults (General Population) | Ecuador | 97% | AF: Willingness to pay was associated with income, employment status and the probability of hospital charges if the virus was contracted. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shakeel, C.S.; Mujeeb, A.A.; Mirza, M.S.; Chaudhry, B.; Khan, S.J. Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines 2022, 10, 110. https://doi.org/10.3390/vaccines10010110
Shakeel CS, Mujeeb AA, Mirza MS, Chaudhry B, Khan SJ. Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines. 2022; 10(1):110. https://doi.org/10.3390/vaccines10010110
Chicago/Turabian StyleShakeel, Choudhary Sobhan, Amenah Abdul Mujeeb, Muhammad Shaheer Mirza, Beenish Chaudhry, and Saad Jawaid Khan. 2022. "Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors" Vaccines 10, no. 1: 110. https://doi.org/10.3390/vaccines10010110
APA StyleShakeel, C. S., Mujeeb, A. A., Mirza, M. S., Chaudhry, B., & Khan, S. J. (2022). Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines, 10(1), 110. https://doi.org/10.3390/vaccines10010110