
Poplar Propolis Improves Insulin Homeostasis in Non-Diabetic Insulin-Resistant Volunteers with Obesity: A Crossover Randomized Controlled Trial

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Design
2.3. Participants
2.4. Dietary Survey
2.5. Outcomes Measurements
2.6. Oral Glucose Tolerance Test (OGTT)
2.7. Measure of Insulin Sensitivity, Insulin Secretion, and Beta Cell Function
2.8. Measure of Biochemical Parameters
2.9. Measure of Anthropometric Parameters
2.10. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Effect of Poplar Propolis on Insulin Resistance (ISI-M), Insulin Secretion, and Pancreatic Beta Cell Function
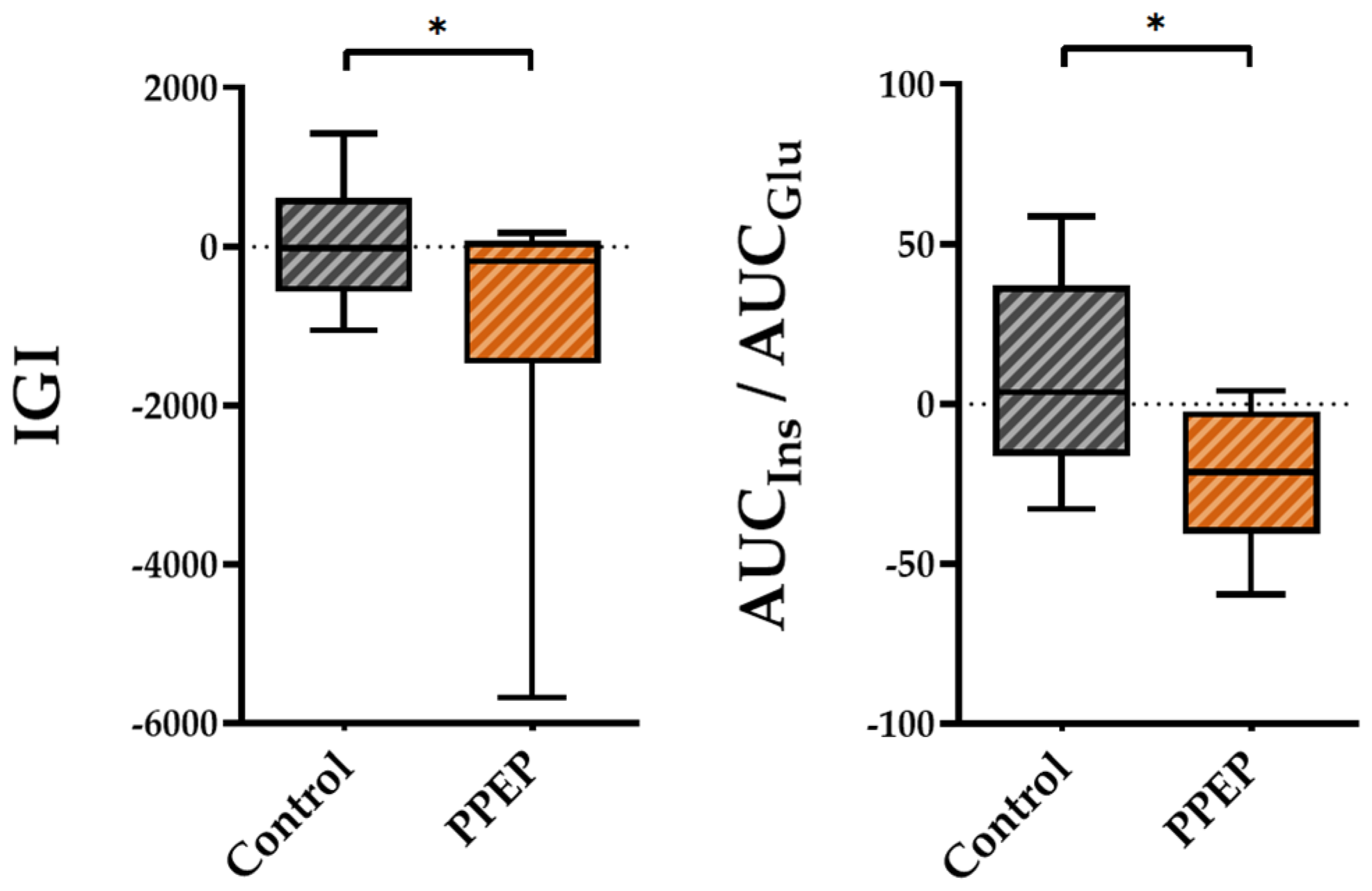
3.3. Effect of Poplar Propolis on Glucose and Insulin Homeostasis during OGTT
3.4. Effect of Poplar Propolis on Anthropometric and Biological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; Pavkov, M.E.; International Diabetes Federation (IDF); et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Ahmad, E.; Lim, S.; Lamptey, R.; Webb, D.R.; Davies, M.J. Type 2 Diabetes. Lancet 2022, 400, 1803–1820. [Google Scholar] [CrossRef] [PubMed]
- Kalin, M.F.; Goncalves, M.; Fonseca, V. Pathogenesis of Type 2 Diabetes Mellitus. Principles of Diabetes Mellitus; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–11. [Google Scholar] [CrossRef]
- Tuso, P. Prediabetes and Lifestyle Modification: Time to Prevent a Preventable Disease. Perm. J. 2014, 18, 88. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; DeFronzo, R.A. Insulin Sensitivity Indices Obtained from Oral Glucose Tolerance Testing: Comparison with the Euglycemic Insulin Clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and Management of Type 2 Diabetes: Dietary Components and Nutritional Strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef] [PubMed]
- Philouze, C.; Martin, J.-C.; Riva, C.; Marziou, A.; Defoort, C.; Couturier, C.; Berton, T.; Astier, J.; Jover, B.; Gayrard, N.; et al. Vitamin D3 Supplementation Alleviates Left Ventricular Dysfunction in a Mouse Model of Diet-Induced Type 2 Diabetes: Potential Involvement of Cardiac Lipotoxicity Modulation. Cardiovasc. Drugs Ther. 2022, 36, 245–256. [Google Scholar] [CrossRef]
- Maiga, B.; Cheick, O.B.; Ahmed, M.A.A.; Anne, A.; Gagnon, M.-P.; Traoré, S.A.; Landrier, J.F.; Geissbuhler, A. Effectiveness of Digital Health Interventions for Diabetes: Systematic Review of Systematic Reviews. Res. Sq. 2020. preprint. [Google Scholar] [CrossRef]
- Ben Amara, N.; Tourniaire, F.; Maraninchi, M.; Attia, N.; Amiot-Carlin, M.J.; Raccah, D.; Valéro, R.; Landrier, J.F.; Darmon, P. Independent Positive Association of Plasma β-Carotene Concentrations with Adiponectin among Non-Diabetic Obese Subjects. Eur. J. Nutr. 2015, 54, 447–454. [Google Scholar] [CrossRef]
- Amiot, M.-J.; Riollet, C.; Landrier, J.-F. Polyphénols et syndrome métabolique: Polyphenols and metabolic syndrome. Médecine Mal. Métab. 2009, 3, 476–482. [Google Scholar] [CrossRef]
- Huang, S.; Zhang, C.-P.; Wang, K.; Li, G.; Hu, F.-L. Recent Advances in the Chemical Composition of Propolis. Molecules 2014, 19, 19610–19632. [Google Scholar] [CrossRef]
- Bankova, V. Chemical Diversity of Propolis and the Problem of Standardization. J. Ethnopharmacol. 2005, 100, 114–117. [Google Scholar] [CrossRef]
- Cardinault, N.; Tourniaire, F.; Astier, J.; Couturier, C.; Bonnet, L.; Seipelt, E.; Karkeni, E.; Letullier, C.; Dlalah, N.; Georgé, S.; et al. Botanic Origin of Propolis Extract Powder Drives Contrasted Impact on Diabesity in High-Fat-Fed Mice. Antioxidants 2021, 10, 411. [Google Scholar] [CrossRef]
- Kurek-Górecka, A.; Rzepecka-Stojko, A.; Górecki, M.; Stojko, J.; Sosada, M.; Świerczek-Zięba, G. Structure and Antioxidant Activity of Polyphenols Derived from Propolis. Molecules 2013, 19, 78–101. [Google Scholar] [CrossRef]
- Kitamura, H. Effects of Propolis Extract and Propolis-Derived Compounds on Obesity and Diabetes: Knowledge from Cellular and Animal Models. Molecules 2019, 24, 4394. [Google Scholar] [CrossRef] [PubMed]
- Cardinault, N.; Tourniaire, F.; Astier, J.; Couturier, C.; Perrin, E.; Dalifard, J.; Seipelt, E.; Mounien, L.; Letullier, C.; Bonnet, L.; et al. Poplar Propolis Ethanolic Extract Reduces Body Weight Gain and Glucose Metabolism Disruption in High-Fat Diet-Fed Mice. Mol. Nutr. Food Res. 2020, 64, 2000275. [Google Scholar] [CrossRef]
- Fuliang, H.U.; Hepburn, H.R.; Xuan, H.; Chen, M.; Daya, S.; Radloff, S.E. Effects of Propolis on Blood Glucose, Blood Lipid and Free Radicals in Rats with Diabetes Mellitus. Pharmacol. Res. 2005, 51, 147–152. [Google Scholar] [CrossRef]
- Zhu, W.; Chen, M.; Shou, Q.; Li, Y.; Hu, F. Biological Activities of Chinese Propolis and Brazilian Propolis on Streptozotocin-Induced Type 1 Diabetes Mellitus in Rats. Evid. Based Complement. Alternat. Med. 2011, 8, 468529. [Google Scholar] [CrossRef] [PubMed]
- Balica, G.; Vostinaru, O.; Stefanescu, C.; Mogosan, C.; Iaru, I.; Cristina, A.; Pop, C.E. Potential Role of Propolis in the Prevention and Treatment of Metabolic Diseases. Plants 2021, 10, 883. [Google Scholar] [CrossRef] [PubMed]
- Gardana, C.; Scaglianti, M.; Pietta, P.; Simonetti, P. Analysis of the Polyphenolic Fraction of Propolis from Different Sources by Liquid Chromatography–Tandem Mass Spectrometry. J. Pharm. Biomed. Anal. 2007, 45, 390–399. [Google Scholar] [CrossRef]
- Reagan-Shaw, S.; Nihal, M.; Ahmad, N. Dose Translation from Animal to Human Studies Revisited. FASEB J. 2008, 22, 659–661. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Obésité: Prévention et Prise en Charge de L’épidémie Mondiale; Rapport d’une Consultation de l’OMS; WHO: Geneva, Switerland, 2003. [Google Scholar]
- Gayoso-Diz, P.; Otero-González, A.; Rodriguez-Alvarez, M.X.; Gude, F.; García, F.; De Francisco, A.; Quintela, A.G. Insulin Resistance (HOMA-IR) Cut-off Values and the Metabolic Syndrome in a General Adult Population: Effect of Gender and Age: EPIRCE Cross-Sectional Study. BMC Endocr. Disord. 2013, 13, 47. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Deheeger, M.; Preziosi, P. SU. VI. MAX SU.VI.MAX. Portions Alimentaires Manuel-Photos Pour L’estimation des Quantites (SU. VI. MAX. Photograph Book for the Estimation of Portion Sizes); Editions Polytechnica; ECONOMICA: Paris, France, 2002. [Google Scholar]
- DeFronzo, R.A.; Matsuda, M. Reduced Time Points to Calculate the Composite Index. Diabetes Care 2010, 33, e93. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.R.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C.; ResearchLaboratories, D. Homeostasis Model Assessment: Insulin Resistance and Fl-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Bastard, J.P.; Vandernotte, J.M.; Faraj, M.; Karelis, A.D.; Messier, L.; Malita, F.M.; Garrel, D.; Prud’homme, D.; Rabasa-Lhoret, R. Relationship between the Hyperinsulinemic–Euglycaemic Clamp and a New Simple Index Assessing Insulin Sensitivity in Overweight and Obese Postmenopausal Women. Diabetes Metab. 2007, 33, 261–268. [Google Scholar] [CrossRef]
- Hanson, R.L.; Pratley, R.E.; Bogardus, C.; Narayan, K.M.; Roumain, J.M.; Imperatore, G.; Fagot-Campagna, A.; Pettitt, D.J.; Bennett, P.H.; Knowler, W.C. Evaluation of Simple Indices of Insulin Sensitivity and Insulin Secretion for Use in Epidemiologic Studies. Am. J. Epidemiol. 2000, 151, 190–198. [Google Scholar] [CrossRef]
- Saisho, Y.; Miyakoshi, K.; Tanaka, M.; Shimada, A.; Ikenoue, S.; Kadohira, I.; Yoshimura, Y.; Itoh, H. Beta Cell Dysfunction and Its Clinical Significance in Gestational Diabetes. Endocr. J. 2010, 57, 973–980. [Google Scholar] [CrossRef] [PubMed]
- De Ligt, M.; Bergman, M.; Fuentes, R.M.; Essers, H.; Moonen-Kornips, E.; Havekes, B.; Schrauwen-Hinderling, V.B.; Schrauwen, P. No Effect of Resveratrol Supplementation after 6 Months on Insulin Sensitivity in Overweight Adults: A Randomized Trial. Am. J. Clin. Nutr. 2020, 112, 1029–1038. [Google Scholar] [CrossRef]
- Siyasinghe, N.M.; Sooriyarachchi, M.R. Guidelines for Calculating Sample Size in 2 × 2 Crossover Trials: A Simulation Study. J. Natl. Sci. Found. Sri Lanka 2011, 39, 77. [Google Scholar] [CrossRef]
- Manach, C.; Williamson, G.; Morand, C.; Scalbert, A.; Rémésy, C. Bioavailability and Bioefficacy of Polyphenols in Humans. I. Review of 97 Bioavailability Studies. Am. J. Clin. Nutr. 2005, 81, 230S–242S. [Google Scholar] [CrossRef]
- Almutairi, R.; Basson, A.R.; Wearsh, P.; Cominelli, F.; Rodriguez-Palacios, A. Validity of Food Additive Maltodextrin as Placebo and Effects on Human Gut Physiology: Systematic Review of Placebo-Controlled Clinical Trials. Eur. J. Nutr. 2022, 61, 2853–2871. [Google Scholar] [CrossRef]
- Gioxari, A.; Amerikanou, C.; Nestoridi, I.; Gourgari, E.; Pratsinis, H.; Kalogeropoulos, N.; Andrikopoulos, N.K.; Kaliora, A.C. Carob: A Sustainable Opportunity for Metabolic Health. Foods 2022, 11, 2154. [Google Scholar] [CrossRef] [PubMed]
- Hallajzadeh, J.; Milajerdi, A.; Amirani, E.; Attari, V.E.; Maghsoudi, H.; Mirhashemi, S.M. Effects of Propolis Supplementation on Glycemic Status, Lipid Profiles, Inflammation and Oxidative Stress, Liver Enzymes, and Body Weight: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. J. Diabetes Metab. Disord. 2021, 20, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Zakerkish, M.; Jenabi, M.; Zaeemzadeh, N.; Hemmati, A.A.; Neisi, N. The Effect of Iranian Propolis on Glucose Metabolism, Lipid Profile, Insulin Resistance, Renal Function and Inflammatory Biomarkers in Patients with Type 2 Diabetes Mellitus: A Randomized Double-Blind Clinical Trial. Sci. Rep. 2019, 9, 7289. [Google Scholar] [CrossRef] [PubMed]
- Afsharpour, F.; Javadi, M.; Hashemipour, S.; Koushan, Y.; Haghighian, H.K. Propolis Supplementation Improves Glycemic and Antioxidant Status in Patients with Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Study. Complement. Ther. Med. 2019, 43, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Samadi, N.; Mozaffari-Khosravi, H.; Rahmanian, M.; Askarishahi, M. Effects of Bee Propolis Supplementation on Glycemic Control, Lipid Profile and Insulin Resistance Indices in Patients with Type 2 Diabetes: A Randomized, Double-Blind Clinical Trial. J. Integr. Med. 2017, 15, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Mujica, V.; Orrego, R.; Pérez, J.; Romero, P.; Ovalle, P.; Zúñiga-Hernández, J.; Arredondo, M.; Leiva, E. The Role of Propolis in Oxidative Stress and Lipid Metabolism: A Randomized Controlled Trial. Evid. Based Complement. Alternat. Med. 2017, 2017, 4272940. [Google Scholar] [CrossRef]
- Fukuda, T.; Fukui, M.; Tanaka, M.; Senmaru, T.; Iwase, H.; Yamazaki, M.; Aoi, W.; Inui, T.; Nakamura, N.; Marunaka, Y. Effect of Brazilian Green Propolis in Patients with Type 2 Diabetes: A Double-Blind Randomized Placebo-Controlled Study. Biomed. Rep. 2015, 3, 355–360. [Google Scholar] [CrossRef]
- Gutch, M.; Kumar, S.; Razi, S.M.; Gupta, K.K.; Gupta, A. Assessment of Insulin Sensitivity/Resistance. Indian J. Endocrinol. Metab. 2015, 19, 160–164. [Google Scholar] [CrossRef]
- Ochoa-Morales, P.D.; González-Ortiz, M.; Martínez-Abundis, E.; Pérez-Rubio, K.G.; Patiño-Laguna, A.D.J. Anti-Hyperglycemic Effects of Propolis or Metformin in Type 2 Diabetes Mellitus. Int. J. Vitam. Nutr. Res. 2022. [Google Scholar] [CrossRef] [PubMed]
- Alyass, A.; Almgren, P.; Akerlund, M.; Dushoff, J.; Isomaa, B.; Nilsson, P.; Tuomi, T.; Lyssenko, V.; Groop, L.; Meyre, D. Modelling of OGTT Curve Identifies 1 h Plasma Glucose Level as a Strong Predictor of Incident Type 2 Diabetes: Results from Two Prospective Cohorts. Diabetologia 2015, 58, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Peddinti, G.; Bergman, M.; Tuomi, T.; Groop, L. 1-Hour Post-OGTT Glucose Improves the Early Prediction of Type 2 Diabetes by Clinical and Metabolic Markers. J. Clin. Endocrinol. Metab. 2019, 104, 1131–1140. [Google Scholar] [CrossRef] [PubMed]
- Vijay Kumar, D.K.; Sultanpur Chandrashekar, M. Comprehensive Review on HbA1c in Diagnosis of Diabetes Mellitus. Int. J. Pharm. Sci. Rev. Res. 2010, 3, 4. [Google Scholar]
- Giessen, R.G.B.; Marburg, K.V.; Bochum, H.S. The United Kingdom Prospective Diabetes Study (UKPDS) Implications for the Pharmacotherapy of Type 2 Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 1998, 106, 369–372. [Google Scholar] [CrossRef]
- Hesami, S.; Hashemipour, S.; Shiri-Shahsavar, M.R.; Koushan, Y.; Khadem Haghighian, H. Administration of Iranian Propolis Attenuates Oxidative Stress and Blood Glucose in Type II Diabetic Patients: A Randomized, Double-Blind, Placebo-Controlled, Clinical Trial. Casp. J. Intern. Med. 2019, 10, 48–54. [Google Scholar] [CrossRef]
- Karimian, J.; Hadi, A.; Pourmasoumi, M.; Najafgholizadeh, A.; Ghavami, A. The Efficacy of Propolis on Markers of Glycemic Control in Adults with Type 2 Diabetes Mellitus: A Systematic Review and Meta-analysis. Phytother. Res. 2019, 33, 1616–1626. [Google Scholar] [CrossRef]
- El-Sharkawy, H.M.; Anees, M.M.; Van Dyke, T.E. Propolis Improves Periodontal Status and Glycemic Control in Patients with Type 2 Diabetes Mellitus and Chronic Periodontitis: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 1418–1426. [Google Scholar] [CrossRef]
- Janhavi, P.; Divyashree, S.; Sanjailal, K.P.; Muthukumar, S.P. DoseCal: A Virtual Calculator for Dosage Conversion between Human and Different Animal Species. Arch. Physiol. Biochem. 2022, 128, 426–430. [Google Scholar] [CrossRef]
- Nie, J.; Chang, Y.; Li, Y.; Zhou, Y.; Qin, J.; Sun, Z.; Li, H. Caffeic Acid Phenethyl Ester (Propolis Extract) Ameliorates Insulin Resistance by Inhibiting JNK and NF-ΚB Inflammatory Pathways in Diabetic Mice and HepG2 Cell Models. J. Agric. Food Chem. 2017, 65, 9041–9053. [Google Scholar] [CrossRef]
- Ueda, M.; Hayashibara, K.; Ashida, H. Propolis Extract Promotes Translocation of Glucose Transporter 4 and Glucose Uptake through Both PI3K- and AMPK-Dependent Pathways in Skeletal Muscle: Propolis Promotes Glucose Uptake and GLUT4 Translocation in Muscle. BioFactors 2013, 39, 457–466. [Google Scholar] [CrossRef]
- Kang, L.-J.; Lee, H.B.; Bae, H.-J.; Lee, S.-G. Antidiabetic Effect of Propolis: Reduction of Expression of Glucose-6-Phosphatase through Inhibition of Y279 and Y216 Autophosphorylation of GSK-3α/β in HepG2 Cells. Phytother. Res. 2010, 24, 1554–1561. [Google Scholar] [CrossRef]
- Ferrannini, E.; Vichi, S.; Beck-Nielsen, H.; Laakso, M.; Paolisso, L.; Smith, G.; European Group for the Study of Insulin Resistance. Insulin Action and Age: European Group for the Study of Insulin Resistance (EGIR). Diabetes 1996, 45, 947–953. [Google Scholar] [CrossRef]
- Paolisso, G.; Tagliamonte, M.R.; Rizzo, M.R.; Giugliano, D. Advancing Age and Insulin Resistance: New Facts about an Ancient History: Advancing Age and Insulin Resistance. Eur. J. Clin. Investig. 1999, 29, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Natsir, R.; Usman, A.N.; Ardyansyah, B.D.; Fendi, F. Propolis and Honey Trigona Decrease Leptin Levels of Central Obesity Patients. Enferm. Clín. 2020, 30, 96–99. [Google Scholar] [CrossRef]
- Gao, W.; Pu, L.; Wei, J.; Yao, Z.; Wang, Y.; Shi, T.; Zhao, L.; Jiao, C.; Guo, C. Serum Antioxidant Parameters Are Significantly Increased in Patients with Type 2 Diabetes Mellitus after Consumption of Chinese Propolis: A Randomized Controlled Trial Based on Fasting Serum Glucose Level. Diabetes Ther. 2018, 9, 101–111. [Google Scholar] [CrossRef]
- Silveira, M.A.D.; Teles, F.; Berretta, A.A.; Sanches, T.R.; Rodrigues, C.E.; Seguro, A.C.; Andrade, L. Effects of Brazilian Green Propolis on Proteinuria and Renal Function in Patients with Chronic Kidney Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. BMC Nephrol. 2019, 20, 140. [Google Scholar] [CrossRef]
- Zhu, A.; Wu, Z.; Zhong, X.; Ni, J.; Li, Y.; Meng, J.; Nakanishi, H.; Wu, S. Brazilian Green Propolis Prevents Cognitive Decline into Mild Cognitive Impairment in Elderly People Living at High Altitude. J. Alzheimers Dis. 2018, 63, 551–560. [Google Scholar] [CrossRef]
- Khayyal, M.T.; El-Ghazaly, M.A.; El-Khatib, A.S.; Hatem, A.M.; de Vries, P.J.F.; El-Shafei, S.; Khattab, M.M. A Clinical Pharmacological Study of the Potential Beneficial Effects of a Propolis Food Product as an Adjuvant in Asthmatic Patients—Khayyal—2003—Fundamental & Clinical Pharmacology—Wiley Online Library. Fundam. Clin. Pharmacol. 2003, 17, 93–102. [Google Scholar] [PubMed]
- Gholaminejad, F.; Javadi, M.; Karami, A.A.; Alizadeh, F.; Kavianpour, M.; Khadem Haghighian, H. Propolis Supplementation Effects on Semen Parameters, Oxidative Stress, Inflammatory Biomarkers and Reproductive Hormones in Infertile Men with Asthenozoospermia; A Randomized Clinical Trial. Int. J. Med. Lab. 2019, 6, 21–32. [Google Scholar] [CrossRef]
- Oršolić, N.; Landeka Jurčević, I.; Đikić, D.; Rogić, D.; Odeh, D.; Balta, V.; Perak Junaković, E.; Terzić, S.; Jutrić, D. Effect of Propolis on Diet-Induced Hyperlipidemia and Atherogenic Indices in Mice. Antioxidants 2019, 8, 156. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polyphenol Content 1 | Quantity 2 |
|---|---|
| Pinocembrin | 3718 |
| Chrysin | 2580 |
| Galangin | 2006 |
| Caffeic acid phenethyl ester (CAPE) | 1782 |
| Coumaric acid | 800 |
| Caffeic acid | 756 |
| Cinnamic acid | 611 |
| Kaempferol | 526 |
| Quercetin | 414 |
| Ferulic acid | 263 |
| Apigenin | 198 |
| Control (n = 9) | p-Value 1 | PPEP (n = 9) | p-Value 1 | p-Value 2 | ||
|---|---|---|---|---|---|---|
| Insulin Homeostasis (mUI/L) | ||||||
| Fasting insulinemia | Baseline | 25.2 ± 12.4 | 0.19 | 29.9 ± 21.7 | 0.91 | |
| 3 months | 17.1 ± 6.8 | 28.7 ± 25.6 | ||||
| Δ | −8.1 ± 16.2 | −1.2 ± 30.1 | 0.56 | |||
| Time 30 of OGTT | Baseline | 79.3 ± 26.2 | 0.80 | 83.1 ± 30.6 | 0.18 | |
| 3 months | 81.9 ± 33.3 | 64.6 ± 36.4 | ||||
| Δ | 2.6 ± 29.1 | −18.6 ± 38.4 | 0.17 | |||
| Time 60 of OGTT | Baseline | 90.6 ± 62.5 | 0.74 | 110.7 ± 54.2 | 0.06 | |
| 3 months | 96.3 ± 61.4 | 76.1 ± 34.7 | ||||
| Δ | 5.7 ± 48.6 | −34.6 ± 47.9 | 0.16 | |||
| Time 90 of OGTT | Baseline | 87.7 ± 48.7 | 0.93 | 109.7 ± 77.3 | 0.10 | |
| 3 months | 86.9 ± 43.7 | 61.7 ± 33.7 | ||||
| Δ | −0.8 ± 26.3 | −48.0 ± 78 | 0.13 | |||
| Time 120 of OGTT | Baseline | 59.9 ± 37.6 | 0.36 | 65.9 ± 49.8 | 0.16 | |
| 3 months | 69.6 ± 43.1 | 44.6 ± 14.7 | ||||
| Δ | 9.7 ± 29.9 | −21.3 ± 40.7 | 0.15 | |||
| Minimum value | Baseline | 23.2 ± 11 | 0.24 | 23.2 ± 16 | 0.41 | |
| 3 months | 17.1 ± 6.8 | 17.1 ± 9.4 | ||||
| Δ | −6.0 ± 13 | −6.1 ± 17.3 | 0.99 | |||
| Maximum value | Baseline | 113.8 ± 60.5 | 0.97 | 132.5 ± 71.1 | 0.17 | |
| 3 months | 114.5 ± 58.8 | 95.1 ± 35.1 | ||||
| Δ | 0.7 ± 47.3 | −37.4 ± 74.1 | 0.49 | |||
| Mean value | Baseline | 68.5 ± 30.5 | 0.82 | 79.9 ± 35.0 | 0.02 | |
| 3 months | 70.3 ± 31.1 | 55.1 ± 17.4 | ||||
| Δ | 1.8 ± 22.6 | −24.7 ± 32.4 | 0.08 | |||
| AUC insulinemia | Baseline | 8933 ± 4109 | 0.32 | 10,704 ± 4718 | 0.01 | |
| 3 months | 10,270 ± 4772 | 6377 ± 1893 | ||||
| Δ | 1336 ± 3783 | −4327 ± 4424 | 0.04 | |||
| Insulin resistance 3 | Yes | 9 (99.9%) | 6 (66.6%) | |||
| No | 0 (0.0%) | 3 (33.3%) | 0.04 | |||
| Control (n = 9) | p-Value 1 | PPEP (n = 9) | p-Value 1 | p-Value 2 | ||
|---|---|---|---|---|---|---|
| Glucose Homeostasis (g/L) | ||||||
| HbA1c (%) | Baseline | 5.47 ± 0.5 | 0.40 | 5.54 ± 0.5 | 0.75 | |
| 3 months | 5.69 ± 0.6 | 5.52 ± 0.5 | ||||
| Δ | 0.22 ± 0.4 | −0.02 ± 0.1 | 0.04 | |||
| Fasting glycemia | Baseline | 0.97 ± 0.3 | 0.29 | 0.97 ± 0.2 | 0.05 | |
| 3 months | 0.87 ± 0.2 | 0.86 ± 0.2 | ||||
| Δ | −0.1 ± 0.2 | −0.1 ± 0.2 | 0.82 | |||
| Time 30 of OGTT | Baseline | 1.4 ± 0.4 | 0.64 | 1.3 ± 0.3 | 0.14 | |
| 3 months | 1.3 ± 0.3 | 1.3 ± 0.2 | ||||
| Δ | 0.22 ± 0.4 | −0.22 ± 0.1 | 0.91 | |||
| Time 60 of OGTT | Baseline | 1.3 ± 0.5 | 0.46 | 1.3 ± 0.4 | 0.15 | |
| 3 months | 1.3 ± 0.5 | 1.2 ± 0.3 | ||||
| Δ | 0.05 ± 0.06 | −0.11 ± 0.21 | 0.06 | |||
| Time 90 of OGTT | Baseline | 1.1 ± 0.4 | 0.99 | 1.1 ± 0.4 | 0.09 | |
| 3 months | 1.1 ± 0.4 | 1.1 ± 0.4 | ||||
| Δ | 0.1 ± 0.2 | −0.1 ± 0.2 | 0.30 | |||
| Time 120 of OGTT | Baseline | 0.90 ± 0.3 | 0.54 | 0.97 ± 0.4 | 0.99 | |
| 3 months | 0.94 ± 0.3 | 0.98 ± 0.4 | ||||
| Δ | 0.03 ± 0.2 | 0.01 ± 0.2 | 0.49 | |||
| Minimum value | Baseline | 0.86 ± 0.3 | 0.37 | 0.82 ± 0.2 | 0.72 | |
| 3 months | 0.82 ± 0.2 | 0.80 ± 0.2 | ||||
| Δ | −0.05 ± 0.2 | −0.02 ± 0.2 | 0.69 | |||
| Maximum value | Baseline | 1.5 ± 0.4 | 0.61 | 1.4 ± 0.3 | 0.19 | |
| 3 months | 1.4 ± 0.5 | 1.3 ± 0.3 | ||||
| Δ | −0.03 ± 0.2 | −0.09 ± 0.2 | 0.30 | |||
| Mean value | Baseline | 1.14 ± 0.3 | 0.58 | 1.15 ± 0.3 | 0.16 | |
| 3 months | 1.11 ± 0.3 | 1.07 ± 0.3 | ||||
| Δ | −0.02 ± 0.1 | −0.08 ± 0.1 | 0.35 | |||
| AUC glycemia | Baseline | 142.3 ± 43.7 | 0.61 | 142.9 ± 36.5 | 0.09 | |
| 3 months | 139.8 ± 38.5 | 133.1 ± 32.8 | ||||
| Δ | −2.5 ± 14.0 | −9.8 ± 17.4 | 0.24 | |||
| Control (n = 9) | p-Value 1 | PPEP (n = 9) | p-Value 1 | p-Value 2 | ||
|---|---|---|---|---|---|---|
| Anthropometric and Nutritional Data | ||||||
| BMI (kg/m 2) | Baseline | 31.7 ± 3.2 | 0.97 | 31.5 ± 3.2 | 0.46 | |
| 3 months | 31.7 ± 3.1 | 31.7 ± 3.1 | ||||
| Δ | −0.01 ± 0.7 | 0.21 ± 0.8 | 0.49 | |||
| Waist circumference | Baseline | 98.7 ± 9.6 | 0.43 | 98.1 ± 9.9 | 0.19 | |
| (cm) | 3 months | 95.1 ± 16.6 | 99.3 ± 8.9 | |||
| Δ | −3.6 ± 12.9 | 1.2 ± 2.5 | 0.29 | |||
| Body fat (%) | Baseline | 41.1 ± 6.8 | 0.62 | 41.2 ± 6.9 | 0.96 | |
| 3 months | 41.4 ± 6.8 | 41.2 ± 6.6 | ||||
| Δ | 0.26 ± 1.4 | −0.03 ± 2.1 | 0.99 | |||
| Lean body mass (%) | Baseline | 58.9 ± 6.8 | 0.62 | 58.6 ± 6.9 | 0.85 | |
| 3 months | 58.6 ± 6.8 | 58.8 ± 6.6 | ||||
| Δ | −0.27 ± 1.4 | 0.14 ± 2.3 | 0.99 | |||
| E/I ratio 3 (kcal/J) | Baseline | 1.60 ± 0.5 | 1.52 ± 0.4 | 0.64 | ||
| Control (n = 9) | p-Value 1 | PPEP (n = 9) | p-Value 1 | p-Value 2 | ||
|---|---|---|---|---|---|---|
| Biological data | ||||||
| Renal function data | ||||||
| Creatinine (µmol/L) | Baseline | 66.9 ± 13 | 0.51 | 65.2 ± 12.6 | 0.22 | |
| 3 months | 68.1 ± 12.8 | 63.1 ± 12.9 | ||||
| Δ | 1.2 ± 5.2 | −2.1 ± 4.7 | 0.57 | |||
| Creatinine clearance 3 | Baseline | 127.2 ± 43.3 | 0.41 | 129.1 ± 43.1 | 0.16 | |
| 3 months | 124.2 ± 41.9 | 133.3 ± 39.9 | ||||
| Δ | −3.1 ± 8.8 | 4.2 ± 9 | 0.30 | |||
| Liver function data | ||||||
| AST (UI/L) | Baseline | 21.4 ± 4.8 | 0.82 | 22.8 ± 4.5 | 0.62 | |
| 3 months | 21.2 ± 5 | 21.9 ± 4.7 | ||||
| Δ | −0.2 ± 2.9 | −0.9 ± 5.3 | 0.89 | |||
| ALT (UI/L) | Baseline | 22 ± 12.7 | 0.99 | 23.1 ± 12.7 | 0.55 | |
| 3 months | 20.7 ± 8.4 | 21.8 ± 10.6 | ||||
| Δ | −1.3 ± 8.2 | −1.3 ± 12.1 | 0.99 | |||
| AST/ALT | Baseline | 1.2 ± 0.5 | 0.99 | 1.3 ± 0.8 | 0.91 | |
| 3 months | 1.2 ± 0.6 | 1.1 ± 0.4 | ||||
| Δ | 0.05 ± 0.3 | −0.12 ± 0.5 | 0.91 | |||
| GGT (UI/L) | Baseline | 23.6 ± 12.1 | 0.83 | 25. 9 ± 14.9 | 0.15 | |
| 3 months | 21 ± 10.6 | 24 ± 12.6 | ||||
| Δ | −2.6 + 11.9 | −1.9 ± 3.5 | 0.88 | |||
| Lipid profile data | ||||||
| Total cholesterol (g/L) | Baseline | 2.1 ± 0.4 | 0.91 | 2.1 ± 0.3 | 0.92 | |
| 3 months | 2.1 ± 0.4 | 2.1 ± 0.3 | ||||
| Δ | 0.03 ± 0.3 | 0.01 ± 0.3 | 0.99 | |||
| Triglycerides (g/L) | Baseline | 1.0 ± 0.4 | 0.76 | 1.1 ± 0.4 | 0.75 | |
| 3 months | 1.0 ± 0.4 | 1.1 ± 0.4 | ||||
| Δ | 0.04 ± 0.4 | 0.02 ± 0.1 | 0.73 | |||
| HDL-cholesterol (g/L) | Baseline | 0.6 ± 0.1 | 0.75 | 0.6 ± 0.1 | 0.31 | |
| 3 months | 0.6 ± 0.1 | 0.5 ± 0.1 | ||||
| Δ | −0.01 ± 0.08 | −0.01 ± 0.04 | 0.82 | |||
| LDL-cholesterol (g/L) | Baseline | 1.3 ± 0.3 | 0.77 | 1.4 ± 0.2 | 0.75 | |
| 3 months | 1.4 ± 0.4 | 1.4 ± 0.2 | ||||
| Δ | 0.03 ± 0.2 | 0.03 ± 0.2 | 0.91 | |||
| Adipose tissue function data | ||||||
| Leptin (pg/mL) | Baseline | 42,931 ± 18,137 | 0.73 | 37,266 ± 16,592 | 0.18 | |
| 3 months | 44,344 ± 18,395 | 45,587 ± 24,241 | ||||
| Δ | 1413 ± 11,710 | 8321 ± 16,861 | 0.36 | |||
| Adiponectin (ng/mL) | Baseline | 6882 ± 4462 | 0.91 | 7010 ± 4883 | 0.34 | |
| 3 months | 6791 ± 4475 | 6655 ± 5069 | ||||
| Δ | −90.6 ± 1107 | −355.4 ± 974 | 0.20 | |||
| Oxidative stress data | ||||||
| 8-iso-PGF 2α (pg/mL) | Baseline | 1533 ± 2812 | 0.16 | 1021 ± 1549 | 0.34 | |
| 3 months | 875 ± 1325 | 425 ± 393 | ||||
| Δ | −659 ± 1512 | −595 ± 1626 | 0.91 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sani, L.; Cardinault, N.; Astier, J.; Darmon, P.; Landrier, J.F. Poplar Propolis Improves Insulin Homeostasis in Non-Diabetic Insulin-Resistant Volunteers with Obesity: A Crossover Randomized Controlled Trial. Antioxidants 2023, 12, 1481. https://doi.org/10.3390/antiox12081481
Sani L, Cardinault N, Astier J, Darmon P, Landrier JF. Poplar Propolis Improves Insulin Homeostasis in Non-Diabetic Insulin-Resistant Volunteers with Obesity: A Crossover Randomized Controlled Trial. Antioxidants. 2023; 12(8):1481. https://doi.org/10.3390/antiox12081481
Chicago/Turabian StyleSani, Lea, Nicolas Cardinault, Julien Astier, Patrice Darmon, and Jean François Landrier. 2023. "Poplar Propolis Improves Insulin Homeostasis in Non-Diabetic Insulin-Resistant Volunteers with Obesity: A Crossover Randomized Controlled Trial" Antioxidants 12, no. 8: 1481. https://doi.org/10.3390/antiox12081481
APA StyleSani, L., Cardinault, N., Astier, J., Darmon, P., & Landrier, J. F. (2023). Poplar Propolis Improves Insulin Homeostasis in Non-Diabetic Insulin-Resistant Volunteers with Obesity: A Crossover Randomized Controlled Trial. Antioxidants, 12(8), 1481. https://doi.org/10.3390/antiox12081481