
The Relationship Between Autoimmune Disorders and Multiple Sclerosis: Clinical Insights and Therapeutic Approaches

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. General Description of the Study Group
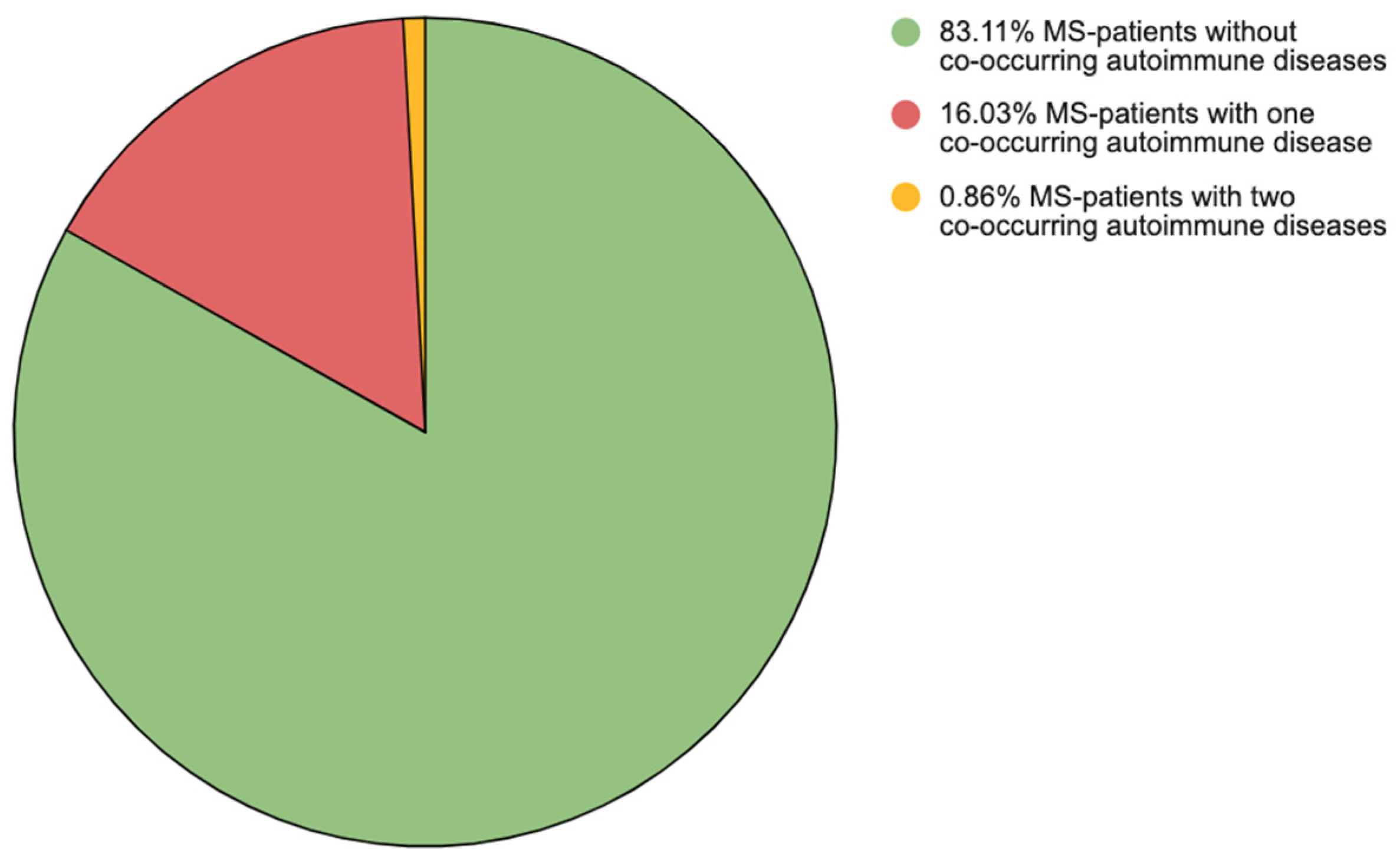
3.2. AIDs in the Study Group
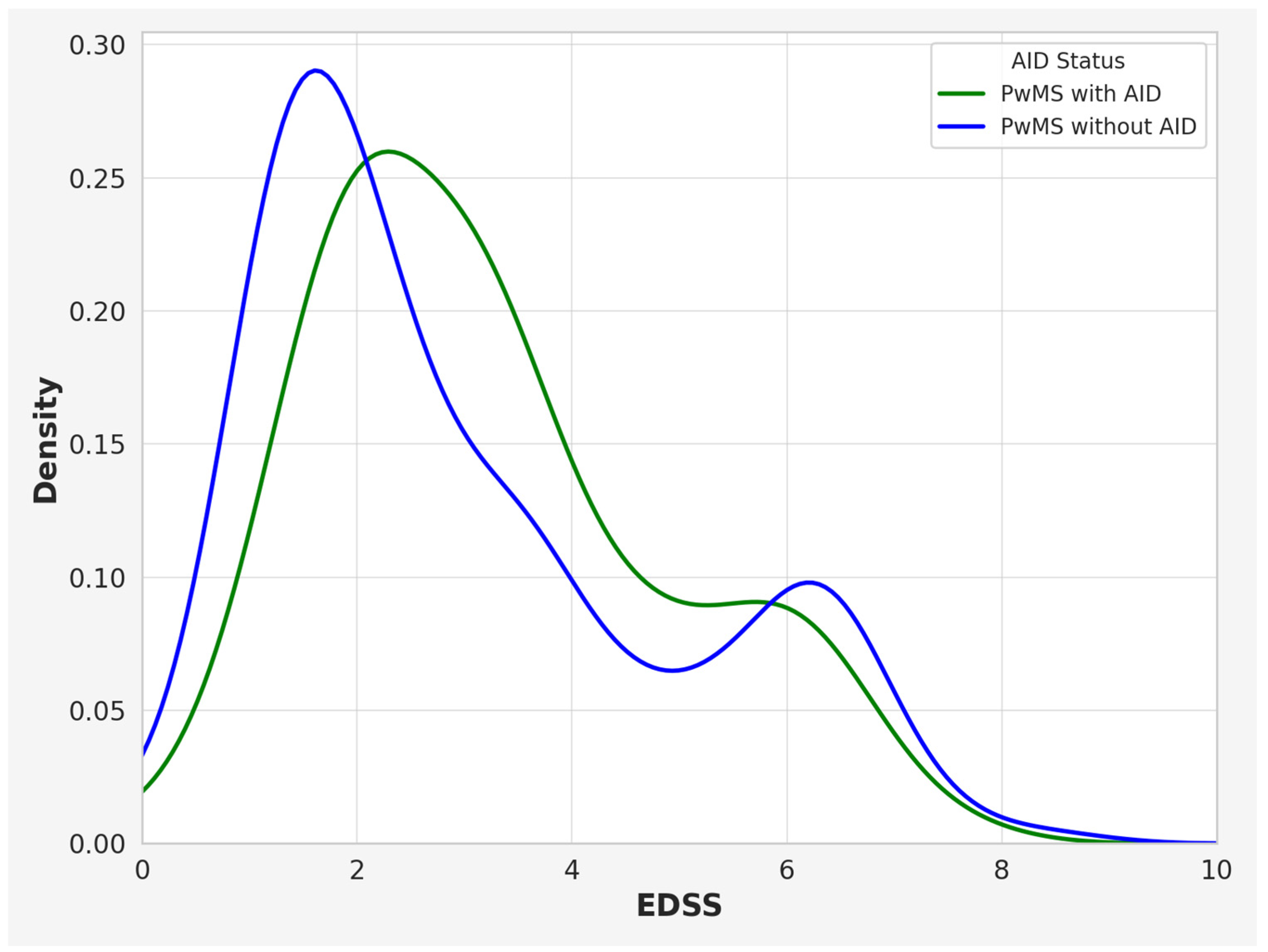
3.3. Comparison Between PwMSs with and Without Co-Occurring AIDs
3.4. The Results of Vitamin D3 and TSH Levels in PwMSs with and Without Co-Occurring AIDs
3.5. Comparison of Groups in Relation to the Prevalence of Thyroid Disease
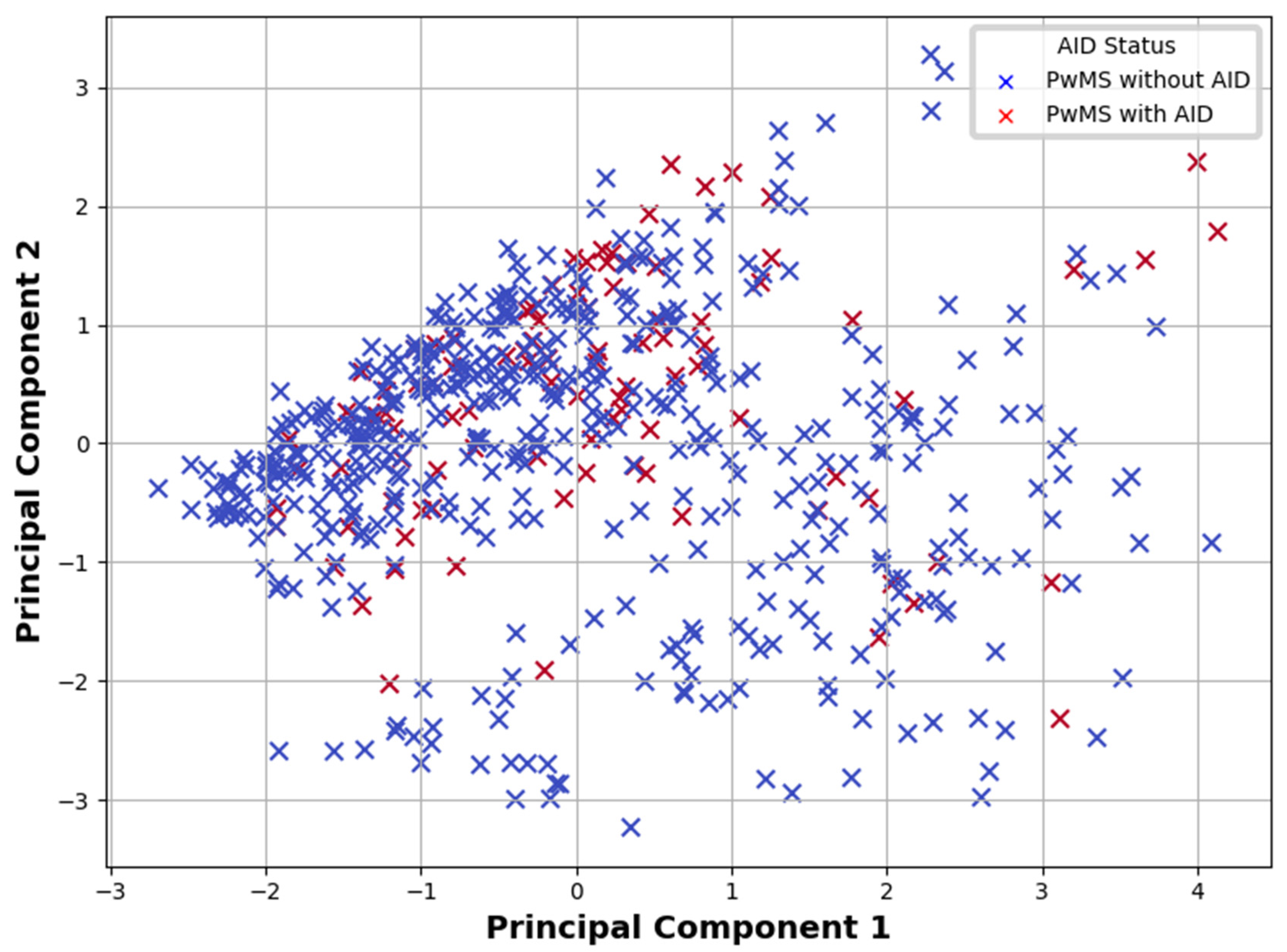
3.6. Multivariate Analyses of AIDs Risk in PwMSs
4. Discussion
4.1. Impact of Coexisting AIDs on MS Course
4.2. Effect of Immunomodulatory Therapies on AID Course and Morbidity
4.3. Co-Occurrence of MS and AIDs
4.4. Thyroid Disorders Are the Most Common AIDs in PwMSs
4.5. Role of Vitamin D3 in the Pathogenesis of MS and AIDs
4.6. Limitations and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MS | Multiple Sclerosis |
| PwMSs | Patients with multiple sclerosis |
| AIDs | Autoimmune diseases |
| EDSS | Expanded Disability Status Scale |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Autoimmune Diseases | n (%) |
|---|---|
| Hypothyroidism | 42 (7.24%) |
| Hashimoto’s disease | 24 (4.18%) |
| Hyperthyroidism | 10 (1.72%) |
| Type 1 diabetes | 9 (1.55%) |
| Inflammatory bowel diseases | 6 (1.03%) |
| Ulcerative colitis | 5 (0.86%) |
| Psoriasis | 3 (0.52%) |
| Connective Tissue Diseases | 3 (0.52%) |
| Atopic dermatitis | 2 (0.34% |
| Rheumatoid arthritis | 2 (0.34%) |
| Crohn’s disease | 1 (0.17%) |
| Psoriatic arthritis | 1 (0.17%) |
| Sjogren’s syndrome | 1 (0.17%) |
| Ankylosing spondylitis | 1 (0.17%) |
| Vitiligo | 1 (0.17%) |
References
- Juncker, A.S.; Appenzeller, S.; de Souza, J.M. Central Nervous System Involvement in Systemic Autoimmune Rheumatic Diseases—Diagnosis and Treatment. Pharmaceuticals 2024, 17, 1044. [Google Scholar] [CrossRef] [PubMed]
- Carver, J.J.; Lau, K.M.; Puckett, A.E.; Didonna, A. Autoimmune demyelination alters hypothalamic transcriptome and endocrine function. J. Neuroinflamm. 2024, 21, 12. [Google Scholar] [CrossRef]
- Hayter, S.M.; Cook, M.C. Updated assessment of the prevalence, spectrum and definition of autoimmune disease. Autoimmun. Rev. 2012, 11, 754–765. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Alroughani, R.; AlMojel, M.; Qasem, D.; Al-Hashel, J.; Ahmed, S.F. Pediatric onset multiple sclerosis in Kuwait. Clin. Neurol. Neurosurg. 2025, 248, 108643. [Google Scholar] [CrossRef]
- Alonso-Magdalena, L.; Carmona i Codina, O.; Zia, E.; Sundström, P.; Pessah-Rasmussen, H. Prevalence and disease disability in immigrants with multiple sclerosis in Malmö, southern Sweden. Clin. Neurol. Neurosurg. 2024, 240, 108255. [Google Scholar] [CrossRef] [PubMed]
- Haki, M.; Al-Biati, H.A.; Al-Tameemi, Z.S.; Ali, I.S.; Al-Hussaniy, H.A. Review of multiple sclerosis: Epidemiology, etiology, pathophysiology, and treatment. Medicine 2024, 103, E37297. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Guerra, T.; Caputo, F.; Paolicelli, D.; Iaffaldano, P. Siponimod from fingolimod direct switch in patients transitioning in secondary progressive multiple sclerosis: A single center case series. Clin. Neurol. Neurosurg. 2024, 245, 108475. [Google Scholar] [CrossRef]
- Granziera, C.; Derfuss, T.; Kappos, L. Time to change the current clinical classification of multiple sclerosis? JAMA Neurol. 2023, 80, 128–130. [Google Scholar] [CrossRef]
- Wnuk, M.; Maluchnik, M.; Perwieniec, J.; Podwojcic, K.; Szelag, M.; Walkiewicz, D.; Zakrzewski, M.; Kulakowska, A.; Brola, W.; Rejdak, K.; et al. Multiple sclerosis incidence and prevalence in Poland: Data from administrative health claims. Mult. Scler. Relat. Disord. 2021, 55, 103162. [Google Scholar] [CrossRef]
- Portaccio, E.; Magyari, M.; Havrdova, E.K.; Ruet, A.; Brochet, B.; Scalfari, A.; Di Filippo, M.; Tur, C.; Montalban, X.; Amato, M.P. Multiple sclerosis: Emerging epidemiological trends and redefining the clinical course. Lancet Reg. Health Eur. 2024, 44, 100977. [Google Scholar] [CrossRef] [PubMed]
- Leavitt, V.M.; Dworkin, J.D.; Kalina, T.; Ratzan, A.S. Sex differences in brain resilience of individuals with multiple sclerosis. Mult. Scler. Relat. Disord. 2024, 87, 105646. [Google Scholar] [CrossRef] [PubMed]
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef]
- Murúa, S.R.; Farez, M.F.; Quintana, F.J. The Immune Response in Multiple Sclerosis. Annual Review of Pathology: Mechanisms of Disease. Annu. Rev. Pathol. Mech. Dis. 2022, 17, 121–139. [Google Scholar] [CrossRef] [PubMed]
- Trapp, B.D.; Nave, K.A. Multiple sclerosis: An immune or neurodegenerative disorder? Annu. Rev. Neurosci. 2008, 31, 247–269. [Google Scholar] [CrossRef]
- Stys, P.K.; Zamponi, G.W.; van Minnen, J.; Geurts, J.J.G. Will the real multiple sclerosis please stand up? Nat. Rev. Neurosci. 2012, 13, 507–514. [Google Scholar] [CrossRef]
- ’t Hart, B.A.; Luchicchi, A.; Schenk, G.J.; Stys, P.K.; Geurts, J.J.G. Mechanistic underpinning of an inside-out concept for autoimmunity in multiple sclerosis. Ann. Clin. Transl. Neurol. 2021, 8, 1709–1719. [Google Scholar] [CrossRef]
- Kutzelnigg, A.; Lucchinetti, C.F.; Stadelmann, C.; Brück, W.; Rauschka, H.; Bergmann, M.; Schmidbauer, M.; Parisi, J.E.; Lassmann, H. Cortical demyelination and diffuse white matter injury in multiple sclerosis. Brain 2005, 128, 2705–2712. [Google Scholar] [CrossRef]
- Kuhlmann, T.; Antel, J. Multiple sclerosis: 2023 update. Free Neuropathol. 2023, 4, 3. [Google Scholar]
- Racosta, J.M.; Kimpinski, K. Autonomic dysfunction, immune regulation, and multiple sclerosis. Clin. Auton. Res. 2016, 26, 23–31. [Google Scholar] [CrossRef]
- Walawska-Hrycek, A.; Galus, W.; Hrycek, E.; Kaczmarczyk, A.; Krzystanek, E. The impact of vitamin D is low on its serum level and cytokine profile in multiple sclerosis patients. J. Clin. Med. 2021, 10, 2781. [Google Scholar] [CrossRef]
- Wang, L.; Wang, F.S.; Gershwin, M.E. Human autoimmune diseases: A comprehensive update. J. Intern. Med. 2015, 278, 369–395. [Google Scholar] [CrossRef] [PubMed]
- University of Oxford, Autoimmune Disorders Found to Affect Around One in Ten People. Available online: https://www.ox.ac.uk/news/2023-05-06-autoimmune-disorders-found-affect-around-one-ten-people (accessed on 24 October 2024).
- Mahler, J.V.; Solti, M.; Apóstolos-Pereira, S.L.; Adoni, T.; Silva, G.D.; Callegaro, D. Vitamin D3 as an add-on treatment for multiple sclerosis: A systematic review and meta-analysis of randomized controlled trials. Mult. Scler. Relat. Disord. 2024, 82, 105433. [Google Scholar] [CrossRef] [PubMed]
- Murdaca, G.; Tonacci, A.; Negrini, S.; Greco, M.; Borro, M.; Puppo, F.; Gangemi, S. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019, 18, 102350. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Giovannoni, G. Autoimmune disease in people with multiple sclerosis and their relatives: A systematic review and meta-analysis. J. Neurol. 2013, 260, 1272–1285. [Google Scholar] [CrossRef]
- Barcellos, L.F.; Kamdar, B.B.; Ramsay, P.P.; DeLoa, C.; Lincoln, R.R.; Caillier, S.; Schmidt, S.; Haines, J.L.; Pericak-Vance, M.A.; Oksenberg, J.R.; et al. Clustering of autoimmune diseases in families with a high-risk for multiple sclerosis: A descriptive study. Lancet Neurol. 2006, 5, 924–931. [Google Scholar] [CrossRef]
- Roshanisefat, H.; Bahmanyar, S.; Hillert, J.; Olsson, T.; Montgomery, S. Shared genetic factors may not explain the raised risk of comorbid inflammatory diseases in multiple sclerosis. Mult. Scler. 2012, 18, 1430–1436. [Google Scholar] [CrossRef]
- Disanto, G.; Ramagopalan, S.V. Multiple sclerosis and co-morbid autoimmune disease: The final nail in the coffin? Mult. Scler. 2012, 18, 1370–1371. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Selmaj, K.; Cree, B.A.C.; Barnett, M.; Thompson, A.; Hartung, H.P. Multiple sclerosis: Time for early treatment with high-efficacy drugs. J. Neurol. 2024, 271, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.M.; Poppe, K.G.; Effraimidis, G. Hyperthyroidism: Aetiology, pathogenesis, diagnosis, management, complications, and prognosis. Lancet Diabetes Endocrinol. 2023, 11, 282–298. [Google Scholar] [CrossRef]
- Zéphir, H.; Gower-Rousseau, C.; Salleron, J.; Simon, O.; Debouverie, M.; Le Page, E.; Bouhnik, Y.; Lebrun-Frenay, C.; Papeix, C.; Vigneron, B.; et al. Milder multiple sclerosis course in patients with concomitant inflammatory bowel disease. Mult. Scler. 2014, 20, 1135–1139. [Google Scholar] [CrossRef] [PubMed]
- Sahraian, M.A.; Owji, M.; Naser Moghadasi, A. Concomitant multiple sclerosis and another autoimmune disease: Does the clinical course change? Clin. Neurol. Neurosurg. 2016, 150, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Wawrzyniak, S.; Rakoca, M.; Kułakowska, A.; Bartosik-Psujek, H.; Koziarska, D.; Kapica-Topczewska, K.; Kubicka-Bączyk, K.; Adamczyk-Sowa, M. Multiple sclerosis, and autoimmune diseases—A case control study. Neurol. Neurochir. Pol. 2023, 57, 344–351. [Google Scholar] [CrossRef]
- Rose, N.R. Prediction and prevention of autoimmune disease in the 21st Century: A review and preview. Am. J. Epidemiol. 2016, 183, 403–406. [Google Scholar] [CrossRef]
- Petranović Ovčariček, P.; Görges, R.; Giovanella, L. Autoimmune Thyroid Diseases. Semin. Nucl. Med. 2024, 54, 219–236. [Google Scholar] [CrossRef]
- Voskuhl, R.R. The effect of sex on multiple sclerosis risk and disease progression. Mult. Scler. J. 2020, 26, 554–560. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Moldovan, I.R.; Cotleur, A.C.; Zamor, N.; Butler, R.S.; Pelfrey, C.M. Multiple sclerosis patients show sexual dimorphism in cytokine responses to myelin antigens. J. Neuroimmunol. 2008, 193, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Baecher-Allan, C.; Kaskow, B.J.; Weiner, H.L. Multiple Sclerosis: Mechanisms and Immunotherapy. Neuron 2018, 97, 742–768. [Google Scholar] [CrossRef] [PubMed]
- Hojjati, S.M.M.; Heidari, B.; Babaei, M. Development of rheumatoid arthritis during treatment of multiple sclerosis with interferon beta 1-a. Coincidence of two conditions or a complication of treatment: A case report. J. Adv. Res. 2016, 7, 611–613. [Google Scholar] [CrossRef]
- Porwal, M.H.; Patel, D.; Maynard, M.; Obeidat, A.Z. Disproportional increase in psoriasis reports in association with B cell depleting therapies in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 63, 103832. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Castellana, M.; Virili, C.; Bellastella, G.; Centanni, M.; Cannavò, S.; Campennì, A.; Ruggeri, R.M.; Giovanella, L.; Trimboli, P. Alemtuzumab-induced thyroid events in multiple sclerosis: A systematic review and meta-analysis. J. Endocrinol. Investig. 2020, 43, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Mahzari, M.; Arnaout, A.; Freedman, M.S. Alemtuzumab Induced Thyroid Disease in Multiple Sclerosis: A Review and Approach to Management. Can. J. Neurol. Sci. 2015, 42, 284–291. [Google Scholar] [CrossRef]
- Kazakou, P.; Tzanetakos, D.; Vakrakou, A.G.; Tzartos, J.S.; Evangelopoulos, M.E.; Anagnostouli, M.; Stathopoulos, P.; Kassi, G.N.; Stefanis, L.; Kilidireas, C.; et al. Thyroid autoimmunity following alemtuzumab treatment in multiple sclerosis patients: A prospective study. Clin. Exp. Med. 2023, 23, 2885–2894. [Google Scholar] [CrossRef]
- Sovetkina, A.; Nadir, R.; Scalfari, A.; Tona, F.; Murphy, K.; Rigoni, E.; Dorsey, R.; Malik, O.; Nandoskar, A.; Singh-Curry, V.; et al. Development of autoimmune thyroid disease in multiple sclerosis patients post-alemtuzumab improves treatment response. J. Clin. Endocrinol. Metab. 2020, 105, E3392–E3399. [Google Scholar] [CrossRef]
- la Mantia, L.; Capsoni, F. Psoriasis during interferon beta treatment for multiple sclerosis. Neurol. Sci. 2010, 31, 337–339. [Google Scholar] [CrossRef]
- Amschler, K.; Meyersburg, D.; Kitze, B.; Schön, M.P.; Mössner, R. Onset of psoriasis upon interferon beta treatment in a multiple sclerosis patient. Eur. J. Dermatol. 2016, 26, 211–212. [Google Scholar] [CrossRef]
- Fellner, A.; Dano, M.; Regev, K.; Mosek, A.; Karni, A. Multiple sclerosis is associated with psoriasis. A case-control study. J. Neurol. Sci. 2014, 338, 226–228. [Google Scholar] [CrossRef]
- Millán-Pascual, J.; Turpín-Fenoll, L.; del Saz-Saucedo, P.; Rueda-Medina, I.; Navarro-Muñoz, S. Psoriasis during natalizumab treatment for multiple sclerosis. J. Neurol. 2012, 259, 2758–2760. [Google Scholar] [CrossRef]
- Su, E.; Novic, J.; Han, M.H. Emergence of rheumatoid arthritis following exposure to natalizumab. Mult. Scler. Relat. Disord. 2020, 40, 101936. [Google Scholar] [CrossRef]
- Oddo, S.; Laroni, A.; Uccelli, A.; Giusti, M. A case of thyroiditis during natalizumab therapy for multiple sclerosis. J. Endocrinol. Investig. 2011, 34, 408–409. [Google Scholar] [CrossRef]
- Pagnini, C.; Arseneau, K.O.; Cominelli, F. Natalizumab in the treatment of Crohn’s disease patients. Expert. Opin. Biol. Ther. 2017, 17, 1433–1438. [Google Scholar] [CrossRef]
- Nelson, S.M.L.; Nguyen, T.M.; Mcdonald, J.W.D.; Macdonald, J.K. Natalizumab for induction of remission in Crohn’s disease. Cochrane Database Syst. Rev. 2018, 8, CD006097. [Google Scholar] [CrossRef]
- Cree, B.A.; Selmaj, K.W.; Steinman, L.; Comi, G.; Bar-Or, A.; Arnold, D.L.; Hartung, H.P.; Montalban, X.; Havrdova, E.K.; Sheffield, J.K.; et al. Long-term safety and efficacy of ozanimod in relapsing multiple sclerosis: Up to 5 years of follow-up in the DAYBREAK open-label extension trial. Mult. Scler. J. 2022, 28, 1944–1962. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; D’Haens, G.; Wolf, D.C.; Jovanovic, I.; Hanauer, S.B.; Ghosh, S.; Petersen, A.; Hua, S.Y.; Lee, J.H.; et al. Ozanimod as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2021, 385, 1280–1291. [Google Scholar] [CrossRef]
- Konen, F.F.; Mohn, N.; Witte, T.; Schefzyk, M.; Wiestler, M.; Lovric, S.; Hufendiek, K.; Schwenkenbecher, P.; Suhs, K.W.; Friese, M.A.; et al. Treatment of autoimmunity: The impact of disease-modifying therapies in multiple sclerosis and comorbid autoimmune disorders. Autoimmun. Rev. 2023, 22, 103312. [Google Scholar] [CrossRef]
- Tłustochowicz, M.; Wierzba, W.; Marczak, M.; Tłustochowicz, W.; Śliwczyński, A.; Raciborski, F.; Kwiatkowska, B.; Brzozowska, M.; Jacyna, A.; Kisiel, B. Trends in psoriatic arthritis epidemiology in Poland. Rheumatol. Int. 2021, 41, 139–145. [Google Scholar] [CrossRef]
- Almutairi, K.B.; Nossent, J.C.; Preen, D.B.; Keen, H.I.; Inderjeeth, C.A. The prevalence of rheumatoid arthritis: A systematic review of population-based studies. J. Rheumatol. 2021, 48, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Crossfield, S.S.R.; Marzo-Ortega, H.; Kingsbury, S.R.; Pujades-Rodriguez, M.; Conaghan, P.G. Changes in ankylosing spondylitis incidence, prevalence and time to diagnosis over two decades. RMD Open 2021, 7, e001888. [Google Scholar] [CrossRef] [PubMed]
- Bibeau, K.; Pandya, A.G.; Ezzedine, K.; Jones, H.; Gao, J.; Lindley, A.; Harris, J.E. Vitiligo prevalence and quality of life among adults in Europe, Japan and the USA. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1831–1844. [Google Scholar] [CrossRef]
- Bylund, S.; von Kobyletzki, L.B.; Svalstedt, M.; Svensson, Å. Prevalence and incidence of atopic dermatitis: A systematic review. Acta Derm. Venereol. 2020, 100, 320–329. [Google Scholar] [CrossRef]
- Borzęcki, A.; Koncewicz, A.; Raszewska-Famielec, M.; Dudra-Jastrzębska, M. Epidemiology of psoriasis in the years 2008–2015 in Poland. Prz. Dermatol. 2018, 105, 693–700. [Google Scholar] [CrossRef]
- Holko, P.; Kawalec, P.; Stawowczyk, E. Prevalence and drug treatment practices of inflammatory bowel diseases in Poland in the years 2012-2014: An analysis of nationwide databases. Eur. J. Gastroenterol. Hepatol. 2018, 30, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Mobasseri, M.; Shirmohammadi, M.; Amiri, T.; Vahed, N.; Fard, H.H.; Ghojazadeh, M. Prevalence and incidence of type 1 diabetes in the world: A systematic review and meta-analysis. Health Promot. Perspect. 2020, 10, 98–115. [Google Scholar] [CrossRef]
- Jaskólska, M.; Chylińska, M.; Masiak, A.; Siemiński, M.; Ziętkiewicz, M.; Czuszyńska, Z.; Smoleńska, Ż.; Zdrojewski, Z. Neuro-Sjögren: Uncommon or underestimated problem? Brain Behav. 2020, 10, e01665. [Google Scholar] [CrossRef]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef]
- Lee, H.J.; Li, C.W.; Hammerstad, S.S.; Stefan, M.; Tomer, Y. Immunogenetics of autoimmune thyroid diseases: A comprehensive review. J. Autoimmun. 2015, 64, 82–90. [Google Scholar] [CrossRef]
- Gandhi, D.N.; Crespin Henriquez, I.P.; Salvador, T.E.; Farrukh, A.M.; Quintanilla Cardona, E.A.; Zakraoui, R.S.; Iglesias Claros, A.A.; Kaiprath, S.; Izaguirre Membreño, A.; Gomez Coral, M.I. Hashimoto’s thyroiditis: A comprehensive review of pathogenesis, clinical manifestations, and management strategies. Ann. Rev. Res. 2023, 10, 555787. [Google Scholar]
- Cao, F.; Liu, Y.C.; Ni, Q.Y.; Chen, Y.; Wan, C.H.; Liu, S.Y.; Tao, L.M.; Jiang, Z.X.; Ni, J.; Pan, H.F. Temporal trends in the prevalence of autoimmune diseases from 1990 to 2019. Autoimmun. Rev. 2023, 22, 103359. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, P.; de Remigis, A.; Rose, N.R. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun. Rev. 2014, 13, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best. Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101367. [Google Scholar] [CrossRef]
- Gautam, S.; Bhattarai, A.; Shah, S.; Thapa, S.; Gyawali, P.; Khanal, P.; Kharel, A.; Sharma, P.; Subedi, P.; Chand, S.; et al. The association of multiple sclerosis with thyroid disease: A meta-analysis. Mult. Scler. Relat. Disord. 2023, 80, 105103. [Google Scholar] [CrossRef]
- Edwards, N.C.; Munsell, M.; Menzin, J.; Phillips, A.L. Comorbidity in US patients with multiple sclerosis. Patient Relat. Outcome Meas. 2018, 9, 97–102. [Google Scholar] [CrossRef]
- Poursadeghfard, M.; Mallahzadeh, A.; Hamidi, A.; Owjfard, M. Thyroid autoantibodies in newly diagnosed multiple sclerosis patients: A cross-sectional study. Health Sci. Rep. 2024, 7, e2247. [Google Scholar] [CrossRef] [PubMed]
- Castello, R.; Caputo, M. Thyroid diseases and gender. Ital. J. Gend.-Specif. Med. 2019, 5, 136–141. [Google Scholar]
- Yang, J.; Sun, Y.; Zhou, X.; Zhang, D.; Xu, Z.; Cao, J.; Fan, B. Risk of secondary autoimmune diseases with alemtuzumab treatment for multiple sclerosis: A systematic review and meta-analysis. Front. Immunol. 2024, 15, 1343971. [Google Scholar]
- Zhang, J.; Shi, S.; Zhang, Y.; Luo, J.; Xiao, Y.; Meng, L.; Yang, X. Alemtuzumab versus interferon beta 1a for relapsing-remitting multiple sclerosis. Cochrane Database Syst. Rev. 2017, 11, CD010968. [Google Scholar] [CrossRef]
| Characteristic | |
|---|---|
| Total number of PwMSs | 580 |
| Sex, n (%) | |
| – Female | 431 (71.71%) |
| – Male | 170 (28.29%) |
| Age, mean ± SD (range) | 42.88 ± 12.56 (range: 18–73) |
| Age at MS diagnosis, mean ± SD | 33.63 ± 11.22 |
| Disease duration, mean ± SD | 9.82 ± 7.58 |
| MS Phenotype, n (%) | |
| – RRMS | 469 (80.86%) |
| – SPMS | 48 (8.28%) |
| – PPMS | 44 (7.58%) |
| – RES-RRMS | 19 (3.28%) |
| EDSS score, median ± IQR | 2.50 (IQR: 1.25–3.75) |
| Treatment Status, n (%) | |
| – LETA | 301 (51.90%) |
| – HETA | 216 (37.24%) |
| – No treatment | 63 (10.86%) |
| Most Common DMTs, n (%) | |
| – Dimethyl fumarate | 168 (28.97%) |
| – Teriflunomide | 64 (11.03%) |
| – Ocrelizumab | 60 (10.34%) |
| – Ofatumumab | 27 (4.66%) |
| Measurement | Mean ± SD | Below Normal (n, %) | Normal Range (n, %) | High/Toxic (n, %) |
|---|---|---|---|---|
| Vitamin D3 serum level | 34.52 ± 27.20 ng/mL | 237 (47.59%) | 250 (50.20%) | 11 (2.29%) |
| TSH level | 2.06 ± 4.54 µIU/mL | 12 (2.42%) | 469 (94.75%) | 14 (2.83%) |
| MS Subtype | Patients with Autoimmune Comorbidities | Patients with Co-Occurring Thyroid Disease |
|---|---|---|
| RRMS | 18.12% | 14.29% |
| SPMS | 16.67% | 14.58% |
| PPMS | 11.36% | 6.82% |
| RRMS-RES | 0.0% | 0.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwan, M.; Wójtowicz, W.; Milczarek, J.; Wyroba, N.; Wydrych, Z.; Falger, O.; Rzepka, M.; Chmiela, T.; Toś, M.; Siuda, J. The Relationship Between Autoimmune Disorders and Multiple Sclerosis: Clinical Insights and Therapeutic Approaches. Brain Sci. 2025, 15, 588. https://doi.org/10.3390/brainsci15060588
Iwan M, Wójtowicz W, Milczarek J, Wyroba N, Wydrych Z, Falger O, Rzepka M, Chmiela T, Toś M, Siuda J. The Relationship Between Autoimmune Disorders and Multiple Sclerosis: Clinical Insights and Therapeutic Approaches. Brain Sciences. 2025; 15(6):588. https://doi.org/10.3390/brainsci15060588
Chicago/Turabian StyleIwan, Magdalena, Weronika Wójtowicz, Jakub Milczarek, Natalia Wyroba, Zuzanna Wydrych, Olga Falger, Michalina Rzepka, Tomasz Chmiela, Mateusz Toś, and Joanna Siuda. 2025. "The Relationship Between Autoimmune Disorders and Multiple Sclerosis: Clinical Insights and Therapeutic Approaches" Brain Sciences 15, no. 6: 588. https://doi.org/10.3390/brainsci15060588
APA StyleIwan, M., Wójtowicz, W., Milczarek, J., Wyroba, N., Wydrych, Z., Falger, O., Rzepka, M., Chmiela, T., Toś, M., & Siuda, J. (2025). The Relationship Between Autoimmune Disorders and Multiple Sclerosis: Clinical Insights and Therapeutic Approaches. Brain Sciences, 15(6), 588. https://doi.org/10.3390/brainsci15060588