
The Effects of Augmented Reality Treadmill Walking on Cognitive Function, Body Composition, Physiological Responses, and Acceptability in Older Adults: A Randomized Controlled Trial

Abstract
1. Introduction
2. Materials and Methods
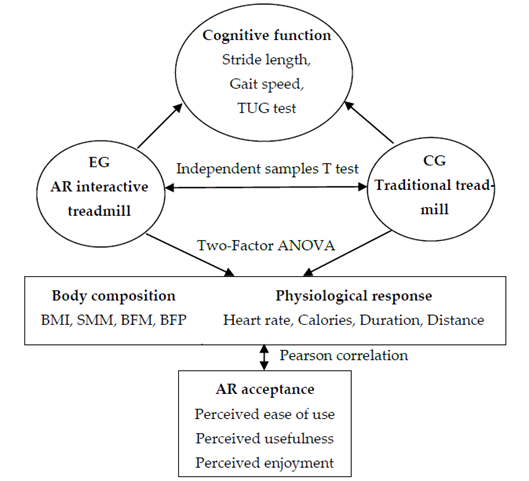
2.1. Research Framework
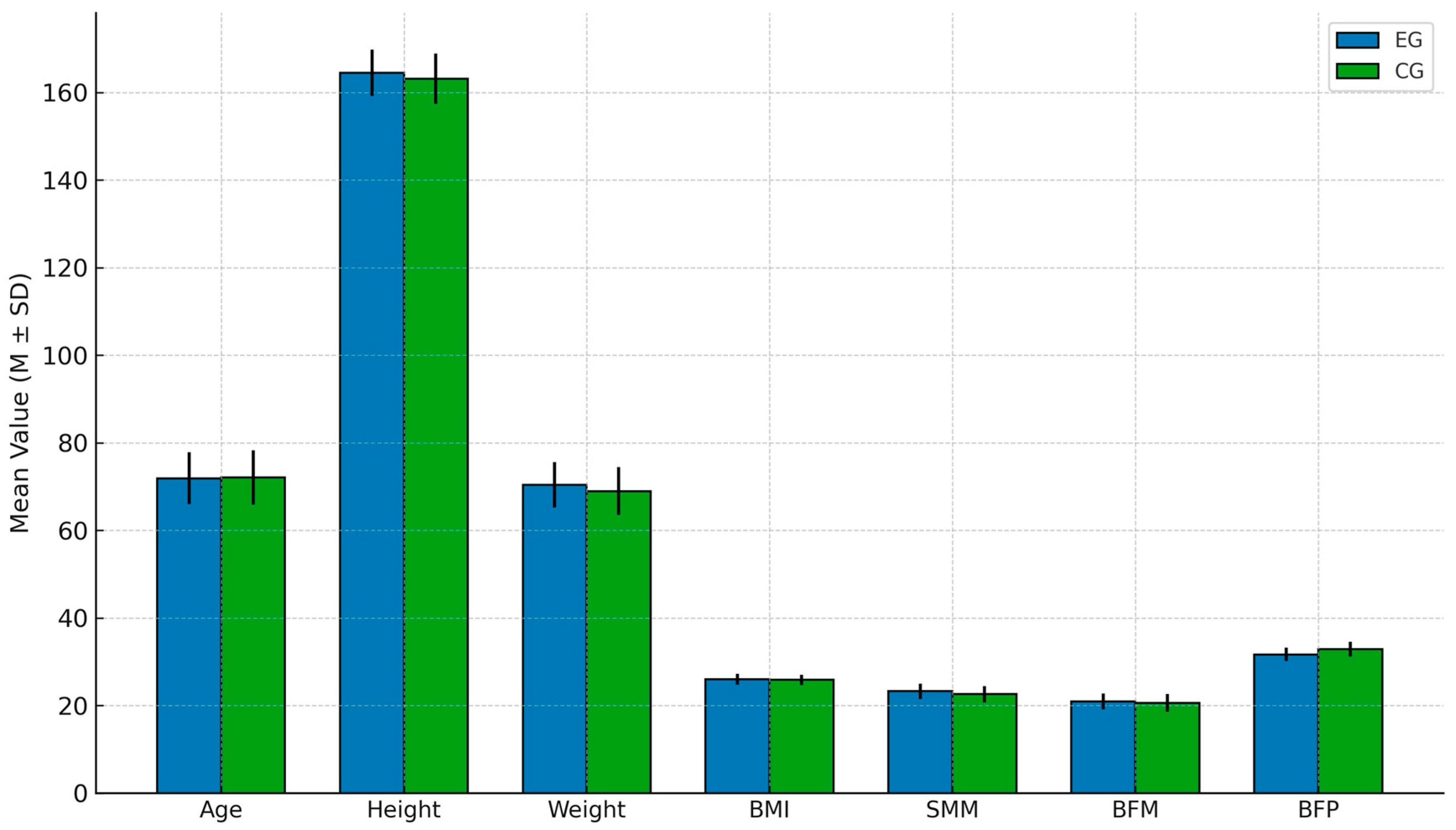
2.2. Participants
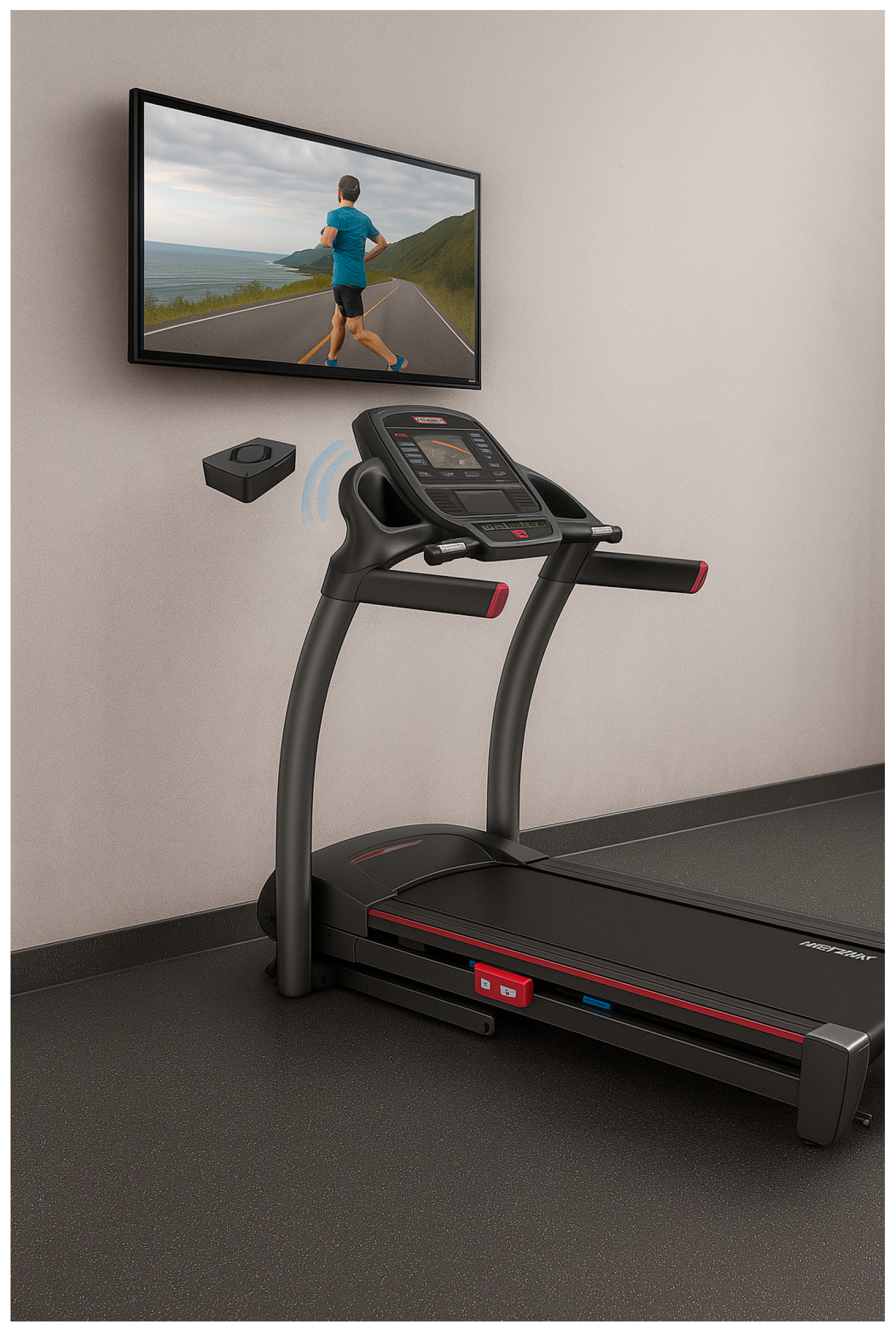
2.3. Intervention
2.4. Measurements
2.4.1. Assessment of Exercise and Cognitive Function in Older Adults
- Stride length: The 2-minute walk test (2MWT) was employed to estimate stride length (cm) by measuring walking distance and time [34]. The average stride length for healthy older adults is approximately 65 cm.
- Gait speed: Participants walked 30 m at a normal pace, and the time required was recorded to calculate gait speed (m/s) [35]. The normal walking speed range for healthy older adults is 1.1–1.5 m/s; if the speed falls below 1.0 m/s, it may indicate a decline in physical activity ability.
- Balance test (timed up and go test, TUG test): Participants stood up from a chair, walked 3 m, turned around, and returned to sit down, with completion time recorded [36]. If the test took more than 20 s, it could suggest balance issues.
2.4.2. Pre- and Post-Test Measurement of Body Composition
2.4.3. Assessment of Physiological Responses
2.4.4. AR Acceptance Scale
2.5. Control Variables
2.6. Statistical Analysis
3. Results
3.1. Effects on Cognitive Function in Older Adults
3.2. Effects of Treadmill Walking Training on Body Composition in Older Adults
3.3. Effects of Treadmill Walking Training on Physiological Responses in Older Adults
3.4. Analysis of the AR Acceptance Scale
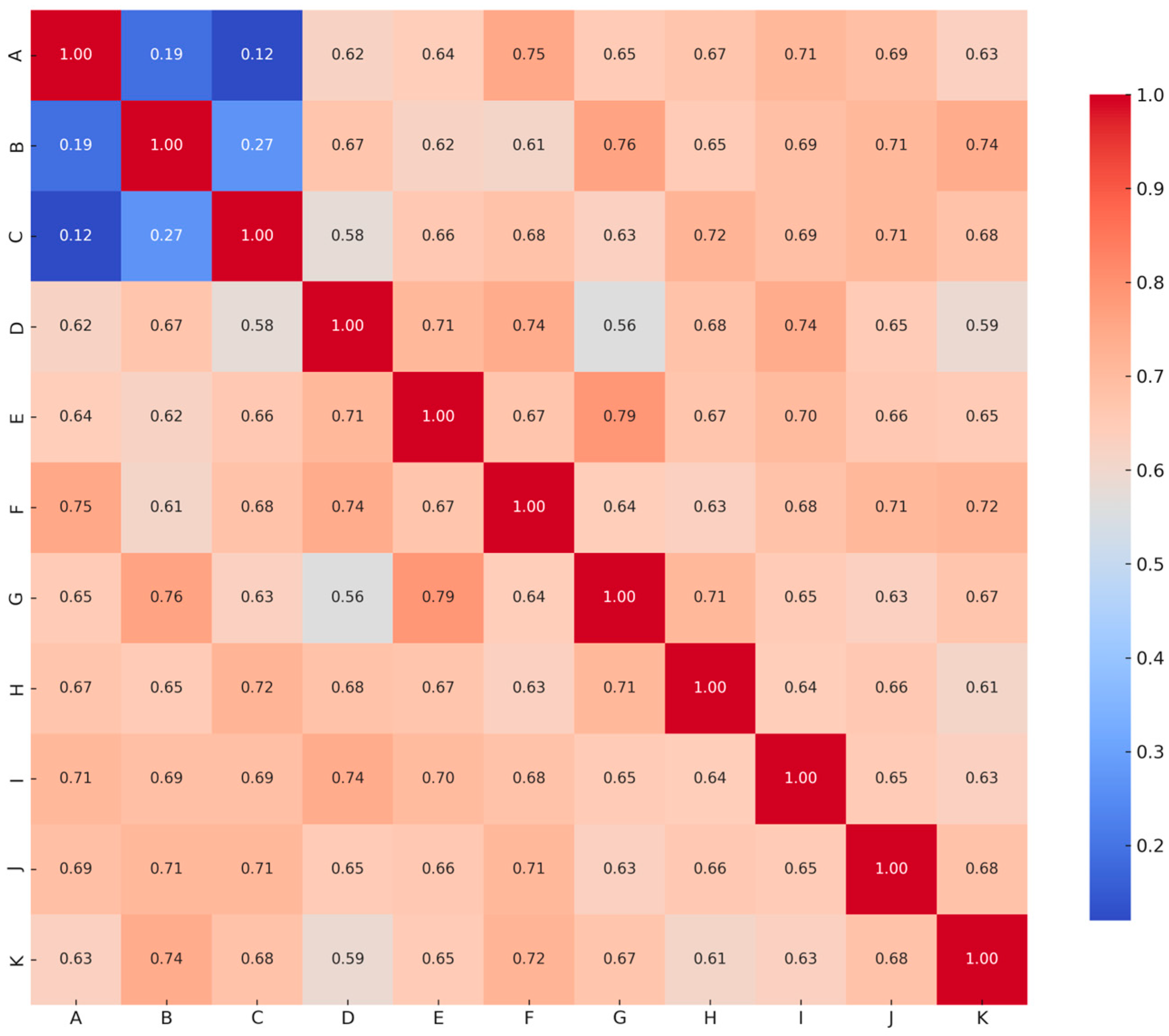
3.5. Correlation Analysis Between Post-Test Body Composition, Physiological Responses, and AR Acceptance in the Experimental Group
4. Discussion
4.1. AR Treadmill Walking Training and Cognitive Function
4.2. AR Treadmill Walking Training Improves Body Composition and Physiological Responses
4.3. Older Adults’ Acceptance of AR
4.4. Future Prospects
4.5. Research Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chia, F.; Huang, W.Y.; Huang, H.; Wu, C.E. Promoting Healthy Behaviors in Older Adults to Optimize Health-Promoting Lifestyle: An Intervention Study. Int. J. Environ. Res. Public Health 2023, 20, 1628. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Soh, K.G.; Chan, Y.M.; Soh, K.L.; Bai, X.R.; Deng, N.N.; Liu, H.G. Effects of physical exercise on physical and mental health in older adults with gait disorders: A systematic review. Geriatr. Nurs. 2025, 63, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Zhang, Y.; Li, S. The impact of mind-body exercise on the quality of life in older adults: The chain mediation effect of perceived social support and psychological resilience. Front. Public Health 2024, 12, 1446295. [Google Scholar] [CrossRef] [PubMed]
- Reljić, V.; Milenković, I.; Dudić, S.; Šulc, J.; Bajči, B. Augmented Reality Applications in Industry 4.0 Environment. Appl. Sci. 2021, 11, 5592. [Google Scholar] [CrossRef]
- Fernández-Moyano, J.A.; Remolar, I.; Gómez-Cambronero, Á. Augmented Reality’s Impact in Industry—A Scoping Review. Appl. Sci. 2025, 15, 2415. [Google Scholar] [CrossRef]
- Denche-Zamorano, A.; Rodriguez-Redondo, Y.; Barrios-Fernandez, S.; Mendoza-Muñoz, M.; Castillo-Paredes, A.; Rojo-Ramos, J.; Garcia-Gordillo, M.A.; Adsuar, J.C. Rehabilitation Is the Main Topic in Virtual and Augmented Reality and Physical Activity Research: A Bibliometric Analysis. Sensors 2023, 23, 2987. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-Y.; Lee, D.-Y.; Hong, J.-H.; Kim, J.-S.; Kim, S.-G.; Seo, Y.-G.; Yu, J.-H. Effects of Augmented Reality-Based Dual-Task Program on Physical Ability by Cognitive Stage with Developmental Disabilities. Healthcare 2022, 10, 2067. [Google Scholar] [CrossRef] [PubMed]
- Parekh, P.; Patel, S.; Patel, N.; Shah, M. Systematic review and meta-analysis of augmented reality in medicine, retail, and games. Vis. Comput. Ind. Biomed. Art 2020, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- Baragash, R.; Aldowah, H.; Ghazal, S. Virtual and augmented reality applications to improve older adults’ quality of life: A systematic mapping review and future directions. Digit. Health 2022, 8, 205520762211320. [Google Scholar] [CrossRef] [PubMed]
- Quigley, A.; MacKay-Lyons, M.; Eskes, G. Effects of Exercise on Cognitive Performance in Older Adults: A Narrative Review of the Evidence, Possible Biological Mechanisms, and Recommendations for Exercise Prescription. J. Aging Res. 2020, 2020, 1407896. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; West, D.; Pellegrini, C.; Wei, J.; Wilcox, S.; Neils-Strunjas, J.; Rudisill, A.C.; Friedman, D.B.; Marquez, D.X.; Dzwierzynski, J.; et al. Walking Interventions and Cognitive Health in Older Adults: A Systematic Review of Randomized Controlled Trials. Am. J. Health Promot. 2025, 31, 8901171251328858. [Google Scholar] [CrossRef] [PubMed]
- Prince, J.B.; Davis, H.L.; Tan, J.; Muller-Townsend, K.; Markovic, S.; Lewis, D.M.G.; Hastie, B.; Thompson, M.B.; Drummond, P.D.; Fujiyama, H.; et al. Cognitive and neuroscientific perspectives of healthy ageing. Neurosci. Biobehav. Rev. 2024, 161, 105649. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Murphy, K.; Andrews, G. Immediate and long-term efficacy of executive functions cognitive training in older adults: A systematic review and meta-analysis. Psychol. Bull. 2019, 145, 698–733. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-García, J.D.; Ortega-Gómez, S.; Martínez-Amat, A.; Álvarez-Salvago, F. Associations of Balance, Strength, and Gait Speed with Cognitive Function in Older Individuals over 60 Years: A Cross-Sectional Study. Appl. Sci. 2024, 14, 1500. [Google Scholar] [CrossRef]
- Xiao, T.; Yang, L.; Smith, L.; Loprinzi, P.D.; Veronese, N.; Yao, J.; Zhang, Z.; Yu, J.J. Correlation Between Cognition and Balance Among Middle-Aged and Older Adults Observed Through a Tai Chi Intervention Program. Front. Psychol. 2020, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Valkanova, V.; Esser, P.; Demnitz, N.; Sexton, C.E.; Zsoldos, E.; Mahmood, A.; Griffanti, L.; Kivimäki, M.; Singh-Manoux, A.; Dawes, H.; et al. Association between gait and cognition in an elderly population based sample. Gait Posture 2018, 65, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Adam, C.E.; Fitzpatrick, A.L.; Leary, C.S.; Hajat, A.; Ilango, S.D.; Park, C.; Phelan, E.A.; Semmens, E.O. Change in gait speed and fall risk among community-dwelling older adults with and without mild cognitive impairment: A retrospective cohort analysis. BMC Geriatr. 2023, 23, 328. [Google Scholar] [CrossRef] [PubMed]
- Anifa, N.; Sanaji, S. Augmented Reality Users: The Effect of Perceived Ease of Use, Perceived Usefulness, and Customer Experience on Repurchase Intention. J. Bus. Manag. Rev. 2022, 3, 252–274. [Google Scholar] [CrossRef]
- Cavalcante, D.; Fonseca, G.; Joaquim, S.; Simões, S. Usability and Applications of Virtual and Augmented Reality in Older Adults; IGI Global: Hershey, PA, USA, 2022; pp. 261–280. [Google Scholar]
- Derby, J.L.; Chaparro, B.S. Use of Augmented Reality by Older Adults. In Human Aspects of IT for the Aged Population. Technologies, Design and User Experience; Springer: Cham, Switzerland, 2020; pp. 125–134. [Google Scholar]
- Maswadi, K.; Ghani, N.; Hamid, S. Factors influencing the elderly’s behavioural intention to use smart home technologies in Saudi Arabia. PLoS ONE 2022, 17, e0272525. [Google Scholar] [CrossRef] [PubMed]
- Fuller, D.; Colwell, E.; Low, J.; Orychock, K.; Tobin, M.A.; Simango, B.; Buote, R.; Van Heerden, D.; Luan, H.; Cullen, K.; et al. Reliability and Validity of Commercially Available Wearable Devices for Measuring Steps, Energy Expenditure, and Heart Rate: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e18694. [Google Scholar] [CrossRef] [PubMed]
- Villagran-Vizcarra, D.C.; Luviano-Cruz, D.; Pérez-Domínguez, L.A.; Méndez-González, L.C.; Garcia-Luna, F. Applications Analyses, Challenges and Development of Augmented Reality in Education, Industry, Marketing, Medicine, and Entertainment. Appl. Sci. 2023, 13, 2766. [Google Scholar] [CrossRef]
- Wild, F.; Klemke, R.; Lefrere, P.; Fominykh, M.; Kuula, T. Technology Acceptance of Augmented Reality and Wearable Technologies; Springer: Cham, Switzerland, 2017; pp. 129–141. [Google Scholar]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Memon, M.; Ting, H.; Cheah, J.-H.; Ramayah, T.; Chuah, F.; Cham, T.-H. Sample Size for Survey Research: Review and Recommendations. J. Appl. Struct. Equ. Model. 2020, 4, i–xx. [Google Scholar] [CrossRef] [PubMed]
- Yue, H. Quantile-Quantile Plot Compared with Stablized Probability Plot in Figure on the Distribution of the Test Research. Am. J. Appl. Math. 2016, 4, 110. [Google Scholar] [CrossRef]
- Martínez-Mesa, J.; González-Chica, D.A.; Bastos, J.L.; Bonamigo, R.R.; Duquia, R.P. Sample size: How many participants do I need in my research? An. Bras. Dermatol. 2014, 89, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Busetto, L.; Carraça, E.V.; Dicker, D.; Encantado, J.; Ermolao, A.; et al. Effect of exercise training on weight loss, body composition changes, and weight maintenance in adults with overweight or obesity: An overview of 12 systematic reviews and 149 studies. Obes. Rev. 2021, 22 (Suppl. 4), e13256. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Kafy, E.M.; Alayat, M.S.; Subahi, M.S.; Badghish, M.S. C-Mill Virtual Reality/Augmented Reality Treadmill Training for Reducing Risk of Fall in the Elderly: A Randomized Controlled Trial. Games Health J. 2024, 13, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-W.; Lin, C.-M.; Yen, C.-W.; Yang, C.-C.; Tanaka, T.; Guo, L.-Y. The Effect of Walking Backward on a Treadmill on Balance, Speed of Walking and Cardiopulmonary Fitness for Patients with Chronic Stroke: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 2376. [Google Scholar] [CrossRef] [PubMed]
- Torre, M.M.; Carrubba, C.; Langeard, A.; Hugues, N.; Laurin, J.; Temprado, J.-J. Is an 8-Week Regimen of Nordic Walking Training Sufficient to Benefit Cognitive Performance in Healthy Older Adults? A Pilot Study. J. Clin. Med. 2024, 13, 1235. [Google Scholar] [CrossRef] [PubMed]
- Dalton, C.; Nantel, J. Nordic Walking Improves Postural Alignment and Leads to a More Normal Gait Pattern Following Weeks of Training: A Pilot Study. J. Aging Phys. Act. 2016, 24, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Virto, N.; Río, X.; Muñoz, I.; Méndez-Zorrilla, A.; García-Zapirain, B. Gait speed in older adults: Exploring the impact of functional, physical and social factors. Retos 2024, 61, 552–566. [Google Scholar] [CrossRef]
- Soto-Varela, A.; Rossi-Izquierdo, M.; Del-Río-Valeiras, M.; Faraldo-García, A.; Vaamonde-Sánchez-Andrade, I.; Lirola-Delgado, A.; Santos-Pérez, S. Modified Timed Up and Go Test for Tendency to Fall and Balance Assessment in Elderly Patients with Gait Instability. Front. Neurol. 2020, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.C. Bioelectrical impedance analysis for body composition assessment: Reflections on accuracy, clinical utility, and standardisation. Eur. J. Clin. Nutr. 2019, 73, 194–199. [Google Scholar] [CrossRef]
- Newman, A.B.; Visser, M.; Kritchevsky, S.B.; Simonsick, E.; Cawthon, P.M.; Harris, T.B. The Health, Aging, and Body Composition (Health ABC) Study-Ground-Breaking Science for 25 Years and Counting. J. Gerontol. A Biol. Sci. Med. Sci. 2023, 78, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Dooley, E.E.; Golaszewski, N.M.; Bartholomew, J.B. Estimating Accuracy at Exercise Intensities: A Comparative Study of Self-Monitoring Heart Rate and Physical Activity Wearable Devices. JMIR Mhealth Uhealth 2017, 5, e34. [Google Scholar] [CrossRef] [PubMed]
- Ustun, A.; Karaoğlan Yılmaz, F.G.; Yılmaz, R.; Ceylan, M.; Uzun, O. Development of UTAUT-based augmented reality acceptance scale: A validity and reliability study. Educ. Inf. Technol. 2023, 29, 11533–11554. [Google Scholar] [CrossRef]
- Cabero-Almenara, J.; Barroso-Osuna, J.; Llorente-Cejudo, C.; Fernández Martínez, M.d.M. Educational Uses of Augmented Reality (AR): Experiences in Educational Science. Sustainability 2019, 11, 4990. [Google Scholar] [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Amirzadeh, S.; Rasouli, D.; Dargahi, H. Assessment of validity and reliability of the feedback quality instrument. BMC Res. Notes 2024, 17, 227. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.W.; Cooper-Thomas, H.D.; Lau, R.S.; Wang, L.C. Reporting reliability, convergent and discriminant validity with structural equation modeling: A review and best-practice recommendations. Asia Pac. J. Manag. 2024, 41, 745–783. [Google Scholar] [CrossRef]
- Kelley, K.; Rausch, J.R. Sample size planning for the standardized mean difference: Accuracy in parameter estimation via narrow confidence intervals. Psychol. Methods 2006, 11, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Lagisz, M.; Yang, Y.; Drobniak, S.M. Finding the right power balance: Better study design and collaboration can reduce dependence on statistical power. PLoS Biol. 2024, 22, e3002423. [Google Scholar] [CrossRef] [PubMed]
- Blomqvist, S.; Seipel, S.; Engström, M. Using augmented reality technology for balance training in the older adults: A feasibility pilot study. BMC Geriatr. 2021, 21, 144. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.; Si, Y.; Guo, C.; Wang, P.; Li, S.; Wang, J.; Wang, X. The prediction model of fall risk for the elderly based on gait analysis. BMC Public Health 2024, 24, 2206. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Xu, X.; Wang, R.; Li, F.; Wang, Y.; Wang, L. Validity and reliability of inertial measurement units on gait, static balance and functional mobility performance among community-dwelling older adults: A systematic review and meta-analysis. EFORT Open Rev. 2025, 10, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Rochester, L.; Reelick, M.; Nieuwhof, F.; Pelosin, E.; Abbruzzese, G.; Dockx, K.; Nieuwboer, A.; Hausdorff, J.M. V-TIME: A treadmill training program augmented by virtual reality to decrease fall risk in older adults: Study design of a randomized controlled trial. BMC Neurol. 2013, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Park, K.; Choi, K.-H.; Lee, J. Mobile Augmented Reality Serious Game for Improving Old Adults’ Working Memory. Appl. Sci. 2021, 11, 7843. [Google Scholar] [CrossRef]
- Quandt, M.; Freitag, M. A Systematic Review of User Acceptance in Industrial Augmented Reality. Front. Educ. 2021, 6, 700760. [Google Scholar] [CrossRef]
- Goumopoulos, C.; Drakakis, E.; Gklavakis, D. Feasibility and Acceptance of Augmented and Virtual Reality Exergames to Train Motor and Cognitive Skills of Elderly. Computers 2023, 12, 52. [Google Scholar] [CrossRef]
- Korn, O.; Buchweitz, L.; Rees, A.; Bieber, G.; Werner, C.; Hauer, K. Using Augmented Reality and Gamification to Empower Rehabilitation Activities and Elderly Persons. A Study Applying Design Thinking; Springer: Cham, Switzerland, 2019; pp. 219–229. [Google Scholar]
- Xu, W.; Liang, H.-N.; Yu, K.; Wen, S.; Baghaei, N.; Tu, H. Acceptance of Virtual Reality Exergames Among Chinese Older Adults. Int. J. Hum.-Comput. Interact. 2022, 39, 1134–1148. [Google Scholar] [CrossRef]
- Simon, J. Investigating the Use of Augmented Reality to Enhance the Indoor Running Experience on a Treadmill. Interdiscip. Descr. Complex Syst. 2023, 21, 341–350. [Google Scholar] [CrossRef]
- Xie, B.; Liu, B.; Chen, X.; Chuan, F.; Liao, K.; Mei, M.; Li, R.; Zhou, B. ALM adjusted by BMI or weight predicts adverse health outcomes in middle-aged and elderly patients with type 2 diabetes. Sci. Rep. 2025, 15, 7963. [Google Scholar] [CrossRef] [PubMed]
- Bichay, A.A.; Ramírez, J.M.; Núñez, V.M.; Lancho, C.; Poblador, M.S.; Lancho, J.L. Efficacy of treadmill exercises on arterial blood oxygenation, oxygen consumption and walking distance in healthy elderly people: A controlled trial. BMC Geriatr. 2016, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- Doré, B.; Gaudreault, A.; Everard, G.; Ayena, J.C.; Abboud, A.; Robitaille, N.; Batcho, C.S. Acceptability, Feasibility, and Effectiveness of Immersive Virtual Technologies to Promote Exercise in Older Adults: A Systematic Review and Meta-Analysis. Sensors 2023, 23, 2506. [Google Scholar] [CrossRef] [PubMed]
- Achilleos, A.; Mettouris, C.; Yeratziotis, A.; Starosta-Sztuczka, J.; Moza, S.; Hadjicosta, A.; Georgiou, S.; Theodorou, C.; Loizou, C.T.; Pecyna, K.; et al. Lessons Learned from Older Adults Fusing of an Augmented Reality, Assisted Living and Social Interaction Platform. SN Comput. Sci. 2023, 4, 378. [Google Scholar] [CrossRef] [PubMed]
- Mahalil, I.; Yusof, A.; Ibrahim, N. A literature review on the usage of Technology Acceptance Model for analysing a virtual reality’s cycling sport applications with enhanced realism fidelity. In Proceedings of the 2020 8th International Conference on Information Technology and Multimedia (ICIMU), Selangor, Malaysia, 24–26 August 2020; pp. 237–242. [Google Scholar]
- Carroll, J.; Hopper, L.; Farrelly, A.; Lombard-Vance, R.; Bamidis, P.; Konstantinidis, E. A Scoping Review of Augmented/ Virtual Reality Health and Wellbeing Interventions for Older Adults: Redefining Immersive Virtual Reality. Front. Virtual Real. 2021, 2, 655338. [Google Scholar] [CrossRef]
- Lee, H.S.; Lee, J. Applying Artificial Intelligence in Physical Education and Future Perspectives. Sustainability 2021, 13, 351. [Google Scholar] [CrossRef]
- Sheehy, L.; Bharadwaj, L.; Nissen, K.A.; Estey, J.L. Non-Immersive Virtual Reality Exercise Can Increase Exercise in Older Adults Living in the Community and in Long-Term Care: A Randomized Controlled Trial. Clin. Interv. Aging 2025, 20, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yuan, Z. A virtual gym in your pocket: The influence of augmented reality exercise app characteristics on user’s continuance intention. Virtual Real. 2024, 28, 54. [Google Scholar] [CrossRef]
- Li, J. Beyond Sight: Enhancing Augmented Reality Interactivity with Audio-Based and Non-Visual Interfaces. Appl. Sci. 2024, 14, 4881. [Google Scholar] [CrossRef]
- Syed, T.A.; Siddiqui, M.S.; Abdullah, H.B.; Jan, S.; Namoun, A.; Alzahrani, A.; Nadeem, A.; Alkhodre, A.B. In-Depth Review of Augmented Reality: Tracking Technologies, Development Tools, AR Displays, Collaborative AR, and Security Concerns. Sensors 2023, 23, 146. [Google Scholar] [CrossRef] [PubMed]
- Soltani, P.; Morice, A.H.P. Augmented reality tools for sports education and training. Comput. Educ. 2020, 155, 103923. [Google Scholar] [CrossRef]
- Piqueras-Sola, B.; Cortés-Martín, J.; Rodríguez-Blanque, R.; Menor-Rodríguez, M.J.; Mellado-García, E.; Merino Lobato, C.; Sánchez-García, J.C. Systematic Review on the Impact of Mobile Applications with Augmented Reality to Improve Health. Bioengineering 2024, 11, 622. [Google Scholar] [CrossRef] [PubMed]
- Cossich, V.R.A.; Carlgren, D.; Holash, R.J.; Katz, L. Technological Breakthroughs in Sport: Current Practice and Future Potential of Artificial Intelligence, Virtual Reality, Augmented Reality, and Modern Data Visualization in Performance Analysis. Appl. Sci. 2023, 13, 12965. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | EG (n = 30) M ± SD | CG (n = 30) M ± SD | t-Value | p-Value |
|---|---|---|---|---|
| Age | 71.9 ± 5.93 | 72.1 ± 6.23 | −0.117 | 0.907 |
| Height | 164.5 ± 5.26 | 163.2 ± 5.75 | 1.050 | 0.303 |
| Weight | 70.4 ± 5.16 | 69.0 ± 5.45 | 0.975 | 0.338 |
| BMI | 26.0 ± 1.25 | 25.9 ± 1.18 | 0.321 | 0.751 |
| SMM | 23.3 ± 1.74 | 22.6 ± 1.86 | 1.356 | 0.185 |
| BFM | 20.9 ± 1.81 | 20.6 ± 2.06 | 0.565 | 0.576 |
| BFP | 31.7 ± 1.53 | 32.9 ± 1.67 | −0.484 | 0.632 |
| Variable | EG (n = 30) M ± SD | CG (n = 30) M ± SD | F-Value Pre-Test and Post-Test | η2 | F-Value Pre- and Post-Tests * Two Groups | η2 | |
|---|---|---|---|---|---|---|---|
| Stride length | Pre | 59.43 ± 2.69 | 60.20 ± 3.15 | 305.40 * | 0.84 | 147.62 * | 0.72 |
| Post | 65.20 ± 3.43 | 61.24 ± 3.18 | |||||
| Gait speed | Pre | 1.00 ± 0.09 | 0.99 ± 0.12 | 664.51 * | 0.92 | 217.70 * | 0.79 |
| Post | 1.19 ± 0.11 | 1.04 ± 0.12 | |||||
| TUG | Pre | 12.81 ± 2.05 | 13.57 ± 1.56 | 296.62 * | 0.84 | 166.97 * | 0.74 |
| Post | 10.03 ± 2.46 | 13.17 ± 1.58 | |||||
| Variable | EG (n = 30) M ± SD | CG (n = 30) M ± SD | F-Value Pre-Test and Post-Test | η2 | F-Value Pre- and Post-Tests * Two Groups | η2 | |
|---|---|---|---|---|---|---|---|
| Weight | Pre | 70.40 ± 5.16 | 68.99 ± 5.45 | 587.35 * | 0.91 | 358.78 * | 0.86 |
| Post | 66.92 ± 4.89 | 68.56 ± 5.44 | |||||
| BMI | Pre | 25.99 ± 1.25 | 25.89 ± 1.18 | 680.11 * | 0.92 | 409.58 * | 0.88 |
| Post | 24.71 ± 1.22 | 25.74 ± 1.19 | |||||
| SMM | Pre | 23.27 ± 1.74 | 22.65 ± 1.86 | 534.48 * | 0.90 | 172.51 * | 0.75 |
| Post | 24.27 ± 1.86 | 22.92 ± 1.89 | |||||
| BFM | Pre | 20.93 ± 1.81 | 20.62 ± 2.06 | 1052.62 * | 0.95 | 482.27 * | 0.89 |
| Post | 18.57 ± 1.74 | 20.16 ± 2.08 | |||||
| BFP | Pre | 31.65 ± 1.53 | 31.87 ± 1.67 | 340.17 * | 0.85 | 210.61 * | 0.78 |
| Post | 28.35 ± 2.03 | 31.47 ± 1.77 | |||||
| Variable | EG (n = 30) M ± SD | CG (n = 30) M ± SD | df | t-Value | p-Value |
|---|---|---|---|---|---|
| Heart rate (times) | 120 ± 6.45 | 115 ± 5.83 | 58 | 3.35 * | 0.001 |
| Calories (kcal) | 209 ± 20.03 | 188 ± 21.07 | 58 | 4.04 * | 0.000 |
| Duration (min) | 32.2 ± 2.70 | 23.4 ± 2.46 | 58 | 13.30 * | 0.000 |
| Distance (km) | 2.59 ± 0.21 | 1.63 ± 0.26 | 58 | 15.77 * | 0.000 |
| Factors | Items | M ± SD | F | LSD |
|---|---|---|---|---|
| 1. Perceived Usefulness | 1. Using an AR treadmill enhances exercise performance. | 4.43 ± 0.50 | 4.19 * | 3 > 2 > 1 |
| 2. Using an AR treadmill aids physiological monitoring. | 4.80 ± 0.40 | |||
| 3. Using an AR treadmill provides physiological data. | 4.83 ± 0.37 | |||
| 4. Using an AR treadmill increases exercise intensity demands. | 4.30 ± 0.59 | |||
| 2. Perceived Ease of Use | 5. Using an AR treadmill is more convenient. | 4.73 ± 0.44 | ||
| 6. Using an AR treadmill is easy to operate. | 4.77 ± 0.42 | |||
| 3. Attitude and Behavioral Intention | 7. Using an AR treadmill motivates participation. | 4.87 ± 0.34 | ||
| 8. Using an AR treadmill makes exercise enjoyable. | 4.83 ± 0.37 | |||
| 9. Using an AR treadmill allows for both play and exercise. | 4.90 ± 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.-Y.; Pan, H.-W.; Wu, C.-E. The Effects of Augmented Reality Treadmill Walking on Cognitive Function, Body Composition, Physiological Responses, and Acceptability in Older Adults: A Randomized Controlled Trial. Brain Sci. 2025, 15, 781. https://doi.org/10.3390/brainsci15080781
Huang W-Y, Pan H-W, Wu C-E. The Effects of Augmented Reality Treadmill Walking on Cognitive Function, Body Composition, Physiological Responses, and Acceptability in Older Adults: A Randomized Controlled Trial. Brain Sciences. 2025; 15(8):781. https://doi.org/10.3390/brainsci15080781
Chicago/Turabian StyleHuang, Wei-Yang, Huei-Wen Pan, and Cheng-En Wu. 2025. "The Effects of Augmented Reality Treadmill Walking on Cognitive Function, Body Composition, Physiological Responses, and Acceptability in Older Adults: A Randomized Controlled Trial" Brain Sciences 15, no. 8: 781. https://doi.org/10.3390/brainsci15080781
APA StyleHuang, W.-Y., Pan, H.-W., & Wu, C.-E. (2025). The Effects of Augmented Reality Treadmill Walking on Cognitive Function, Body Composition, Physiological Responses, and Acceptability in Older Adults: A Randomized Controlled Trial. Brain Sciences, 15(8), 781. https://doi.org/10.3390/brainsci15080781