Catalase Activity in the Brain Is Associated with Recovery from Brain Injury in a Piglet Model of Traumatic Brain Injury

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
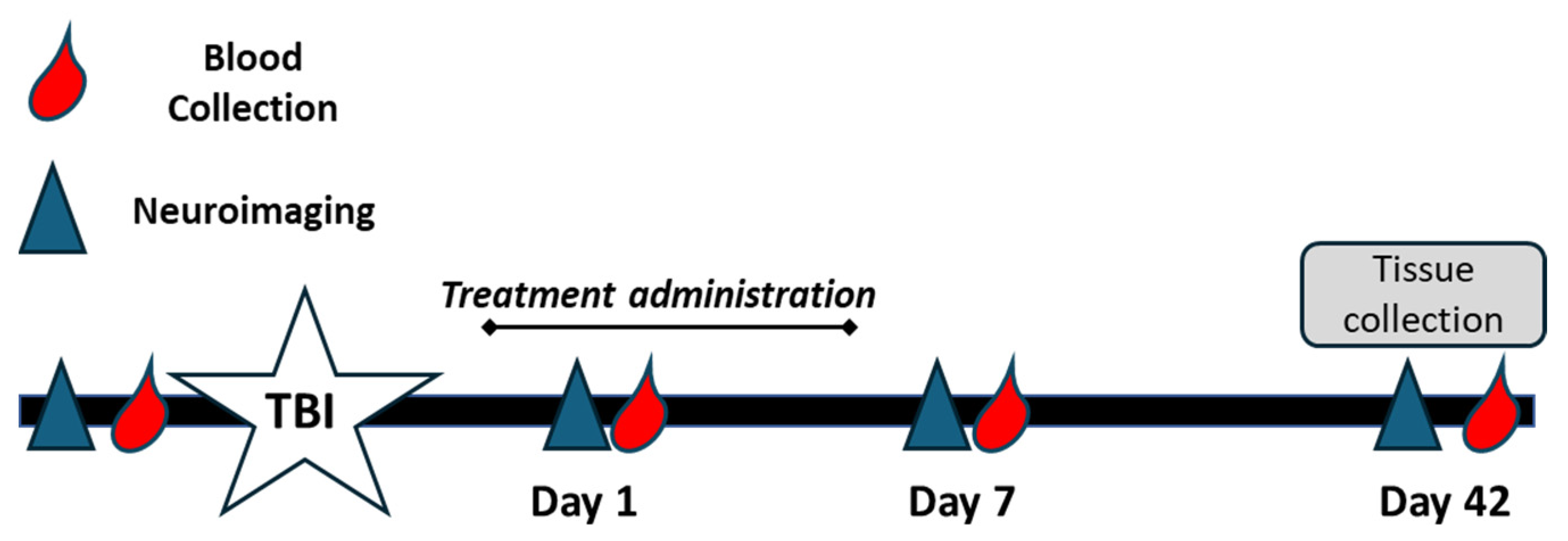
2.1. Animal Handling and Study Design
2.1.1. Controlled Cortical Impact of Traumatic Brain Injury
2.1.2. Plasma, Liver, and Brain Tissue Collection
2.2. Measurement of Catalase and Superoxide Dismutase Activity in Plasma and Tissue
2.3. Statistical Analysis
3. Results
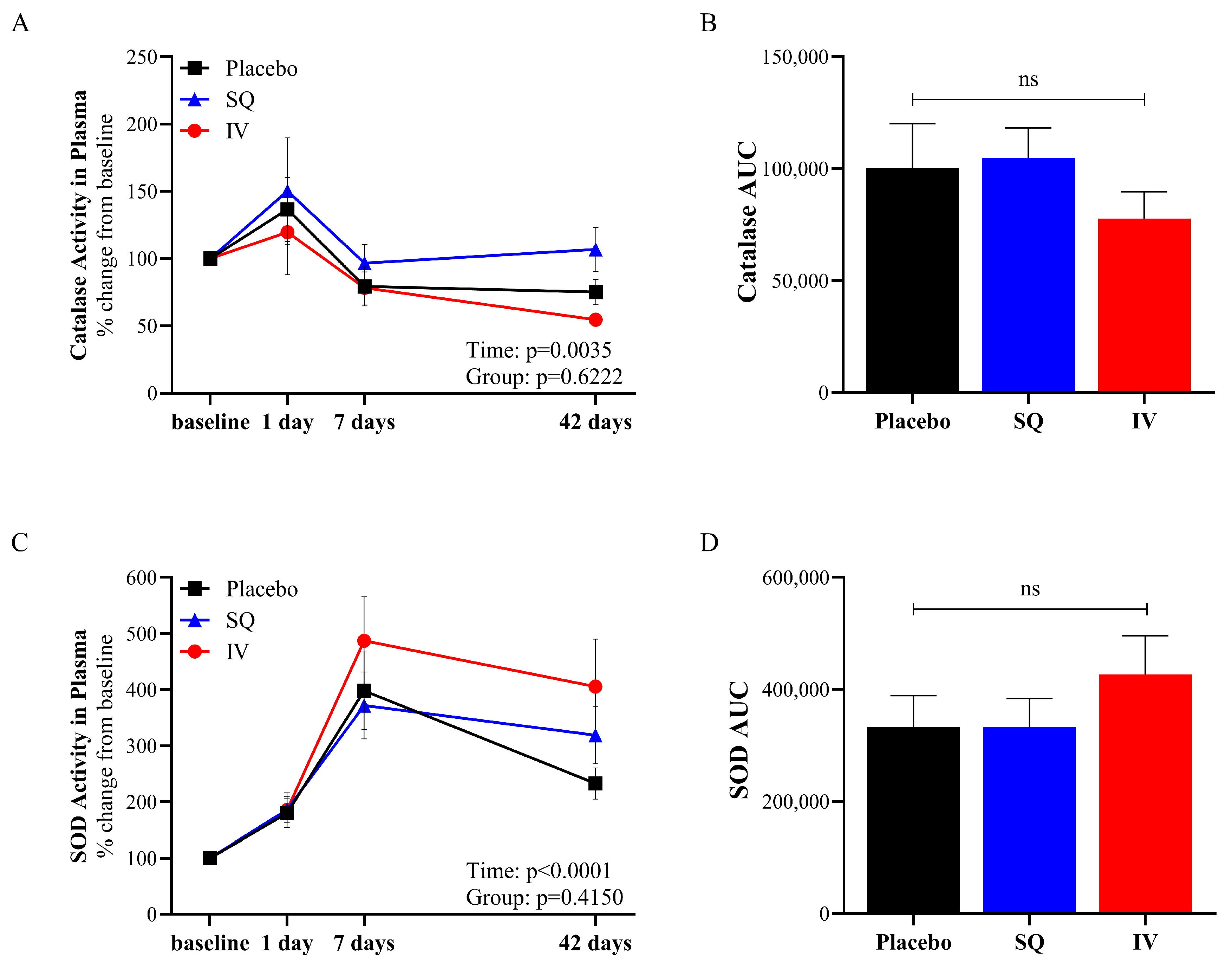
3.1. Antioxidant Enzyme Activity in Plasma Changed over Time Following TBI
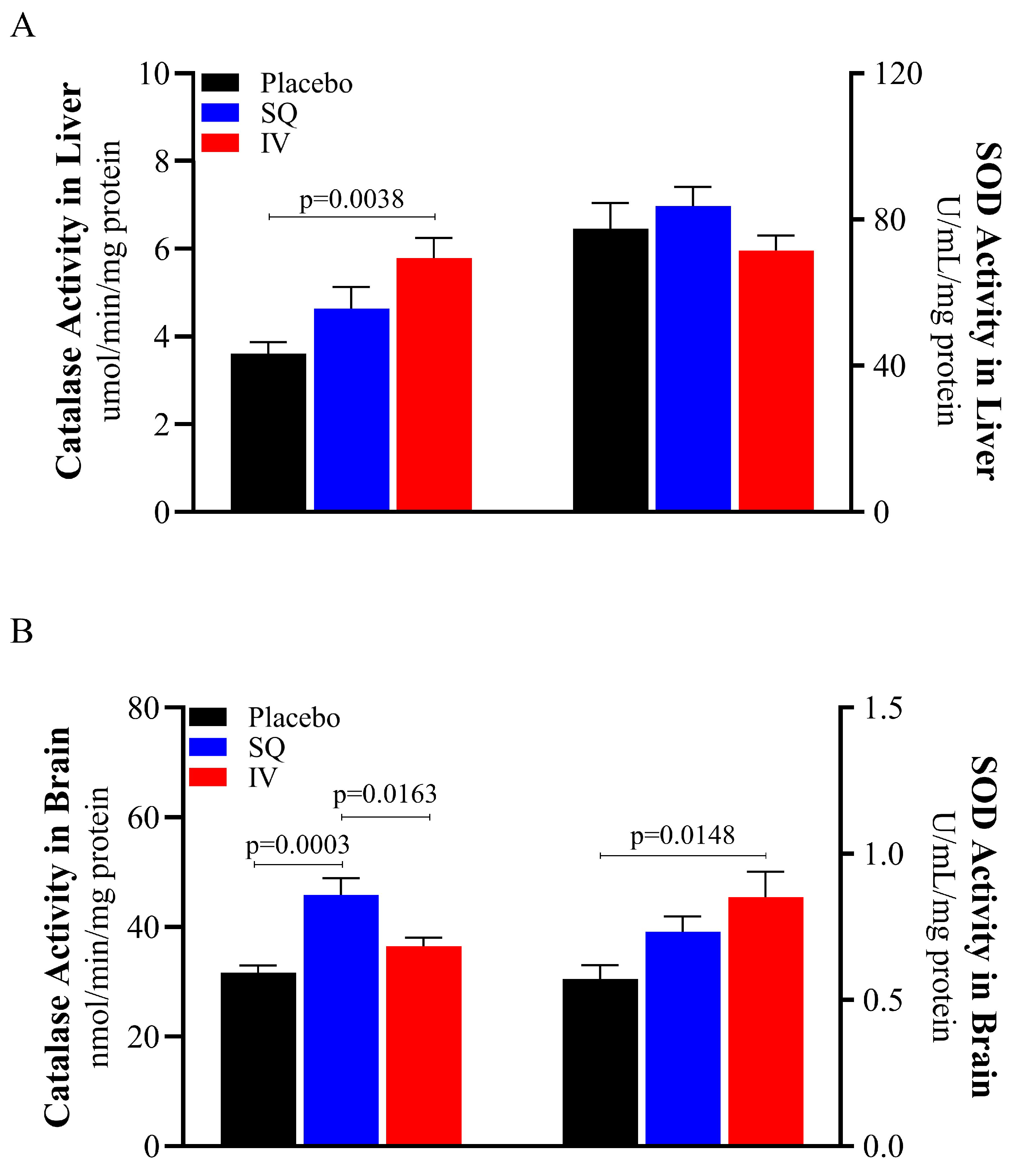
3.2. Administration Route of CMX-2043 Differentially Altered Antioxidant Status in Liver and Brain Following TBI
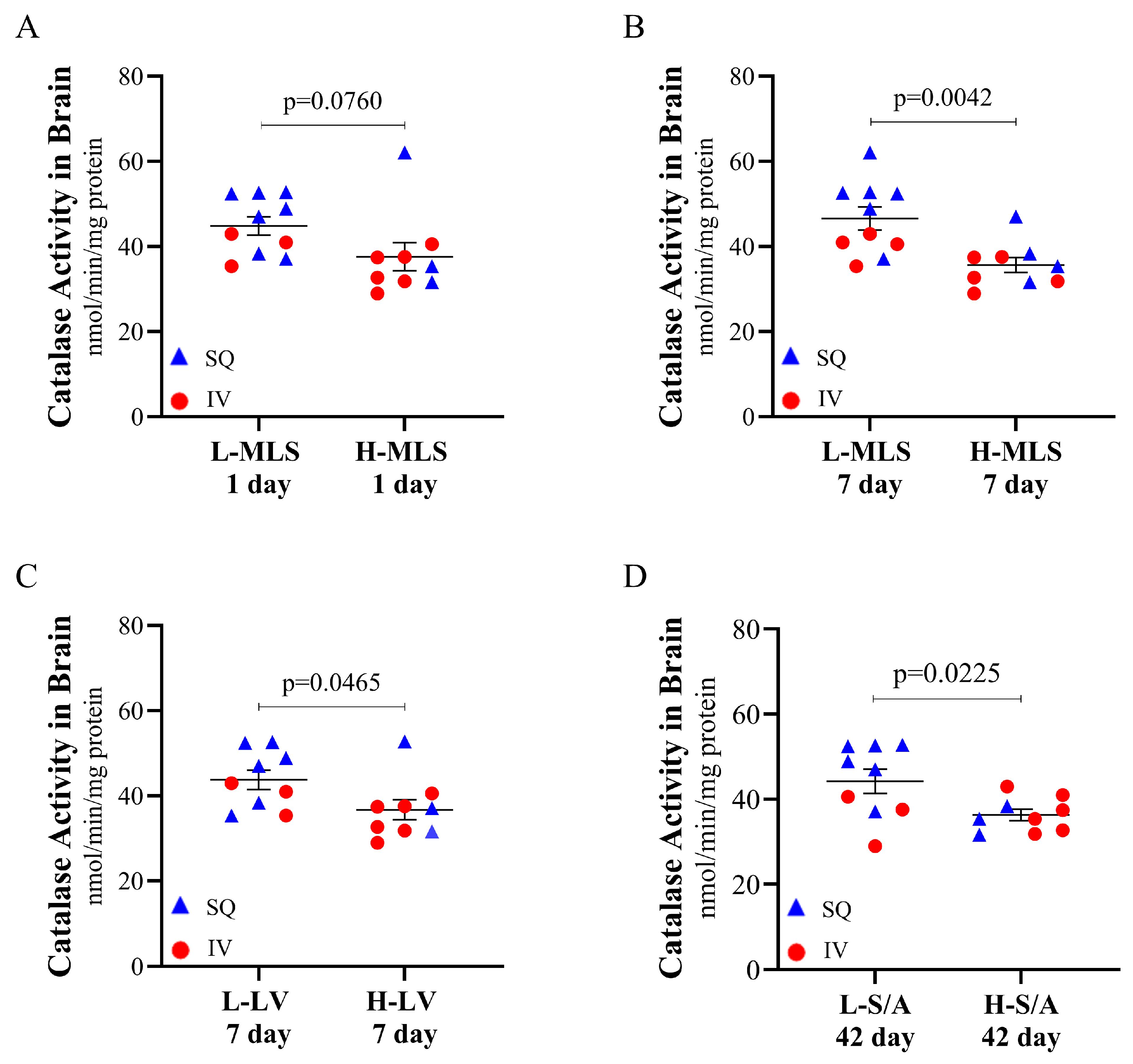
3.3. Catalase Activity in the Brain Is Associated with Decreased Brain Tissue Damage Following TBI
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Fesharaki-Zadeh, A. Oxidative Stress in Traumatic Brain Injury. Int. J. Mol. Sci. 2022, 23, 13000. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, A.G.; Alshboul, O.A. Pathophysiology of traumatic brain injury. Neurosciences 2013, 18, 222–234. [Google Scholar] [PubMed]
- Ryan, A.K.; Rich, W.; Reilly, M.A. Oxidative stress in the brain and retina after traumatic injury. Front. Neurosci. 2023, 17, 1021152. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.; Engelhard, K. Pathophysiology of traumatic brain injury. Br. J. Anaesth. 2007, 99, 4–9. [Google Scholar] [CrossRef]
- Greve, M.W.; Zink, B.J. Pathophysiology of traumatic brain injury. Mt. Sinai J. Med. 2009, 76, 97–104. [Google Scholar] [CrossRef]
- Cornelius, C.; Crupi, R.; Calabrese, V.; Graziano, A.; Milone, P.; Pennisi, G.; Radak, Z.; Calabrese, E.J.; Cuzzocrea, S. Traumatic brain injury: Oxidative stress and neuroprotection. Antioxid. Redox Signal. 2013, 19, 836–853. [Google Scholar] [CrossRef]
- Khatri, N.; Sumadhura, B.; Kumar, S.; Kaundal, R.K.; Sharma, S.; Datusalia, A.K. The Complexity of Secondary Cascade Consequent to Traumatic Brain Injury: Pathobiology and Potential Treatments. Curr. Neuropharmacol. 2021, 19, 1984–2011. [Google Scholar] [CrossRef]
- Shi, K.; Zhang, J.; Dong, J.F.; Shi, F.D. Dissemination of brain inflammation in traumatic brain injury. Cell. Mol. Immunol. 2019, 16, 523–530. [Google Scholar] [CrossRef]
- Cenini, G.; Lloret, A.; Cascella, R. Oxidative Stress in Neurodegenerative Diseases: From a Mitochondrial Point of View. Oxidative Med. Cell. Longev. 2019, 2019, 2105607. [Google Scholar] [CrossRef]
- Lee, K.H.; Cha, M.; Lee, B.H. Neuroprotective Effect of Antioxidants in the Brain. Int. J. Mol. Sci. 2020, 21, 7152. [Google Scholar] [CrossRef]
- Packer, L.; Tritschler, H.J.; Wessel, K. Neuroprotection by the metabolic antioxidant alpha-lipoic acid. Free Radic. Biol. Med. 1997, 22, 359–378. [Google Scholar] [CrossRef] [PubMed]
- Venegoni, W.; Shen, Q.; Thimmesch, A.R.; Bell, M.; Hiebert, J.B.; Pierce, J.D. The use of antioxidants in the treatment of traumatic brain injury. J. Adv. Nurs. 2017, 73, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Zhe, Y.; Gomez-Pinilla, F. Vitamin E protects against oxidative damage and learning disability after mild traumatic brain injury in rats. Neurorehabil Neural Repair. 2010, 24, 290–298. [Google Scholar] [CrossRef]
- Di Pietro, V.; Yakoub, K.M.; Caruso, G.; Lazzarino, G.; Signoretti, S.; Barbey, A.K.; Tavazzi, B.; Lazzarino, G.; Belli, A.; Amorini, A.M. Antioxidant Therapies in Traumatic Brain Injury. Antioxidants 2020, 9, 260. [Google Scholar] [CrossRef]
- Goss, J.R.; Taffe, K.M.; Kochanek, P.M.; DeKosky, S.T. The antioxidant enzymes glutathione peroxidase and catalase increase following traumatic brain injury in the rat. Exp. Neurol. 1997, 146, 291–294. [Google Scholar] [CrossRef]
- Ismail, H.; Shakkour, Z.; Tabet, M.; Abdelhady, S.; Kobaisi, A.; Abedi, R.; Nasrallah, L.; Pintus, G.; Al-Dhaheri, Y.; Mondello, S.; et al. Traumatic Brain Injury: Oxidative Stress and Novel Anti-Oxidants Such as Mitoquinone and Edaravone. Antioxidants 2020, 9, 943. [Google Scholar] [CrossRef]
- Jomova, K.; Alomar, S.Y.; Alwasel, S.H.; Nepovimova, E.; Kuca, K.; Valko, M. Several lines of antioxidant defense against oxidative stress: Antioxidant enzymes, nanomaterials with multiple enzyme-mimicking activities, and low-molecular-weight antioxidants. Arch. Toxicol. 2024, 98, 1323–1367. [Google Scholar] [CrossRef]
- Handy, D.E.; Loscalzo, J. Redox Regulation of Mitochondrial Function. Antioxid. Redox Signal. 2011, 16, 1323–1367. [Google Scholar] [CrossRef]
- Armogida, M.; Nisticò, R.; Mercuri, N.B. Therapeutic potential of targeting hydrogen peroxide metabolism in the treatment of brain ischaemia. Br. J. Pharmacol. 2012, 166, 1211–1224. [Google Scholar] [CrossRef]
- Floyd, R.A.; Carney, J.M. Free radical damage to protein and DNA: Mechanisms involved and relevant observations on brain undergoing oxidative stress. Ann. Neurol. 1992, 32, S22–S27. [Google Scholar] [CrossRef]
- Wang, H.-C.; Lin, Y.-J.; Shih, F.-Y.; Chang, H.-W.; Su, Y.-J.; Cheng, B.-C.; Su, C.-M.; Tsai, N.-W.; Chang, Y.-T.; Kwan, A.-L.; et al. The Role of Serial Oxidative Stress Levels in Acute Traumatic Brain Injury and as Predictors of Outcome. World Neurosurg. 2016, 87, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Lader, A.S.; Baguisi, A.; Casale, R.; Kates, S.A.; Beeuwkes III, R. CMX-2043 mechanisms of action in vitro. J. Cardiovasc. Pharmacol. 2016, 68, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, O.; Sen, C.K.; Roy, S.; Kobayashi, M.S.; Packer, L. Neuroprotective effects of alpha-lipoic acid and its positively charged amide analogue. Free Radic. Biol. Med. 1999, 26, 1418–1426. [Google Scholar] [CrossRef]
- Rochette, L.; Ghibu, S.; Richard, C.; Zeller, M.; Cottin, Y.; Vergely, C. Direct and indirect antioxidant properties of α-lipoic acid and therapeutic potential. Mol. Nutr. Food Res. 2013, 57, 114–125. [Google Scholar] [CrossRef]
- Mahdavi, R.; Khabbazi, T.; Safa, J. Alpha lipoic acid supplementation improved antioxidant enzyme activities in hemodialysis patients. Int. J. Vitam. Nutr. Res. 2019, 89, 161–167. [Google Scholar] [CrossRef]
- Sumathi, R.; Jayanthi, S.; Kalpanadevi, V.; Varalakshmi, P. Effect of DL α-Lipoic Acid on Tissue Lipid Peroxidation and Antioxidant Systems in Normal and Glycollate Treated Rats. Pharmacol. Res. 1993, 27, 309–318. [Google Scholar] [CrossRef]
- Baguisi, A.; Casale, R.A.; Kates, S.A.; Lader, A.S.; Stewart, K.; Beeuwkes, R. CMX-2043 Efficacy in a Rat Model of Cardiac Ischemia–Reperfusion Injury. J. Cardiovasc. Pharmacol. Ther. 2016, 21, 563–569. [Google Scholar] [CrossRef]
- Wang, L.; Wu, C.G.; Fang, C.Q.; Gao, J.; Liu, Y.Z.; Chen, Y.; Chen, Y.N.; Xu, Z.G. The protective effect of α-Lipoic acid on mitochondria in the kidney of diabetic rats. Int. J. Clin. Exp. Med. 2013, 6, 90–97. [Google Scholar] [PubMed]
- Nickander, K.K.; McPhee, B.R.; Low, P.A.; Tritschler, H. Alpha-lipoic acid: Antioxidant potency against lipid peroxidation of neural tissues in vitro and implications for diabetic neuropathy. Free Radic. Biol. Med. 1996, 21, 631–639. [Google Scholar] [CrossRef]
- Kim, J.; De Jesus, O. Medication Routes of Administration. In StatPearls; StatPearls Publishing: Petersburg, FL, USA, 2025. [Google Scholar]
- Diaz-Arrastia, R.; Kochanek, P.M.; Bergold, P.; Kenney, K.; Marx, C.E.; Grimes, C.J.; Loh, L.T.; Adam, L.T.; Oskvig, D.; Curley, K.C.; et al. Pharmacotherapy of traumatic brain injury: State of the science and the road forward: Report of the Department of Defense Neurotrauma Pharmacology Workgroup. J. Neurotrauma 2014, 31, 135–158. [Google Scholar] [CrossRef]
- Open Resources for Nursing. Open RN OER Textbooks. In Nursing Pharmacology; Ernstmeyer, K., Christman, E., Eds.; Chippewa Valley Technical College: Eau Claire, WI, USA, 2023. [Google Scholar]
- Claassen, V. (Ed.) 4-Subcutaneous Drug Administration. In Techniques in the Behavioral and Neural Sciences; Elsevier: Amsterdam, The Netherlands, 1994; Volume 12, pp. 35–45. [Google Scholar]
- Kim, H.; Park, H.; Lee, S.J. Effective method for drug injection into subcutaneous tissue. Sci. Rep. 2017, 7, 9613. [Google Scholar] [CrossRef] [PubMed]
- Kinder, H.A.; Baker, E.W.; Wang, S.; Fleischer, C.C.; Howerth, E.W.; Duberstein, K.J.; Mao, H.; Platt, S.R.; West, F.D. Traumatic Brain Injury Results in Dynamic Brain Structure Changes Leading to Acute and Chronic Motor Function Deficits in a Pediatric Piglet Model. J. Neurotrauma 2019, 36, 2930–2942. [Google Scholar] [CrossRef] [PubMed]
- Kinder, H.A.; Baker, E.W.; West, F.D. The pig as a preclinical traumatic brain injury model: Current models, functional outcome measures, and translational detection strategies. Neural Regen. Res. 2019, 14, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Friess, S.H.; Ichord, R.N.; Owens, K.; Ralston, J.; Rizol, R.; Overall, K.L.; Smith, C.; Helfaer, M.A.; Margulies, S.S. Neurobehavioral functional deficits following closed head injury in the neonatal pig. Exp. Neurol. 2007, 204, 234–243. [Google Scholar] [CrossRef]
- Schantz, S.L.; Sneed, S.E.; Fagan, M.M.; Golan, M.E.; Cheek, S.R.; Kinder, H.A.; Duberstein, K.J.; Kaiser, E.E.; West, F.D. Human-Induced Pluripotent Stem Cell-Derived Neural Stem Cell Therapy Limits Tissue Damage and Promotes Tissue Regeneration and Functional Recovery in a Pediatric Piglet Traumatic-Brain-Injury Model. Biomedicines 2024, 12, 1663. [Google Scholar] [CrossRef]
- Council, N.R. Nutrient Requirements of Swine; The National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Field, C.L.; Whoriskey, S.T.; Zhao, X.; Papich, M.G. Pharmacokinetics of Subcutaneous Alpha Lipoic Acid, a Proposed Therapeutic Aid for Domoic Acid Intoxication in California Sea Lions (Zalophus californianus). J. Zoo Wildl. Med. 2021, 52, 872–879. [Google Scholar] [CrossRef]
- Fagan, M.M.; Welch, C.B.; Scheulin, K.M.; Sneed, S.E.; Jeon, J.H.; Golan, M.E.; Cheek, S.R.; Barany, D.A.; Oeltzschner, G.; Callaway, T.R.; et al. Fecal microbial transplantation limits neural injury severity and functional deficits in a pediatric piglet traumatic brain injury model. Front. Neurosci. 2023, 17, 1249539. [Google Scholar] [CrossRef]
- Baker, E.W.; Kinder, H.A.; Hutcheson, J.M.; Duberstein, K.J.J.; Platt, S.R.; Howerth, E.W.; West, F.D. Controlled Cortical Impact Severity Results in Graded Cellular, Tissue, and Functional Responses in a Piglet Traumatic Brain Injury Model. J. Neurotrauma 2019, 36, 61–73. [Google Scholar] [CrossRef]
- Sani, M.; Sebaï, H.; Gadacha, W.; Boughattas, N.A.; Reinberg, A.; Mossadok, B.A. Catalase activity and rhythmic patterns in mouse brain, kidney and liver. Comp. Biochem. Physiol. Part B Biochem. Mol. Biol. 2006, 145, 331–337. [Google Scholar] [CrossRef]
- Caccialanza, R.; Constans, T.; Cotogni, P.; Zaloga, G.P.; Pontes-Arruda, A. Subcutaneous Infusion of Fluids for Hydration or Nutrition: A Review. J. Parenter. Enter. Nutr. 2018, 42, 296–307. [Google Scholar] [CrossRef]
- Nishimura, K.; Cordeiro, J.G.; Ahmed, A.I.; Yokobori, S.; Gajavelli, S. Advances in Traumatic Brain Injury Biomarkers. Cureus 2022, 14, e23804. [Google Scholar] [CrossRef] [PubMed]
- Joyce, J.M.; La, P.L.; Walker, R.; Harris, A.D. Magnetic Resonance Spectroscopy of Traumatic Brain Injury and Subconcussive Hits: A Systematic Review and Meta-Analysis. J. Neurotrauma 2022, 39, 1455–1476. [Google Scholar] [CrossRef]
- Huang, S.; Lyu, Y.; Liu, T.; Zhu, D. Metabolite changes and impact factors in mild traumatic brain injury patients: A review on magnetic resonance spectroscopy. Meta-Radiol. 2024, 2, 100056. [Google Scholar] [CrossRef]
- Tsuru-Aoyagi, K.; Potts, M.B.; Trivedi, A.; Pfankuch, T.; Raber, J.; Wendland, M.; Claus, C.P.; Koh, S.E.; Ferriero, D.; Noble-Haeusslein, L.J. Glutathione peroxidase activity modulates recovery in the injured immature brain. Ann. Neurol. 2009, 65, 540–549. [Google Scholar] [CrossRef]
- Crack, P.J.; Taylor, J.M.; de Haan, J.B.; Kola, I.; Hertzog, P.; Iannello, R.C. Glutathione Peroxidase-1 Contributes to the Neuroprotection Seen in the Superoxide Dismutase-1 Transgenic Mouse in Response to Ischemia/Reperfusion Injury. J. Cereb. Blood Flow. Metab. 2003, 23, 19–22. [Google Scholar] [CrossRef]
- Yang, T.; Kong, B.; Gu, J.W.; Kuang, Y.Q.; Cheng, L.; Yang, W.T.; Xia, X.; Shu, H.F. Anti-apoptotic and anti-oxidative roles of quercetin after traumatic brain injury. Cell. Mol. Neurobiol. 2014, 34, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, C.; Peng, W.; Xia, Z.; Gan, P.; Huang, W.; Shi, Y.; Fan, R. Hydroxysafflor yellow A exerts antioxidant effects in a rat model of traumatic brain injury. Mol. Med. Rep. 2016, 14, 3690–3696. [Google Scholar] [CrossRef]
- Dabrowska-Schlepp, P.; Busch, A.; Shen, J.-S.; Cheong, R.Y.; Madsen, L.B.; Mascher, D.; Schiffmann, R.; Schaaf, A. Comparison of efficacy between subcutaneous and intravenous application of moss-aGal in the mouse model of Fabry disease. JIMD Rep. 2023, 64, 460–467. [Google Scholar] [CrossRef]
- Moeller, J.; Green, M.D.; Ramnath, N. Pros and cons of subcutaneous (SC) versus intravenous (IV) administration of immune checkpoint inhibitors in non-small cell lung cancer. Transl. Lung Cancer Res. 2024, 13, 1444–1449. [Google Scholar] [CrossRef]
- Taylor, S.D.; Hart, K.A.; Vaughn, S.; Giancola, S.C.; Serpa, P.B.S.; Santos, A.P. Effects of intravenous administration of ascorbic acid (vitamin C) on oxidative status in healthy adult horses. J. Vet. Intern. Med. 2024, 38, 460–468. [Google Scholar] [CrossRef]
- Dias-Junior, C.A.; Souza-Costa, D.C.; Zerbini, T.; da Rocha, J.B.T.; Gerlach, R.F.; Tanus-Santos, J.E. The Effect of Sildenafil on Pulmonary Embolism-Induced Oxidative Stress and Pulmonary Hypertension. Anesth. Analg. 2005, 101, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Uchida, R.; Okamoto, H.; Ikuta, N.; Terao, K.; Hirota, T. Enantioselective Pharmacokinetics of α-Lipoic Acid in Rats. Int. J. Mol. Sci. 2015, 16, 22781–22794. [Google Scholar] [CrossRef] [PubMed]
- Krenzlin, H.; Wesp, D.; Schmitt, J.; Frenz, C.; Kurz, E.; Masomi-Bornwasser, J.; Lotz, J.; Ringel, F.; Kerz, T.; Keric, N. Decreased Superoxide Dismutase Concentrations (SOD) in Plasma and CSF and Increased Circulating Total Antioxidant Capacity (TAC) Are Associated with Unfavorable Neurological Outcome after Aneurysmal Subarachnoid Hemorrhage. J. Clin. Med. 2021, 10, 1188. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Narabayashi, H.; Sata, T.; Takeshige, K. Kinetics of superoxide formation by respiratory chain NADH-dehydrogenase of bovine heart mitochondria. J. Biochem. 1983, 94, 1301–1306. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MRI Measurement | r | p-Value |
|---|---|---|
| 1 Day Midline Shift | −0.4557 | 0.0148 |
| 7 Day Midline Shift | −0.6241 | 0.0004 |
| 42 Day Midline Shift | −0.5448 | 0.0033 |
| 1 Day Lesion Volume | −0.3433 | 0.0860 |
| 7 Day Lesion Volume | −0.3419 | 0.0749 |
| 42 Day Lesion Volume | −0.5770 | 0.0016 |
| 1 Day Swelling/Atrophy | −0.4084 | 0.0383 |
| 42 Day Swelling/Atrophy | 0.1686 | 0.4005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubrof, S.T.; Schantz, S.L.; LePage, T.H.; Sneed, S.E.; Cheek, S.R.; Kinder, H.A.; Duberstein, K.J.; DeWahl, D.A.; Stern, J.O.; Baguisi, A.B.; et al. Catalase Activity in the Brain Is Associated with Recovery from Brain Injury in a Piglet Model of Traumatic Brain Injury. Brain Sci. 2025, 15, 608. https://doi.org/10.3390/brainsci15060608
Dubrof ST, Schantz SL, LePage TH, Sneed SE, Cheek SR, Kinder HA, Duberstein KJ, DeWahl DA, Stern JO, Baguisi AB, et al. Catalase Activity in the Brain Is Associated with Recovery from Brain Injury in a Piglet Model of Traumatic Brain Injury. Brain Sciences. 2025; 15(6):608. https://doi.org/10.3390/brainsci15060608
Chicago/Turabian StyleDubrof, Stephanie T., Sarah L. Schantz, Taylor H. LePage, Sydney E. Sneed, Savannah R. Cheek, Holly A. Kinder, Kylee J. Duberstein, David A. DeWahl, Jerry O. Stern, Alexander B. Baguisi, and et al. 2025. "Catalase Activity in the Brain Is Associated with Recovery from Brain Injury in a Piglet Model of Traumatic Brain Injury" Brain Sciences 15, no. 6: 608. https://doi.org/10.3390/brainsci15060608
APA StyleDubrof, S. T., Schantz, S. L., LePage, T. H., Sneed, S. E., Cheek, S. R., Kinder, H. A., Duberstein, K. J., DeWahl, D. A., Stern, J. O., Baguisi, A. B., Kaiser, E. E., West, F. D., & Park, H. J. (2025). Catalase Activity in the Brain Is Associated with Recovery from Brain Injury in a Piglet Model of Traumatic Brain Injury. Brain Sciences, 15(6), 608. https://doi.org/10.3390/brainsci15060608