
Exploratory Role of Flavonoids on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in a South Italian Cohort

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
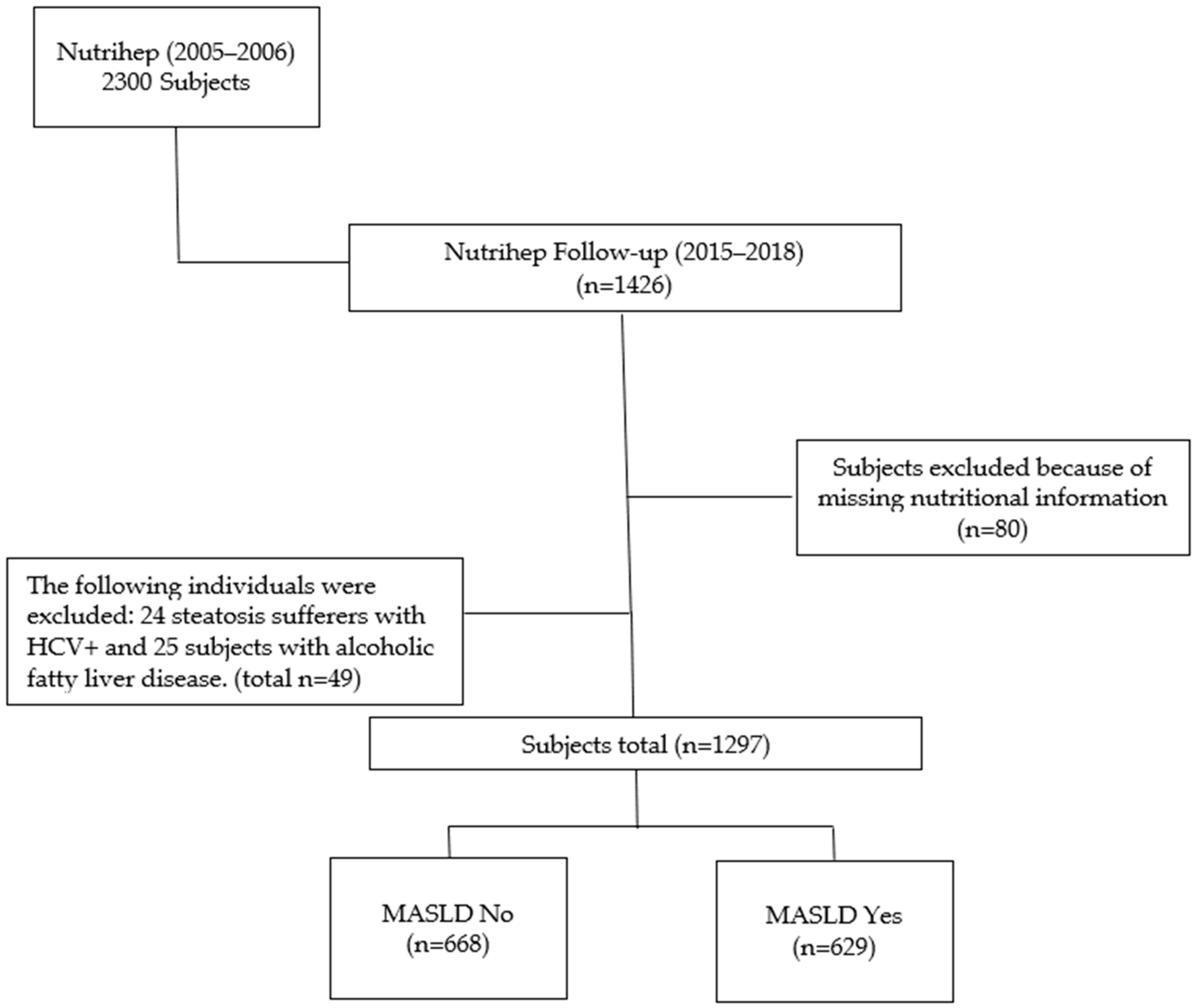
2.1. Study Population
2.2. Outcome Assessment
2.3. Assessment of Flavonoid Intake
2.4. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, W.-K.; Chuah, K.-H.; Rajaram, R.B.; Lim, L.-L.; Ratnasingam, J.; Vethakkan, S.R. Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A State-of-the-Art Review. J. Obes. Metab. Syndr. 2023, 32, 197–213. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, J.; Viggiano, T.; McGill, D.; Oh, B. Nonalcoholic Steatohepatitis: Mayo Clinic Experiences with a Hitherto Unnamed Disease. Mayo Clin. Proc. 1980, 55, 434–438. [Google Scholar] [PubMed]
- Farrell, G.C.; Chitturi, S.; Lau, G.K.; Sollano, J.D.; Asia–Pacific Working Party on NAFLD. Guidelines for the Assessment and Management of Non-alcoholic Fatty Liver Disease in the Asia–Pacific Region: Executive Summary. J. Gastro. Hepatol. 2007, 22, 775–777. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Bellentani, S.; Cortez-Pinto, H.; Day, C.; Marchesini, G. A Position Statement on NAFLD/NASH Based on the EASL 2009 Special Conference. J. Hepatol. 2010, 53, 372–384. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multisociety Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. Hepatology 2023, 78, 1966–1986. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.-S.; Rinella, M. Non-Alcoholic Fatty Liver Disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A New Definition for Metabolic Dysfunction-Associated Fatty Liver Disease: An International Expert Consensus Statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Singh, S.; Allen, A.M.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Loomba, R. Fibrosis Progression in Nonalcoholic Fatty Liver vs Nonalcoholic Steatohepatitis: A Systematic Review and Meta-Analysis of Paired-Biopsy Studies. Clin. Gastroenterol. Hepatol. 2015, 13, 643–654.e9. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased Risk of Mortality by Fibrosis Stage in Nonalcoholic Fatty Liver Disease: Systematic Review and Meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef]
- Le, M.H.; Yeo, Y.H.; Li, X.; Li, J.; Zou, B.; Wu, Y.; Ye, Q.; Huang, D.Q.; Zhao, C.; Zhang, J.; et al. 2019 Global NAFLD Prevalence: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 2809–2817.e28. [Google Scholar] [CrossRef]
- Huh, Y.; Cho, Y.J.; Nam, G.E. Recent Epidemiology and Risk Factors of Nonalcoholic Fatty Liver Disease. J. Obes. Metab. Syndr. 2022, 31, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Farrell, G.C.; Wong, V.W.-S.; Chitturi, S. NAFLD in Asia—As Common and Important as in the West. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.-S.; Chan, R.S.-M.; Wong, G.L.-H.; Cheung, B.H.-K.; Chu, W.C.-W.; Yeung, D.K.-W.; Chim, A.M.-L.; Lai, J.W.-Y.; Li, L.S.; Sea, M.M.-M.; et al. Community-Based Lifestyle Modification Programme for Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. J. Hepatol. 2013, 59, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Lassailly, G.; Caiazzo, R.; Buob, D.; Pigeyre, M.; Verkindt, H.; Labreuche, J.; Raverdy, V.; Leteurtre, E.; Dharancy, S.; Louvet, A.; et al. Bariatric Surgery Reduces Features of Nonalcoholic Steatohepatitis in Morbidly Obese Patients. Gastroenterology 2015, 149, 379–388. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean Diet and Health Status: Active Ingredients and Pharmacological Mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Corradini, E.; Foglia, P.; Giansanti, P.; Gubbiotti, R.; Samperi, R.; Laganà, A. Flavonoids: Chemical Properties and Analytical Methodologies of Identification and Quantitation in Foods and Plants. Nat. Prod. Res. 2011, 25, 469–495. [Google Scholar] [CrossRef]
- Crozier, A.; Jaganath, I.B.; Clifford, M.N. Dietary Phenolics: Chemistry, Bioavailability and Effects on Health. Nat. Prod. Rep. 2009, 26, 1001. [Google Scholar] [CrossRef]
- AboZaid, O.; AbdEl-hamid, O.; Atwa, S. Biochemical Alterations of Resveratrol on Oxidative Stress in Experimental Induced Non—Alcoholic Fatty Liver Disease in Rats. Benha Vet. Med. J. 2015, 28, 166–177. [Google Scholar] [CrossRef]
- Schmatz, R.; Perreira, L.B.; Stefanello, N.; Mazzanti, C.; Spanevello, R.; Gutierres, J.; Bagatini, M.; Martins, C.C.; Abdalla, F.H.; Daci Da Silva Serres, J.; et al. Effects of Resveratrol on Biomarkers of Oxidative Stress and on the Activity of Delta Aminolevulinic Acid Dehydratase in Liver and Kidney of Streptozotocin-Induced Diabetic Rats. Biochimie 2012, 94, 374–383. [Google Scholar] [CrossRef]
- Ying, H.-Z.; Liu, Y.-H.; Yu, B.; Wang, Z.-Y.; Zang, J.-N.; Yu, C.-H. Dietary Quercetin Ameliorates Nonalcoholic Steatohepatitis Induced by a High-Fat Diet in Gerbils. Food Chem. Toxicol. 2013, 52, 53–60. [Google Scholar] [CrossRef]
- Cozzolongo, R.; Osella, A.R.; Elba, S.; Petruzzi, J.; Buongiorno, G.; Giannuzzi, V.; Leone, G.; Bonfiglio, C.; Lanzilotta, E.; Manghisi, O.G.; et al. Epidemiology of HCV Infection in the General Population: A Survey in a Southern Italian Town. Am. J. Gastroenterol. 2009, 104, 2740–2746. [Google Scholar] [CrossRef] [PubMed]
- United Nations Educational, Scientific and Cultural Organization. International Standard Classification of Education, ISCED 1997. In Advances in Cross-National Comparison: A European Working Book for Demographic and Socio-Economic Variables; Springer: Boston, MA, USA, 2003; Available online: https://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-1997-en_0.pdf (accessed on 20 October 2024).
- International Standard Classification of Occupations, International Labour Office. Available online: https://www.ilo.org/sites/default/files/wcmsp5/groups/public/@dgreports/@dcomm/@publ/documents/publication/wcms_172572.pdf (accessed on 20 October 2024).
- Sever, P. New Hypertension Guidelines from the National Institute for Health and Clinical Excellence and the British Hypertension Society. J. Renin Angiotensin Aldosterone Syst. 2006, 7, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Riboli, E. The EPIC Project: Rationale and Study Design. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26, S6–S14. [Google Scholar] [CrossRef] [PubMed]
- Riboli, E.; Hunt, K.; Slimani, N.; Ferrari, P.; Norat, T.; Fahey, M.; Charrondière, U.; Hémon, B.; Casagrande, C.; Vignat, J.; et al. European Prospective Investigation into Cancer and Nutrition (EPIC): Study Populations and Data Collection. Public Health Nutr. 2002, 5, 1113–1124. [Google Scholar] [CrossRef]
- Kalligeros, M.; Vassilopoulos, A.; Vassilopoulos, S.; Victor, D.W.; Mylonakis, E.; Noureddin, M. Prevalence of Steatotic Liver Disease (MASLD, MetALD, and ALD) in the United States: NHANES 2017–2020. Clin. Gastroenterol. Hepatol. 2024, 22, 1330–1332.e4. [Google Scholar] [CrossRef]
- Neveu, V.; Perez-Jimenez, J.; Vos, F.; Crespy, V.; Du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An Online Comprehensive Database on Polyphenol Contents in Foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef]
- Peterson, J.J.; Dwyer, J.T.; Jacques, P.F.; McCullough, M.L. Improving the Estimation of Flavonoid Intake for Study of Health Outcomes. Nutr. Rev. 2015, 73, 553–576. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Belsley, D.A.; Kuh, E.; Welsch, R.E. Regression Diagnostics: Identifying Influential Data and Sources of Collinearity; Wiley: New York, NY, USA, 1980. [Google Scholar]
- Ritz, C.; Jensen, S.M.; Gerhard, D.; Streibig, J.C. Dose-Response Analysis Using R, 1st ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2019; ISBN 978-1-315-27009-8. [Google Scholar]
- Desquilbet, L.; Mariotti, F. Dose-response Analyses Using Restricted Cubic Spline Functions in Public Health Research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Ruppert, D.; Wand, M.P.; Frontmatter, R.J.C. Semiparametric Regression. Cambridge Series in Statistical and Probabilistic Mathematics; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Harrell, F. Regression Modeling Strategies. R Package, Version 6.8-0; 2024. Available online: https://cran.r-project.org/web/packages/rms/rms.pdf (accessed on 20 October 2024).
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024. [Google Scholar]
- Faghihzadeh, F.; Adibi, P.; Rafiei, R.; Hekmatdoost, A. Resveratrol Supplementation Improves Inflammatory Biomarkers in Patients with Nonalcoholic Fatty Liver Disease. Nutr. Res. 2014, 34, 837–843. [Google Scholar] [CrossRef]
- Chen, S.; Zhao, X.; Ran, L.; Wan, J.; Wang, X.; Qin, Y.; Shu, F.; Gao, Y.; Yuan, L.; Zhang, Q.; et al. Resveratrol Improves Insulin Resistance, Glucose and Lipid Metabolism in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Dig. Liver Dis. 2015, 47, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Heebøll, S.; Kreuzfeldt, M.; Hamilton-Dutoit, S.; Kjær Poulsen, M.; Stødkilde-Jørgensen, H.; Møller, H.J.; Jessen, N.; Thorsen, K.; Kristina Hellberg, Y.; Bønløkke Pedersen, S.; et al. Placebo-Controlled, Randomised Clinical Trial: High-Dose Resveratrol Treatment for Non-Alcoholic Fatty Liver Disease. Scand. J. Gastroenterol. 2016, 51, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: An Overview. J. Nutr. Sci. 2016, 5, e47. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, H. Structure-Dependent Membrane Interaction of Flavonoids Associated with Their Bioactivity. Food Chem. 2010, 120, 1089–1096. [Google Scholar] [CrossRef]
- Maleki, S.J.; Crespo, J.F.; Cabanillas, B. Anti-Inflammatory Effects of Flavonoids. Food Chem. 2019, 299, 125124. [Google Scholar] [CrossRef]
- Kaigongi, M.M.; Lukhoba, C.W.; Ochieng‘, P.J.; Taylor, M.; Yenesew, A.; Makunga, N.P. LC-MS-Based Metabolomics for the Chemosystematics of Kenyan Dodonaea Viscosa Jacq (Sapindaceae) Populations. Molecules 2020, 25, 4130. [Google Scholar] [CrossRef]
- Mazidi, M.; Katsiki, N.; Banach, M. A Higher Flavonoid Intake Is Associated with Less Likelihood of Nonalcoholic Fatty Liver Disease: Results from a Multiethnic Study. J. Nutr. Biochem. 2019, 65, 66–71. [Google Scholar] [CrossRef]
- Van De Wier, B.; Koek, G.H.; Bast, A.; Haenen, G.R.M.M. The Potential of Flavonoids in the Treatment of Non-Alcoholic Fatty Liver Disease. Crit. Rev. Food Sci. Nutr. 2017, 57, 834–855. [Google Scholar] [CrossRef]
- Skibola, C.F.; Smith, M.T. Potential Health Impacts of Excessive Flavonoid Intake. Free Radic. Biol. Med. 2000, 29, 375–383. [Google Scholar] [CrossRef]
- Wang, S.; Sheng, F.; Zou, L.; Xiao, J.; Li, P. Hyperoside Attenuates Non-Alcoholic Fatty Liver Disease in Rats via Cholesterol Metabolism and Bile Acid Metabolism. J. Adv. Res. 2021, 34, 109–122. [Google Scholar] [CrossRef]
- Liu, B.; Zhang, J.; Sun, P.; Yi, R.; Han, X.; Zhao, X. Raw Bowl Tea (Tuocha) Polyphenol Prevention of Nonalcoholic Fatty Liver Disease by Regulating Intestinal Function in Mice. Biomolecules 2019, 9, 435. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, R.; Shen, Z.; Cai, G. Combination of Luteolin and Lycopene Effectively Protect against the “Two-Hit” in NAFLD through Sirt1/AMPK Signal Pathway. Life Sci. 2020, 256, 117990. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Gao, L.; Lin, H.; Wu, Y.; Han, X.; Zhu, Y.; Li, J. Luteolin Improves Non-Alcoholic Fatty Liver Disease in Db/Db Mice by Inhibition of Liver X Receptor Activation to down-Regulate Expression of Sterol Regulatory Element Binding Protein 1c. Biochem. Biophys. Res. Commun. 2017, 482, 720–726. [Google Scholar] [CrossRef]
- Yang, H.; Yang, T.; Heng, C.; Zhou, Y.; Jiang, Z.; Qian, X.; Du, L.; Mao, S.; Yin, X.; Lu, Q. Quercetin Improves Nonalcoholic Fatty Liver by Ameliorating Inflammation, Oxidative Stress, and Lipid Metabolism in Db/Db Mice. Phytother. Res. 2019, 33, 3140–3152. [Google Scholar] [CrossRef]
- Tan, P.; Jin, L.; Qin, X.; He, B. Natural Flavonoids: Potential Therapeutic Strategies for Non-Alcoholic Fatty Liver Disease. Front. Pharmacol. 2022, 13, 1005312. [Google Scholar] [CrossRef]
- Xiao, M.; Chen, G.; Zeng, F.; Qiu, R.; Shi, W.; Lin, J.; Cao, Y.; Li, H.; Ling, W.; Chen, Y. Higher Serum Carotenoids Associated with Improvement of Non-Alcoholic Fatty Liver Disease in Adults: A Prospective Study. Eur. J. Nutr. 2019, 58, 721–730. [Google Scholar] [CrossRef]
- Wang, M.; Qiao, X.; Fang, Q.; Fu, S.; Li, X.; Huang, F.; Lin, Y. Effect of Different Polar Extracts of Scutellaria baicalensis Total Flavonoids on Non-Alcoholic Fatty Liver Model Rats. Chin. Pharm. 2022, 33, 1338–1342. [Google Scholar]
- González-Gallego, J.; García-Mediavilla, M.V.; Sánchez-Campos, S.; Tuñón, M.J. Fruit Polyphenols, Immunity and Inflammation. Br. J. Nutr. 2010, 104, S15–S27. [Google Scholar] [CrossRef]
- Abu-Elsaad, N.; El-Karef, A. Protection against Nonalcoholic Steatohepatitis through Targeting IL-18 and IL-1alpha by Luteolin. Pharmacol. Rep. 2019, 71, 688–694. [Google Scholar] [CrossRef]
- Visioli, F.; Davalos, A. Polyphenols and Cardiovascular Disease: A Critical Summary of the Evidence. Mini Rev. Med. Chem. 2011, 11, 1186–1190. [Google Scholar] [CrossRef]
- Middleton, E., Jr.; Kandaswami, C.; Theoharides, T.C. The Effects of Plant Flavonoids on Mammalian Cells: Implications for Inflammation, Heart Disease, and Cancer. Pharmacol. Rev. 2000, 52, 673–751. [Google Scholar] [PubMed]
- Rietman, A.; Sluik, D.; Feskens, E.J.M.; Kok, F.J.; Mensink, M. Associations between Dietary Factors and Markers of NAFLD in a General Dutch Adult Population. Eur. J. Clin. Nutr. 2018, 72, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Papamiltiadous, E.S.; Roberts, S.K.; Nicoll, A.J.; Ryan, M.C.; Itsiopoulos, C.; Salim, A.; Tierney, A.C. A Randomised Controlled Trial of a Mediterranean Dietary Intervention for Adults with Non Alcoholic Fatty Liver Disease (MEDINA): Study Protocol. BMC Gastroenterol. 2016, 16, 14. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, A.; De Pergola, G. Mediterranean Diet Pyramid: A Proposal for Italian People. Nutrients 2014, 6, 4302–4316. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.S.; De Oliveira, V.S.; Chávez, D.W.H.; Chaves, D.S.; Riger, C.J.; Sawaya, A.C.H.F.; Guizellini, G.M.; Sampaio, G.R.; Torres, E.A.F.D.S.; Saldanha, T. Bioactive Compounds of Parsley (Petroselinum crispum), Chives (Allium schoenoprasum L.) and Their Mixture (Brazilian cheiro-verde) as Promising Antioxidant and Anti-Cholesterol Oxidation Agents in a Food System. Food Res. Int. 2022, 151, 110864. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Parameters a | MASLD | ||
|---|---|---|---|
| Whole Sample b | No | Yes | |
| N (%) | 1297 | 668 (51.50) | 629 (48.50) |
| Age (years) | 54.33 (14.34) | 49.24 (13.80) | 59.74 (12.86) |
| Age categories (years) (%) | |||
| <65 | 955 (73.6) | 565 (59.2) | 390 (40.8%) |
| ≥65 | 342 (26.4) | 103 (30.1) | 239 (69.9%) |
| Gender (%) | |||
| Female | 744 (57.4) | 417 (56.0) | 327 (44.0%) |
| Male | 553 (42.6) | 251 (45.4) | 302 (54.6%) |
| Flavonoids (mg/day) | 203.89 (126.36) | 192.30 (123.03) | 216.19 (128.75) |
| rMED (median (IQR)) | 8.00 (6.00; 10.00) | 8.00 (6.00; 10.00) | 8.00 (6.00; 10.00) |
| BMI (kg/m2) | 27.58 (5.05) | 25.04 (3.59) | 30.28 (4.97) |
| Weight (kg) | 72.93 (14.87) | 66.66 (12.02) | 79.58 (14.73) |
| Waist (cm) | 90.45 (13.46) | 83.04 (10.38) | 98.32 (11.79) |
| SBP (mmHg) | 120.93 (15.81) | 115.64 (15.35) | 126.52 (14.30) |
| DBP (mmHg) | 77.68 (8.00) | 75.69 (7.88) | 79.78 (7.58) |
| HbA1c (mmol/mol) | 38.07 (6.87) | 36.59 (5.05) | 39.64 (8.09) |
| HOMA | 1.89 (1.88) | 1.33 (0.90) | 2.43 (2.38) |
| ALT (U/L) | 22.20 (16.21) | 19.70 (8.27) | 24.86 (21.37) |
| γGT (U/L) | 17.58 (13.46) | 14.80 (7.67) | 20.54 (17.16) |
| AST (U/L) | 21.74 (10.87) | 20.70 (5.94) | 22.85 (14.29) |
| TG (mg/dL) | 98.41 (69.23) | 80.73 (58.55) | 117.22 (74.60) |
| C-reactive protein (mg/dL) | 0.26 (0.55) | 0.21 (0.52) | 0.31 (0.58) |
| TC (mg/dL) | 191.35 (35.36) | 188.90 (33.06) | 193.96 (37.50) |
| HDL (mg/dL) | 50.79 (12.59) | 53.18 (12.80) | 48.24 (11.85) |
| Glucose (mg/dL) | 95.34 (17.34) | 90.13 (10.54) | 100.89 (21.06) |
| ALP (U/L) | 52.98 (16.10) | 50.10 (15.56) | 56.04 (16.11) |
| Alcohol intake (g/day) | 10.58 (12.72) | 10.74 (13.41) | 10.42 (11.96) |
| Kcal (day) | 2056.26 (750.22) | 2100.33 (724.88) | 2009.46 (774.05) |
| Smoker (%) | |||
| Never/Former | 1137 (87.7) | 587 (51.6) | 550 (48.4) |
| Current | 159 (12.3) | 81 (50.9) | 78 (49.1) |
| Hypertension (%) | |||
| No | 847 (68.8) | 517 (61.0) | 330 (39.0) |
| Yes | 385 (31.2) | 115 (29.9) | 270 (70.1) |
| Dyslipidemia (%) | |||
| No | 1047 (85.1) | 561 (53.6) | 486 (46.4) |
| Yes | 184 (14.9) | 71 (38.6) | 113 (61.4) |
| Diabetes (%) | |||
| No | 1148 (93.2) | 620 (54.0) | 528 (46.0) |
| Yes | 84 (6.8) | 12 (14.3) | 72 (85.7) |
| Marital Status (%) | |||
| Single | 181 (14.0) | 115 (63.5) | 66 (36.5) |
| Married or living together | 1034 (79.7) | 519 (50.2) | 515 (49.8) |
| Separated or divorced | 28 (2.2) | 20 (71.4) | 8 (28.6) |
| Widow/er | 54 (4.2) | 14 (25.9) | 40 (74.1) |
| Education (%) | |||
| Primary school | 282 (21.8) | 71 (25.2) | 211 (74.8) |
| Secondary school | 383 (29.5) | 171 (44.6) | 212 (55.5) |
| High school | 460 (35.5) | 307 (66.7) | 153 (33.3) |
| Graduate | 172 (13.3) | 119 (69.2) | 53 (30.8) |
| Job (%) | |||
| Managers and professionals | 102 (7.9) | 57 (55.9) | 45 (44.1) |
| Craft, agricultural, and sales Workers | 469 (36.2) | 285 (60.8) | 184 (39.2) |
| Elementary occupations | 185 (14.1) | 93 (50.3) | 92 (49.7) |
| Housewife | 141 (10.9) | 74 (52.5) | 67 (47.5) |
| Pensioner | 325 (25.1) | 110 (33.8) | 215 (66.2) |
| Unemployed | 75 (5.8) | 49 (65.3) | 26 (34.7) |
| Family income assessment (%) | |||
| Insufficient | 27 (2.1) | 10 (37.0) | 17 (63.0) |
| Just sufficient | 167 (12.9) | 81 (48.5) | 86 (51.5) |
| Sufficient | 1019 (78.6) | 521 (51.1) | 498 (48.9) |
| More than sufficient | 64 (4.9) | 44 (68.8) | 20 (31.2) |
| Good | 20 (1.5) | 12 (60.0) | 8 (40.0) |
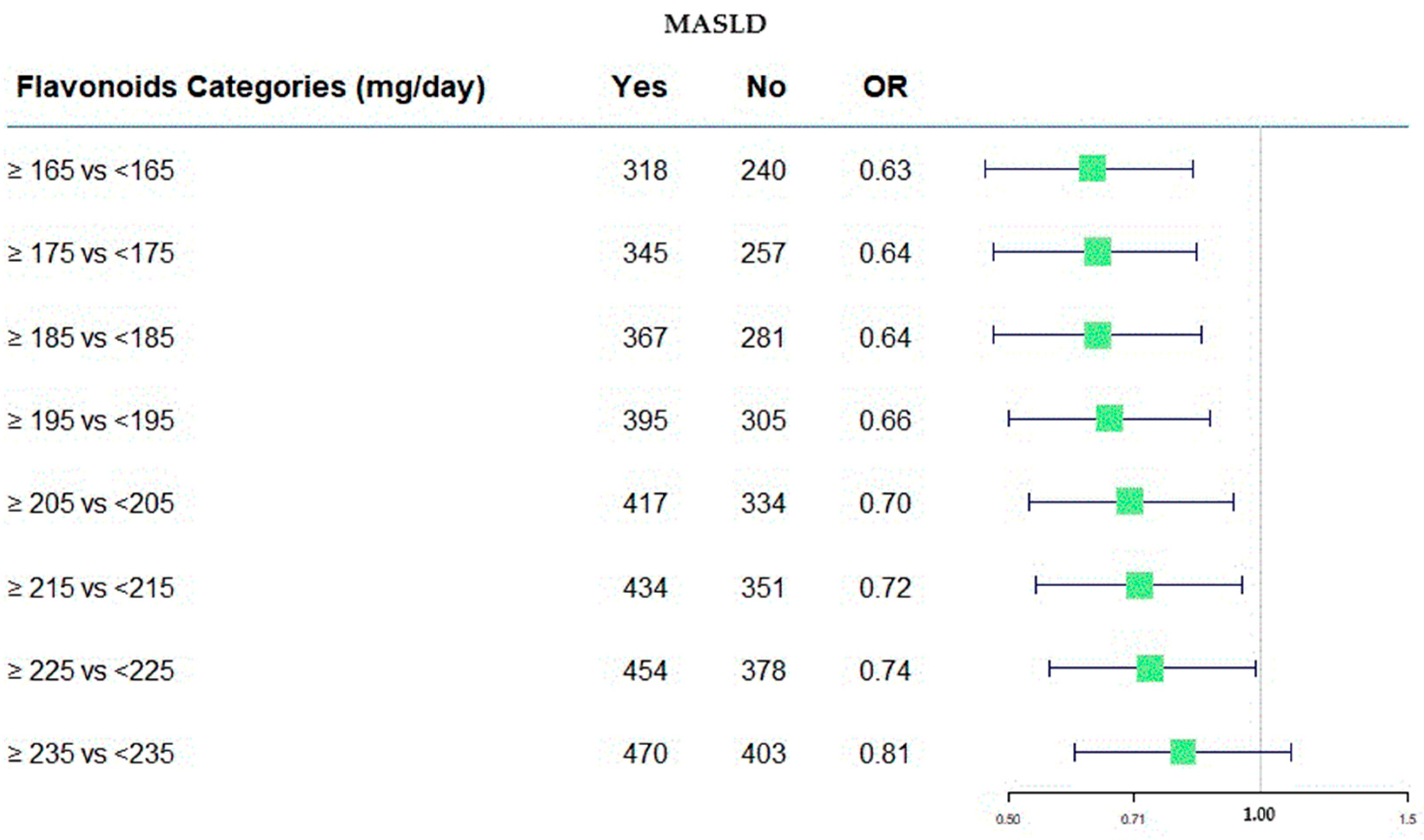
| Flavonoids (mg/day) | MASLD | |||
|---|---|---|---|---|
| OR | SE (OR) | p-Value | 95% C.I. | |
| Categories b: | ||||
| ≥165 vs. <165 | 0.63 | 0.09 | 0.001 | 0.47; 0.83 |
| ≥175 vs. ≤175 | 0.64 | 0.09 | 0.002 | 0.48; 0.84 |
| ≥185 vs. <185 a | 0.64 | 0.09 | 0.002 | 0.48; 0.85 |
| ≥195 vs. <195 | 0.66 | 0.09 | 0.004 | 0.50; 0.87 |
| ≥205 vs. <205 | 0.70 | 0.10 | 0.014 | 0.53; 0.93 |
| ≥215 vs. <215 | 0.72 | 0.10 | 0.023 | 0.54; 0.95 |
| ≥225 vs. <225 | 0.74 | 0.11 | 0.045 | 0.56; 0.99 |
| ≥235 vs. <235 | 0.81 | 0.12 | 0.170 | 0.60; 1.09 |
| continuous | 1.001 | 0.001 | 0.016 | 1.000; 1.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonfiglio, C.; Tatoli, R.; Donghia, R.; Guido, D.; Giannelli, G. Exploratory Role of Flavonoids on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in a South Italian Cohort. Antioxidants 2024, 13, 1286. https://doi.org/10.3390/antiox13111286
Bonfiglio C, Tatoli R, Donghia R, Guido D, Giannelli G. Exploratory Role of Flavonoids on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in a South Italian Cohort. Antioxidants. 2024; 13(11):1286. https://doi.org/10.3390/antiox13111286
Chicago/Turabian StyleBonfiglio, Caterina, Rossella Tatoli, Rossella Donghia, Davide Guido, and Gianluigi Giannelli. 2024. "Exploratory Role of Flavonoids on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in a South Italian Cohort" Antioxidants 13, no. 11: 1286. https://doi.org/10.3390/antiox13111286
APA StyleBonfiglio, C., Tatoli, R., Donghia, R., Guido, D., & Giannelli, G. (2024). Exploratory Role of Flavonoids on Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) in a South Italian Cohort. Antioxidants, 13(11), 1286. https://doi.org/10.3390/antiox13111286