
Relationship Between Nutritional Indexes and Clinical Outcomes in Stroke Patients Undergoing Mechanical Thrombectomy



Abstract
1. Introduction
2. Materials and Methods
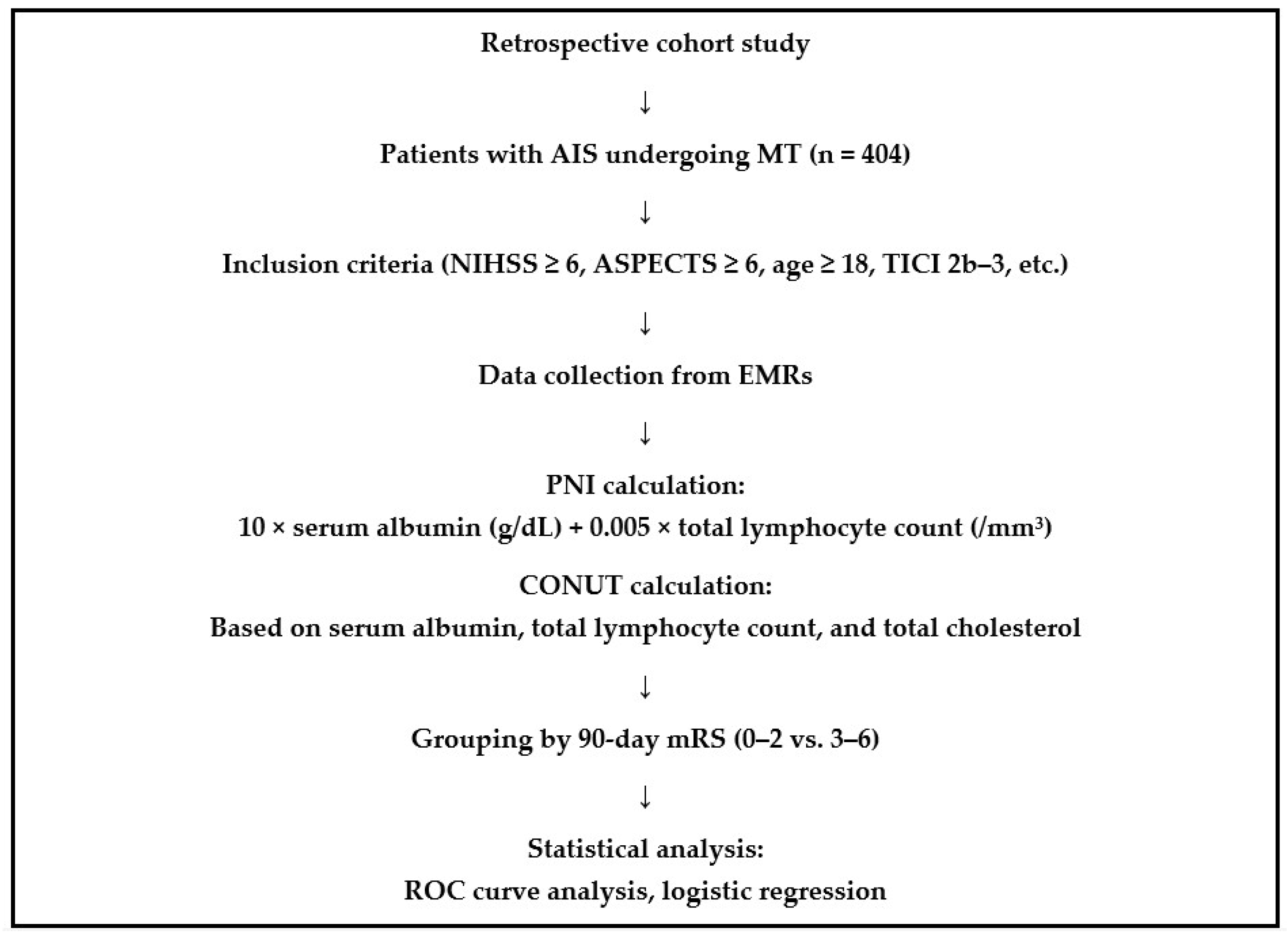
2.1. Study Design
2.2. Inclusion Criteria
- Diagnosed with AIS due to large artery occlusion, confirmed by cranial CT angiography, cranial MRI angiography, or digital subtraction angiography;
- Presented to the hospital within 24 h of symptom onset;
- NIHSS score ≥ 6 on admission;
- ASPECTS ≥ 6;
- No evidence of intracranial hemorrhage on initial CT or MRI;
- Underwent mechanical thrombectomy within 6 h of symptom onset, or between 6 and 24 h in accordance with the eligibility criteria of the DAWN or DEFUSE trials;
- Achieved successful reperfusion, defined as a post-thrombectomy Thrombolysis in Cerebral Infarction (TICI) score of 2b-3;
- Pre-stroke mRS score between 0 and 2;
- Age 18 years or older.
2.3. Exclusion Criteria
- Patients with incomplete clinical or laboratory data
2.4. Data Collection
2.5. Calculation of Nutritional Indices
2.5.1. PNI Calculation
2.5.2. CONUT Calculation
2.6. Clinical Outcome Assessment
2.7. Statistical Analysis
3. Results
3.1. Clinical Outcomes and Baseline Characteristics
3.2. Stroke Severity, Imaging Scores, and Procedural Times
3.3. Stroke Etiology and Vascular Occlusion Sites
3.4. Recanalization and Procedure Parameters
3.5. Laboratory Findings and Nutritional Indices
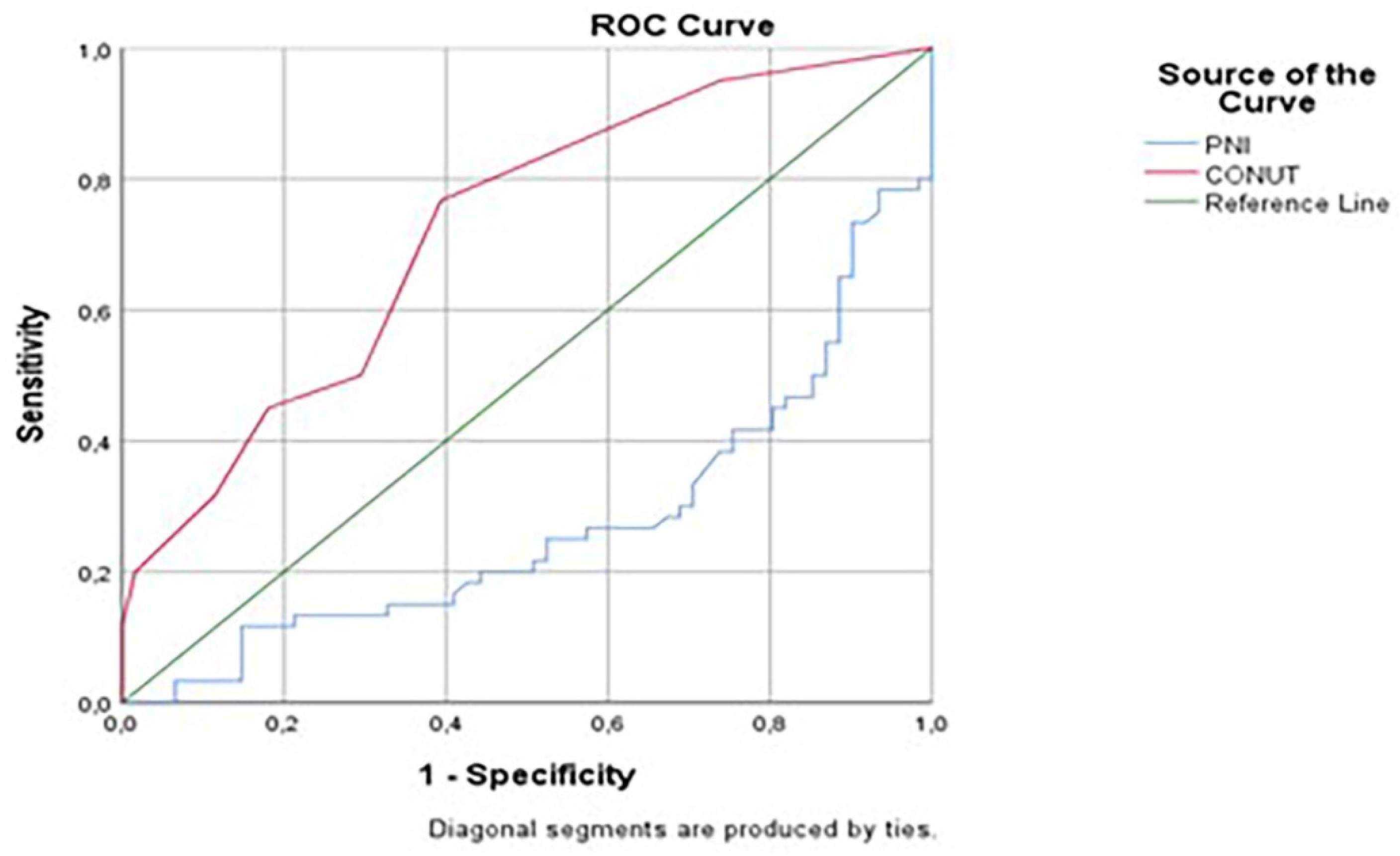
3.6. Predictive Value of Nutritional Indices: ROC Analysis
3.7. Independent Predictors of Clinical Outcome: Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Stroke Collaborators. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized evaluation of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Román, L.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 hours of symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef]
- Berkhemer, O.A.; Fransen, P.S.; Beumer, D.; Van Den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A randomized trial of intra-arterial therapy for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef]
- Lindsberg, P.J.; Sairanen, T.; Nagel, S.; Salonen, O.; Silvennoinen, H.; Strbian, D. Recanalization treatments in basilar artery occlusion—Systematic analysis. Eur. Stroke J. 2016, 1, 41–50. [Google Scholar] [CrossRef]
- Hussein, H.M.; Saleem, M.A.; Qureshi, A.I. Rates and predictors of futile recanalization in patients undergoing endovascular treatment in a multicenter clinical trial. Neuroradiology 2018, 60, 557–563. [Google Scholar] [CrossRef]
- Kokura, Y.; Kimoto, K.; Okada, Y.; Kawakita, S. The Controlling Nutritional Status score as a functional prognostic marker in patients with acute stroke: A multicenter retrospective cohort study. Nutrition 2020, 79–80, 110889. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN Guidelines on Definitions and Terminology of Clinical Nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Serón-Arbeloa, C.; Labarta-Monzón, L.; Puzo-Foncillas, J.; Mallor-Bonet, T.; Lafita-López, A.; Bueno-Vidales, N.; Montoro-Huguet, M. Malnutrition Screening and Assessment. Nutrients 2022, 14, 2392. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.; Smith, T. Malnutrition: Causes and consequences. Clin. Med. 2010, 10, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Xiang, W.; Chen, X.; Ye, W.; Li, J.; Zhang, X.; Xie, D. Prognostic Nutritional Index for Predicting 3-Month Outcomes in Ischemic Stroke Patients Undergoing Thrombolysis. Front. Neurol. 2020, 11, 599. [Google Scholar] [CrossRef] [PubMed]
- Aliasghari, F.; Izadi, A.; Khalili, M.; Farhoudi, M.; Ahmadiyan, S.; Deljavan, R. Impact of Premorbid Malnutrition and Dysphagia on Ischemic Stroke Outcome in Elderly Patients: A Community-Based Study. J. Am. Coll. Nutr. 2019, 38, 318–326. [Google Scholar] [CrossRef]
- Cai, Z.M.; Wu, Y.Z.; Chen, H.M.; Feng, R.Q.; Liao, C.W.; Ye, S.L.; Liu, Z.P.; Zhang, M.M.; Zhu, B.L. Being at risk of malnutrition predicts poor outcomes at 3 months in acute ischemic stroke patients. Eur. J. Clin. Nutr. 2020, 74, 796–805. [Google Scholar] [CrossRef]
- Choi, H.; Jo, Y.J.; Sohn, M.K.; Lee, J.; Shin, Y.I.; Oh, G.J.; Lee, Y.S.; Joo, M.C.; Lee, S.Y.; Song, M.K.; et al. The significance of an initial controlling nutritional status score in predicting the functional outcome, complications, and mortality in a first-ever ischemic stroke. Nutrients 2024, 16, 3461. [Google Scholar] [CrossRef]
- Huppertz, V.; Guida, S.; Holdoway, A.; Strilciuc, S.; Baijens, L.; Schols, J.M.G.A.; van Helvoort, A.; Lansink, M.; Muresanu, D.F. Impaired Nutritional Condition After Stroke from the Hyperacute to the Chronic Phase: A Systematic Review and Meta-Analysis. Front. Neurol. 2022, 12, 780080. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef]
- Zhang, G.; Pan, Y.; Zhang, R.; Wang, M.; Meng, X.; Li, Z.; Li, H.; Wang, Y.; Zhao, X.; Liu, G.; et al. Prevalence and prognostic significance of malnutrition risk in patients with acute ischemic stroke: Results from the third china national stroke registry. Stroke 2022, 53, 111–119. [Google Scholar] [CrossRef]
- Lo Buglio, A.; Bellanti, F.; Capurso, C.; Vendemiale, G. Controlling Nutritional Status (CONUT) score as a predictive marker in hospitalized frail elderly patients. J. Pers. Med. 2023, 13, 1119. [Google Scholar] [CrossRef] [PubMed]
- Nakagomi, A.; Kohashi, K.; Morisawa, T.; Kosugi, M.; Endoh, I.; Kusama, Y.; Atarashi, H.; Shimizu, W. Nutritional status is associated with inflammation and predicts a poor outcome in patients with chronic heart failure. J. Atheroscler. Thromb. 2016, 23, 713–727. [Google Scholar] [CrossRef] [PubMed]
- Di Vincenzo, O.; D’Elia, L.; Ballarin, G.; Pasanisi, F.; Scalfi, L. Controlling Nutritional Status (CONUT) score and the risk of mortality or impaired physical function in stroke patients: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yang, H.; Lan, M.; Wei, H.; Chen, Y. The controlling nutritional status score and risk factors associated with malnutrition in patients with acute ischemic stroke. Front. Neurol. 2023, 14, 1067706. [Google Scholar] [CrossRef]
- Naito, H.; Nezu, T.; Hosomi, N.; Aoki, S.; Kinoshita, N.; Kuga, J.; Shimomura, R.; Araki, M.; Ueno, H.; Ochi, K.; et al. Controlling nutritional status score for predicting 3-mo functional outcome in acute ischemic stroke. Nutrition 2018, 55–56, 1–6. [Google Scholar] [CrossRef]
- Zhao, W.; An, Z.; Hong, Y.; Zhou, G.; Guo, J.; Zhang, Y.; Yang, Y.; Ning, X.; Wang, J. Low total cholesterol level is the independent predictor of poor outcomes in patients with acute ischemic stroke: A hospital-based prospective study. BMC Neurol. 2016, 16, 36. [Google Scholar] [CrossRef]
- Dirajlal-Fargo, S.; Kulkarni, M.; Bowman, E.; Shan, L.; Sattar, A.; Funderburg, N.; McComsey, G.A. Serum albumin is associated with higher inflammation and carotid atherosclerosis in treated human immunodeficiency virus infection. Open Forum Infect. Dis. 2018, 5, ofy291. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Elenkov, I.J.; Chrousos, G.P. Stress hormones, proinflammatory and antiinflammatory cytokines, and autoimmunity. Ann. N. Y. Acad. Sci. 2002, 966, 290–303. [Google Scholar] [CrossRef]
- Alawieh, A.; Vargas, J.; Fargen, K.M.; Langley, E.F.; Starke, R.M.; De Leacy, R.; Chatterjee, R.; Rai, A.; Dumont, T.; Kan, P.; et al. Impact of Procedure Time on Outcomes of Thrombectomy for Stroke. J. Am. Coll. Cardiol. 2019, 73, 879–890. [Google Scholar] [CrossRef]
- Perez-Vega, C.; Domingo, R.A.; Tripathi, S.; Ramos-Fresnedo, A.; Kashyap, S.; Quinones-Hinojosa, A.; Lin, M.P.; Fox, W.C.; Tawk, R.G. Influence of glucose levels on clinical outcome after mechanical thrombectomy for large-vessel occlusion: A systematic review and meta-analysis. J. Neurointerv. Surg. 2022, 14. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Favorable Outcome (N = 204) | Unfavorable Outcome (N = 200) | p-Value |
|---|---|---|---|
| Age, Median (IQR) | 71 (59.00–78.00) | 78 (71.25–84.00) | 0.001 * |
| Sex, n (%) | |||
| Female | 91 (44.6) | 108 (54.0) | 0.194 |
| Male | 113 (55.4) | 92 (46.0) | |
| Medical history, n (%) | |||
| Hypertension | 157 (77.0) | 163 (81.5) | 0.654 |
| Diabetes Mellitus | 63 (30.9) | 80 (40.0) | 0.346 |
| Atrial Fibrillation | 100 (49.0) | 110 (55.0) | 0.522 |
| Hyperlipidemia | 80 (39.2) | 70 (35.0) | 0.304 |
| Coronary Artery Disease | 97 (47.5) | 107 (53.5) | 0.587 |
| Heart Failure | 43 (21.1) | 47 (23.5) | 0.830 |
| Previous Stroke | 33 (16.2) | 50 (25.0) | 0.241 |
| Malignancy | 7 (3.3) | 7 (3.5) | 0.987 |
| Smoking | 63 (30.9) | 53 (26.5) | 0.689 |
| Alcohol | 20 (9.8) | 17 (8.5) | 0.744 |
| Clinical features | |||
| Intravenous Thrombolysis | 100 (49.01) | 85 (42.5) | 0.255 |
| NIHSS, Median (IQR) | 13 (10.00–17.50) | 17 (14.00–22.00) | 0.001 * |
| ASPECTS, Median (IQR) | 9 (9–10) | 7 (7–8) | 0.001 * |
| Symptom-to-Puncture Time (min), Median (IQR) | 240 (150.00–312.50) | 275 (200.00–360.00) | 0.106 |
| Puncture-to-Recanalization Time (min), Median (IQR) | 30.00 (25.00–50.00) | 47.50 (30.00–87.50) | 0.003 * |
| Stroke Type, n (%) | |||
| Cardioembolism | 114 (55.9) | 113 (56.5) | 0.305 |
| Large Artery Atherosclerosis | 40 (19.6) | 56 (28.0) | |
| Other | 50 (24.5) | 30 (15.0) | |
| Vascular Occlusion Site, n (%) | |||
| MCA M1 | 97 (47.5) | 100 (50.0) | 0.619 |
| MCA M2 | 30 (14.7) | 17 (8.5) | |
| ICA T/L | 20 (9.8) | 47 (23.5) | |
| Basilar | 27 (13.2) | 17 (8.5) | |
| PCA | 7 (3.3) | 0 (0) | |
| Tandem | 23 (11.3) | 20 (10.0) | |
| TICI Score, n (%) | |||
| 2b | 20 (9.8) | 63 (31.5) | 0.001 * |
| 2c | 47 (23.0) | 73 (36.5) | |
| 3 | 137 (67.2) | 63 (31.5) | |
| Thrombectomy Technique, n (%) | |||
| Solumbra | 147 (72.1) | 150 (75.0) | 0.736 |
| ADAPT | 30 (14.7) | 30 (15.0) | |
| Solumbra + ADAPT | 27 (13.2) | 20 (10.0) | |
| Number of Passes, Median (IQR) | 1 (1–2) | 2 (1–3) | 0.001 * |
| Parameter | Favorable Outcome (N = 204) | Unfavorable Outcome (N = 200) | p-Value |
|---|---|---|---|
| Glucose (mg/dL), Median (IQR) | 127.0 (114.0–155.5) | 154.0 (120.0–196.0) | 0.029 * |
| Creatinine (mg/dL), Median (IQR) | 0.82 (0.69–1.00) | 0.85 (0.68–1.27) | 0.469 |
| Hemoglobin (g/dL), Mean ± SD | 13.48 ± 2.33 | 12.70 ± 2.10 | 0.057 |
| LDL (mg/dL), Mean ± SD | 108.14 ± 30.94 | 98.61 ± 30.76 | 0.092 |
| Total Cholesterol (mg/dL), Mean ± SD | 171.77 ± 35.56 | 160.63 ± 36.71 | 0.093 |
| Serum Albumin (g/dL), Median (IQR) | 38 (36–40) | 36 (30–39) | 0.003 * |
| Lymphocytes (103/µL), Median (IQR) | 1.99 (1.28–3.30) | 1.29 (0.86–2.05) | 0.001 * |
| Prognostic Nutritional Index (PNI), Mean ± SD | 49.7 ± 7.75 | 42.8 ± 8.97 | 0.001 * |
| Controlling Nutritional Status (CONUT), Median (IQR) | 1 (1–3) | 2.5 (2–5) | 0.001 * |
| Variables | OR (95% CI) | p-Value |
|---|---|---|
| Admission NIHSS | 0.881 (0.807–0.962) | 0.005 * |
| ASPECT Score | 3.414 (2.022–5.764) | 0.001 * |
| Puncture-to-Recanalization Time | 1.007 (0.984–1.031) | 0.556 |
| Number of Passes | 0.460 (0.194–1.095) | 0.039 * |
| Glucose | 0.995 (0.985–1.006) | 0.387 |
| Age | 0.945 (0.901–0.991) | 0.020 * |
| CONUT Score | 0.728 (0.543–0.976) | 0.034 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ertuğrul, Ö.Z.; Karaaslan, F.; Yılmaz, R.; Tuncer, M.C. Relationship Between Nutritional Indexes and Clinical Outcomes in Stroke Patients Undergoing Mechanical Thrombectomy. Brain Sci. 2025, 15, 704. https://doi.org/10.3390/brainsci15070704
Ertuğrul ÖZ, Karaaslan F, Yılmaz R, Tuncer MC. Relationship Between Nutritional Indexes and Clinical Outcomes in Stroke Patients Undergoing Mechanical Thrombectomy. Brain Sciences. 2025; 15(7):704. https://doi.org/10.3390/brainsci15070704
Chicago/Turabian StyleErtuğrul, Özgür Zülfükar, Fırat Karaaslan, Reşit Yılmaz, and Mehmet Cudi Tuncer. 2025. "Relationship Between Nutritional Indexes and Clinical Outcomes in Stroke Patients Undergoing Mechanical Thrombectomy" Brain Sciences 15, no. 7: 704. https://doi.org/10.3390/brainsci15070704
APA StyleErtuğrul, Ö. Z., Karaaslan, F., Yılmaz, R., & Tuncer, M. C. (2025). Relationship Between Nutritional Indexes and Clinical Outcomes in Stroke Patients Undergoing Mechanical Thrombectomy. Brain Sciences, 15(7), 704. https://doi.org/10.3390/brainsci15070704