
Dried Blood Spot Biomarkers of Oxidative Stress and Inflammation Associated with Blood Pressure in Rural Senegalese Women with Incident Hypertension

 ,
,  , and
, and
Abstract
:
1. Introduction
2. Method
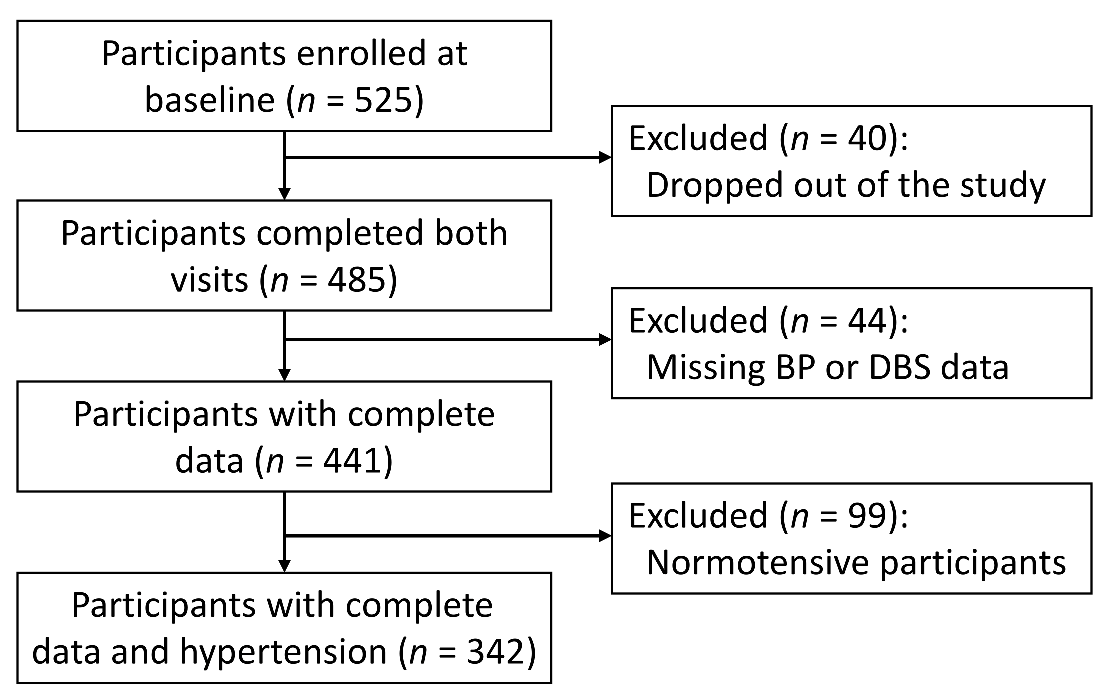
2.1. Study Participants
2.2. BP Measurement
2.3. DBS Analysis
2.4. Statistical Analysis
3. Results
3.1. Demographics of Study Participants
3.2. BP and DBS Biomarkers at Baseline and Follow-Up
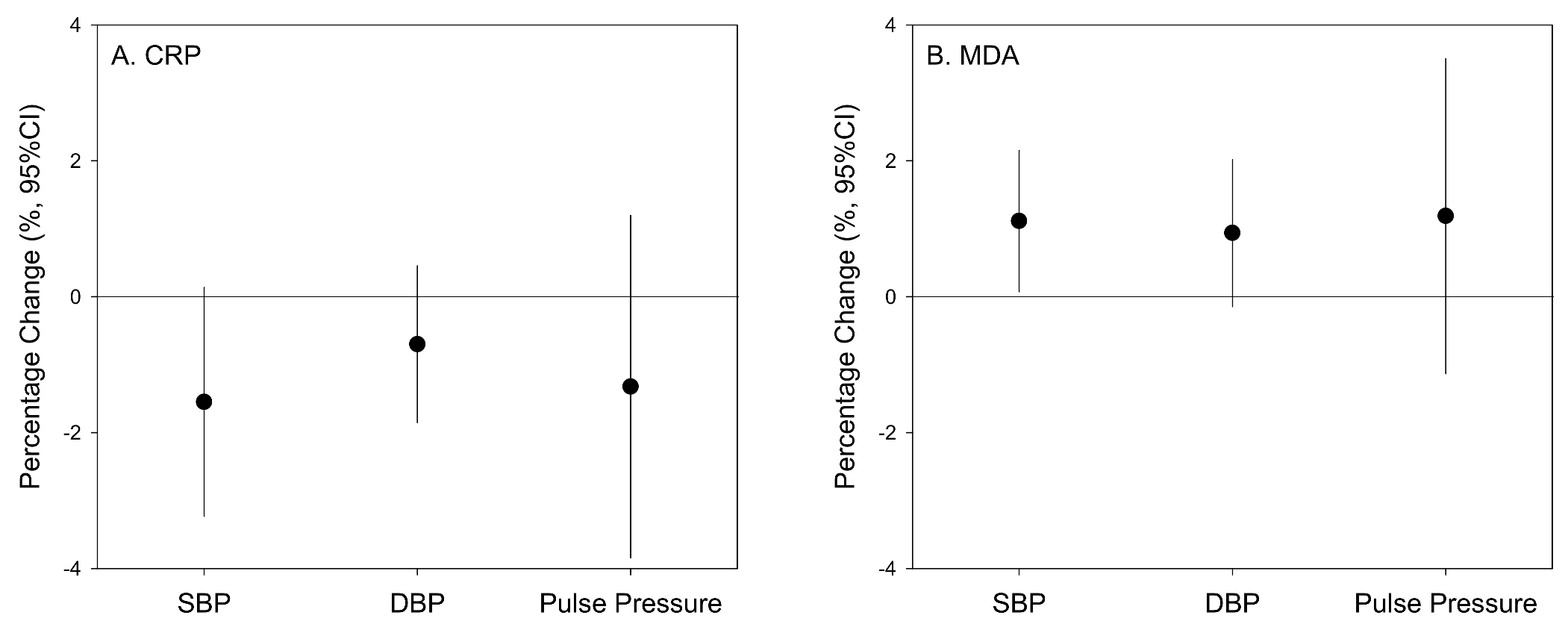
3.3. Associations between BP and DBS Biomarkers
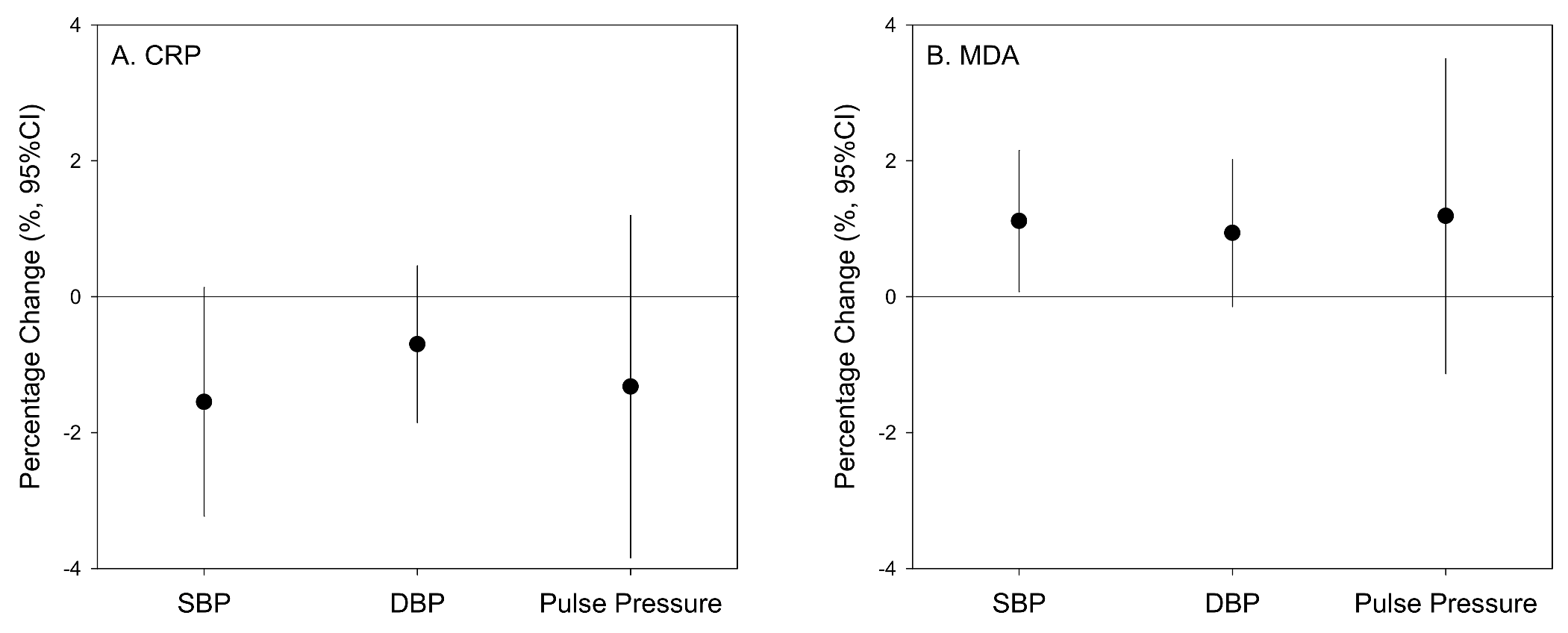
3.4. Associations between Baseline DBS Biomarkers and 1-Year BP Changes
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- Gaziano, T.A. Cardiovascular Disease in the Developing World and Its Cost-Effective Management. Circulation 2005, 112, 3547–3553. [Google Scholar] [CrossRef]
- Thaha, M.; Kadariswantiningsih, I.N.; Empitu, M.A. Association of high blood pressure with elevated oxidative stress, inflammatory marker and albuminuria in chronic kidney disease patients. J. Med. 2019, 20, 12–18. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Sesso, H.D.; Buring, J.E.; Rifai, N.; Blake, G.J.; Gaziano, J.M.; Ridker, P.M. C-Reactive Protein and the Risk of Developing Hyper-tension. J. Am. Med. Assoc. 2003, 290, 2945–2951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakoski, S.G.; Herrington, D.M.; Siscovick, D.M.; Hulley, S.B. C-reactive protein concentration and incident hypertension in young adults: The CARDIA study. Arch. Intern. Med. 2006, 166, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Carbone, F.; Elia, E.; Casula, M.; Bonaventura, A.; Liberale, L.; Bertolotto, M.; Artom, N.; Minetti, S.; Dallegri, F.; Contini, P.; et al. Baseline hs-CRP predicts hypertension re-mission in metabolic syndrome. Eur. J. Clin. Invest. 2019, 49, e13128. [Google Scholar] [CrossRef]
- Lin, Y.; Qiu, X.; Yu, N.; Yang, Q.; Araujo, J.A.; Zhu, Y. Urinary Metabolites of Polycyclic Aromatic Hydrocarbons and the Asso-ciation with Lipid Peroxidation: A Biomarker-Based Study between Los Angeles and Beijing. Environ. Sci. Technol. 2016, 50, 3738–3745. [Google Scholar] [CrossRef]
- Lin, Y.; Ramanathan, G.; Zhu, Y.; Yin, F.; Rea, N.D.; Lu, X.; Tseng, C.H.; Faull, K.F.; Yoon, A.J.; Jerrett, M.; et al. Pro-Oxidative and Proinflammatory Effects after Traveling from Los Angeles to Beijing: A Biomarker-Based Natural Experiment. Circulation 2019, 140, 1995–2004. [Google Scholar] [CrossRef]
- Urso, M.L.; Clarkson, P.M. Oxidative stress, exercise, and antioxidant supplementation. Toxicology 2003, 189, 41–54. [Google Scholar] [CrossRef]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Allen, A.M.; Lundeen, K.; Murphy, S.E.; Spector, L.; Harlow, B.L. Web-Delivered Multimedia Training Materials for the Self-Collection of Dried Blood Spots: A Formative Project. JMIR Form. Res. 2018, 2, e11025. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Wang, X.; Lenz, L.; Ndiaye, O.; Qin, J.; Wang, X.; Huang, H.; Jeuland, M.A.; Zhang, J. (Jim) Malondialdehyde in dried blood spots: A biomarker of systemic lipid peroxidation linked to cardiopulmonary symptoms and risk factors. J. Thorac. Dis. 2021, 13, 3731–3740. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: A report of the American college of cardiology/American Heart Association task. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef]
- Ridker, P.M. C-reactive protein: A simple test to help predict risk of heart attack and stroke. Circulation 2003, 108, e81–e85. [Google Scholar] [CrossRef]
- Chuang, S.-Y.; Hsu, P.-F.; Chang, H.-Y.; Bai, C.-H.; Yeh, W.-T.; Pan, H.-W. C-reactive Protein Predicts Systolic Blood Pressure and Pulse Pressure but not Diastolic Blood Pressure: The Cardiovascular Disease Risk Factors Two-Township Study. Am. J. Hypertens. 2013, 26, 657–664. [Google Scholar] [CrossRef] [Green Version]
- Vongpatanasin, W.; Thomas, G.D.; Schwartz, R.; Cassis, L.A.; Osborne-Lawrence, S.; Hahner, L.; Gibson, L.L.; Black, S.; Samols, D.; Shaul, P.W. C-Reactive Protein Causes Downregulation of Vascular Angiotensin Subtype 2 Receptors and Systolic Hypertension in Mice. Circulation 2007, 115, 1020–1028. [Google Scholar] [CrossRef]
- Li, X.; Yang, G.; Zhao, G.; Wu, B.; Edin, M.L.; Zeldin, D.; Wang, D.W. Rosuvastatin attenuates the elevation in blood pressure induced by overexpression of human C-reactive protein. Hypertens. Res. 2011, 34, 869–875. [Google Scholar] [CrossRef]
- Mahmud, A.; Feely, J. Arterial Stiffness Is Related to Systemic Inflammation in Essential Hypertension. Hypertension 2005, 46, 1118–1122. [Google Scholar] [CrossRef] [Green Version]
- Iwashima, Y.; Horio, T.; Kamide, K.; Rakugi, H.; Ogihara, T.; Kawano, Y. C-Reactive Protein, Left Ventricular Mass Index, and Risk of Cardiovascular Disease in Essential Hypertension. Hypertens. Res. 2007, 30, 1177–1185. [Google Scholar] [CrossRef] [Green Version]
- Idemudia, J.O.; Idogun, E.S. High sensitive C-reactive protein (HsCRP) as a cardiovascular risk factor in hypertensive Nigerans. Niger. Postgrad. Med. J. 2012, 19, 163–166. [Google Scholar]
- Deeg, M.; Baiyewu, O.; Gao, S.; Ogunniyi, A.; Shen, J.; Gureje, O.; Taylor, S.; Murrell, J.; Unverzagt, F.; Smith-Gamble, V.; et al. A comparison of cardiovascular disease risk factor bi-omarkers in African Americans and Yoruba Nigerians. Ethn. Dis. 2008, 18, 427–433. [Google Scholar]
- Lakoski, S.G.; Cushman, M.; Palmas, W.; Blumenthal, R.; D’Agostino, R.B.; Herrington, D.M. The Relationship Between Blood Pressure and C-Reactive Protein in the Multi-Ethnic Study of Atherosclerosis (MESA). J. Am. Coll. Cardiol. 2005, 46, 1869–1874. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Wang, C.H.; Li, S.H.; Dumont, A.S.; Fedak, P.W.; Badiwala, M.V.; Dhillon, B.; Weisel, R.D.; Li, R.K.; Mickle, D.A.; et al. A self-fulfilling prophecy: C-reactive protein attenuates nitric oxide production and inhibits angiogenesis. Circulation 2002, 106, 913–919. [Google Scholar] [CrossRef]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., III; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and car-diovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the centers for disease control and prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Saijo, Y.; Utsugi, M.; Yoshioka, E.; Fukui, T.; Sata, F.; Nakagawa, N.; Hasebe, N.; Yoshida, T.; Kishi, R. Inflammation as a cardiovascular risk factor and pulse wave velocity as a marker of early-stage atherosclerosis in the Japanese population. Environ. Heal. Prev. Med. 2009, 14, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, R.; González, J.; Paoletto, F. The role of oxidative stress in the pathophysiology of hypertension. Hypertens. Res. 2011, 34, 431–440. [Google Scholar] [CrossRef] [Green Version]
- Gkaliagkousi, E.; Gavriilaki, E.; Triantafyllou, A.; Douma, S. Clinical Significance of Endothelial Dysfunction in Essential Hypertension. Curr. Hypertens. Rep. 2015, 17, 1–9. [Google Scholar] [CrossRef]
- Liu, Q.; Gu, X.; Deng, F.; Mu, L.; Baccarelli, A.A.; Guo, X.; Wu, S. Ambient particulate air pollution and circulating C-reactive protein level: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2019, 222, 756–764. [Google Scholar] [CrossRef]
- Li, Z.; Liu, Q.; Xu, Z.; Guo, X.; Wu, S. Association between short-term exposure to ambient particulate air pollution and bi-omarkers of oxidative stress: A meta-analysis. Environ. Res. 2020, 191, 110105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Hypertensive (n = 342) a | Normotensive (n = 99) | p-Value b |
|---|---|---|---|
| Age, years | 33 ± 10 | 28 ± 9 | <0.001 |
| Ethnicity | 0.84 | ||
| Poulard | 82 (24%) | 21 (21%) | |
| Wolof | 246 (72%) | 76 (77%) | |
| Others | 14 (4%) | 2 (2%) | |
| Education | 0.002 | ||
| Religious school | 96 (28%) | 37 (37%) | |
| < Middle school | 234 (68%) | 55 (56%) | |
| Middle or high school | 12 (4%) | 4 (4%) | |
| > High school | 0 (0%) | 3 (3%) | |
| District | 0.40 | ||
| Birkelane (in Kaffrine) | 22 (6%) | 8 (8%) | |
| Kaffrine (in Kaffrine) | 67 (20%) | 24 (24%) | |
| Koungheul (in Kaffrine) | 60 (18%) | 21 (21%) | |
| Dagana (in Saint Louis) | 92 (27%) | 27 (27%) | |
| Podor (in Saint Louis) | 49 (14%) | 11 (11%) | |
| Saint Louis (in Saint Louis) | 52 (15%) | 8 (8%) | |
| Systolic blood pressure, mmHg | 126 ± 19 | 112 ± 9 | <0.001 |
| Diastolic blood pressure, mmHg | 86 ± 12 | 72 ± 5 | <0.001 |
| Pulse pressure, mmHg | 40 ± 14 | 39 ± 9 | 0.53 |
| C-reactive protein, µg/g hemoglobin | 2.1 (1.0–5.0) | 2.2 (0.7–5.9) | 0.80 |
| Malondialdehyde, µg/g hemoglobin | 103 (91–155) | 112 (89–153) | 0.41 |
| Parameter | Visit 2018 | Visit 2019 | Percentage Change (95%CI) b | Spearman’s Q |
|---|---|---|---|---|
| Systolic blood pressure, mmHg | 126 ± 19 a | 115 ± 17 | −9.4 (−10.8, −8.0) | 0.54 c |
| Diastolic blood pressure, mmHg | 86 ± 12 | 78 ± 12 | −9.1 (−10.7, −7.6) | 0.42 c |
| Pulse pressure, mmHg | 40 ± 14 | 36 ± 11 | −9.9 (−13.3, −6.5) | 0.42 c |
| C-reactive protein, µg/g hemoglobin | 2.1 (1.0, 5.0) | 2.8 (1.1, 7.6) | 30 (12, 51) | 0.41 c |
| Malondialdehyde, µg/g hemoglobin | 104 (91, 155) | 59 (45, 83) | −42 (−50, −35) | 0.05 |
| Parameters | CRP Values | Ptrend Value (CRP < 10 mg/L) | Ptrend Value (All Ranges) | |||
|---|---|---|---|---|---|---|
| <1 mg/L (n = 116) | 1–3 mg/L (n = 79) | 3–10 mg/L (n = 89) | >10 mg/L (n = 85) | |||
| Relative ΔSBP (95% CI, mmHg) | ||||||
| Model 1 a | 0.00 (ref) | 2.57 (−2.13, 7.27) | 5.78 (1.24, 10.3) | 2.23 (−2.95, 7.41) | 0.01 | 0.10 |
| Model 2 b | 0.00 (ref) | 2.06 (−2.78, 6.89) | 4.98 (0.38, 9.58) | 1.66 (−3.53, 6.85) | 0.03 | 0.19 |
| Model 3 c | 0.00 (ref) | 2.11 (−2.79, 7.02) | 4.68 (0.01, 9.36) | 2.01 (−3.27, 7.30) | 0.04 | 0.18 |
| Relative ΔDBP (95% CI, mmHg) | ||||||
| Model 1 | 0.00 (ref) | 3.11 (−0.55, 6.77) | 2.63 (−0.91, 6.16) | 3.00 (−1.04, 7.04) | 0.13 | 0.11 |
| Model 2 | 0.00 (ref) | 2.47 (−1.28, 6.22) | 1.97 (−1.60, 5.53) | 2.55 (−1.48, 6.57) | 0.23 | 0.20 |
| Model 3 | 0.00 (ref) | 2.77 (−1.01, 6.54) | 1.86 (−1.73, 5.46) | 3.46 (−0.61, 7.53) | 0.26 | 0.12 |
| Relative ΔPP (95% CI, mmHg) | ||||||
| Model 1 | 0.00 (ref) | 0.54 (−3.14, 4.21) | −3.16 (−6.70, 0.39) | 0.77 (−3.28, 4.82) | 0.10 | 0.59 |
| Model 2 | 0.00 (ref) | 0.41 (−3.43, 4.26) | −3.01 (−6.67, 0.64) | 0.88 (−3.24, 5.01) | 0.12 | 0.68 |
| Model 3 | 0.00 (ref) | 0.65 (−3.22, 4.53) | −2.82 (−6.52, 0.87) | 1.44 (−2.73, 5.62) | 0.16 | 0.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.; Wang, X.; Lenz, L.; Ndiaye, O.; Qin, J.; Wang, X.; Huang, H.; Jeuland, M.A.; Zhang, J. Dried Blood Spot Biomarkers of Oxidative Stress and Inflammation Associated with Blood Pressure in Rural Senegalese Women with Incident Hypertension. Antioxidants 2021, 10, 2026. https://doi.org/10.3390/antiox10122026
Lin Y, Wang X, Lenz L, Ndiaye O, Qin J, Wang X, Huang H, Jeuland MA, Zhang J. Dried Blood Spot Biomarkers of Oxidative Stress and Inflammation Associated with Blood Pressure in Rural Senegalese Women with Incident Hypertension. Antioxidants. 2021; 10(12):2026. https://doi.org/10.3390/antiox10122026
Chicago/Turabian StyleLin, Yan, Xiangtian Wang, Luciane Lenz, Ousmane Ndiaye, Jian Qin, Xiaoli Wang, Hui Huang, Marc A. Jeuland, and Junfeng Zhang. 2021. "Dried Blood Spot Biomarkers of Oxidative Stress and Inflammation Associated with Blood Pressure in Rural Senegalese Women with Incident Hypertension" Antioxidants 10, no. 12: 2026. https://doi.org/10.3390/antiox10122026
APA StyleLin, Y., Wang, X., Lenz, L., Ndiaye, O., Qin, J., Wang, X., Huang, H., Jeuland, M. A., & Zhang, J. (2021). Dried Blood Spot Biomarkers of Oxidative Stress and Inflammation Associated with Blood Pressure in Rural Senegalese Women with Incident Hypertension. Antioxidants, 10(12), 2026. https://doi.org/10.3390/antiox10122026