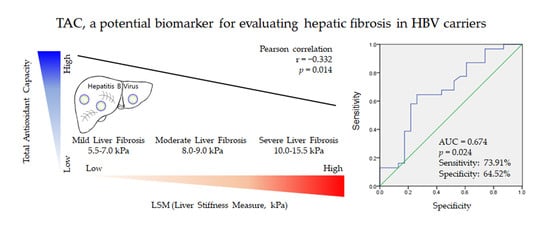
Total Antioxidant Capacity in HBV Carriers, a Promising Biomarker for Evaluating Hepatic Fibrosis: A Pilot Study




Abstract
1. Introduction
2. Subjects and Methods
2.1. Subjects and Study Design
2.2. Liver Stiffness Measurement by FibroScan
2.3. Complete Blood Count, Fasting Blood Glucose, and Serum Biochemical Analysis
2.4. Serum Lipid Peroxide Determination
2.5. Serum Total Reactive Oxygen Species Determination
2.6. Serum Superoxide Dismutase Determination
2.7. Serum Catalase Determination
2.8. Serum Total Glutathione Content, Glutathione Peroxidase, and Glutathione Reductase Activity Determination
2.9. Serum Total Antioxidant Capacity Assay
2.10. Statistical Analysis
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Inoue, T.; Tanaka, Y. The Role of Hepatitis B Core-Related Antigen. Genes 2019, 10, 357. [Google Scholar] [CrossRef]
- Nelson, N.P.; Easterbrook, P.J.; McMahon, B.J. Epidemiology of Hepatitis B Virus Infection and Impact of Vaccination on Disease. Clin. Liver Dis. 2016, 20, 607–628. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Subic, M.; Zoulim, F. How to improve access to therapy in hepatitis B patients. Liver Int. 2018, 38 (Suppl. 1), 115–121. [Google Scholar] [CrossRef]
- Altamirano-Barrera, A.; Barranco-Fragoso, B.; Mendez-Sanchez, N. Management strategies for liver fibrosis. Ann. Hepatol. 2017, 16, 48–56. [Google Scholar] [CrossRef]
- Hsiao, C.Y.; Teng, X.; Su, T.H.; Lee, P.H.; Kao, J.H.; Huang, K.W. Improved quantitative assessment of HBV-associated liver fibrosis using second-harmonic generation microscopy with feature selection. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 12–20. [Google Scholar] [CrossRef]
- Barcena Marugan, R.; Garcia Garzon, S. DNA-guided hepatitis B treatment, viral load is essential, but not sufficient. World J. Gastroenterol. 2009, 15, 423–430. [Google Scholar] [CrossRef]
- Li, S.; Hong, M.; Tan, H.Y.; Wang, N.; Feng, Y. Insights into the Role and Interdependence of Oxidative Stress and Inflammation in Liver Diseases. Oxidative Med. Cell. Longev. 2016, 2016, 4234061. [Google Scholar] [CrossRef]
- Luangmonkong, T.; Suriguga, S.; Mutsaers, H.A.M.; Groothuis, G.M.M.; Olinga, P.; Boersema, M. Targeting Oxidative Stress for the Treatment of Liver Fibrosis. Rev. Physiol. Biochem. Pharmacol. 2018, 175, 71–102. [Google Scholar] [CrossRef]
- Sies, H. Oxidative stress: From basic research to clinical application. Am. J. Med. 1991, 91, 31S–38S. [Google Scholar] [CrossRef]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxidative Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Chan, T.C.; Wilkinson Berka, J.L.; Deliyanti, D.; Hunter, D.; Fung, A.; Liew, G.; White, A. The role of reactive oxygen species in the pathogenesis and treatment of retinal diseases. Exp. Eye Res. 2020, 201, 108255. [Google Scholar] [CrossRef]
- Vranova, E.; Inze, D.; Van Breusegem, F. Signal transduction during oxidative stress. J. Exp. Bot. 2002, 53, 1227–1236. [Google Scholar] [CrossRef]
- Singal, A.K.; Jampana, S.C.; Weinman, S.A. Antioxidants as therapeutic agents for liver disease. Liver Int. 2011, 31, 1432–1448. [Google Scholar] [CrossRef]
- Gong, Y.; Yang, Y. Activation of Nrf2/AREs-mediated antioxidant signalling, and suppression of profibrotic TGF-beta1/Smad3 pathway: A promising therapeutic strategy for hepatic fibrosis—A review. Life Sci. 2020, 256, 117909. [Google Scholar] [CrossRef]
- Wong, G.L. Non-invasive assessments for liver fibrosis: The crystal ball we long for. J. Gastroenterol. Hepatol. 2018, 33, 1009–1015. [Google Scholar] [CrossRef]
- Afdhal, N.H. Fibroscan (transient elastography) for the measurement of liver fibrosis. Gastroenterol. Hepatol. 2012, 8, 605–607. [Google Scholar]
- Yen, Y.H.; Kuo, F.Y.; Kee, K.M.; Chang, K.C.; Tsai, M.C.; Hu, T.H.; Lu, S.N.; Wang, J.H.; Hung, C.H.; Chen, C.H. APRI and FIB-4 in the evaluation of liver fibrosis in chronic hepatitis C patients stratified by AST level. PLoS ONE 2018, 13, e0199760. [Google Scholar] [CrossRef]
- Gudowska, M.; Gruszewska, E.; Panasiuk, A.; Cylwik, B.; Flisiak, R.; Swiderska, M.; Szmitkowski, M.; Chrostek, L. Hyaluronic acid concentration in liver diseases. Clin. Exp. Med. 2016, 16, 523–528. [Google Scholar] [CrossRef]
- Loaeza-del-Castillo, A.; Paz-Pineda, F.; Oviedo-Cardenas, E.; Sanchez-Avila, F.; Vargas-Vorackova, F. AST to platelet ratio index (APRI) for the noninvasive evaluation of liver fibrosis. Ann. Hepatol. 2008, 7, 350–357. [Google Scholar] [CrossRef]
- Alavian, S.M.; Showraki, A. Hepatitis B and its Relationship with Oxidative Stress. Hepat. Mon. 2016, 16, e37973. [Google Scholar] [CrossRef]
- Tapper, E.B.; Castera, L.; Afdhal, N.H. FibroScan (vibration-controlled transient elastography): Where does it stand in the United States practice. Clin. Gastroenterol. Hepatol. 2015, 13, 27–36. [Google Scholar] [CrossRef]
- Satoh, K. Serum lipid peroxide in cerebrovascular disorders determined by a new colorimetric method. Clin. Chim. Acta 1978, 90, 37–43. [Google Scholar] [CrossRef]
- Shankar, K.; Mehendale, H.M. Oxidative Stress. In Encyclopedia of Toxicology, 3rd ed.; Wexler, P., Ed.; Academic Press: Oxford, UK, 2014; pp. 735–737. [Google Scholar] [CrossRef]
- Hayashi, I.; Morishita, Y.; Imai, K.; Nakamura, M.; Nakachi, K.; Hayashi, T. High-throughput spectrophotometric assay of reactive oxygen species in serum. Mutat. Res. 2007, 631, 55–61. [Google Scholar] [CrossRef]
- Wheeler, C.R.; Salzman, J.A.; Elsayed, N.M.; Omaye, S.T.; Korte, D.W., Jr. Automated assays for superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase activity. Anal. Biochem. 1990, 184, 193–199. [Google Scholar] [CrossRef]
- Kambayashi, Y.; Binh, N.T.; Asakura, H.W.; Hibino, Y.; Hitomi, Y.; Nakamura, H.; Ogino, K. Efficient assay for total antioxidant capacity in human plasma using a 96-well microplate. J. Clin. Biochem. Nutr. 2009, 44, 46–51. [Google Scholar] [CrossRef]
- Zhang, Z.Q.; Shi, B.S.; Lu, W.; Liu, D.P.; Huang, D.; Feng, Y.L. Quantitative HBcrAg and HBcAb versus HBsAg and HBV DNA in predicting liver fibrosis levels of chronic hepatitis B patients. Gastroenterol. Hepatol. 2020, 43, 526–536. [Google Scholar] [CrossRef]
- Parikh, P.; Ryan, J.D.; Tsochatzis, E.A. Fibrosis assessment in patients with chronic hepatitis B virus (HBV) infection. Ann. Transl. Med. 2017, 5, 40. [Google Scholar] [CrossRef]
- Lin, L.; Zhou, F.; Shen, S.; Zhang, T. Fighting Liver Fibrosis with Naturally Occurring Antioxidants. Planta Med. 2018, 84, 1318–1333. [Google Scholar] [CrossRef]
- Sanchez-Valle, V.; Chavez-Tapia, N.C.; Uribe, M.; Mendez-Sanchez, N. Role of oxidative stress and molecular changes in liver fibrosis: A review. Curr. Med. Chem. 2012, 19, 4850–4860. [Google Scholar] [CrossRef]
- Gomez-Dominguez, E.; Mendoza, J.; Rubio, S.; Moreno-Monteagudo, J.A.; Garcia-Buey, L.; Moreno-Otero, R. Transient elastography: A valid alternative to biopsy in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2006, 24, 513–518. [Google Scholar] [CrossRef]
- Fung, J.; Lee, C.K.; Chan, M.; Seto, W.K.; Wong, D.K.; Lai, C.L.; Yuen, M.F. Defining normal liver stiffness range in a normal healthy Chinese population without liver disease. PLoS ONE 2013, 8, e85067. [Google Scholar] [CrossRef]
- Linden, A. Measuring diagnostic and predictive accuracy in disease management: An introduction to receiver operating characteristic (ROC) analysis. J. Eval. Clin. Pract. 2006, 12, 132–139. [Google Scholar] [CrossRef]
- Yang, J.; Xiong, Y.; Zhou, L.; Huang, Y.; Chen, W.; Wang, B. Soluble E-cadherin is associated with oxidative stress in patients with chronic HBV infection. J. Med. Virol. 2020, 92, 34–44. [Google Scholar] [CrossRef]
- Duygu, F.; Karsen, H.; Aksoy, N.; Taskin, A. Relationship of oxidative stress in hepatitis B infection activity with HBV DNA and fibrosis. Ann. Lab. Med. 2012, 32, 113–118. [Google Scholar] [CrossRef]
- Rubio, C.P.; Hernandez-Ruiz, J.; Martinez-Subiela, S.; Tvarijonaviciute, A.; Ceron, J.J. Spectrophotometric assays for total antioxidant capacity (TAC) in dog serum: An update. BMC Vet. Res. 2016, 12, 166. [Google Scholar] [CrossRef]
- Sies, H. Total antioxidant capacity: Appraisal of a concept. J. Nutr. 2007, 137, 1493–1495. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Bernardi, M.; Maggioli, C.; Zaccherini, G. Human albumin in the management of complications of liver cirrhosis. Crit. Care 2012, 16, 211. [Google Scholar] [CrossRef]
- Jang, T.Y.; Yeh, M.L.; Huang, C.I.; Lin, Z.Y.; Chen, S.C.; Hsieh, M.H.; Dai, C.Y.; Huang, J.F.; Huang, C.F.; Chuang, W.L.; et al. Association of hyperuricemia with disease severity in chronic hepatitis C patients. PLoS ONE 2018, 13, e0207043. [Google Scholar] [CrossRef]
- Plantier, J.L.; Duretz, V.; Devos, V.; Urbain, R.; Jorieux, S. Comparison of antioxidant properties of different therapeutic albumin preparations. Biologicals 2016, 44, 226–233. [Google Scholar] [CrossRef]
- Oliveira, V.O.; Oliveira, J.P.; Franca, E.V.; Brito, H.L.; Nascimento, T.V.; Franca, A. Advanced liver injury in patients with chronic hepatitis b and viral load below 2000 IU/mL. Rev. Inst. Med. Trop. Sao Paulo 2016, 58, 65. [Google Scholar] [CrossRef][Green Version]
- Tong, M.J.; Pan, C.Q.; Hann, H.W.; Kowdley, K.V.; Han, S.H.; Min, A.D.; Leduc, T.S. The management of chronic hepatitis B in Asian Americans. Dig. Dis. Sci. 2011, 56, 3143–3162. [Google Scholar] [CrossRef]
- Ijaz, B.; Ahmad, W.; Javed, F.T.; Gull, S.; Hassan, S. Revised cutoff values of ALT and HBV DNA level can better differentiate HBeAg (-) chronic inactive HBV patients from active carriers. Virol. J. 2011, 8, 86. [Google Scholar] [CrossRef]
- Proskurnina, E.V.; Izmailov, D.Y.; Sozarukova, M.M.; Zhuravleva, T.A.; Leneva, I.A.; Poromov, A.A. Antioxidant Potential of Antiviral Drug Umifenovir. Molecules 2020, 25, 1577. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Male | Female | Total |
|---|---|---|---|
| Subject number | 44 | 10 | 54 |
| Median age (year, range) | 51 (36–66) | 54 (45–65) | 52 (36–66) |
| Average height (cm, range) | 170 (158–180) | 159 (155–174) | 168 (155–180) |
| Average weight (kg, range) | 69.5 (49.6–87.0) | 57.5 (43.0–70.9) | 67 (43.0–87.0) |
| Mean BMI (value, range) | 24.0 (18.4–29.4) | 22.8 (18.1–27.2) | 23.8 (18.1–29.4) |
| Antiviral drug +/− | 27/17 | 8/2 | 35/19 |
| HBV DNA viral load (IU/mL, n) | <2000, 29; >2000, 15 | <2000, 6; >2000, 4 | <2000, 34; >2000, 20 |
| Blood/Serum parameters | |||
| Average AST (U/L) | 31 (15–83) | 30 (19–60) | 31 (15–83) |
| Average ALT (U/L) | 34 (16–166) | 29 (14–68) | 33 (14–166) |
| Average GGT (U/L) | 37 (11–208) | 18 (8–37) | 34 (8–208) |
| Mean Platelets (1010/L) | 18.1 (8.0–36.4) | 13.0 (8.3–19.1) | 17.2 (8.0–36.4) |
| Average FBG (mg/dL) | 103 (81–149) | 100 (72–122) | 103 (72–149) |
| Liver fibrotic biomarkers | |||
| Average LSM (kPa, range) | 8.6 (5.5–15.5) | 7.7 (5.6–10.1) | 8.4 (5.5–15.5) |
| Mean APRI (value, range) | 0.46 (0.15–1.0) | 0.64 (0.28–1.44) | 0.49 (0.15–1.44) |
| Mean FIB-4 (score, range) | 1.71 (0.74–5.2) | 2.65 (1.16–4.69) | 1.89 (0.74–5.2) |
| Mean HA (ng/mL, range) | 44 (2–338) | 51 (4–145) | 45 (2–338) |
| Measurements | Mild Hepatic Fibrosis | Moderate/Severe Hepatic Fibrosis | t-Test | ||||
|---|---|---|---|---|---|---|---|
| LSM < 8.5 kPa | LSM > 8.5 kPa | ||||||
| Total 31 (M/F:23/8) | Total 23 (M/F:21/2) | p Value | |||||
| Mean | SD | Mean | SD | ||||
| LSM (kPa) | 6.7 | ± | 0.9 | 10.8 | ± | 1.8 | 0.00 |
| TAC (μM/mL) | 511.5 | ± | 144.4 | 406.8 | ± | 143.5 | 0.01 |
| MDA (μM/mL) | 77.5 | ± | 40.2 | 79.4 | ± | 52.7 | 0.89 |
| ROS (U/mL) | 23.7 | ± | 5.1 | 23.4 | ± | 6.6 | 0.84 |
| SOD (U/mL) | 6.1 | ± | 3.4 | 6.0 | ± | 2.7 | 0.90 |
| Catalase (U/mL) | 5.9 | ± | 2.7 | 4.9 | ± | 2.1 | 0.13 |
| GSH (μM/mL) | 2.4 | ± | 1.3 | 2.1 | ± | 0.9 | 0.29 |
| GPx (U/mL) | 100.8 | ± | 50.9 | 88.8 | ± | 33.0 | 0.30 |
| GRed (U/mL) | 49.8 | ± | 17.2 | 50.1 | ± | 25.8 | 0.96 |
| APRI | 0.4 | ± | 0.2 | 0.6 | ± | 0.3 | 0.03 |
| FIB-4 | 1.7 | ± | 0.9 | 2.2 | ± | 1.1 | 0.09 |
| HA (ng/mL) | 41.9 | ± | 34.5 | 49.6 | ± | 70.2 | 0.63 |
| TGF-β1 (ng/mL) | 1.3 | ± | 1.1 | 1.5 | ± | 0.9 | 0.47 |
| PDGF (ng/mL) | 0.6 | ± | 0.5 | 0.5 | ± | 0.4 | 0.71 |
| Platelets (1010/L) | 18.8 | ± | 6.6 | 14.9 | ± | 4.5 | 0.01 |
| Albumin (g/dL) | 4.47 | ± | 0.22 | 4.54 | ± | 0.18 | 0.20 |
| Uric acid (mg/dL) | 2.85 | ± | 0.89 | 3.03 | ± | 0.93 | 0.47 |
| AST (U/L) | 29.2 | ± | 10.6 | 32.3 | ± | 14.4 | 0.40 |
| ALT (U/L) | 31.3 | ± | 15.4 | 35.4 | ± | 31.1 | 0.57 |
| FBG (mg/dL) | 101.2 | ± | 13.1 | 104.5 | ± | 17.0 | 0.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.-H.; Lee, S.-B.; Lee, D.-S.; Son, C.-G. Total Antioxidant Capacity in HBV Carriers, a Promising Biomarker for Evaluating Hepatic Fibrosis: A Pilot Study. Antioxidants 2021, 10, 77. https://doi.org/10.3390/antiox10010077
Wang J-H, Lee S-B, Lee D-S, Son C-G. Total Antioxidant Capacity in HBV Carriers, a Promising Biomarker for Evaluating Hepatic Fibrosis: A Pilot Study. Antioxidants. 2021; 10(1):77. https://doi.org/10.3390/antiox10010077
Chicago/Turabian StyleWang, Jing-Hua, Sung-Bae Lee, Dong-Soo Lee, and Chang-Gue Son. 2021. "Total Antioxidant Capacity in HBV Carriers, a Promising Biomarker for Evaluating Hepatic Fibrosis: A Pilot Study" Antioxidants 10, no. 1: 77. https://doi.org/10.3390/antiox10010077
APA StyleWang, J.-H., Lee, S.-B., Lee, D.-S., & Son, C.-G. (2021). Total Antioxidant Capacity in HBV Carriers, a Promising Biomarker for Evaluating Hepatic Fibrosis: A Pilot Study. Antioxidants, 10(1), 77. https://doi.org/10.3390/antiox10010077