Effects of 2-Year Cognitive–Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
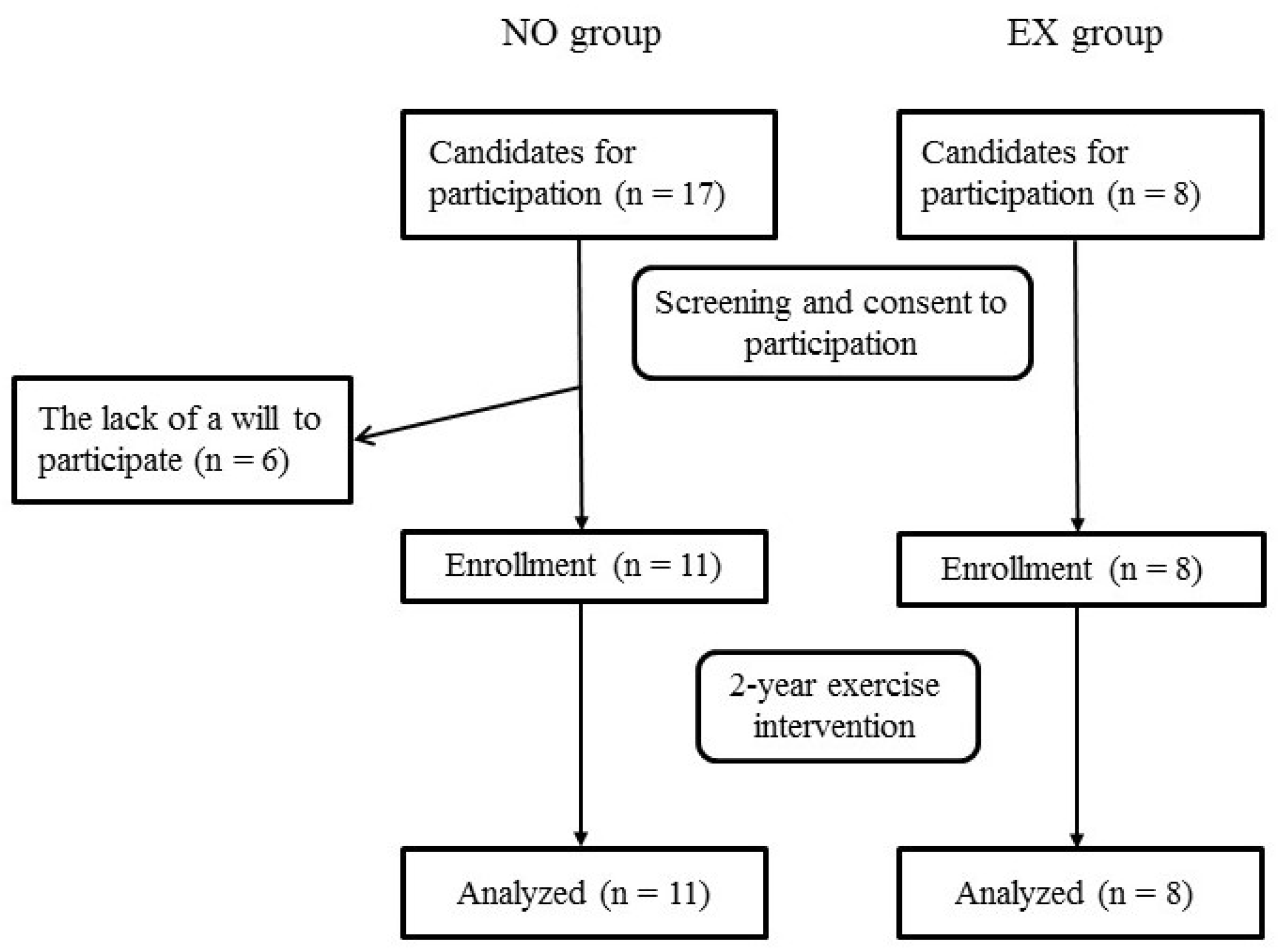
2.1. Participants
2.2. Study Design
2.3. Exercise Intervention
2.4. Demographic Data and Anthropometry
2.5. Cognitive Function
2.6. Quadriceps Isometric Muscle Strength and Motor Ability
2.7. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Subjects
3.2. Effects of DT Training on Body Composition, Muscle Strength, and Motor Ability
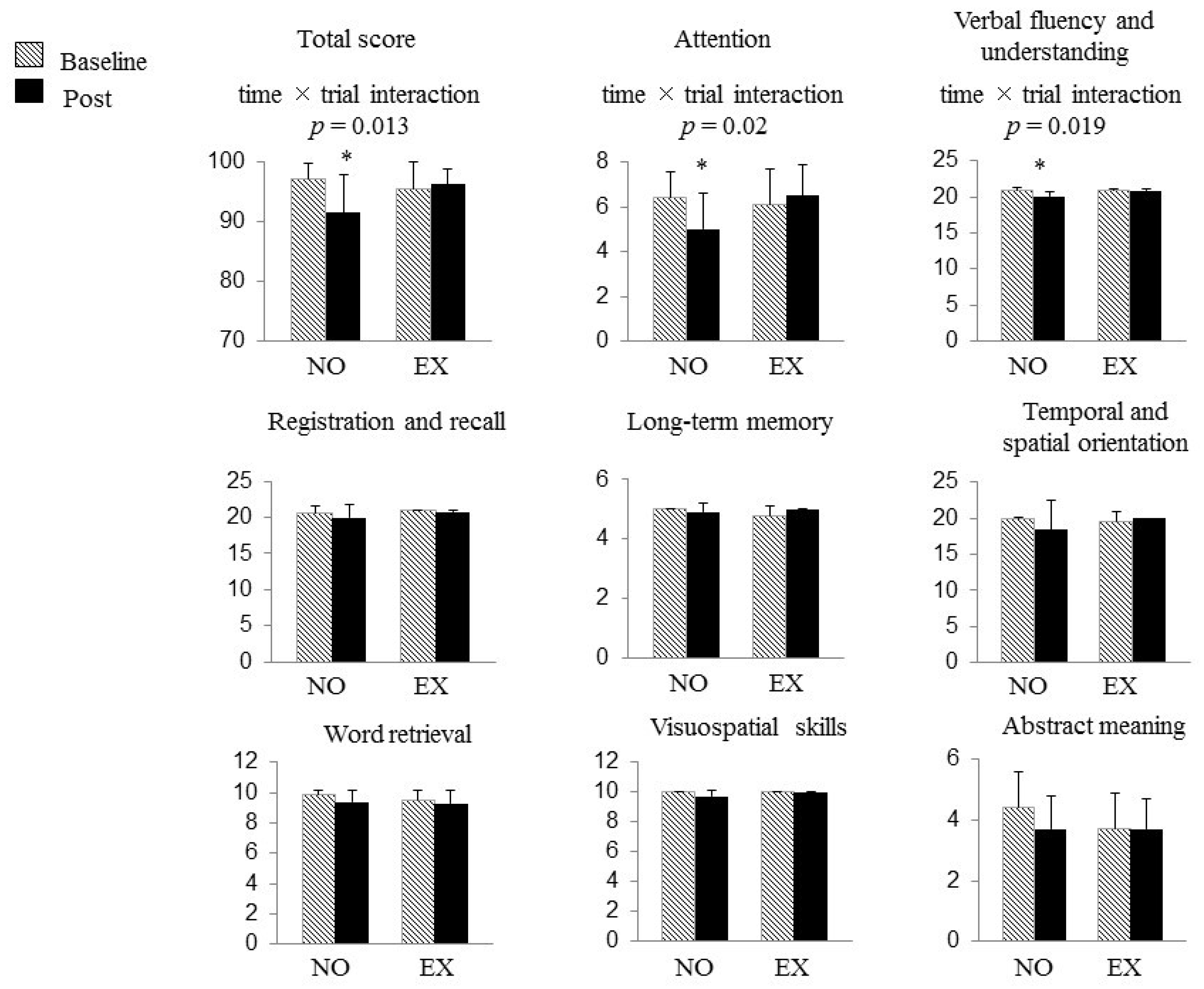
3.3. Cognitive Function Outcome
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016 Improving Healthcare for People Living with Dementia. Coverage, Quality AND Costs Now and in the Future. Alzheimer’s Disease International: London, 2016; Available online: Https://www.alz.co.uk/research/WorldAlzheimerReport2016.pdf (accessed on 3 October 2017).
- Ministry of Health L and Welfare. Number of elderly persons with Dementia. January 2017. Available online: http://www.mhlw.go.jp/file/04-Houdouhappyou-12304500-Roukenkyoku-Ninchishougyakutaiboushitaisakusuishinshitsu/02_1.pdf (accessed on 3 October 2017).
- Bruvik, F.K.; Ulstein, I.D.; Ranhoff, A.H.; Engedal, K. The quality of life of people with dementia and their family carers. Dement. Geriatr. Cogn. Disord. 2012, 34, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Karttunen, K.; Karppi, P.; Hiltunen, A.; Vanhanen, M.; Valimaki, T.; Martikainen, J.; Valtonen, H.; Sivenius, J.; Soininen, H.; Hartikainen, S.; et al. Neuropsychiatric symptoms and quality of life in patients with very mild and mild Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2011, 26, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Etters, L.; Goodall, D.; Harrison, B.E. Caregiver burden among dementia patient caregivers: A review of the literature. J. Am. Acad. Nurse. Pract. 2008, 20, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Chang, M.; Rose, K.; Kim, S. Predictors of caregiver burden in caregivers of individuals with dementia. J. Adv. Nurs. 2012, 68, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.W.; Sano, M. Economic considerations in the management of Alzheimer’s disease. Clin. Interv. Aging 2006, 1, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Nouchi, R.; Taki, Y.; Takeuchi, H.; Hashizume, H.; Nozawa, T.; Sekiguchi, A.; Nouchi, H.; Kawashima, R. Beneficial effects of reading aloud and solving simple arithmetic calculations (learning therapy) on a wide range of cognitive functions in the healthy elderly: Study protocol for a randomized controlled trial. Trials 2012, 6, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Berch, D.B.; Helmers, K.F.; Jobe, J.B.; Leveck, M.D.; Marsiske, M.; Morris, J.N.; Rebok, G.W.; Smith, D.M.; Tennstedt, S.L.; et al. Effects of cognitive training interventions with older adults: A randomized controlled trial. JAMA 2002, 288, 2271–2281. [Google Scholar] [CrossRef] [PubMed]
- Mozolic, J.L.; Long, A.B.; Morgan, A.R.; Rawley-Payne, M.; Laurienti, P.J. A cognitive training intervention improves modality-specific attention in a randomized controlled trial of healthy older adults. Neurobiol. Aging 2011, 32, 655–668. [Google Scholar] [CrossRef] [PubMed]
- Larson, E.B.; Wang, L.; Bowen, J.D.; McCormick, W.C.; Teri, L.; Crane, P.; Kukull, W. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann. Intern. Med. 2006, 144, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Heyn, P.C.; Johnson, K.E.; Kramer, A.F. Endurance and strength training outcomes on cognitively impaired and cognitively intact older adults: A meta-analysis. J. Nutr. Health Aging 2008, 12, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Blankevoort, C.G.; van Heuvelen, M.J.; Boersma, F.; Luning, H.; de Jong, J.; Scherder, E.J. Review of effects of physical activity on strength, balance, mobility and ADL performance in elderly subjects with dementia. Dement. Geriatr. Cogn. Disord. 2010, 30, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Okazaki, K.; Imai, D.; Yamashina, Y.; Takeda, R.; Naghavi, N.; Ota, A.; Hirasawa, Y.; Miyagawa, T. The effect of cognitive-motor dual-task training on cognitive function and plasma amyloid beta peptide 42/40 ratio in healthy elderly persons: A randomized controlled trial. BMC Geriatr. 2015, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Teng, E.L.; Chui, H.C. The Modified Mini-Mental State (3MS) examination. J. Clin. Psychiatry 1987, 48, 314–318. [Google Scholar] [PubMed]
- Hamada, K.; Koga, N.; Hamada, T. Usefulness of a Japanese verision of the modified mini-mental state (3MS) examination as a screening test for patients with dementia. Jpn. J. Geriatr. Psychiatry 1992, 3, 425–432. [Google Scholar]
- Van Uffelen, J.G.; Chinapaw, M.J.; van Mechelen, W.; Hopman-Rock, M. Walking or vitamin B for cognition in older adults with mild cognitive impairment? A randomised controlled trial. Br. J. Sports. Med. 2008, 42, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of aerobic exercise on mild cognitive impairment: A controlled trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Cassilhas, R.C.; Viana, V.A.; Grassmann, V.; Santos, R.T.; Santos, R.F.; Tufik, S.; Mello, M.T. The impact of resistance exercise on the cognitive function of the elderly. Med. Sci. Sports. Exerc. 2007, 39, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Graf, P.; Beattie, B.L.; Ashe, M.C.; Handy, T.C. Resistance training and executive functions: A 12-month randomized controlled trial. Arch. Intern. Med. 2010, 170, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Desjardins-Crepeau, L.; Berryman, N.; Fraser, S.A.; Vu, T.T.; Kergoat, M.J.; Li, K.Z.; Bosquet, L.; Bherer, L. Effects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adults. Clin. Interv. Aging 2016, 11, 1287–1299. [Google Scholar] [CrossRef] [PubMed]
- Ohsugi, H.; Ohgi, S.; Shigemori, K.; Schneider, E.B. Differences in dual-task performance and prefrontal cortex activation between younger and older adults. BMC Neurosci. 2013, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Law, L.L.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of combined cognitive and exercise interventions on cognition in older adults with and without cognitive impairment: A systematic review. Ageing Res. Rev. 2014, 15, 61–75. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, L.S.; Chan, A.; Davis, J.C.; Beattie, B.L.; Graf, P.; Voss, M.W.; Sharma, D.; Liu-Ambrose, T. Physical activity improves verbal and spatial memory in older adults with probable mild cognitive impairment: A 6-month randomized controlled trial. J. Aging Res. 2013, 2013, 861893. [Google Scholar] [CrossRef] [PubMed]
- Ruitenberg, A.; den Heijer, T.; Bakker, S.L.; van Swieten, J.C.; Koudstaal, P.J.; Hofman, A.; Breteler, M.M. Cerebral hypoperfusion and clinical onset of dementia: The Rotterdam Study. Ann. Neurol. 2005, 57, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Rhyu, I.J.; Bytheway, J.A.; Kohler, S.J.; Lange, H.; Lee, K.J.; Boklewski, J.; McCormick, K.; Williams, N.I.; Stanton, G.B.; Greenough, W.T.; et al. Effects of aerobic exercise training on cognitive function and cortical vascularity in monkeys. Neuroscience 2010, 167, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Shimada, H.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T. Association of insulin-like growth factor-1 with mild cognitive impairment and slow gait speed. Neurobiol. Aging 2015, 36, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Cassilhas, R.C.; Lee, K.S.; Fernandes, J.; Oliveira, M.G.; Tufik, S.; Meeusen, R.; de Mello, M.T. Spatial memory is improved by aerobic and resistance exercise through divergent molecular mechanisms. Neuroscience 2012, 202, 309–317. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017; p. 193. [Google Scholar]
- Basu, R. Effects of education and income on cognitive functioning among Indians aged 50 years and older: Evidence from the Study on Global Ageing and Adult Health (SAGE) Wave 1 (2007–2010). WHO South East. Asia J. Public Health 2013, 2, 156–164. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 19) | Non-Exercise Group (n = 11) | Exercise Group (n = 8) | p | |
|---|---|---|---|---|
| Gender (n, %) | 0.202 | |||
| Male | 2 (10.5%) | 2 (18.2%) | 0 (0%) | |
| Female | 17 (89.5%) | 9 (81.8%) | 8 (100%) | |
| Age (years) | 73.2 ± 3.5 | 71.9 ± 4.0 | 75.0 ± 1.5 | 0.056 |
| Education (years) | 12.3 ± 1.7 | 12.7 ± 1.9 | 11.6 ± 1.0 | 0.127 |
| Medication (n, %) | 0.633 | |||
| Yes | 9 (47.4%) | 5 (45.5%) | 4 (50.0%) | |
| No | 10 (52.6%) | 6 (54.5%) | 4 (50.0%) | |
| Past history (n, %) | 0.361 | |||
| Yes | 7 (36.8%) | 5 (45.5%) | 2 (25.0%) | |
| No | 12 (63.2%) | 6 (54.5%) | 6 (75.0%) | |
| Knee osteoarthritis | 2 (10.5%) | 1 (9.1%) | 1 (12.5%) | 0.811 |
| Cancer | 3 (15.8%) | 2 (18.2%) | 1 (12.5%) | 0.737 |
| Others | 2 (10.5%) | 2 (18.2%) | 0 (0%) | 0.202 |
| Present illness (n, %) | 0.463 | |||
| Yes | 10 (52.6%) | 5 (45.5%) | 5 (62.5%) | |
| No | 9 (47.4%) | 6 (54.5%) | 3 (37.5%) | |
| Hypertension | 6 (31.6%) | 2 (18.2%) | 4 (50.0%) | 0.141 |
| Hyperlipidemia | 4 (21.1%) | 2 (18.2%) | 2 (25.0%) | 0.719 |
| Others | 4 (21.1%) | 2 (18.2%) | 2 (25.0%) | 0.719 |
| Non-Exercise Group (n = 11) | Exercise Group (n = 8) | p | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Post | Baseline | Post | Main Effect of Intervention | Main Effect of Group | Intervention × Group Interaction | ||
| SBP | (mmHg) | 138 ± 17 | 144 ± 19 | 136 ± 17 | 135 ± 15 | 0.464 | 0.501 | 0.286 |
| DBP | (mmHg) | 79 ± 10 | 82 ± 10 | 82 ± 9 | 85 ± 9 | 0.267 | 0.499 | 0.918 |
| BMI | (kg/m2) | 22.5 ± 3.7 | 21.9 ± 4.1 | 22.4 ± 4.6 | 21.9 ± 5.0 * | 0.006 | 0.968 | 0.889 |
| Body fat | (%) | 27.2 ± 6.4 | 26.6 ± 8.4 | 27.8 ± 6.5 | 27.2 ± 6.7 | 0.307 | 0.852 | 0.986 |
| Leg muscle mass | (kg) | 8.7 ± 2.4 | 8.6 ± 2.4 | 7.6 ± 1.1 | 7.7 ± 0.9 | 0.903 | 0.269 | 0.593 |
| Quad. muscle strength | (kg) | 30.5 ± 8.1 | 26.9 ± 8.7 * | 27.4 ± 6.0 | 20.8 ± 4.1 * | <0.001 | 0.173 | 0.119 |
| MSL | (cm) | 109.5 ± 10.8 | 86.8 ± 10.0 * | 103.5 ± 12.2 | 83.8 ± 10.1 * | <0.001 | 0.338 | 0.455 |
| TUG | (sec) | 5.28 ± 0.73 | 6.49 ± 0.71 * | 5.61 ± 0.67 | 6.67 ± 0.99 * | <0.001 | 0.443 | 0.678 |
| Single-leg standing | (sec) | 87.4 ± 44.1 | 57.4 ± 45.6 * | 87.9 ± 42.1 | 71.6 ± 48.9 | 0.008 | 0.711 | 0.388 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morita, E.; Yokoyama, H.; Imai, D.; Takeda, R.; Ota, A.; Kawai, E.; Suzuki, Y.; Okazaki, K. Effects of 2-Year Cognitive–Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study. Brain Sci. 2018, 8, 86. https://doi.org/10.3390/brainsci8050086
Morita E, Yokoyama H, Imai D, Takeda R, Ota A, Kawai E, Suzuki Y, Okazaki K. Effects of 2-Year Cognitive–Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study. Brain Sciences. 2018; 8(5):86. https://doi.org/10.3390/brainsci8050086
Chicago/Turabian StyleMorita, Emiko, Hisayo Yokoyama, Daiki Imai, Ryosuke Takeda, Akemi Ota, Eriko Kawai, Yuta Suzuki, and Kazunobu Okazaki. 2018. "Effects of 2-Year Cognitive–Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study" Brain Sciences 8, no. 5: 86. https://doi.org/10.3390/brainsci8050086
APA StyleMorita, E., Yokoyama, H., Imai, D., Takeda, R., Ota, A., Kawai, E., Suzuki, Y., & Okazaki, K. (2018). Effects of 2-Year Cognitive–Motor Dual-Task Training on Cognitive Function and Motor Ability in Healthy Elderly People: A Pilot Study. Brain Sciences, 8(5), 86. https://doi.org/10.3390/brainsci8050086