The Multiple Hit Hypothesis for Gulf War Illness: Self-Reported Chemical/Biological Weapons Exposure and Mild Traumatic Brain Injury




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Self-Reported Mild Traumatic Brain Injury (mTBI)
“Some people have the misconception that mild traumatic brain injury (also known as ‘concussion’) only happens when you lose consciousness after being hit on the head or when the symptoms last for a long time. However, a mild traumatic brain injury occurs anytime you have an impact to the head that causes symptoms for any amount of time (e.g., seconds or longer). These symptoms include: sensitivity to light or noise, headache, dizziness, balance problems, nausea, vomiting, trouble sleeping, fatigue, confusion, difficulty remembering, difficulty concentrating, or loss of consciousness.”
2.3. Demographics, Chemical/Biological Weapon (CBW) Exposure, and Health Outcome Surveys
2.4. Clinical Interview
2.5. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. CBW and mTBI Self-Reported Exposures in GWIC Cohort
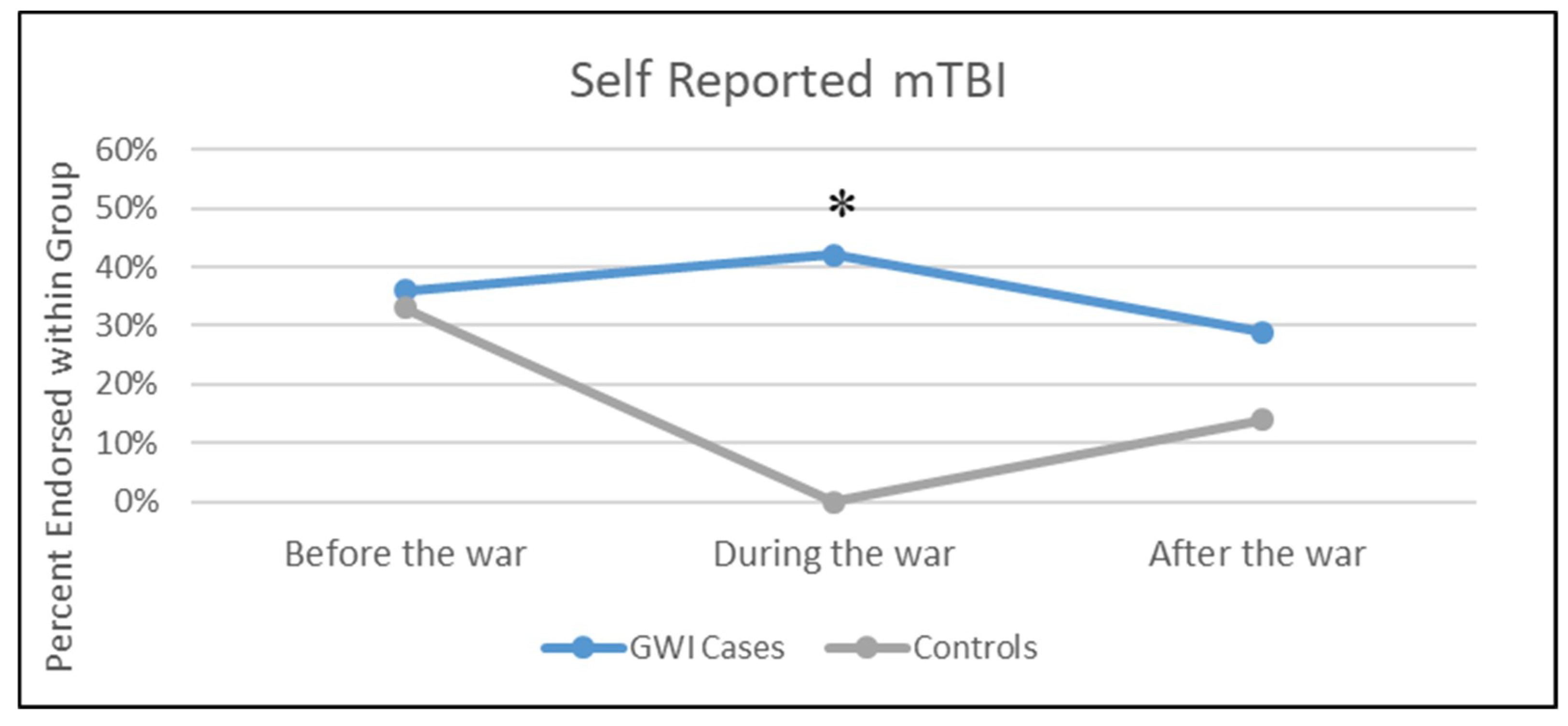
3.3. Results of mTBI and CBW Self-Reported Exposure by GWI Case Status
3.4. Participant Characteristics by Exposure Categories
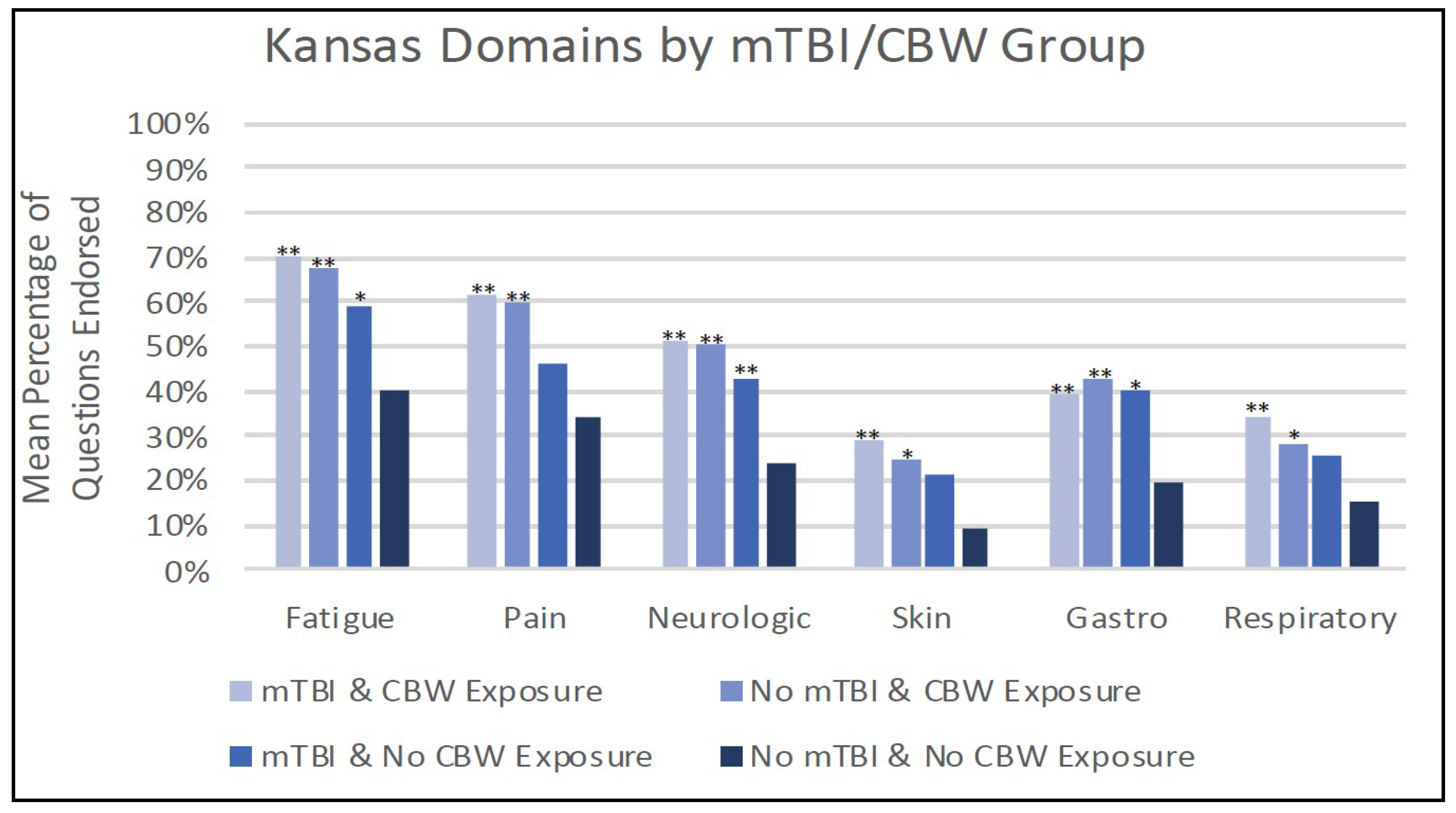
3.5. Kansas Criteria by Exposure Group
3.6. Association between Exposure Groups and Chronic Health Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sullivan, K.; Krengel, M.; Bradford, W.; Stone, C.; Thompson, T.A.; Heeren, T.; White, R.F. Neuropsychological functioning in military pesticide applicators from the Gulf War: Effects on information processing speed, attention and visual memory. Neurotoxicol. Teratol. 2018, 65, 1–13. [Google Scholar] [CrossRef] [PubMed]
- White, R.F.; Steele, L.; O’Callaghan, J.P.; Sullivan, K.; Binns, J.H.; Golomb, B.A.; Bloom, F.E.; Bunker, J.A.; Crawford, F.; Graves, J.C.; et al. Recent research on Gulf War illness and other health problems in veterans of the 1991 Gulf War: Effects of toxicant exposures during deployment. Cortex 2016, 74, 449–475. [Google Scholar] [CrossRef] [PubMed]
- Research Advisory Committee on Gulf War Veterans’ Illnesses. Gulf War Illness and the Health of Gulf War Veterans: Research update and recommendations, 2009–2013; Updated Scientific Findings and Recommendations; US Government Printing Office: Washington, DC, USA, 2014.
- Research Advisory Committee on Gulf War Veterans’ Illnesses. Gulf War Illness and the Health of Gulf War Veterans: Scientific Findings and Recommendations; US Government Printing Office: Washington, DC, USA, 2008.
- Sullivan, K.; Krengel, M.; Proctor, S.; Devine, S.; Heeren, T.; White, R. Cognitive Functioning in Treatment-Seeking Gulf War Veterans: Pyridostigmine Bromide Use and PTSD. J. Psychopathol. Behav. Assess. 2003, 25, 95–103. [Google Scholar] [CrossRef]
- Proctor, S.P.; Heeren, T.; White, R.F.; Wolfe, J.; Borgos, M.S.; Davis, J.D.; Pepper, L.; Clapp, R.; Sutker, P.B.; Vasterling, J.J.; et al. Health status of Persian Gulf War veterans: Self-reported symptoms, environmental exposures and the effect of stress. Int. J. Epidemiol. 1998, 27, 1000–1010. [Google Scholar] [CrossRef] [PubMed]
- Chao, L.L.; Reeb, R.; Esparza, I.L.; Abadjian, L.R. Associations between the self-reported frequency of hearing chemical alarms in theater and regional brain volume in Gulf War Veterans. NeuroToxicology 2016, 53, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Chronic Multisymptom Illness in Gulf War Veterans: Case Definitions Reexamined; The National Academies Press: Washington, DC, USA, 2014. [Google Scholar]
- Fukuda, K.; Nisenbaum, R.; Stewart, G.; Thompson, W.W.; Robin, L.; Washko, R.M.; Noah, D.L.; Barrett, D.H.; Randall, B.; Herwaldt, B.L.; et al. Chronic multisymptom illness affecting Air Force veterans of the Gulf War. JAMA 1998, 280, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Steele, L. Prevalence and Patterns of Gulf War Illness in Kansas Veterans: Association of Symptoms with Characteristics of Person, Place, and Time of Military Service. Am. J. Epidemiol. 2000, 152, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Haley, R.W.; Tuite, J.J. Epidemiologic Evidence of Health Effects from Long-Distance Transit of Chemical Weapons Fallout from Bombing Early in the 1991 Persian Gulf War. Neuroepidemiology 2013, 40, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Steele, L.; Sastre, A.; Gerkovich, M.M.; Cook, M.R. Complex Factors in the Etiology of Gulf War Illness: Wartime Exposures and Risk Factors in Veteran Subgroups. Environ. Health Perspect. 2011, 120, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, J.; Proctor, S.P.; Erickson, D.J.; Hu, H. Risk factors for multisymptom illness in US Army veterans of the Gulf War. J. Occup. Environ. Med. 2002, 44, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Proctor, S.P.; Heaton, K.J.; Heeren, T.; White, R.F. Effects of sarin and cyclosarin exposure during the 1991 Gulf War on neurobehavioral functioning in US army veterans. NeuroToxicology 2006, 27, 931–939. [Google Scholar] [CrossRef] [PubMed]
- White, R.F.; Proctor, S.P.; Heeren, T.; Wolfe, J.; Krengel, M.; Vasterling, J.; Ozonoff, D.M. Neuropsychological function in Gulf War veterans: Relationships to self-reported toxicant exposures. Am. J. Ind. Med. 2001, 40, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Yee, M.; Janulewicz, P.; Seichepine, D.; Sullivan, K.; Proctor, S.; Krengel, M. Multiple Mild Traumatic Brain Injuries Are Associated with Increased Rates of Health Symptoms and Gulf War Illness in a Cohort of 1990–1991 Gulf War Veterans. Brain Sci. 2017, 7, 79. [Google Scholar] [CrossRef] [PubMed]
- Yee, M.K.; Seichepine, D.R.; Janulewicz, P.A.; Sullivan, K.A.; Proctor, S.P.; Krengel, M.H. Self-Reported Traumatic Brain Injury, Health and Rate of Chronic Multisymptom Illness in Veterans from the 1990–1991 Gulf War. J. Head Trauma Rehabil. 2016, 31, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Chao, L.L. The Relationship Between Traumatic Brain Injury and Rates of Chronic Symptomatic Illness in 202 Gulf War Veterans. Mil. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Feng, L. Alpha-Synuclein and the Multiple Hit Hypothesis of Parkinson’s Disease. Ph.D. Thesis, Georgetown University, Washington, DC, USA, 2012. [Google Scholar]
- Barnett, M.L.; Tusor, N.; Ball, G.; Chew, A.; Falconer, S.; Aljabar, P.; Counsell, S.J. Exploring the multiple-hit hypothesis of preterm white matter damage using diffusion MRI. NeuroImage Clin. 2018, 17, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Sulzer, D. Multiple hit hypotheses for dopamine neuron loss in Parkinson’s disease. Trends Neurosci. 2007, 30, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.A.; Raina, A.K.; Perry, G.; Zhu, X. S4-02-01 Alzheimer disease: The two hit hypothesis. Neurobiol. Aging 2004, 25, S68. [Google Scholar] [CrossRef]
- Feigenson, K.A.; Kusnecov, A.W.; Silverstein, S.M. Inflammation and the two-hit hypothesis of schizophrenia. Neurosci. Biobehav. Rev. 2014, 38, 72–93. [Google Scholar] [CrossRef] [PubMed]
- Vynorius, K.C.; Paquin, A.M.; Seichepine, D.R. Lifetime Multiple Mild Traumatic Brain Injuries Are Associated with Cognitive and Mood Symptoms in Young Healthy College Students. Front. Neurol. 2016, 7. [Google Scholar] [CrossRef] [PubMed]
- Robbins, C.A.; Daneshevar, D.H.; Picano, J.D.; Gevett, B.E.; Baugh, C.M.; Riley, D.O.; Nowinski, C.J.; McKee, A.C.; Cantu, R.C.; Stern, R.A. Self-reported concussion history: Impact of providing a definition of concussion. Open Access J. Sports Med. 2014, 7, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Seichepine, D.R.; Stamm, J.M.; Daneshvar, D.H.; Riley, D.O.; Baugh, C.M.; Gavett, B.E.; Tripodis, Y.; Martin, B.; Chaisson, C.; McKee, A.C.; et al. Profile of self-reported problems with executive functioning in college and professional football players. J. Neurotrauma 2013, 30, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Proctor, S.P. Development of a Structured Neurotoxicant Assessment Checklist (SNAC) for Clinical Use in Veteran Populations. Department of Veterans Affairs, VA Boston Healthcare System, 2006. Available online: https://www.va.gov/RAC-GWVI/meetings/sep2014/Presentation7KimberlySullivanNancyKlimas.pdf (accessed on 11 November 2018).
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a clinician-administered PTSD scale. J. Trauma. Stress 1995, 8, 75–90. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B. Structured Clinical Interview for the DSM-IV Axis, I. Disorders. 1996. Available online: https://www.ptsd.va.gov/professional/assessment/adult-int/scid-ptsd-module.asp#obtain (accessed on 11 November 2018).
- Van Riper, S.M.; Alexander, A.L.; Koltyn, K.F.; Stegner, A.J.; Ellingson, L.D.; Destiche, D.J.; Cook, D.B. Cerebral white matter structure is disrupted in Gulf War Veterans with chronic musculoskeletal pain. Pain 2017, 158, 2364–2375. [Google Scholar] [CrossRef] [PubMed]
- Chao, L.L.; Zhang, Y.; Buckley, S. Effects of low-level sarin and cyclosarin exposure on white matter integrity in Gulf War Veterans. NeuroToxicology 2015, 48, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Rayhan, R.U.; Stevens, B.W.; Timbol, C.R.; Adewuyi, O.; Walitt, B.; VanMeter, J.W.; Baraniuk, J.N. Increased Brain White Matter Axial Diffusivity Associated with Fatigue, Pain and Hyperalgesia in Gulf War Illness. PLoS ONE 2013, 8, e58493. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, J.P.; Michalovicz, L.T.; Kelly, K.A. Supporting a Neuroimmune Basis of Gulf War Illness. EBioMedicine 2016, 13, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Georgopoulos, A.P.; James, L.M.; Carpenter, A.F.; Engdahl, B.E.; Leuthold, A.C.; Lewis, S.M. Gulf War illness (GWI) as a neuroimmune disease. Exp. Brain Res. 2017, 10, 3217–3225. [Google Scholar] [CrossRef] [PubMed]
- Banks, C.N.; Lein, P.J. A review of experimental evidence linking neurotoxic organophosphorus compounds and inflammation. Neurotoxicology 2012, 33, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Abou-Donia, M.B.; Conboy, L.A.; Kokkotou, E.; Jacobson, E.; Elmasry, E.M.; Elkafrawy, P.; Neely, M.; Bass, C.R.; Sullivan, K. Screening for novel central nervous system biomarkers in veterans with Gulf War Illness. Neurotoxicol. Teratol. 2017, 61, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Matzinger, P. An innate sense of danger. Ann. N. Y. Acad. Sci. 2002, 961, 341–342. [Google Scholar] [CrossRef] [PubMed]
- Matzinger, P. The danger model: A renewed sense of self. Science 2002, 296, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.Y.; Matzinger, P. Hydrophobicity: An ancient damage-associated molecular pattern that initiates innate immune responses. Nat. Rev. Immunol. 2004, 4, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, F.; Mander, K.A.; Leonard, A.V.; Vink, R. Neurogenic inflammation after traumatic brain injury and its potentiation of classical inflammation. J. Neuroinflamm. 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Borlongan, C.; Acosta, S.; De la Pena, I.; Tajiri, N.; Kaneko, Y.; Lozano, D.; Gonzales-Portillo, G. Neuroinflammatory responses to traumatic brain injury: Etiology, clinical consequences, and therapeutic opportunities. Neuropsychiatr. Dis. Treat. 2015, 11, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Rathbone, A.T.; Tharmaradinam, S.; Jiang, S.; Rathbone, M.P.; Kumbhare, D.A. A review of the neuro- and systemic inflammatory responses in post-concussion symptoms: Introduction of the “post-inflammatory brain syndrome” PIBS. Brain Behav. Immun. 2015, 46, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.J.; Ivins, B.J.; Schwab, K.A. Self-reported mild TBI and postconcussive symptoms in a peacetime active duty military population: Effect of multiple TBI history versus single mild TBI. J. Head. Trauma. Rehabil. 2013, 28, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Alhasson, F.; Seth, R.K.; Sarkar, S.; Kimono, D.A.; Albadrani, M.S.; Dattaroy, D.; Chandrashekaran, V.; Scott, G.I.; Raychoudhury, S.; Nagarkatti, M.; et al. High circulatory leptin mediated NOX-2-peroxynitrite-miR21 axis activate mesangial cells and promotes renal inflammatory pathology in nonalcoholic fatty liver disease. Redox Biol. 2018, 17, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Seth, R.K.; Kimono, D.; Alhasson, F.; Sarkar, S.; Albadrani, M.; Lasley, S.K.; Horner, R.; Janulewicz, P.; Nagarkatti, M.; Nagarkatti, P.; et al. Increased butyrate priming in the gut stalls microbiome associated-gastrointestinal inflammation and hepatic metabolic reprogramming in a mouse model of Gulf War Illness. Toxicol. Appl. Pharmacol. 2018, 350, 64–77. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Sample = 125 | |
|---|---|
| Age, years: Mean (SD) | 51.5 (6.0) |
| Females: n (%) | 19 (15.2%) |
| Race: n (%) | |
| Black/African America n | 18 (14.4%) |
| White/Caucasian | 93 (74.4%) |
| Other/Multiracial | 14 (11.2%) |
| Hispanic or Latino: n (%) | 12 (9.6%) |
| Education: n (%) | |
| Grade 12 | 8 (6.4%) |
| GED | 1 (0.8%) |
| HS plus technical training | 13 (10.4%) |
| Associate/2 years college | 29 (23.2%) |
| Some college | 17 (13.6%) |
| Bachelors | 22 (17.6%) |
| Advanced degree | 35 (28.0%) |
| Military Branch: n (%) | |
| Army | 84 (67.2%) |
| Marines | 13 (10.4%) |
| Navy | 20 (16.0%) |
| Air Force | 8 (6.4%) |
| Current PTSD: n (%) [n = 91] | 34 (37.4%) |
| GWI Case (Kansas): n (%) | 104 (83.2%) |
| Self-reported mTBI, during deployment: n (%) | 44 (35.2%) [Mean SD among those with: 2.0 (1.4)] |
| Self-reported mTBI, prior to deployment: n (%) | 46 (36.8%) [Mean SD among those with: 2.5 (2.3)] |
| Self-reported mTBI, after deployment: n (%) | 33 (26.4%) [Mean SD among those with: 2.4 (2.0)] |
| Self-reported chemical/biological exposure: n (%) | 59 (47.2%) |
| Variable | n Mean (SD) | mTBI & CBW | mTBI & No CBW | No mTBI & CBW | No mTBI & No CBW | p-Value |
|---|---|---|---|---|---|---|
| Age | n | 26 | 18 | 33 | 48 | 0.50 |
| Mean (SD) | 50.1 (6.0) | 51.3 (5.1) | 51.4 (4.9) | 52.4 (7.0) | ||
| Gender | Female, n (%) | 5 (19.2%) | 1 (5.6%) | 9 (27.3%) | 4 (8.3%) | 0.07 |
| Male, n (%) | 21 (80.8%) | 17 (94.4%) | 24 (72.7%) | 44 (91.7%) | ||
| Race | Black/African American, n (%) | 4 (15.4%) | 5 (27.8%) | 2 (6.1%) | 7 (14.6%) | 0.49 |
| White/Caucasian, n (%) | 18 (69.2%) | 11 (61.1%) | 28 (84.8%) | 36 (75.0%) | ||
| Other/Multiracial, n (%) | 4 (15.4%) | 2 (11.1%) | 3 (9.1%) | 5 (10.4%) | ||
| Hispanic or Latino | Yes, n (%) | 6 (23.1%) | 1 (5.6%) | 0 (0.0%) | 5 (10.4%) | 0.03 |
| No, n (%). | 20 (76.9%) | 17 (94.4%) | 33 (100.0%) | 43 (89.6%) | ||
| Education | Grade 12, n (%) | 0 (0.0%) | 2 (11.1%) | 0 (0.0%) | 6 (12.5%) | 0.50 |
| GED, n (%) | 0 (0.0%) | 0 (0.0%) | 1 (3.0%) | 0 (0.0%) | ||
| HS plus technical training, n (%) | 3 (11.5%) | 4 (22.2%) | 2 (6.1%) | 4 (8.3%) | ||
| Associate/2 years college, n (%) | 6 (23.1%) | 5 (27.8%) | 9 (27.3%) | 9 (18.8%) | ||
| Some college, n (%) | 5 (19.2%) | 2 (11.1%) | 4 (12.1%) | 6 (12.5%) | ||
| Bachelors, n (%) | 6 (23.1%) | 2 (11.1%) | 6 (18.2%) | 8 (16.7%) | ||
| Advanced degree, n (%) | 6 (23.1%) | 3 (16.7%) | 11 (33.3%) | 15 (31.3%) | ||
| Current PTSD (n = 91) | Yes, n (%) | 10 (50.0%) | 2 (22.2%) | 8 (33.3%) | 14 (36.8%) | 0.49 |
| No, n (%) | 10 (50.0%) | 7 (77.8%) | 16 (66.7%) | 24 (63.2%) | ||
| GWI case (Kansas) | Yes, n (%) | 26 (100.0%) | 18 (100.0%) | 30 (90.9%) | 30 (62.5%) | <0.01 |
| No, n (%) | 0 (0.0%) | 0 (0.0%) | 3 (9.1%) | 18 (37.5%) | ||
| Military Branch | Army, n (%) | 18 (69.2%) | 11 (61.1%) | 26 (78.8%) | 29 (60.4%) | 0.68 |
| Marines, n (%) | 3 (11.5%) | 2 (11.1%) | 4 (12.1%) | 4 (8.3%) | ||
| Navy, n (%) | 3 (11.5%) | 4 (22.2%) | 2 (6.1%) | 11 (22.9%) | ||
| Air Force, n (%) | 2 (7.7%) | 1 (5.6%) | 1 (3.0%) | 4 (8.3%) |
| Variable | CBW Exposure Only vs. Neither | mTBI Exposure Only vs. Neither | mTBI + CBW Exposure vs. Neither |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| High Blood Pressure | 0.80 (0.32,1.99) | 2.80 (0.90,8.72) | 0.88 (0.33,2.32) |
| Heart Attack or MI | 1.47 (0.09,24.35) | 2.76 (0.16,46.70) | 1.88 (0.11,31.35) |
| Asthma 1 | 5.11 (0.96,27.13) | 2.87 (0.37,22.13) | 6.90 (1.28,37.18) * |
| High sugar/diabetes 1 | 2.07 (0.43,9.92) | 4.28 (0.85,21.49) | 4.50 (1.02,19.81) * |
| Respiratory allergies or sinus problems 1,2,3 | 5.88 (2.16,16.00) * | 5.42 (1.67,17.61) * | 6.93 (2.37,20.26) * |
| Arthritis, rheumatism or gout | 1.54 (0.59,3.99) | 2.69 (0.88,8.27) | 1.68 (0.61,4.64) |
| Repeated trouble with neck, back or spine 1,2,3 | 3.30 (1.30,8.35) * | 4.86 (1.52,15.51) * | 10.20 (3.21,32.44) * |
| Blindness or trouble seeing with either eye 1 | 3.33 (0.77,14.44) | 4.29 (0.85,21.50) | 7.94 (1.92,32.88) * |
| Chronic lung disease 1 | 4.70 (0.47,47.30) | 9.40 (0.91,97.25) | 20.89 (2.44,179.09) * |
| Chronic skin conditions 1 | 2.93 (0.99,8.62) | 2.25 (0.61,8.32) | 6.83 (2.25,20.78) * |
| Memory loss 1,2,3 | 5.67 (2.05,15.65) * | 3.97 (1.22,12.95) * | 8.39 (2.50,28.21) * |
| Deafness or trouble hearing in either ear 1 | 1.62 (0.57,4.67) | 2.76 (0.84,9.09) | 4.33 (1.51,12.46) * |
| Depression 1,2,3 | 2.64 (1.05,6.61) * | 4.40 (1.39,13.96) * | 4.16 (1.51,11.44) * |
| Current PTSD [N = 91] | 0.86 (0.29, 2.51) | 0.49 (0.09, 2.69) | 1.71 (0.57, 5.13) |
| Chemical sensitivity 1 | 2.62 (0.83,8.27) | 3.50 (0.95,12.85) | 8.17 (2.58,25.83) * |
| Chronic Fatigue Syndrome 1,2 | 5.17 (1.96,13.65) * | 2.69 (0.85,8.48) | 9.13 (3.05,27.35) * |
| Irritable Bowel Syndrome 1,2 | 4.71 (1.82,12.22) * | 1.71 (0.55,5.37) | 4.31 (1.56,11.88) * |
| Other GI disorders 1 | 1.46 (0.55,3.87) | 1.12 (0.33,3.81) | 3.40 (1.24,9.36) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janulewicz, P.; Krengel, M.; Quinn, E.; Heeren, T.; Toomey, R.; Killiany, R.; Zundel, C.; Ajama, J.; O’Callaghan, J.; Steele, L.; et al. The Multiple Hit Hypothesis for Gulf War Illness: Self-Reported Chemical/Biological Weapons Exposure and Mild Traumatic Brain Injury. Brain Sci. 2018, 8, 198. https://doi.org/10.3390/brainsci8110198
Janulewicz P, Krengel M, Quinn E, Heeren T, Toomey R, Killiany R, Zundel C, Ajama J, O’Callaghan J, Steele L, et al. The Multiple Hit Hypothesis for Gulf War Illness: Self-Reported Chemical/Biological Weapons Exposure and Mild Traumatic Brain Injury. Brain Sciences. 2018; 8(11):198. https://doi.org/10.3390/brainsci8110198
Chicago/Turabian StyleJanulewicz, Patricia, Maxine Krengel, Emily Quinn, Timothy Heeren, Rosemary Toomey, Ronald Killiany, Clara Zundel, Joy Ajama, James O’Callaghan, Lea Steele, and et al. 2018. "The Multiple Hit Hypothesis for Gulf War Illness: Self-Reported Chemical/Biological Weapons Exposure and Mild Traumatic Brain Injury" Brain Sciences 8, no. 11: 198. https://doi.org/10.3390/brainsci8110198
APA StyleJanulewicz, P., Krengel, M., Quinn, E., Heeren, T., Toomey, R., Killiany, R., Zundel, C., Ajama, J., O’Callaghan, J., Steele, L., Klimas, N., & Sullivan, K. (2018). The Multiple Hit Hypothesis for Gulf War Illness: Self-Reported Chemical/Biological Weapons Exposure and Mild Traumatic Brain Injury. Brain Sciences, 8(11), 198. https://doi.org/10.3390/brainsci8110198