Higher Serum Melatonin Levels during the First Week of Malignant Middle Cerebral Artery Infarction in Non-Surviving Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Subjects
2.2. Determinations of Serum Melatonin Levels
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Sainz, R.M.; Lopez-Burillo, S.; Mayo, J.C.; Manchester, L.C.; Tan, D.X. Melatonin ameliorates neurologic damage and neurophysiologic deficits in experimental models of stroke. Ann. N. Y. Acad. Sci. 2003, 993, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Esposito, E.; Cuzzocrea, S. Antiinflammatory activity of melatonin in central nervous system. Curr. Neuropharmacol. 2010, 8, 228–242. [Google Scholar] [CrossRef] [PubMed]
- Andrabi, S.S.; Parvez, S.; Tabassum, H. Melatonin and Ischemic Stroke: Mechanistic Roles and Action. Adv. Pharmacol. Sci. 2015, 2015, 384750. [Google Scholar] [CrossRef]
- Paterniti, I.; Cordaro, M.; Esposito, E.; Cuzzocrea, S. The antioxidative property of melatonin against brain ischemia. Expert Rev. Neurother. 2016, 16, 841–848. [Google Scholar] [CrossRef]
- Ramos, E.; Patiño, P.; Reiter, R.J.; Gil-Martín, E.; Marco-Contelles, J.; Parada, E.; de Los Rios, C.; Romero, A.; Egea, J. Ischemic brain injury: New insights on the protective role of melatonin. Free Radic. Biol. Med. 2017, 104, 32–53. [Google Scholar] [CrossRef]
- Atanassova, P.A.; Terzieva, D.D.; Dimitrov, B.D. Impaired nocturnal melatonin in acute phase of ischaemic stroke: Cross-sectional matched case-control analysis. J. Neuroendocrinol. 2009, 21, 657–663. [Google Scholar] [CrossRef]
- Adamczak-Ratajczak, A.; Kupsz, J.; Owecki, M.; Zielonka, D.; Sowinska, A.; Checinska-Maciejewska, Z.; Krauss, H.; Michalak, S.; Gibas-Dorna, M. Circadian rhythms of melatonin and cortisol in manifest Huntington’s disease and in acute cortical ischemic stroke. J. Physiol. Pharmacol. 2017, 68, 539–546. [Google Scholar]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Pérez-Cejas, A.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Cáceres, J.J.; Jiménez, A.; García-Marín, V. Serum melatonin levels are associated with mortality in patients with malignant middle cerebral artery infarction. J. Int. Med. Res. 2018, 46, 3268–3277. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Pérez-Cejas, A.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Cáceres, J.J.; Jiménez, A.; García-Marín, V. Serum melatonin levels in survivor and non-survivor patients with traumatic brain injury. BMC Neurol. 2017, 17, 138. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Cáceres, J.J.; Jiménez, A.; García-Marín, V. The Serum Melatonin Levels and Mortality of Patients with Spontaneous Intracerebral Hemorrhage. Brain Sci. 2019, 9, E263. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessement of coma and impaired conciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; del Zoppo, G.; Alberts, M.J.; Bhatt, D.L.; Brass, L.; Furlan, A.; Grubb, R.L.; Higashida, R.T.; Jauch, E.C.; Kidwell, C.; et al. Guidelines for the early management of adults with ischemic stroke: A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007, 38, 1655–1711. [Google Scholar]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Riaño-Ruiz, M.; Jiménez, A. Serum malondialdehyde levels in patients with malignant middle cerebral artery infarction are associated with mortality. PLoS ONE 2015, 10, e0125893. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Sabatel, R.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Cáceres, J.J.; Jiménez, A.; García-Marín, V. Non-survivor patients with malignant middle cerebral artery infarction showed persistently high serum malondialdehyde levels. BMC Neurol. 2019, 19, 238. [Google Scholar] [CrossRef]
- Draper, H.H.; Hadley, M. Malondialdehyde determination as index of lipid peroxidation. Methods Enzymol. 1990, 186, 421431. [Google Scholar]
- Dalle-Donne, I.; Rossi, R.; Colombo, R.; Giustarini, D.; Milzani, A. Biomarkers of oxidative damage in human disease. Clin. Chem. 2006, 52, 601–623. [Google Scholar] [CrossRef]
- Cuzzocrea, S.; Costantino, G.; Gitto, E.; Mazzon, E.; Fulia, F.; Serraino, I.; Cordaro, S.; Barberi, I.; De Sarro, A.; Caputi, A.P. Protective effects of melatonin in ischemic brain injury. J. Pineal Res. 2000, 29, 217–227. [Google Scholar] [CrossRef]
- Koh, P.O. Melatonin attenuates the cerebral ischemic injury via the MEK/ERK/p90RSK/bad signaling cascade. J. Vet. Med. Sci. 2008, 70, 1219–1223. [Google Scholar] [CrossRef]
- Tai, S.H.; Hung, Y.C.; Lee, E.J.; Lee, A.C.; Chen, T.Y.; Shen, C.C.; Chen, H.Y.; Lee, M.Y.; Huang, S.Y.; Wu, T.S. Melatonin protects against transient focal cerebral ischemia in both reproductively active and estrogen-deficient female rats: The impact of circulating estrogen on its hormetic dose-response. J. Pineal Res. 2011, 50, 292–303. [Google Scholar] [CrossRef] [PubMed]
- Koh, P.O. Melatonin regulates the calcium-buffering proteins, parvalbumin and hippocalcin, in ischemic brain injury. J. Pineal Res. 2012, 53, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Balduini, W.; Carloni, S.; Perrone, S.; Bertrando, S.; Tataranno, M.L.; Negro, S.; Proietti, F.; Longini, M.; Buonocore, G. The use of melatonin in hypoxic-ischemic brain damage: An experimental study. J. Matern. Fetal Neonatal Med. 2012, 25, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Feng, Q.; Ma, J.; Feng, Z.; Zhan, M.; Ouyang, L.; Mu, S.; Liu, B.; Jiang, Z.; Jia, Y.; et al. Melatonin ameliorates injury and specific responses of ischemic striatal neurons in rats. J. Histochem. Cytochem. 2013, 61, 591–605. [Google Scholar] [CrossRef]
- Li, H.; Wang, Y.; Feng, D.; Liu, Y.; Xu, M.; Gao, A.; Tian, F.; Zhang, L.; Cui, Y.; Wang, Z.; et al. Alterations in the time course of expression of the Nox family in the brain in a rat experimental cerebral ischemia and reperfusion model: Effects of melatonin. J. Pineal Res. 2014, 57, 110–119. [Google Scholar] [CrossRef]
- Bhattacharya, P.; Pandey, A.K.; Paul, S.; Patnaik, R. Melatonin renders by protein kinase C mediated aquaporin-4 inhibition in animal model of focal cerebral ischemia. Life Sci. 2014, 100, 97–109. [Google Scholar] [CrossRef]
- Yang, Y.; Jiang, S.; Dong, Y.; Fan, C.; Zhao, L.; Yang, X.; Li, J.; Di, S.; Yue, L.; Liang, G.; et al. Melatonin prevents cell death and mitochondrial dysfunction via a SIRT1-dependent mechanism during ischemic-stroke in mice. J. Pineal Res. 2015, 58, 61–70. [Google Scholar] [CrossRef]
- Paredes, S.D.; Rancan, L.; Kireev, R.; González, A.; Louzao, P.; González, P.; Rodríguez-Bobada, C.; García, C.; Vara, E.; Tresguerres, J.A. Melatonin Counteracts at a Transcriptional Level the Inflammatory and Apoptotic Response Secondary to Ischemic Brain Injury Induced by Middle Cerebral Artery Blockade in Aging Rats. BioRes. Open Access 2015, 4, 407–416. [Google Scholar] [CrossRef]
- Feng, D.; Wang, B.; Wang, L.; Abraham, N.; Tao, K.; Huang, L.; Shi, W.; Dong, Y.; Qu, Y. Pre-ischemia melatonin treatment alleviated acute neuronal injury after ischemic stroke by inhibiting endoplasmic reticulum stress-dependent autophagy via PERK and IRE1 signalings. J. Pineal Res. 2017, 62, 3. [Google Scholar] [CrossRef]
- Blanco, S.; Hernández, R.; Franchelli, G.; Ramos-Álvarez, M.M.; Peinado, M.ÁÁ. Melatonin influences NO/NOS pathway and reduces oxidative and nitrosative stress in a model of hypoxic-ischemic brain damage. Nitric Oxide 2017, 62, 32–43. [Google Scholar] [CrossRef]
- Lin, Y.W.; Chen, T.Y.; Hung, C.Y.; Tai, S.H.; Huang, S.Y.; Chang, C.C.; Hung, H.Y.; Lee, E.J. Melatonin protects brain against ischemia/reperfusion injury by attenuating endoplasmic reticulum stress. Int. J. Mol. Med. 2018, 42, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, H.; Chen, W.; Chen, L.; Liu, D.; Wang, X.; Wang, X. Melatonin attenuates white matter damage after focal brain ischemia in rats by regulating the TLR4/NF-κB pathway. Brain Res. Bull. 2019, 150, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Kryl’skii, E.D.; Popova, T.N.; Safonova, O.A.; Stolyarova, A.O.; Razuvaev, G.A.; de Carvalho, M.A.P. Transcriptional Regulation of Antioxidant Enzymes Activity and Modulation of Oxidative Stress by Melatonin in Rats under Cerebral Ischemia / Reperfusion Conditions. Neuroscience 2019, 406, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Lu, C.; Li, T.; Wang, W.; Ye, W.; Zeng, R.; Ni, L.; Lai, Z.; Wang, X.; Liu, C. The protective effect of melatonin on brain ischemia and reperfusion in rats and humans: In vivo assessment and a randomized controlled trial. J. Pineal Res. 2018, 65, e12521. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Non-Survivors (n = 34) | Survivors (n = 34) | p-Value | |
|---|---|---|---|
| Gender female-n (%) | 13 (38.2) | 14 (41.2) | 0.99 |
| Arterial hypertension-n (%) | 16 (47.1) | 19 (55.9) | 0.63 |
| Diabetes mellitus-n (%) | 9 (26.5) | 4 (11.8) | 0.22 |
| Age (years)-m (p 25–75) | 63 (53–70) | 59 (47–68) | 0.36 |
| GCS score-m (p 25–75) | 6 (3–7) | 7 (6–8) | 0.01 |
| Thrombolysis-n (%) | 10 (29.4) | 11 (32.4) | 0.99 |
| Volumen infarction (mL)-m (p 25–75) | 180 (60–277) | 173 (100–231) | 0.64 |
| Midline shift (mm)-m (p 25–75) | 9.0 (3.5–15.0) | 6.0 (2.5–11.5) | 0.43 |
| Hemorrhagic transformation-n (%) | 6 (17.6) | 7 (20.6) | 0.99 |
| Lactic acid (mmol/L)-m (p 25–75) | 1.55 (1.00–2.70) | 1.20 (0.90–1.70) | 0.05 |
| Sodium (mEq/L)-m (p 25–75) | 140 (139–145) | 139 (136–145) | 0.38 |
| Bilirubin (mg/dL)-m (p 25–75) | 0.60 (0.33–1.10) | 0.60 (0.40–0.83) | 0.95 |
| Creatinine (mg/dL)-m (p 25–75) | 1.00 (0.70–1.25) | 0.80 (0.60–1.13) | 0.19 |
| Glycemia (g/dL)-m (p 25–75) | 136 (118–162) | 127 (100–170) | 0.40 |
| PaO2 (mmHg)-m (p 25–75) | 115 (94–267) | 156 (105–293) | 0.26 |
| PaO2/FI02 ratio-m (p 25–75) | 254 (192–325) | 300 (198–369) | 0.24 |
| Platelets-m×103/mm3 (p 25–75) | 175 (136–216) | 202 (171–265) | 0.02 |
| Leukocytes-m×103/mm3 (p 25–75) | 13.9 (9.7–20.1) | 12.4 (9.6–16.9) | 0.32 |
| Hemoglobin (g/dL)-m (p 25-75) | 12.5 (11.0–14.8) | 12.1 (11.4–14.0) | 0.81 |
| Fibrinogen (mg/dL)-m (p 25–75) | 419 (337–631) | 443 (416–489) | 0.90 |
| INR-m (p 25–75) | 1.20 (1.01–1.31) | 1.06 (1.00–1.20) | 0.07 |
| aPTT (seconds)-m (p 25–75) | 27 (26–32) | 28 (25–30) | 0.91 |
| APACHE-II score-m (p 25–75) | 22 (19–27) | 20 (16–25) | 0.06 |
| Decompressive craniectomy-n (%) | 7 (20.6) | 9 (26.5) | 0.78 |
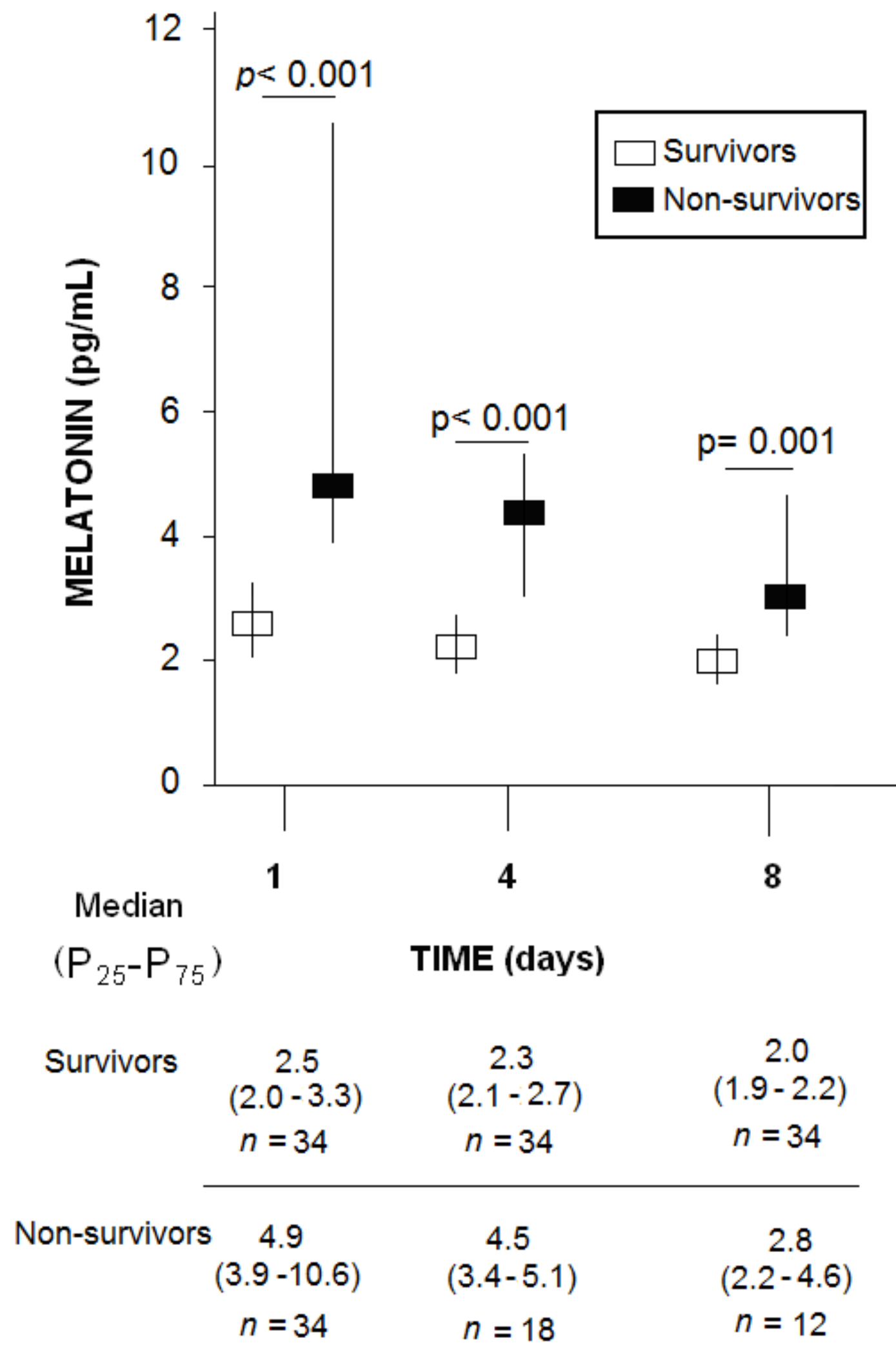
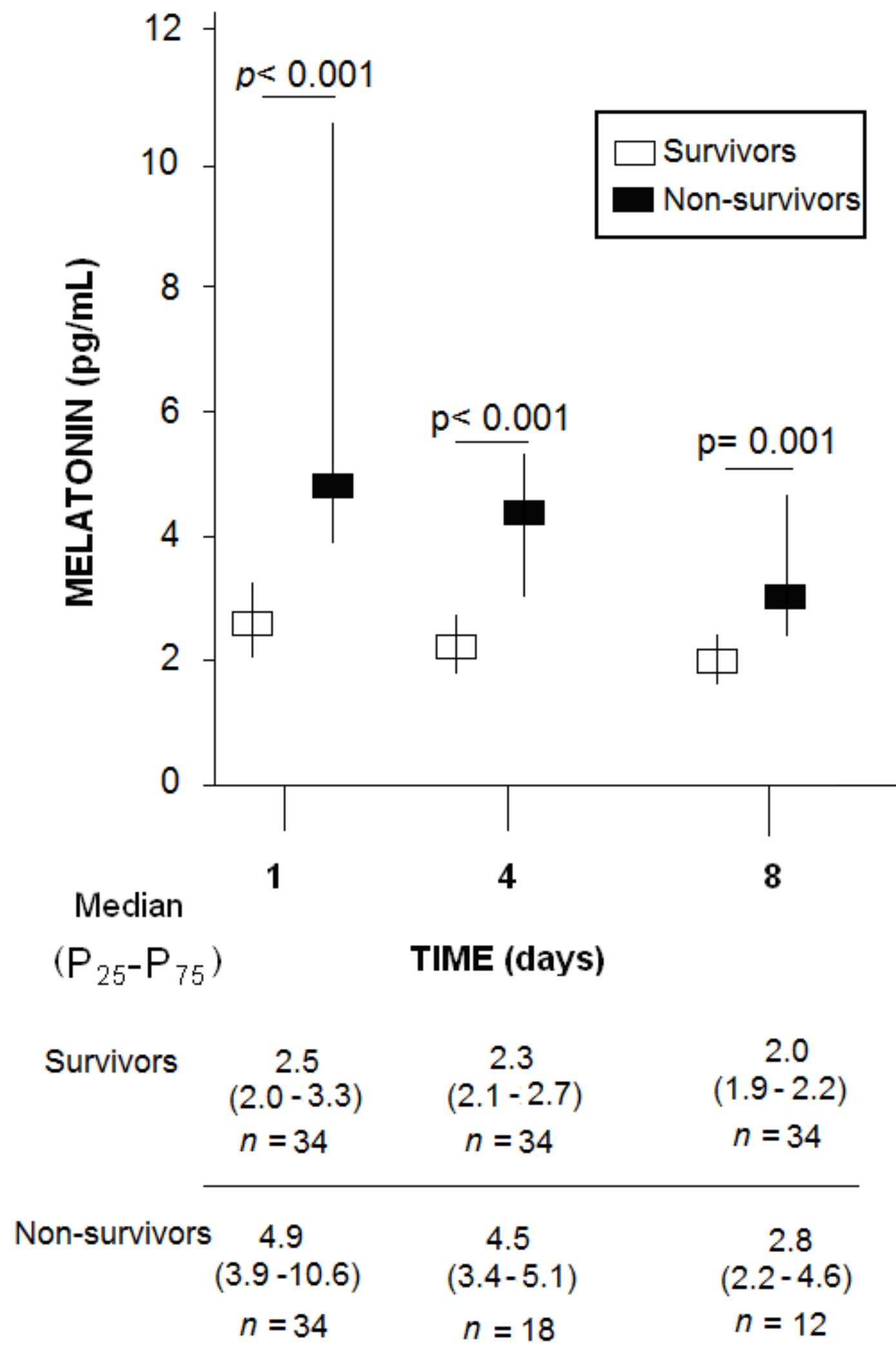
| Melatonin (pg/mL)-m (p 25–75) | 4.9 (3.9–10.6) | 2.5 (2.0–3.3) | <0.001 |
| Day 1 | Day 4 | Day 8 | |
|---|---|---|---|
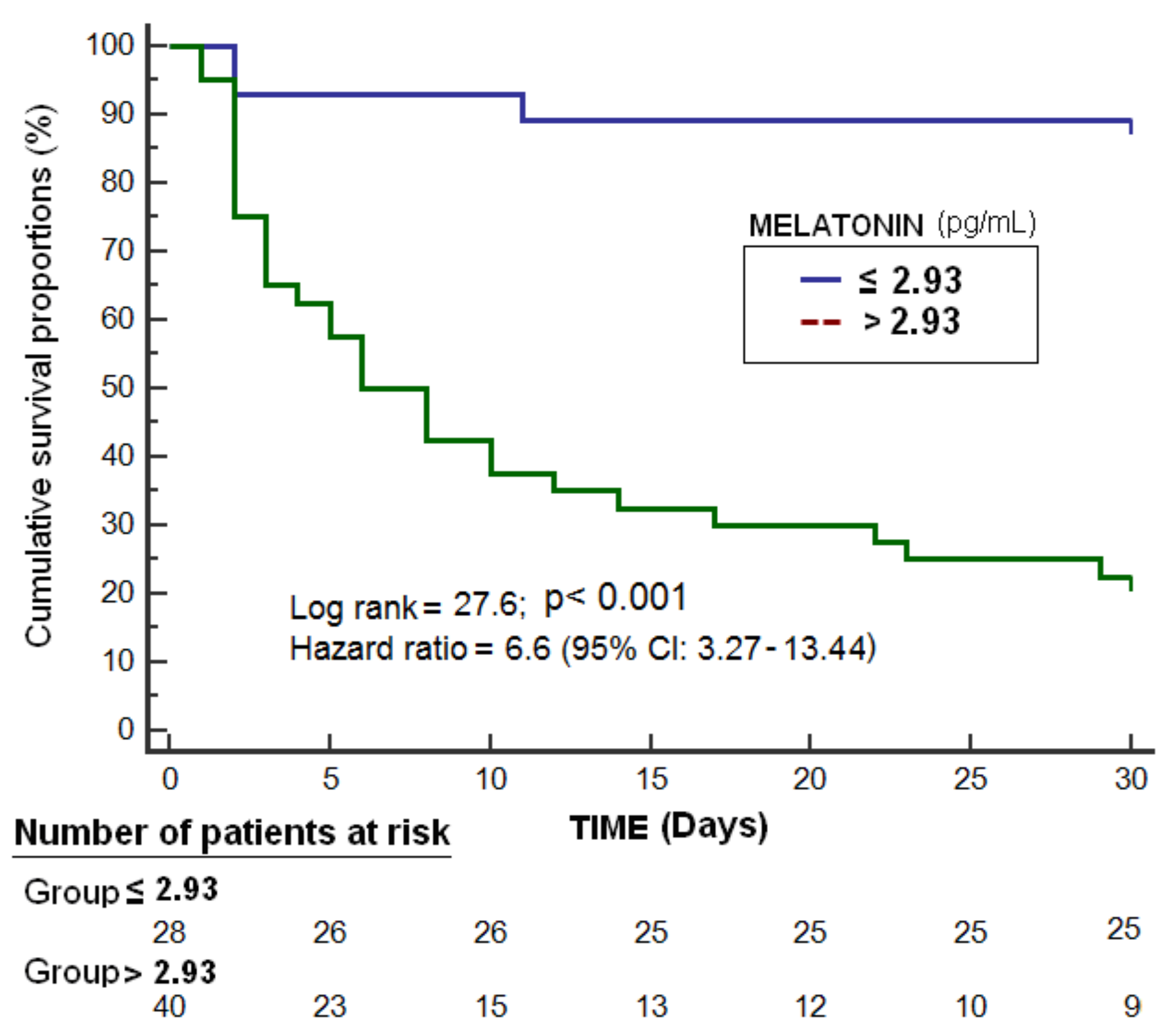
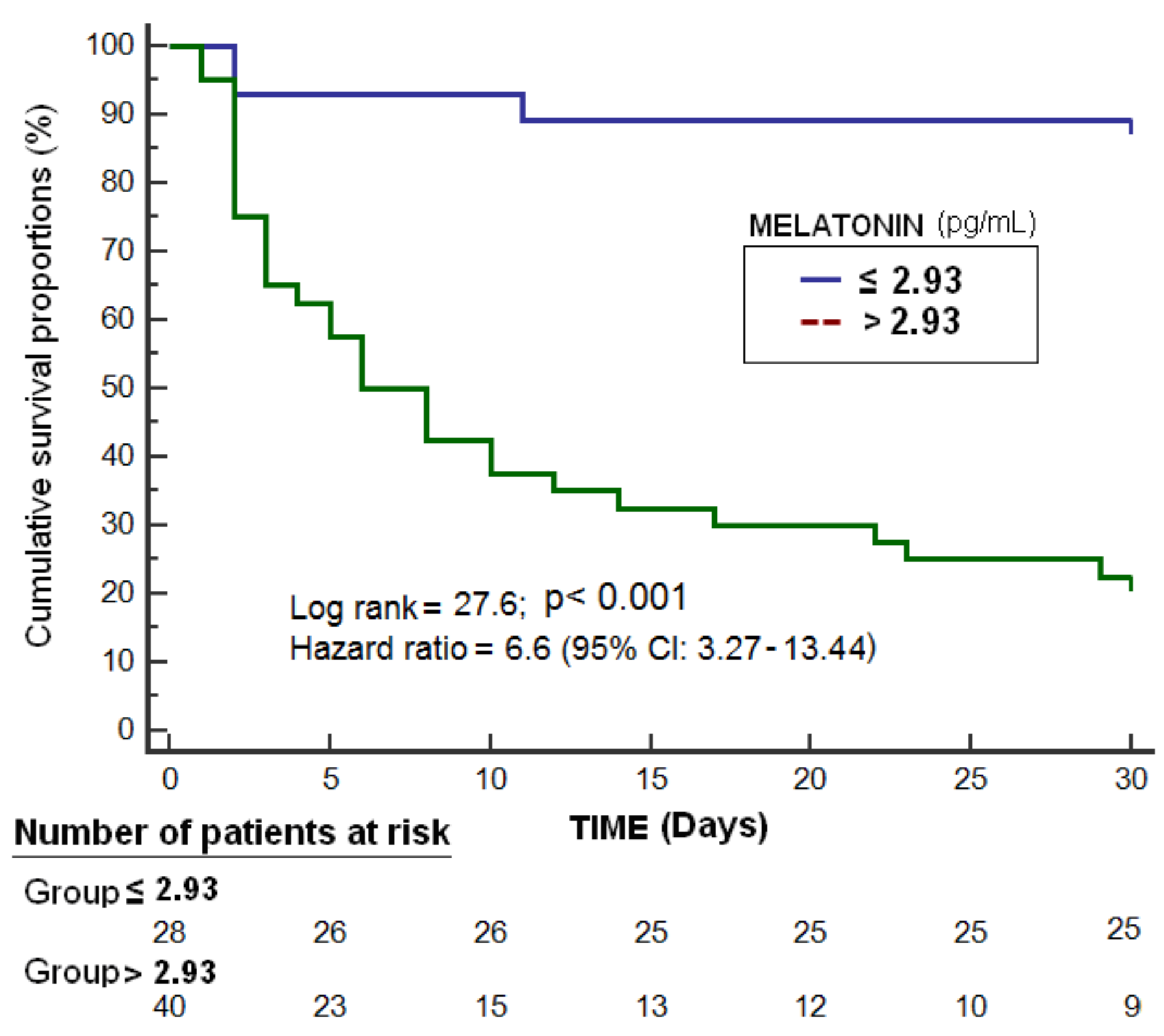
| Cut-off of melatonin (pg/mL) | >2.93 | >3.14 | >2.27 |
| Sensitivity (95% CI) | 91% (76%–98%) | 83% (59%–96%) | 75% (43%–95%) |
| Specificity (95% CI) | 74% (56%–87%) | 88% (73%–97%) | 82% (66%–93%) |
| Positive predictive value (95% CI) | 78% (66%–86%) | 79% (59%–91%) | 60% (40%–77%) |
| Positive likelihood ratio (95% CI) | 3.4 (1.9–6.1) | 7.1 (2.8–18.2) | 4.3 (1.9–9.4) |
| Negative predictive value (95% CI) | 89% (74%–96%) | 91% (78%–97%) | 90% (78%–96%) |
| Negative likelihood ratio (95% CI) | 0.12 (0.04–0.40) | 0.19 (0.07–0.50) | 0.30 (0.10–0.80) |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Serum melatonin levels (pg/mL) | 2.369 | 1.328–4.227 | 0.004 |
| Glasgow Coma Scale (points) | 0.695 | 0.472–1.022 | 0.06 |
| Lactic acid (mmol/L) | 1.134 | 0.576–2.232 | 0.72 |
| Platelet count (each 1000/mm3) | 0.997 | 0.987–1.008 | 0.63 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorente, L.; Martín, M.M.; Abreu-González, P.; Sabatel, R.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Cáceres, J.J.; Jiménez, A.; García-Marín, V. Higher Serum Melatonin Levels during the First Week of Malignant Middle Cerebral Artery Infarction in Non-Surviving Patients. Brain Sci. 2019, 9, 346. https://doi.org/10.3390/brainsci9120346
Lorente L, Martín MM, Abreu-González P, Sabatel R, Ramos L, Argueso M, Solé-Violán J, Cáceres JJ, Jiménez A, García-Marín V. Higher Serum Melatonin Levels during the First Week of Malignant Middle Cerebral Artery Infarction in Non-Surviving Patients. Brain Sciences. 2019; 9(12):346. https://doi.org/10.3390/brainsci9120346
Chicago/Turabian StyleLorente, Leonardo, María M. Martín, Pedro Abreu-González, Rafael Sabatel, Luis Ramos, Mónica Argueso, Jordi Solé-Violán, Juan J. Cáceres, Alejandro Jiménez, and Victor García-Marín. 2019. "Higher Serum Melatonin Levels during the First Week of Malignant Middle Cerebral Artery Infarction in Non-Surviving Patients" Brain Sciences 9, no. 12: 346. https://doi.org/10.3390/brainsci9120346
APA StyleLorente, L., Martín, M. M., Abreu-González, P., Sabatel, R., Ramos, L., Argueso, M., Solé-Violán, J., Cáceres, J. J., Jiménez, A., & García-Marín, V. (2019). Higher Serum Melatonin Levels during the First Week of Malignant Middle Cerebral Artery Infarction in Non-Surviving Patients. Brain Sciences, 9(12), 346. https://doi.org/10.3390/brainsci9120346