
The Effects of Polyphenols on Bone Metabolism in Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Control Trials

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statystical Analysis
3. Results
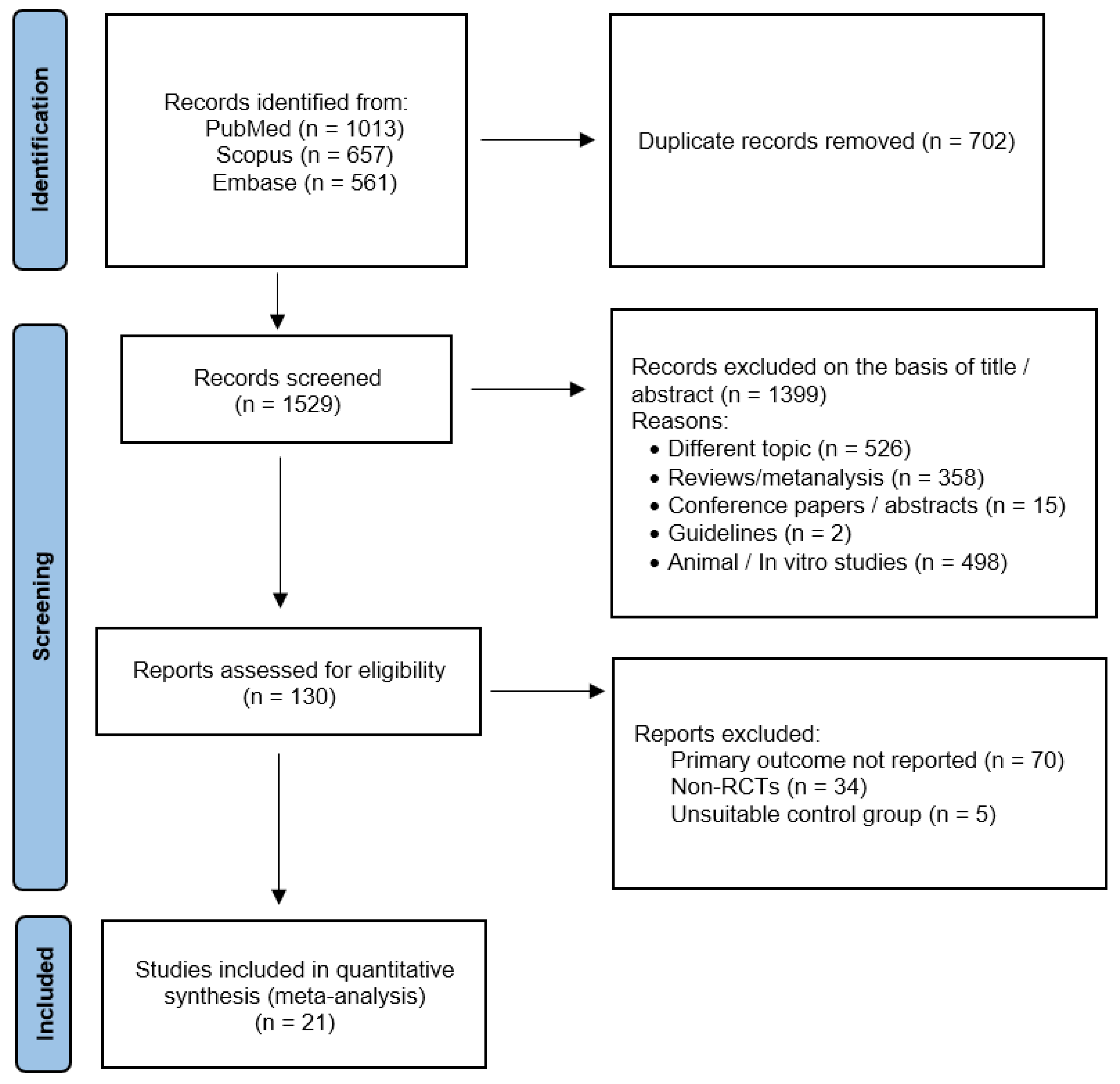
3.1. Study Selection
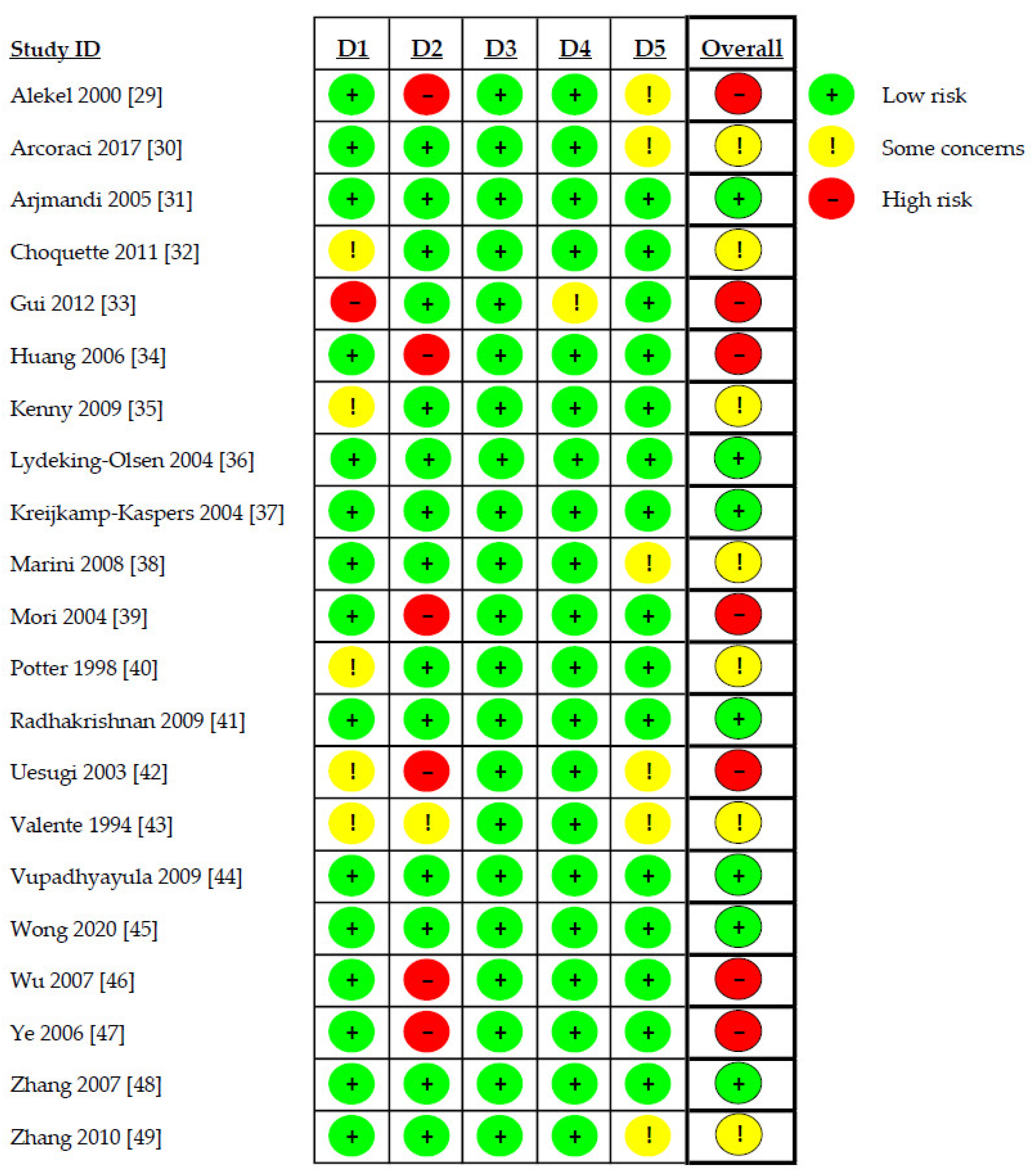
3.2. Risk of Bias Assessment
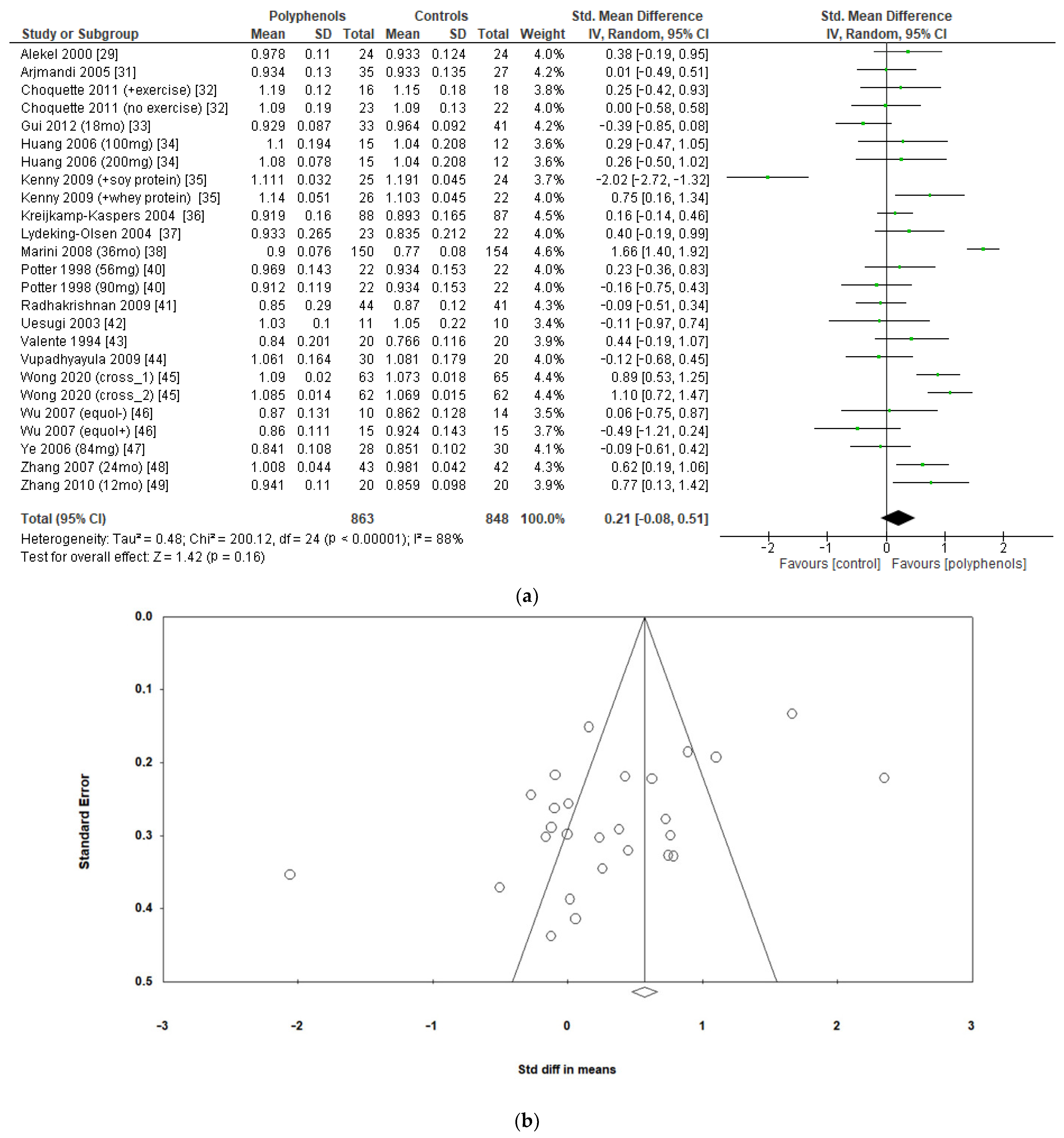
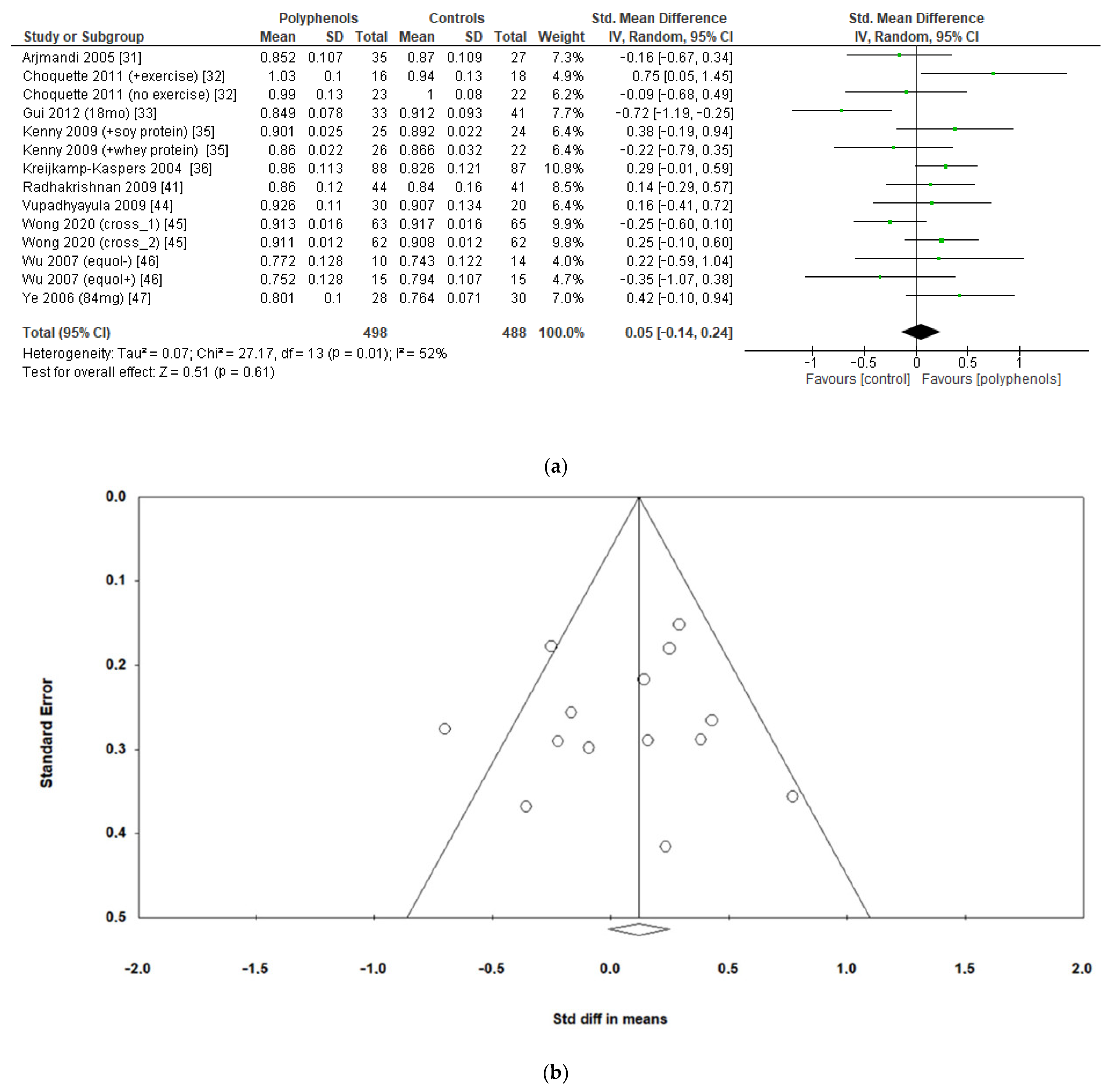
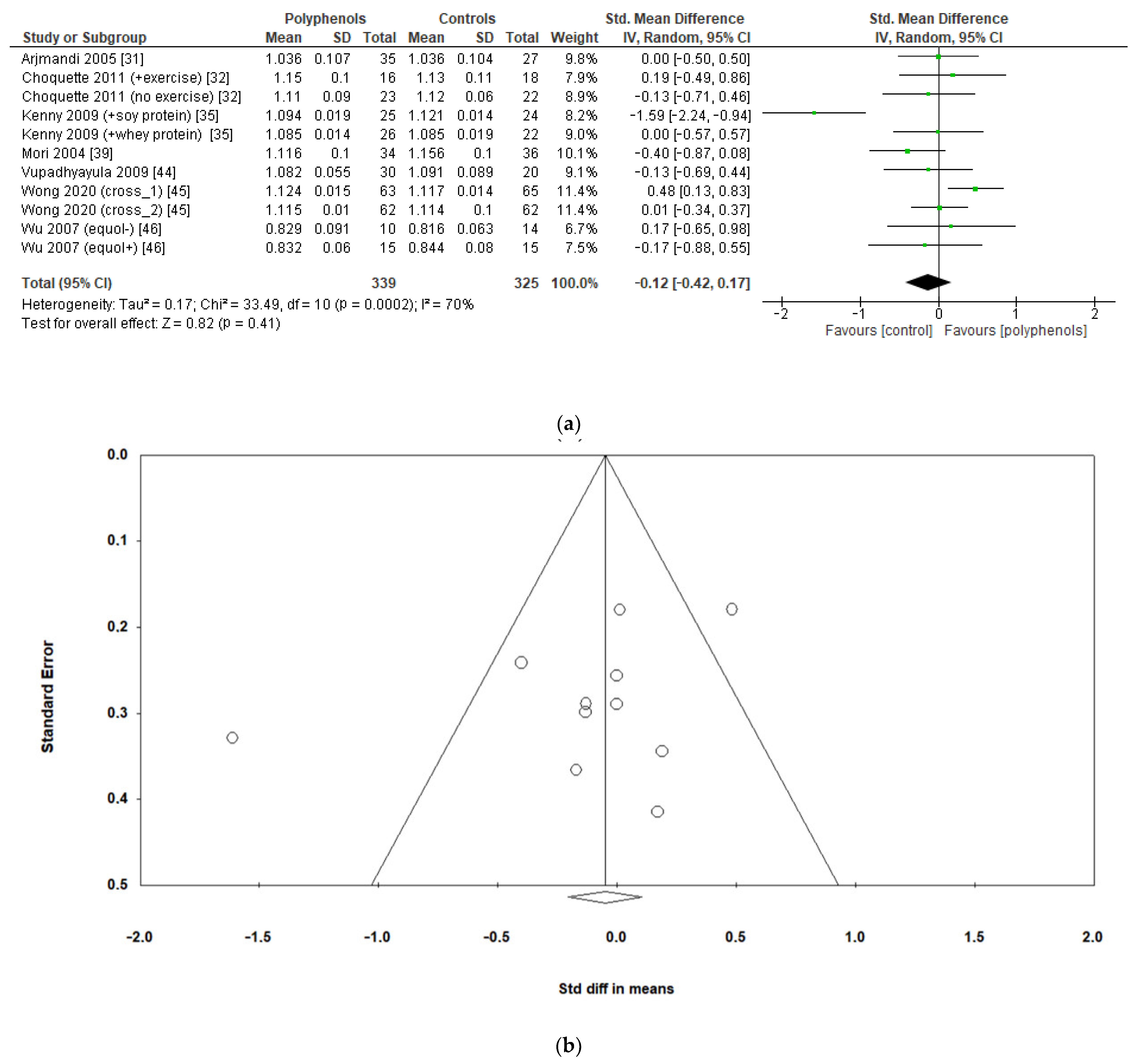
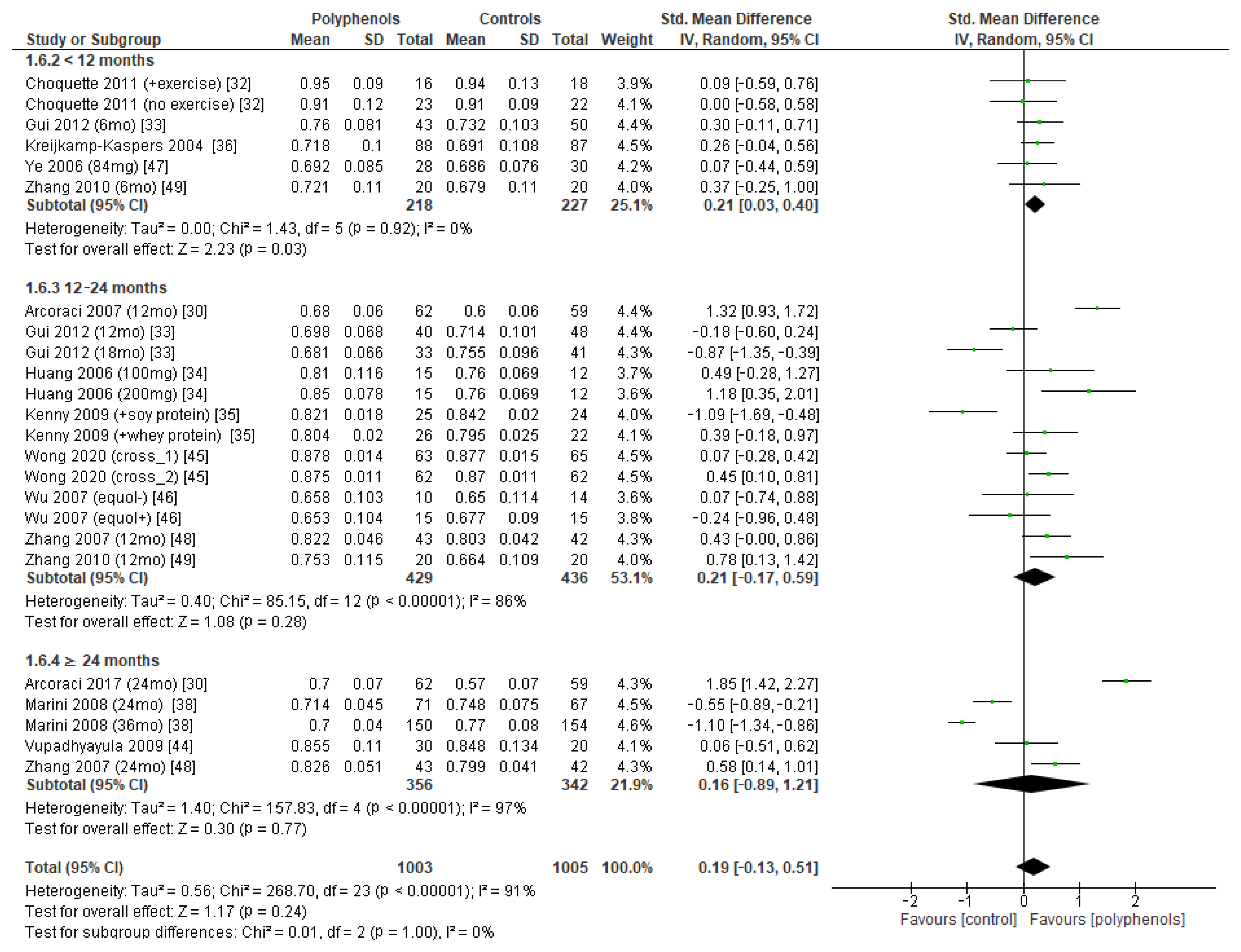
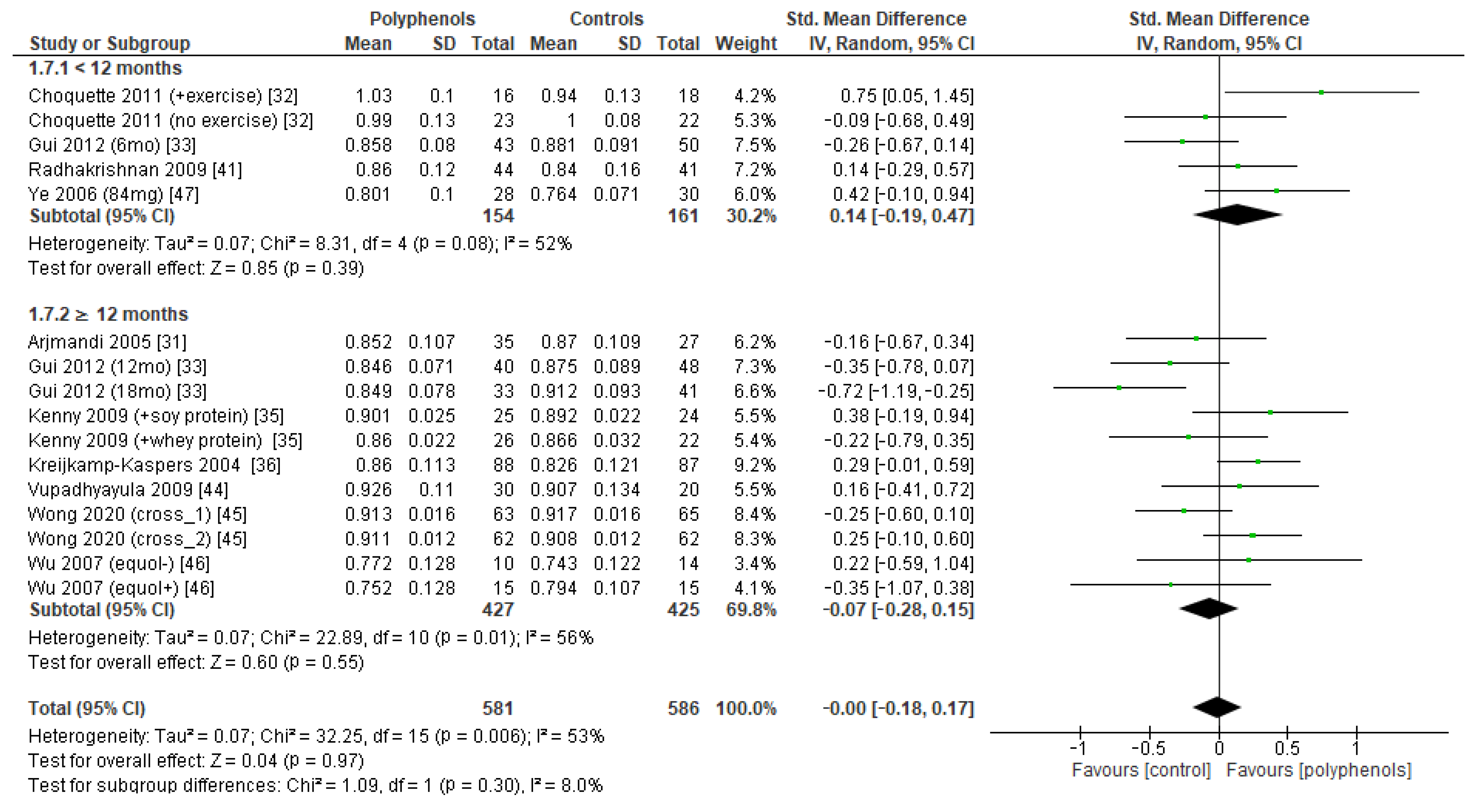
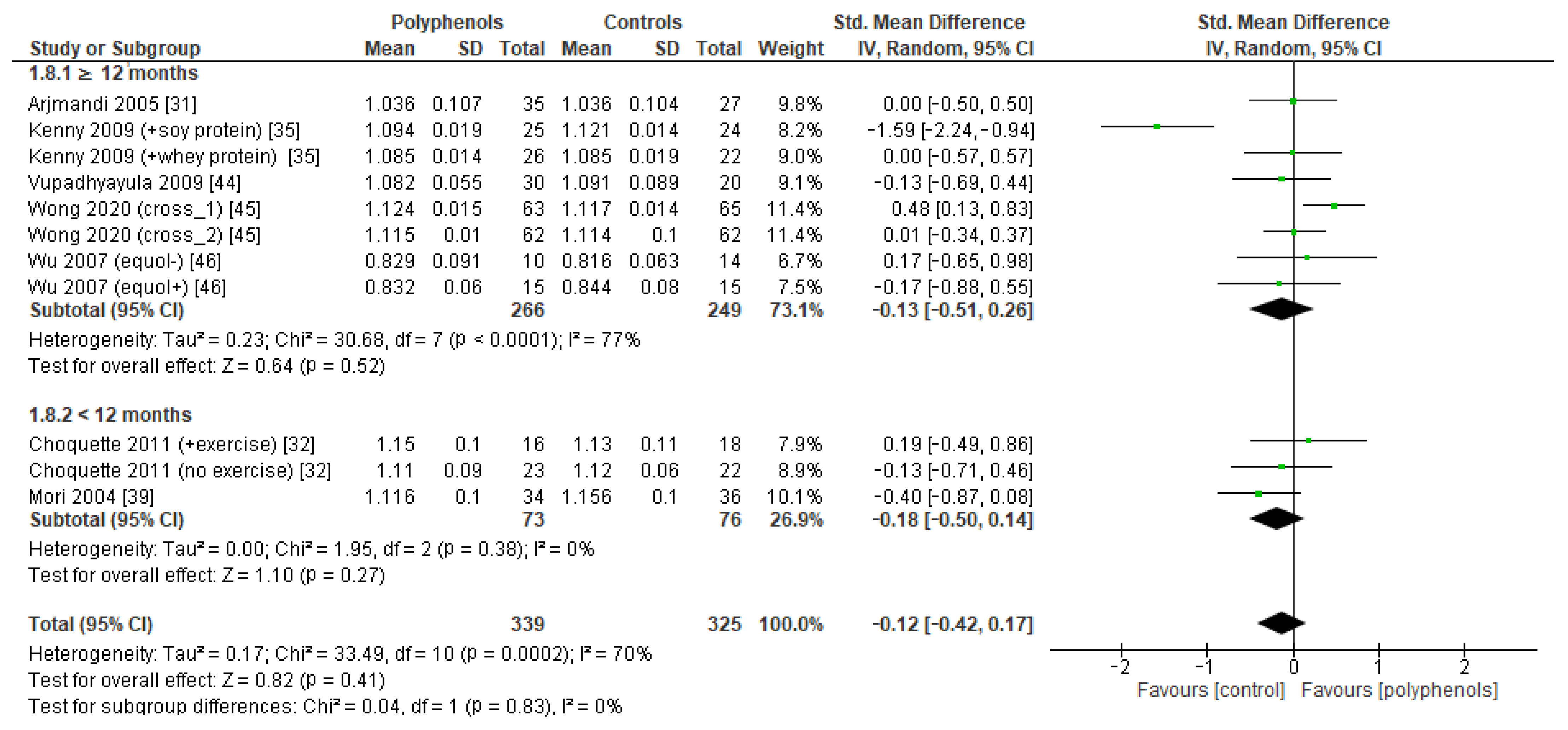
3.3. Primary Outcome: Effects of Polyphenols on Bone Mineral Density
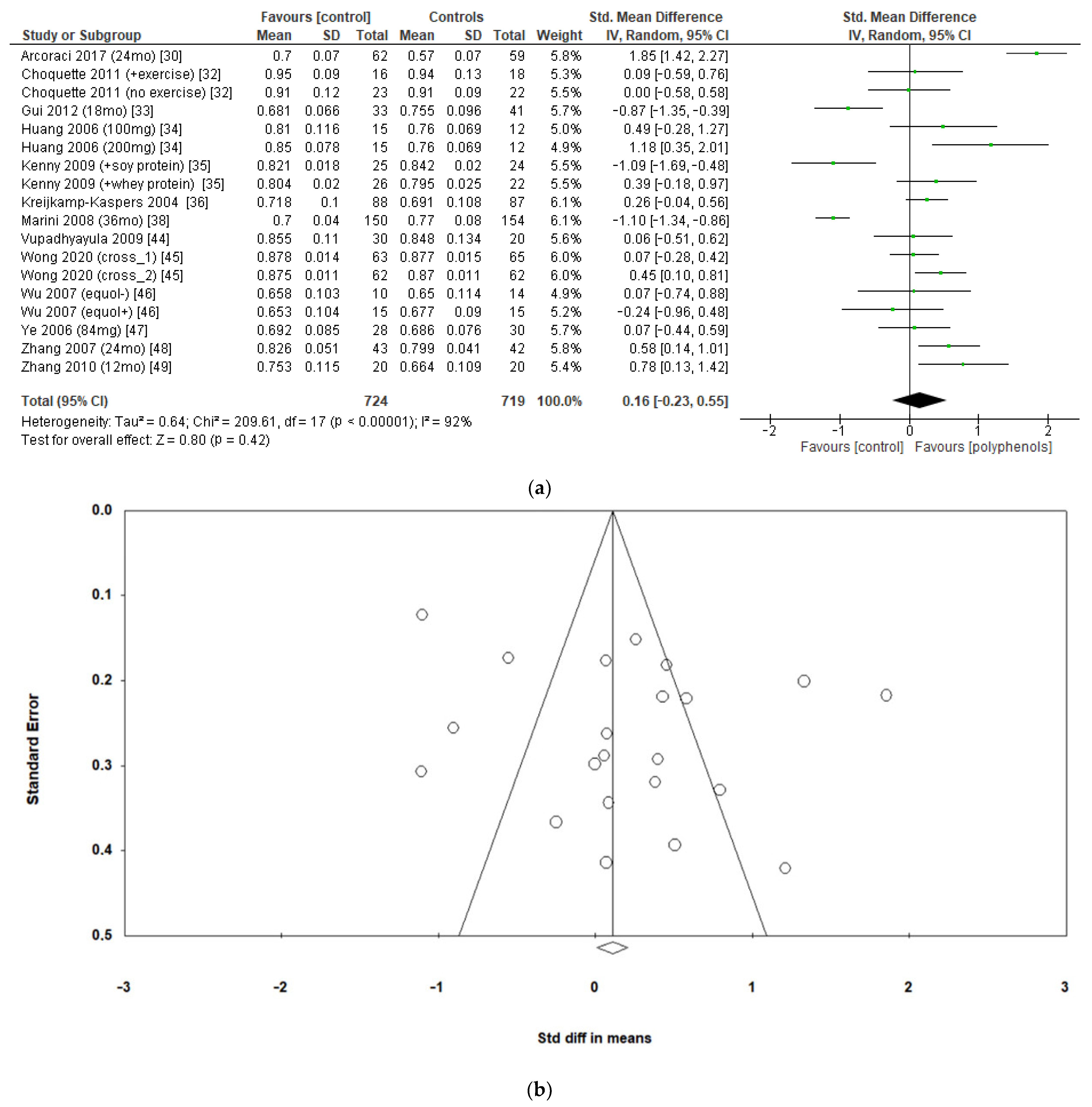
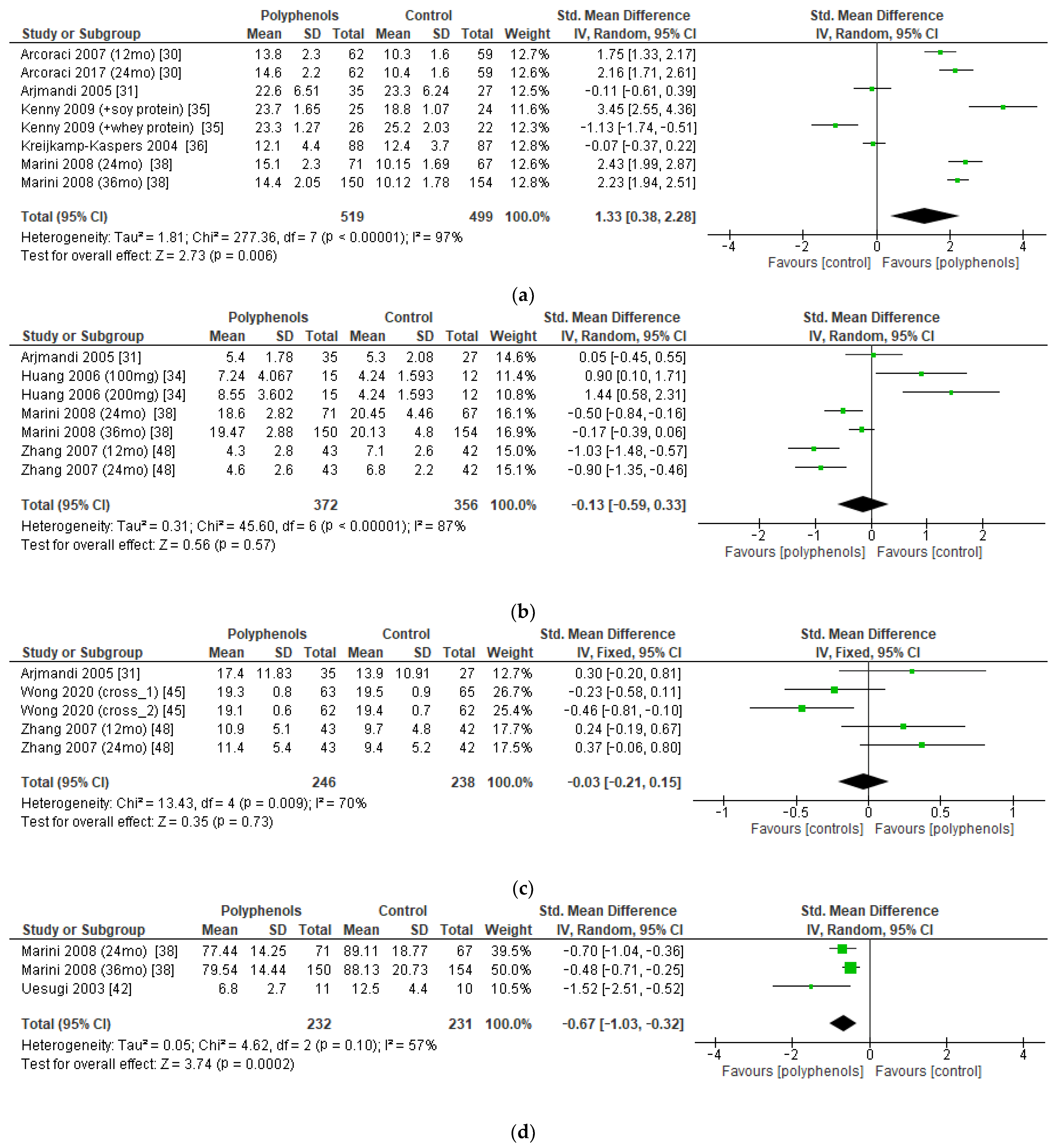
3.4. Secondary Outcome: Effects of Polyphenols on Bone Turnover Markers
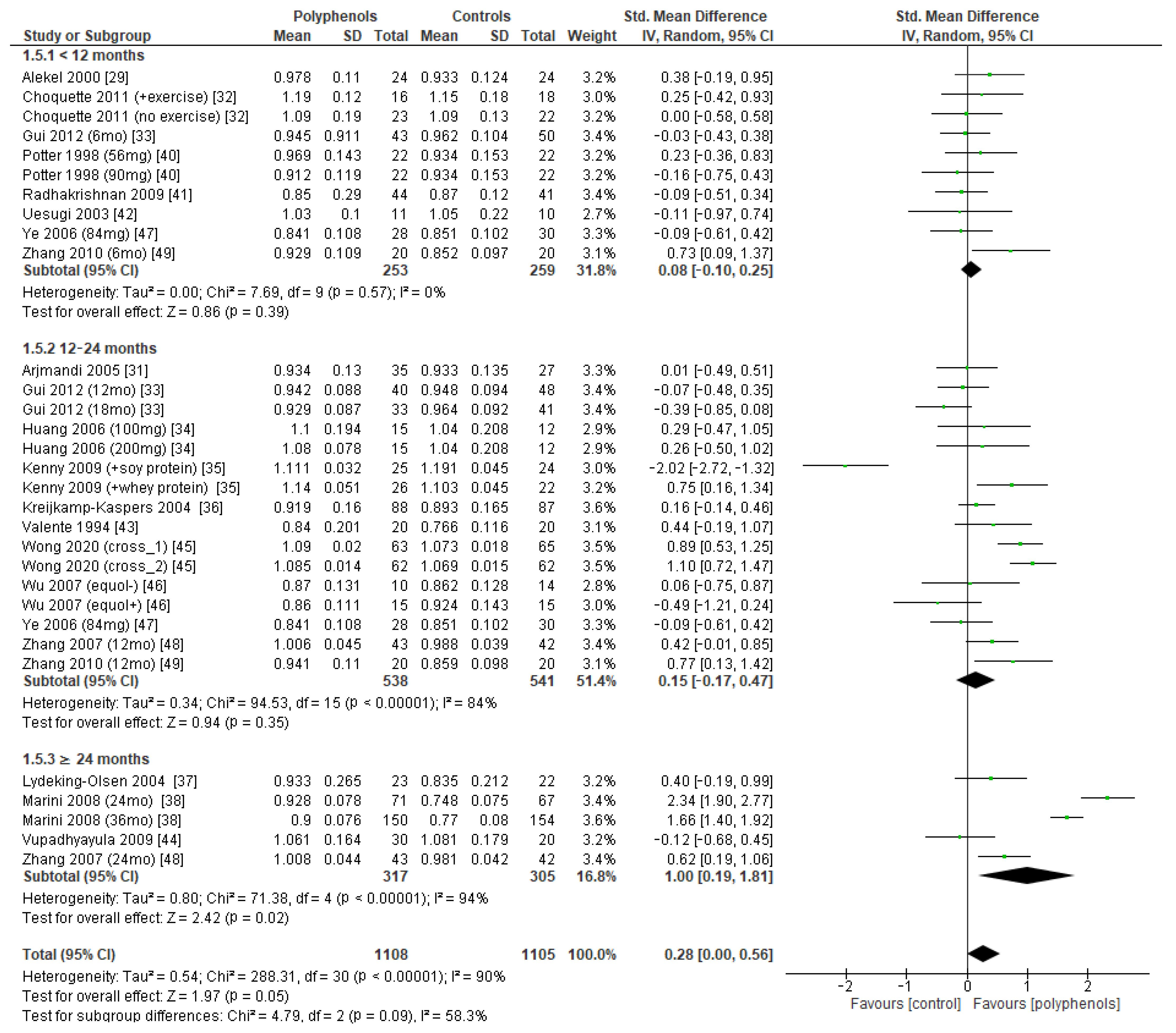
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gullberg, B.; Johnell, O.; Kanis, J.A. World-Wide Projections for Hip Fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and Economic Burden of Osteoporosis-Related Fractures in the United States, 2005–2025. J. Bone Miner. Res. 2007, 22, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An Estimate of the Worldwide Prevalence and Disability Associated with Osteoporotic Fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Kalervo Väänänen, H.; Härkönen, P.L. Estrogen and Bone Metabolism. Maturitas 1996, 23, S65–S69. [Google Scholar] [CrossRef] [PubMed]
- Bowring, C.E.; Francis, R.M. National Osteoporosis Society’s Position Statement on Hormone Replacement Therapy in the Prevention and Treatment of Osteoporosis. Menopause Int. 2011, 17, 63–65. [Google Scholar] [CrossRef]
- Collaborative Group on Epidemiological Studies of Ovarian Cancer. Menopausal Hormone Use and Ovarian Cancer Risk: Individual Participant Meta-Analysis of 52 Epidemiological Studies. Lancet 2015, 385, 1835–1842. [Google Scholar] [CrossRef]
- Shi, L.; Wu, Y.; Li, C. Hormone Therapy and Risk of Ovarian Cancer in Postmenopausal Women: A Systematic Review and Meta-Analysis. Menopause 2016, 23, 417–424. [Google Scholar] [CrossRef]
- Greiser, C.M.; Greiser, E.M.; Dören, M. Menopausal Hormone Therapy and Risk of Ovarian Cancer: Systematic Review and Meta-Analysis. Hum. Reprod. Update 2007, 13, 453–463. [Google Scholar] [CrossRef]
- Zhou, B.; Sun, Q.; Cong, R.; Gu, H.; Tang, N.; Yang, L.; Wang, B. Hormone Replacement Therapy and Ovarian Cancer Risk: A Meta-Analysis. Gynecol. Oncol. 2008, 108, 641–651. [Google Scholar] [CrossRef]
- Kimball, J.S.; Johnson, J.P.; Carlson, D.A. Oxidative Stress and Osteoporosis. J. Bone Jt. Surg. 2021, 103, 1451–1461. [Google Scholar] [CrossRef]
- Cramer, J.A.; Amonkar, M.M.; Hebborn, A.; Altman, R. Compliance and Persistence with Bisphosphonate Dosing Regimens among Women with Postmenopausal Osteoporosis. Curr. Med. Res. Opin. 2005, 21, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Delaney, M.F. Strategies for the Prevention and Treatment of Osteoporosis during Early Postmenopause. Am. J. Obstet. Gynecol. 2006, 194, S12–S23. [Google Scholar] [CrossRef] [PubMed]
- Martiniakova, M.; Babikova, M.; Mondockova, V.; Blahova, J.; Kovacova, V.; Omelka, R. The Role of Macronutrients, Micronutrients and Flavonoid Polyphenols in the Prevention and Treatment of Osteoporosis. Nutrients 2022, 14, 523. [Google Scholar] [CrossRef]
- Wu, Q.; Zhou, J. The Application of Polyphenols in Food Preservation. In Advances in Food and Nutrition Research; Elsevier: Amsterdam, The Netherlands, 2021; Volume 98, pp. 35–99. ISBN 978-0-12-822506-6. [Google Scholar]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary Patterns in Relation to Low Bone Mineral Density and Fracture Risk: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 219–236. [Google Scholar] [CrossRef]
- Martiniakova, M.; Babikova, M.; Omelka, B. Pharmacological Agents and Natural Compounds: Available Treatments for Osteoporosis. J. Physiol. Pharmacol. 2020, 71, 307–320. [Google Scholar] [CrossRef]
- Rietjens, I.M.C.M.; Sotoca, A.M.; Vervoort, J.; Louisse, J. Mechanisms Underlying the Dualistic Mode of Action of Major Soy Isoflavones in Relation to Cell Proliferation and Cancer Risks. Mol. Nutr. Food Res. 2013, 57, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Burns, K.A.; Korach, K.S. Estrogen Receptors and Human Disease: An Update. Arch. Toxicol. 2012, 86, 1491–1504. [Google Scholar] [CrossRef]
- Brzozowski, A.M.; Pike, A.C.W.; Dauter, Z.; Hubbard, R.E.; Bonn, T.; Engström, O.; Öhman, L.; Greene, G.L.; Gustafsson, J.-Å.; Carlquist, M. Molecular Basis of Agonism and Antagonism in the Oestrogen Receptor. Nature 1997, 389, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Sampson, J.N.; Falk, R.T.; Schairer, C.; Moore, S.C.; Fuhrman, B.J.; Dallal, C.M.; Bauer, D.C.; Dorgan, J.F.; Shu, X.-O.; Zheng, W.; et al. Association of Estrogen Metabolism with Breast Cancer Risk in Different Cohorts of Postmenopausal Women. Cancer Res. 2017, 77, 918–925. [Google Scholar] [CrossRef]
- Ronis, M.J.J. Effects of Soy Containing Diet and Isoflavones on Cytochrome P450 Enzyme Expression and Activity. Drug Metab. Rev. 2016, 48, 331–341. [Google Scholar] [CrossRef]
- Gupta, M.; McDougal, A.; Safe, S. Estrogenic and Antiestrogenic Activities of 16α- and 2-Hydroxy Metabolites of 17β-Estradiol in MCF-7 and T47D Human Breast Cancer Cells. J. Steroid Biochem. Mol. Biol. 1998, 67, 413–419. [Google Scholar] [CrossRef]
- Klinge, C.M.; Blankenship, K.A.; Risinger, K.E.; Bhatnagar, S.; Noisin, E.L.; Sumanasekera, W.K.; Zhao, L.; Brey, D.M.; Keynton, R.S. Resveratrol and Estradiol Rapidly Activate MAPK Signaling through Estrogen Receptors α and β in Endothelial Cells. J. Biol. Chem. 2005, 280, 7460–7468. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, F.; Zhang, P.; Wang, H.; Qu, Z.; Jia, P.; Yao, Z.; Shen, G.; Li, G.; Zhao, G.; et al. Human Type H Vessels Are a Sensitive Biomarker of Bone Mass. Cell Death Dis 2017, 8, e2760. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; ISBN 978-1-119-53662-8. [Google Scholar]
- Fu, R.; Holmer, H.K. Change Score or Follow-up Score? Choice of Mean Difference Estimates Could Impact Meta-Analysis Conclusions. J. Clin. Epidemiol. 2016, 76, 108–117. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Alekel, D.L.; Germain, A.S.; Peterson, C.T.; Hanson, K.B.; Stewart, J.W.; Toda, T. Isoflavone-Rich Soy Protein Isolate Attenuates Bone Loss in the Lumbar Spine of Perimenopausal Women. Am. J. Clin. Nutr. 2000, 72, 844–852. [Google Scholar] [CrossRef]
- Arcoraci, V.; Atteritano, M.; Squadrito, F.; D’Anna, R.; Marini, H.; Santoro, D.; Minutoli, L.; Messina, S.; Altavilla, D.; Bitto, A. Antiosteoporotic Activity of Genistein Aglycone in Postmenopausal Women: Evidence from a Post-Hoc Analysis of a Multicenter Randomized Controlled Trial. Nutrients 2017, 9, 179. [Google Scholar] [CrossRef]
- Arjmandi, B.H.; Lucas, E.A.; Khalil, D.A.; Devareddy, L.; Smith, B.J.; McDonald, J.; Arquitt, A.B.; Payton, M.E.; Mason, C. One Year Soy Protein Supplementation Has Positive Effects on Bone Formation Markers but Not Bone Density in Postmenopausal Women. Nutr. J. 2005, 4, 8. [Google Scholar] [CrossRef]
- Choquette, S.; Riesco, É.; Cormier, É.; Dion, T.; Aubertin-Leheudre, M.; Dionne, I.J. Effects of Soya Isoflavones and Exercise on Body Composition and Clinical Risk Factors of Cardiovascular Diseases in Overweight Postmenopausal Women: A 6-Month Double-Blind Controlled Trial. Br. J. Nutr. 2011, 105, 1199–1209. [Google Scholar] [CrossRef]
- Gui, J.-C.; Brašić, J.R.; Liu, X.-D.; Gong, G.-Y.; Zhang, G.-M.; Liu, C.-J.; Gao, G.-Q. Bone Mineral Density in Postmenopausal Chinese Women Treated with Calcium Fortification in Soymilk and Cow’s Milk. Osteoporos. Int. 2012, 23, 1563–1570. [Google Scholar] [CrossRef]
- Huang, H.-Y.; Yang, H.-P.; Yang, H.-T.; Yang, T.-C.; Shieh, M.-J.; Huang, S.-Y. One-Year Soy Isoflavone Supplementation Prevents Early Postmenopausal Bone Loss but without a Dose-Dependent Effect. J. Nutr. Biochem. 2006, 17, 509–517. [Google Scholar] [CrossRef]
- Kenny, A.M.; Mangano, K.M.; Abourizk, R.H.; Bruno, R.S.; Anamani, D.E.; Kleppinger, A.; Walsh, S.J.; Prestwood, K.M.; Kerstetter, J.E. Soy Proteins and Isoflavones Affect Bone Mineral Density in Older Women: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2009, 90, 234–242. [Google Scholar] [CrossRef]
- Kreijkamp-Kaspers, S.; Kok, L.; Grobbee, D.E.; De Haan, E.H.F.; Aleman, A.; Lampe, J.W.; Van Der Schouw, Y.T. Effect of Soy Protein Containing Isoflavones on Cognitive Function, Bone Mineral Density, and Plasma Lipids in Postmenopausal Women: A Randomized Controlled Trial. JAMA 2004, 292, 65–74. [Google Scholar] [CrossRef]
- Lydeking–Olsen, E.; Beck-Jensen, J.-E.; Setchell, K.D.R.; Holm–Jensen, T. Soymilk or Progesterone for Prevention of Bone Loss: A 2 Year Randomized, Placebo–Controlled Trial. Eur. J. Nutr. 2004, 43, 246–257. [Google Scholar] [CrossRef]
- Marini, H.; Bitto, A.; Altavilla, D.; Burnett, B.P.; Polito, F.; Di Stefano, V.; Minutoli, L.; Atteritano, M.; Levy, R.M.; D’Anna, R.; et al. Breast Safety and Efficacy of Genistein Aglycone for Postmenopausal Bone Loss: A Follow-Up Study. J. Clin. Endocrinol. Metab. 2008, 93, 4787–4796. [Google Scholar] [CrossRef]
- Mori, M.; Aizawa, T.; Tokoro, M.; Miki, T.; Yamori, Y. Soy Isoflavone Tablets Reduce Osteoporosis Risk Factors and Obesity in Middle-Aged Japanese Women. Clin. Exp. Pharmacol. Physiol. 2004, 31, S39–S41. [Google Scholar] [CrossRef]
- Potter, S.M.; Baum, J.A.; Teng, H.; Stillman, R.J.; Shay, N.F.; Erdman, J.W. Soy Protein and Isoflavones: Their Effects on Blood Lipids and Bone Density in Postmenopausal Women. Am. J. Clin. Nutr. 1998, 68, 1375S–1379S. [Google Scholar] [CrossRef]
- Radhakrish, G.; Rashmi; Agarwal, N.; Vaid, N.B. Evaluation of Isoflavone Rich Soy Protein Supplementation for Ostmenopausal Therapy. Pak. J. Nutr. 2009, 8, 1009–1017. [Google Scholar] [CrossRef]
- Uesugi, T.; Toda, T.; Okuhira, T.; Chen, J. Evidence of Estrogenic Effect by the Three-Month-Intervention of Isoflavone on Vaginal Maturation and Bone Metabolism in Early Postmenopausal Women. Endocr. J. 2003, 50, 613–619. [Google Scholar] [CrossRef][Green Version]
- Valente, M.; Bufalino, L.; Castiglione, G.N.; D’Angelo, R.; Mancuso, A.; Galoppi, P.; Zichella, L. Effects of 1-Year Treatment with Ipriflavone on Bone in Postmenopausal Women with Low Bone Mass. Calcif. Tissue Int. 1994, 54, 377–380. [Google Scholar] [CrossRef]
- Vupadhyayula, P.M.; Gallagher, J.C.; Templin, T.; Logsdon, S.M.; Smith, L.M. Effects of Soy Protein Isolate on Bone Mineral Density and Physical Performance Indices in Postmenopausal Women-a 2-Year Randomized, Double-Blind, Placebo-Controlled Trial. Menopause 2009, 16, 320–328. [Google Scholar] [CrossRef]
- Wong, R.H.; Thaung Zaw, J.J.; Xian, C.J.; Howe, P.R. Regular Supplementation With Resveratrol Improves Bone Mineral Density in Postmenopausal Women: A Randomized, Placebo-Controlled Trial. J. Bone Miner. Res. 2020, 35, 2121–2131. [Google Scholar] [CrossRef]
- Wu, J.; Oka, J.; Ezaki, J.; Ohtomo, T.; Ueno, T.; Uchiyama, S.; Toda, T.; Uehara, M.; Ishimi, Y. Possible Role of Equol Status in the Effects of Isoflavone on Bone and Fat Mass in Postmenopausal Japanese Women: A Double-Blind, Randomized, Controlled Trial. Menopause 2007, 14, 866–874. [Google Scholar] [CrossRef]
- Ye, Y.-B.; Tang, X.-Y.; Verbruggen, M.A.; Su, Y.-X. Soy Isoflavones Attenuate Bone Loss in Early Postmenopausal Chinese Women: A Single-Blind Randomized, Placebo-Controlled Trial. Eur. J. Nutr. 2006, 45, 327–334. [Google Scholar] [CrossRef]
- Zhang, G.; Qin, L.; Shi, Y. Epimedium-Derived Phytoestrogen Flavonoids Exert Beneficial Effect on Preventing Bone Loss in Late Postmenopausal Women: A 24-Month Randomized, Double-Blind and Placebo-Controlled Trial. J. Bone Miner. Res. 2007, 22, 1072–1079. [Google Scholar] [CrossRef]
- Zhang, X.; Li, S.-W.; Wu, J.-F.; Dong, C.-L.; Zheng, C.-X.; Zhang, Y.-P.; Du, J. Effects of Ipriflavone on Postmenopausal Syndrome and Osteoporosis. Gynecol. Endocrinol. 2010, 26, 76–80. [Google Scholar] [CrossRef]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The Effects of Polyphenols and Other Bioactives on Human Health. Food Funct. 2019, 10, 514–528. [Google Scholar] [CrossRef]
- Miyata, Y.; Shida, Y.; Hakariya, T.; Sakai, H. Anti-Cancer Effects of Green Tea Polyphenols Against Prostate Cancer. Molecules 2019, 24, 193. [Google Scholar] [CrossRef]
- Tangney, C.C.; Rasmussen, H.E. Polyphenols, Inflammation, and Cardiovascular Disease. Curr. Atheroscler. Rep. 2013, 15, 324. [Google Scholar] [CrossRef]
- Hanga-Farcaș, A.; Miere, F.; Filip, G.A.; Clichici, S.; Fritea, L.; Vicaș, L.G.; Marian, E.; Pallag, A.; Jurca, T.; Filip, S.M.; et al. Phytochemical Compounds Involved in the Bone Regeneration Process and Their Innovative Administration: A Systematic Review. Plants 2023, 12, 2055. [Google Scholar] [CrossRef]
- Wang, T.; Liu, Q.; Tjhioe, W.; Zhao, J.; Lu, A.; Zhang, G.; Tan, R.X.; Zhou, M.; Xu, J.; Feng, H.T. Therapeutic Potential and Outlook of Alternative Medicine for Osteoporosis. Curr. Drug Targets 2017, 18, 1051–1068. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.-P.; Wu, A.H.; Wang, R.; Ang, L.-W.; Heng, D.; Yuan, J.-M.; Yu, M.C. Gender-Specific Associations Between Soy and Risk of Hip Fracture in the Singapore Chinese Health Study. Am. J. Epidemiol. 2009, 170, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Cai, H.; Gao, Y.; Dai, Q.; Yang, G.; Zheng, W.; Shu, X.-O. Associations of Dietary Intakes of Calcium, Magnesium and Soy Isoflavones with Osteoporotic Fracture Risk in Postmenopausal Women: A Prospective Study. J. Nutr. Sci. 2022, 11, e62. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Cai, H.; Zheng, W.; Shu, X. Associations of Dietary Intakes of Calcium, Magnesium, and Soy Isoflavones With Bone Fracture Risk in Men: A Prospective Study. JBMR Plus 2022, 6, e10563. [Google Scholar] [CrossRef]
- Li, Q.; Yang, G.; Xu, H.; Tang, S.; Lee, W.Y. Effects of Resveratrol Supplementation on Bone Quality: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BMC Complement. Med. Ther. 2021, 21, 214. [Google Scholar] [CrossRef]
- Ma, D.-F.; Qin, L.-Q.; Wang, P.-Y.; Katoh, R. Soy Isoflavone Intake Increases Bone Mineral Density in the Spine of Menopausal Women: Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. 2008, 27, 57–64. [Google Scholar] [CrossRef]
- Bonnick, S.L. Monitoring Changes in Bone Density. Women’s Health 2008, 4, 89–97. [Google Scholar] [CrossRef]
- Choplin, R.H.; Lenchik, L.; Wuertzer, S. A Practical Approach to Interpretation of Dual-Energy X-Ray Absorptiometry (DXA) for Assessment of Bone Density. Curr. Radiol. Rep. 2014, 2, 48. [Google Scholar] [CrossRef]
- Akhlaghi, M.; Ghasemi Nasab, M.; Riasatian, M.; Sadeghi, F. Soy Isoflavones Prevent Bone Resorption and Loss, a Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Rev. Food Sci. Nutr. 2020, 60, 2327–2341. [Google Scholar] [CrossRef]
- Black, D.M.; Bauer, D.C.; Vittinghoff, E.; Lui, L.-Y.; Grauer, A.; Marin, F.; Khosla, S.; De Papp, A.; Mitlak, B.; Cauley, J.A.; et al. Treatment-Related Changes in Bone Mineral Density as a Surrogate Biomarker for Fracture Risk Reduction: Meta-Regression Analyses of Individual Patient Data from Multiple Randomised Controlled Trials. Lancet Diabetes Endocrinol. 2020, 8, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Eastell, R.; Vittinghoff, E.; Lui, L.; McCulloch, C.E.; Pavo, I.; Chines, A.; Khosla, S.; Cauley, J.A.; Mitlak, B.; Bauer, D.C.; et al. Validation of the Surrogate Threshold Effect for Change in Bone Mineral Density as a Surrogate Endpoint for Fracture Outcomes: The FNIH-ASBMR SABRE Project. J. Bone Miner. Res. 2022, 37, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Fatoye, F.; Smith, P.; Gebrye, T.; Yeowell, G. Real-World Persistence and Adherence with Oral Bisphosphonates for Osteoporosis: A Systematic Review. BMJ Open 2019, 9, e027049. [Google Scholar] [CrossRef]
- Tsai, Y.-L.; Wu, C.-H.; Li, C.-C.; Shih, C.-A.; Chang, Y.-F.; Hwang, J.-S.; Tai, T.-W. Drug Adherence and Treatment Duration for Denosumab and Mortality Risk among Hip Fracture Patients. Osteoporos. Int. 2023, 34, 1783–1791. [Google Scholar] [CrossRef]
- Deng, Y.-L.; Hsu, C.-S.; Hsu, C.-Y.; Chen, C.-H.; Ou, S.-F.; Liu, C.-F.; Yang, S.-H.; Shih, C.-H.; Chen, Y.-M.; Lee, H.-T. Predictors for Self-Discontinuation of Anti-Osteoporosis Medication: A Hospital-Based Real-World Study. PLoS ONE 2022, 17, e0275020. [Google Scholar] [CrossRef] [PubMed]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Diab, D.L.; Eldeiry, L.S.; Farooki, A.; Harris, S.T.; Hurley, D.L.; Kelly, J.; Lewiecki, E.M.; et al. American Association of Clinical Endocrinologists/American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis—2020 Update. Endocr. Pract. 2020, 26, 1–46. [Google Scholar] [CrossRef]
- Kanadys, W.; Barańska, A.; Błaszczuk, A.; Polz-Dacewicz, M.; Drop, B.; Malm, M.; Kanecki, K. Effects of Soy Isoflavones on Biochemical Markers of Bone Metabolism in Postmenopausal Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 5346. [Google Scholar] [CrossRef]
- Schyver, T.; Smith, C. Reported Attitudes and Beliefs toward Soy Food Consumption of Soy Consumers versus Nonconsumers in Natural Foods or Mainstream Grocery Stores. J. Nutr. Educ. Behav. 2005, 37, 292–299. [Google Scholar] [CrossRef]
- Duthie, S.J.; Duthie, G.G.; Russell, W.R.; Kyle, J.A.M.; Macdiarmid, J.I.; Rungapamestry, V.; Stephen, S.; Megias-Baeza, C.; Kaniewska, J.J.; Shaw, L.; et al. Effect of Increasing Fruit and Vegetable Intake by Dietary Intervention on Nutritional Biomarkers and Attitudes to Dietary Change: A Randomised Trial. Eur. J. Nutr. 2018, 57, 1855–1872. [Google Scholar] [CrossRef]
- LeBoff, M.S.; Greenspan, S.L.; Insogna, K.L.; Lewiecki, E.M.; Saag, K.G.; Singer, A.J.; Siris, E.S. The Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2022, 33, 2049–2102. [Google Scholar] [CrossRef]
- Pellegrino, R.; Paganelli, R.; Bandinelli, S.; Cherubini, A.; Andrés-Lacueva, C.; Di Iorio, A.; Sparvieri, E.; Zamora-Ros, R.; Ferrucci, L. Urinary and Daily Assumption of Polyphenols and Hip-Fracture Risk: Results from the InCHIANTI Study. Nutrients 2022, 14, 4754. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Country | Sample Size | Mean Age ± SD | Type of Polyphenols | Daily Dose (mg) | Additional Therapy | Type of Control |
|---|---|---|---|---|---|---|---|---|
| Alekel [29] | 2000 | USA | 69 | Poly: 50.2 (median) Ctrl: 50.9 (median) | Soy isoflavones | 80.4 (aglycone) | Oral calcium 160 mg/day | Whey protein diet |
| Arcoraci [30] | 2017 | Italy | 121 | Poly: 54.5 ± 2.9 Ctrl: 54.3 ± 2.4 | Genistein | 54 (aglycone) | 1000 mg calcium carbonate and 800 IU vitamin D3 | Placebo |
| Arjmandi [31] | 2005 | USA | 87 | Poly: 53 ± 6 Ctrl: 56 ± 6 | Soy isoflavones | 60 (isoflavones) | 25 g proteins from soy products | Regular diet |
| Choquette [32] | 2011 | Canada | 100 | Poly: 61 ± 3 Ctrl: 58 ± 6 | Soy isoflavones | 70 (isoflavones) | Exercise | Exercise + placebo |
| Gui [33] | 2012 | China | 100 | Poly: 56.1 ± 4.2 Ctrl: 55.8 ± 4.1 | Soy isoflavones | 3.75–4.5 (isoflavones) | 250 mg calcium | Cowmilk |
| Huang [34] | 2006 | China | 43 | Poly: 51.9 ± 5.8 Ctrl: 51.2 ± 1.5 | Soy isoflavones | 100–200 (isoflavones) | - | Regular diet |
| Kenny [35] | 2009 | USA | 131 | Poly: 73 ± 5.7 Ctrl: 74 ± 6.2 | Soy isoflavones | 105 (aglycone) | Dietary calcium intake of 1200–1500 mg/d ± soy protein | Placebo + soy protein |
| Kreijkamp-Kaspers [36] | 2004 | Netherlands | 202 | Poly: 66.5 ± 4.7 Ctrl: 66.7 ± 4.8 | Soy isoflavones | 99 (aglycone) | Riboflavin. Pyridoxine hydrochloride. Cyanocobalamin. Folic acid. Cholecalciferol. And calcium | Placebo |
| Lydeking-Olsen [37] | 2004 | Denmark | 107 | Poly: 57.8 ± 8.4 Ctrl: 56.3 ± 6.7 | Soy isoflavones | 76 (aglycone) | 1500 mg calcium and 200 UI vitamin D | Placebo |
| Marini [38] | 2008 | Italy | 389 | Poly: 53.8 ± 2.9 Ctrl: 53.5 ± 2 | Genistein | 54 (aglycone) | 1000 mg calcium carbonate and 800 IU vitamin D3 | Placebo |
| Mori [39] | 2004 | Japan | 81 | Poly: 50.1 ± 4.8 Ctrl: 49.4 ± 4.8 | Soy isoflavones | 100 (isoflavones) | - | Placebo |
| Potter [40] | 1998 | USA | 66 | Poly: 59 ± 9.1 Ctrl: 61.3 ± 6.3 | Soy isoflavones | 56–90 (isoflavones) | Calcium phosphate (dosage not available) | Nonfat dry milk |
| Radhakrishnan [41] | 2009 | India | 100 | Poly: 48.07 ± 5.4 Ctrl: 49.71 ± 7.3 | Soy isoflavones | 75 (isoflavones) | 900 mg elemental calcium | Placebo |
| Uesugi [42] | 2003 | Japan | 22 | Poly: 54.9 ± 7.5 Ctrl: 82.5 ± 6.8 | Soy isoflavones | 61.8 (isoflavones) | - | Placebo |
| Valente [43] | 1994 | Italy | 40 | Poly: 55.9 ± 4.2 Ctrl: 56.8 ± 4.5 | Ipriflavone | 600 (ipriflavone) | 1000 mg calcium | Placebo |
| Vupadhyayula [44] | 2009 | USA | 203 | Poly: 63.42 ± 3.1 Ctrl: 63.63 ± 2.5 | Soy isoflavones | 90 (aglycone) | 500 mg calcium and 125 IU vitamin D | Soy protein without isoflavones |
| Wong [45] | 2020 | Australia | 146 | Poly: 64.3 ± 1.3 Ctrl: 65.8 ± 1.3 | Resveratrol | 150 (resveratrol) | - | Placebo |
| Wu [46] | 2007 | Japan | 54 | Poly: 54.5 ± 2 Ctrl: 54.8 ± 2.7 | Soy isoflavones | 75 (isoflavone) 47 (aglycone) | - | Placebo |
| Ye [47] | 2006 | China | 90 | Poly: 52.5 ± 3 Ctrl: 52.7 ± 3.7 | Soy isoflavones | 84–126 (isoflavones) | - | Placebo |
| Zhang [48] | 2007 | China | 100 | Poly: 64 ± 4 Ctrl: 63 ± 3 | EPFs | 78 (aglycone) | 300 mg elemental calcium | Placebo |
| Zhang [49] | 2010 | China | 60 | NA | Ipriflavone | 600 (ipriflavone) | Vitamin AD guttate and 1000 mg compound calcium acid chelate | Placebo and 1000 mg compound calcium acid chelate |
| First Author | Year | Follow-Up (Months) | Drop-Out | Adherence | DXA Scanner |
|---|---|---|---|---|---|
| Alekel [29] | 2000 | 6 | 0% | Excellent | Hologic QDR2000+ |
| Arcoraci [30] | 2017 | 12–24 | NA | Not assessed | Hologic QDR 4500 W |
| Arjmandi [31] | 2005 | 12 | 28.7% | Not assessed | Hologic QDR-4500C |
| Choquette [32] | 2011 | 6 | 21.0% | Not assessed | Ge Lunar Prodigy |
| Gui [33] | 2012 | 6–18 | 14% (6 month) 20% (12 month) 34% (18 month) | Not assessed | Hologic QDR Discovery-W |
| Huang [34] | 2006 | 12 | 2.3% | Not assessed | Lunar DPXL |
| Kenny [35] | 2009 | 12 | 26.0% | 90% | Ge Lunar DPX-IQ |
| Kreijkamp-Kaspers [36] | 2004 | 12 | 24.3% | Good | Hologic QDR1000 |
| Lydeking-Olsen [37] | 2004 | 24 | 11.5% | Not assessed | Norland xR 26 Mark II |
| Marini [38] | 2008 | 24–36 | 21.9% (2 year) 64.5% (3 year) | Not assessed | Hologic QDR4500 W |
| Mori [39] | 2004 | 6 | 13.6% | Not assessed | GE Lunar DPX-NT |
| Potter [40] | 1998 | 6 | NA | Not assessed | Hologic QDR2000 |
| Radhakrishnan [41] | 2009 | 6 | 15.0% | Not assessed | Unspecified |
| Uesugi [42] | 2003 | 3 | 4.5% | Assessed but not reported | GE Lunar DPX-L |
| Valente [43] | 1994 | 12 | 12.5% | Excellent | Hologic QDR 1000 |
| Vupadhyayula [44] | 2009 | 24 | 58.1% | 95% | GE Lunar DPX-L |
| Wong [45] | 2020 | 12 | 12.3% | 94% | GE Lunar (unspecified) |
| Wu [46] | 2007 | 12 | NA | Not assessed | Hologic QDR-4500A |
| Ye [47] | 2006 | 6 | 6.7% | Excellent | Hologic QDR2000+ |
| Zhang [48] | 2007 | 12–24 | 15.0% | Assessed but not reported | GE Lunar DPX-L |
| Zhang [49] | 2010 | 6–12 | 0% | Not assessed | Hologic QDR1000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvio, G.; Ciarloni, A.; Gianfelice, C.; Lacchè, F.; Sabatelli, S.; Giacchetti, G.; Balercia, G. The Effects of Polyphenols on Bone Metabolism in Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Control Trials. Antioxidants 2023, 12, 1830. https://doi.org/10.3390/antiox12101830
Salvio G, Ciarloni A, Gianfelice C, Lacchè F, Sabatelli S, Giacchetti G, Balercia G. The Effects of Polyphenols on Bone Metabolism in Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Control Trials. Antioxidants. 2023; 12(10):1830. https://doi.org/10.3390/antiox12101830
Chicago/Turabian StyleSalvio, Gianmaria, Alessandro Ciarloni, Claudio Gianfelice, Francesca Lacchè, Sofia Sabatelli, Gilberta Giacchetti, and Giancarlo Balercia. 2023. "The Effects of Polyphenols on Bone Metabolism in Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Control Trials" Antioxidants 12, no. 10: 1830. https://doi.org/10.3390/antiox12101830
APA StyleSalvio, G., Ciarloni, A., Gianfelice, C., Lacchè, F., Sabatelli, S., Giacchetti, G., & Balercia, G. (2023). The Effects of Polyphenols on Bone Metabolism in Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Control Trials. Antioxidants, 12(10), 1830. https://doi.org/10.3390/antiox12101830