
The Potential Role of Psilocybin in Traumatic Brain Injury Recovery: A Narrative Review


Abstract
1. Introduction
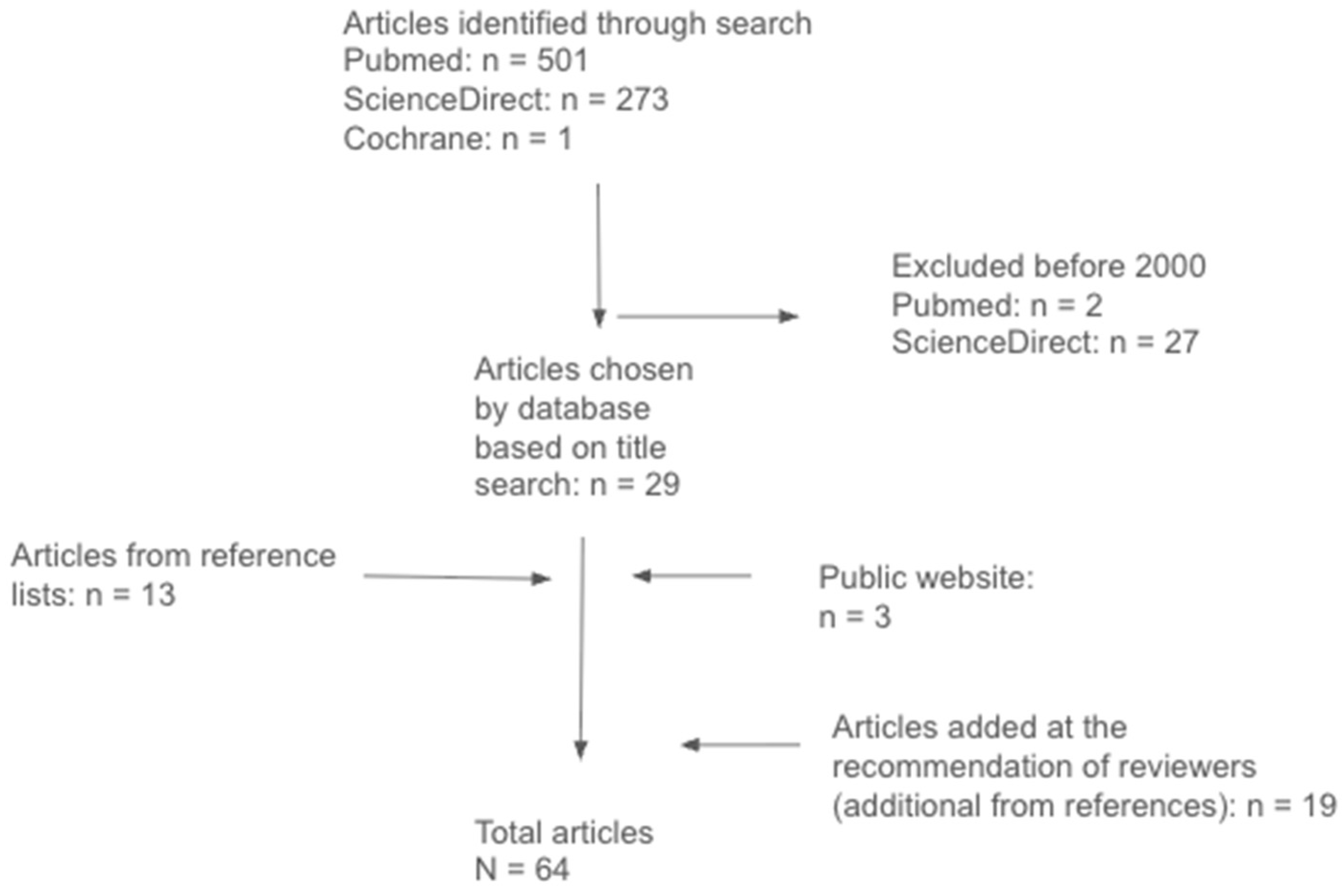
2. Methods
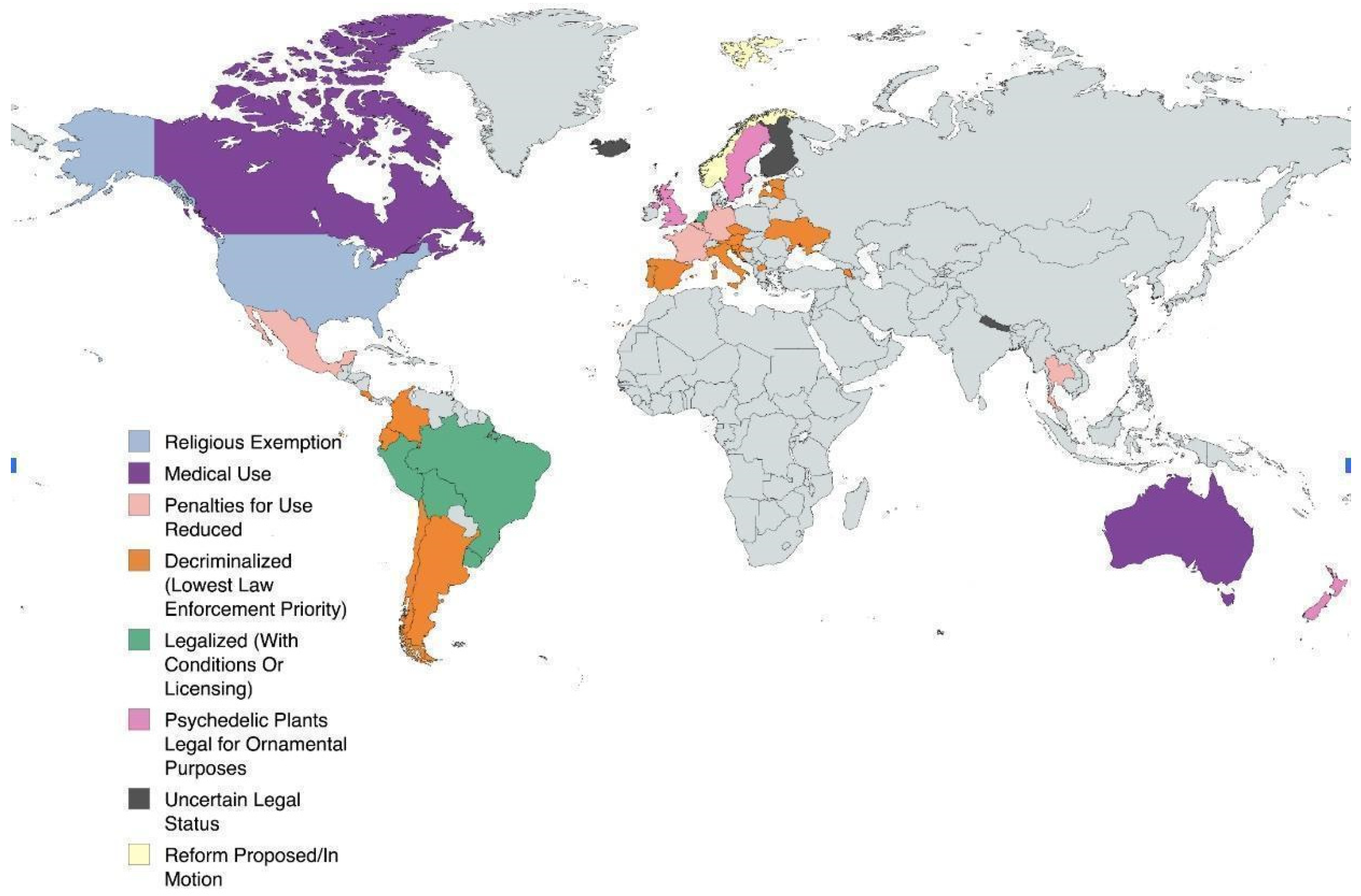
3. Legality
4. Indications
5. Biochemistry
6. Pharmacokinetics
7. Anti-Inflammatory Effects
8. Plasticity
9. Cognitive Effects
10. Psychological Effects
11. Adverse Effects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Common Adverse Effects | Mechanism of Action |
|---|---|
| Headache | Possibly due to release of nitric oxide [57] |
| Nausea | Possibly the result of agonist action on 5-HT2A and 5-HT3 receptors affecting both central and peripheral serotonergic pathways [58,59] |
| Dizziness | Increases entropy of neural signaling, which can disrupt the ability to maintain a sense of balance and spatial orientation [60] |
| Elevated blood pressure | 5-HT2A activation can result in vasoconstriction and increased cardiac output [58] |
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the Global Incidence of Traumatic Brain Injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Galgano, M.; Toshkezi, G.; Qiu, X.; Russell, T.; Chin, L.; Zhao, L.-R. Traumatic Brain Injury: Current Treatment Strategies and Future Endeavors. Cell Transplant. 2017, 26, 1118–1130. [Google Scholar] [CrossRef]
- Raghupathi, R. Cell Death Mechanisms Following Traumatic Brain Injury. Brain Pathol. 2004, 14, 215–222. [Google Scholar] [CrossRef]
- Braun, M.; Khan, Z.T.; Khan, M.B.; Kumar, M.; Ward, A.; Achyut, B.R.; Arbab, A.S.; Hess, D.C.; Hoda, M.N.; Baban, B.; et al. Selective Activation of Cannabinoid Receptor-2 Reduces Neuroinflammation after Traumatic Brain Injury via Alternative Macrophage Polarization. Brain Behav. Immun. 2018, 68, 224–237. [Google Scholar] [CrossRef]
- Gotvaldová, K.; Hájková, K.; Borovička, J.; Jurok, R.; Cihlářová, P.; Kuchař, M. Stability of Psilocybin and Its Four Analogs in the Biomass of the Psychotropic Mushroom Psilocybe cubensis. Drug Test. Anal. 2021, 13, 439–446. [Google Scholar] [CrossRef]
- Allen, J.; Dames, S.S.; Foldi, C.J.; Shultz, S.R. Psychedelics for acquired brain injury: A review of molecular mechanisms and therapeutic potential. Mol. Psychiatry 2024, 29, 671–685. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Carter, G.T.; Aggarwal, S.K.; Holland, J.; Khan, S.M. Psychedelics for Brain Injury: A Mini-Review. Front. Neurol. 2021, 12, 685085. [Google Scholar] [CrossRef]
- Sharma, P.; Nguyen, Q.A.; Matthews, S.J.; Carpenter, E.; Mathews, D.B.; Patten, C.A.; Hammond, C.J. Psilocybin history, action and reaction: A narrative clinical review. J. Psychopharmacol. 2023, 37, 849–865. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.S.; Daily, J.E.; Perry, D.A.; Nicol, G.E. Psychedelic Drug Legislative Reform and Legalization in the US. JAMA Psychiatry 2023, 80, 77–83. [Google Scholar] [CrossRef]
- Alpha, P. Psychedelics Legalization & Decriminalization Tracker. Available online: https://psychedelicalpha.com/data/psychedelic-laws (accessed on 3 March 2025).
- Alpha, P. Worldwide Psychedelic Laws. Available online: https://psychedelicalpha.com/data/worldwide-psychedelic-laws (accessed on 11 March 2025).
- Johnson, M.W.; Griffiths, R.R. Potential Therapeutic Effects of Psilocybin. Neurotherapeutics 2017, 14, 734–740. [Google Scholar] [CrossRef]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin Produces Substantial and Sustained Decreases in Depression and Anxiety in Patients with Life-Threatening Cancer: A Randomized Double-Blind Trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.L.; Bolstridge, M.; Rucker, J.; Day, C.M.J.; Erritzoe, D.; Kaelen, M.; Bloomfield, M.; Rickard, J.A.; Forbes, B.; Feilding, A.; et al. Psilocybin with Psychological Support for Treatment-Resistant Depression: An Open-Label Feasibility Study. Lancet Psychiatry 2016, 3, 619–627. [Google Scholar] [CrossRef]
- Goodwin, G.M.; Croal, M.; Feifel, D.; Kelly, J.R.; Marwood, L.; Mistry, S.; O’keane, V.; Peck, S.K.; Simmons, H.; Sisa, C.; et al. Psilocybin for treatment resistant depression in patients taking a concomitant SSRI medication. Neuropsychopharmacology 2023, 48, 1492–1499. [Google Scholar] [CrossRef]
- Erkizia-Santamaría, I.; Alles-Pascual, R.; Horrillo, I.; Meana, J.; Ortega, J. Serotonin 5-HT2A, 5-HT2c and 5-HT1A Receptor Involvement in the Acute Effects of Psilocybin in Mice. In Vitro Pharmacological Profile and Modulation of Thermoregulation and Head-Twich Response. Biomed. Pharmacother. 2022, 154, 113612. [Google Scholar] [CrossRef]
- Ivan, V.E.; Tomàs-Cuesta, D.P.; Esteves, I.M.; Luczak, A.; Mohajerani, M.; McNaughton, B.L.; Gruber, A.J. Psilocybin Reduces Functional Correlation and the Encoding of Spatial Information by Neurons in Mouse Retrosplenial Cortex. Eur. J. Neurosci. 2024, 60, 6395–6407. [Google Scholar] [CrossRef] [PubMed]
- MacCallum, C.A.; Lo, L.A.; Pistawka, C.A.; Deol, J.K. Therapeutic Use of Psilocybin: Practical Considerations for Dosing and Administration. Front. Psychiatry 2022, 13, 1040217. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Romeu, A.; Barrett, F.S.; Carbonaro, T.M.; Johnson, M.W.; Griffiths, R.R. Optimal Dosing for Psilocybin Pharmacotherapy: Considering Weight-Adjusted and Fixed Dosing Approaches. J. Psychopharmacol. 2021, 35, 353–361. [Google Scholar] [CrossRef]
- Otto, M.E.; van der Heijden, K.V.; Schoones, J.W.; van Esdonk, M.J.; Borghans, L.G.J.M.; Jacobs, G.E.; van Hasselt, J.G.C. Clinical Pharmacokinetics of Psilocin After Psilocybin Administration: A Systematic Review and Post-Hoc Analysis. Clin. Pharmacokinet. 2025, 64, 53–66. [Google Scholar] [CrossRef]
- Huang, Z.; Yao, Y.; Di, R.; Zhang, J.; Pan, Y.; Liu, G. De Novo Biosynthesis of Antidepressant Psilocybin in Escherichia coli. Microb. Biotechnol. 2025, 18, e70135. [Google Scholar] [CrossRef]
- Horita, A.; Weber, L.J. Dephosphorylation of psilocybin to psilocin by alkaline phosphatase. Exp. Biol. Med. 1961, 106, 32–34. [Google Scholar] [CrossRef]
- Horita, A.; Weber, L. The enzymic dephosphorylation and oxidation of psilocybin and psilocin by mammalian tissue homogenates. Biochem. Pharmacol. 1961, 7, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Hasler, F.; Bourquin, D.; Brenneisen, R.; Vollenweider, F.X. Renal excretion profiles of psilocin following oral administration of psilocybin: A controlled study in man. J. Pharm. Biomed. Anal. 2002, 30, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Kamata, T.; Katagi, M.; Kamata, H.T.; Miki, A.; Shima, N.; Zaitsu, K.; Nishikawa, M.; Tanaka, E.; Honda, K.; Tsuchihashi, H. Metabolism of the psychotomimetic tryptamine derivative 5-methoxy-NN-diisopropyltryptamine in humans: Identification and quantification of its urinary metabolites. Drug Metab. Dispos. 2006, 34, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Manevski, N.; Kurkela, M.; Höglund, C.; Mauriala, T.; Court, M.H.; Yli-Kauhaluoma, J.; Finel, M. Glucuronidation of psilocin and 4-hydroxyindole by the human UDP-glucuronosyltransferases. Drug Metab. Dispos. 2010, 38, 386–395. [Google Scholar] [CrossRef]
- Szpręgiel, I.; Bysiek, A. Psilocybin and the glutamatergic pathway: Implications for the treatment of neuropsychiatric diseases. Pharmacol. Rep. 2024, 76, 1297–1304. [Google Scholar] [CrossRef]
- Meinhardt, M.W.; Pfarr, S.; Fouquet, G.; Rohleder, C.; Meinhardt, M.L.; Barroso-Flores, J.; Hoffmann, R.; Jeanblanc, J.; Paul, E.; Wagner, K.; et al. Psilocybin targets a common molecular mechanism for cognitive impairment and increased craving in alcoholism. Sci. Adv. 2021, 7, eabh2399. [Google Scholar] [CrossRef]
- Holze, F.; Becker, A.M.; Kolaczynska, K.E.; Duthaler, U.; Liechti, M.E. Pharmacokinetics and Pharmacodynamics of Oral Psilocybin Administration in Healthy Participants. Clin. Pharmacol. Ther. 2023, 113, 822–831. [Google Scholar] [CrossRef]
- Robinson, G.I.; Li, D.; Wang, B.; Rahman, T.; Gerasymchuk, M.; Hudson, D.; Kovalchuk, O.; Kovalchuk, I. Psilocybin and Eugenol Reduce Inflammation in Human 3D EpiIntestinal Tissue. Life 2023, 13, 2345. [Google Scholar] [CrossRef]
- Mason, N.; Szabo, A.; Kuypers, K.; Mallaroni, P.; Fornell, R.d.l.T.; Reckweg, J.; Tse, D.; Hutten, N.; Feilding, A.; Ramaekers, J. Psilocybin Induces Acute and Persisting Alterations in Immune Status in Healthy Volunteers: An Experimental, Placebo-Controlled Study. Brain Behav. Immun. 2023, 114, 299–310. [Google Scholar] [CrossRef]
- Jasey, N.; Ward, I. Neuroplasticity in Brain Injury: Maximizing Recovery. Curr. Phys. Med. Rehabil. Rep. 2019, 7, 333–340. [Google Scholar] [CrossRef]
- Jorge, R.E.; Acion, L.; Starkstein, S.E.; Magnotta, V. Hippocampal Volume and Mood Disorders After Traumatic Brain Injury. Biol. Psychiatry 2007, 62, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Monti, J.M.; Voss, M.W.; Pence, A.; McAuley, E.; Kramer, A.F.; Cohen, N.J. History of Mild Traumatic Brain Injury Is Associated with Deficits in Relational Memory, Reduced Hippocampal Volume, and Less Neural Activity Later in Life. Front. Aging Neurosci. 2013, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Shao, L.-X.; Liao, C.; Gregg, I.; Davoudian, P.A.; Savalia, N.K.; Delagarza, K.; Kwan, A.C. Psilocybin Induces Rapid and Persistent Growth of Dendritic Spines in Frontal Cortex In Vivo. Neuron 2021, 109, 2535–2544.e4. [Google Scholar] [CrossRef]
- Raval, N.R.; Johansen, A.; Donovan, L.L.; Ros, N.F.; Ozenne, B.; Hansen, H.D.; Knudsen, G.M. A Single Dose of Psilocybin Increases Synaptic Density and Decreases 5-HT2A Receptor Density in the Pig Brain. Int. J. Mol. Sci. 2021, 22, 835. [Google Scholar] [CrossRef]
- Moliner, R.; Girych, M.; Brunello, C.A.; Kovaleva, V.; Biojone, C.; Enkavi, G.; Antenucci, L.; Kot, E.F.; Goncharuk, S.A.; Kaurinkoski, K.; et al. Psychedelics Promote Plasticity by Directly Binding to BDNF Receptor TrkB. Nat. Neurosci. 2023, 26, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Mallaroni, P.; Mason, N.L.; Reckweg, J.T.; Paci, R.; Ritscher, S.; Toennes, S.W.; Theunissen, E.L.; Kuypers, K.P.; Ramaekers, J.G. Assessment of the Acute Effects of 2C-B vs. Psilocybin on Subjective Experience, Mood, and Cognition. Clin. Pharmacol. Ther. 2023, 114, 423–433. [Google Scholar] [CrossRef]
- Vollenweider, F.X.; Csomor, P.A.; Knappe, B.; Geyer, M.A.; Quednow, B.B. The Effects of the Preferential 5-HT2A Agonist Psilocybin on Prepulse Inhibition of Startle in Healthy Human Volunteers Depend on Interstimulus Interval. Neuropsychopharmacology 2007, 32, 1876–1887. [Google Scholar] [CrossRef]
- Rucker, J.J.; Marwood, L.; Ajantaival, R.-L.J.; Bird, C.; Eriksson, H.; Harrison, J.; Lennard-Jones, M.; Mistry, S.; Saldarini, F.; Stansfield, S.; et al. The Effects of Psilocybin on Cognitive and Emotional Functions in Healthy Participants: Results from a Phase 1, Randomised, Placebo-Controlled Trial Involving Simultaneous Psilocybin Administration and Preparation. J. Psychopharmacol. 2022, 36, 114–125. [Google Scholar] [CrossRef]
- Williams, G.V.; Rao, S.G.; Goldman-Rakic, P.S. The Physiological Role of 5-HT2A Receptors in Working Memory. J. Neurosci. 2002, 22, 2843–2854. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; Stone, J.M.; Reed, L.J.; Colasanti, A.; Tyacke, R.J.; Leech, R.; Malizia, A.L.; Murphy, K.; et al. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc. Natl. Acad. Sci. USA 2012, 109, 2138–2143. [Google Scholar] [CrossRef]
- Carter, O.L.; Burr, D.C.; Pettigrew, J.D.; Wallis, G.M.; Hasler, F.; Vollenweider, F.X. Using Psilocybin to Investigate the Relationship between Attention, Working Memory, and the Serotonin 1A and 2A Receptors. J. Cogn. Neurosci. 2005, 17, 1497–1508. [Google Scholar] [CrossRef] [PubMed]
- Barrett, F.S.; Carbonaro, T.M.; Hurwitz, E.; Johnson, M.W.; Griffiths, R.R. Double-blind comparison of the two hallucinogens psilocybin and dextromethorphan: Effects on cognition. Psychopharmacology 2018, 235, 2915–2927. [Google Scholar] [CrossRef] [PubMed]
- Wittmann, M.; Carter, O.; Hasler, F.; Cahn, B.R.; Grimberg, U.; Spring, P.; Hell, D.; Flohr, H.; Vollenweider, F.X. Effects of psilocybin on time perception and temporal control of behaviour in humans. J. Psychopharmacol. 2007, 21, 50–64. [Google Scholar] [CrossRef]
- Singh, R.; Mason, S.; Lecky, F.; Dawson, J. revalence of Depression after TBI in a Prospective Cohort: The SHEFBIT Study. Brain Inj. 2018, 32, 84–90. [Google Scholar] [CrossRef]
- Bombardier, C.H.; Fann, J.R.; Temkin, N.R.; Esselman, P.C.; Barber, J.; Dikmen, S.S. Rates of Major Depressive Disorder and Clinical Outcomes Following Traumatic Brain Injury. JAMA 2010, 303, 1938–1945. [Google Scholar] [CrossRef]
- Winter, J.; Rice, K.; Amorosi, D.; Rabin, R. Psilocybin-Induced Stimulus Control in the Rat. Pharmacol. Biochem. Behav. 2007, 87, 472–480. [Google Scholar] [CrossRef]
- Holtzheimer, P.E.; Mayberg, H.S. Stuck in a Rut: Rethinking Depression and Its Treatment. Trends Neurosci. 2011, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kraehenmann, R.; Preller, K.H.; Scheidegger, M.; Pokorny, T.; Bosch, O.G.; Seifritz, E.; Vollenweider, F.X. Psilocybin-Induced Decrease in Amygdala Reactivity Correlates with Enhanced Positive Mood in Healthy Volunteers. Biol. Psychiatry 2015, 78, 572–581. [Google Scholar] [CrossRef]
- Kraehenmann, R.; Schmidt, A.; Friston, K.; Preller, K.H.; Seifritz, E.; Vollenweider, F.X. The Mixed Serotonin Receptor Agonist Psilocybin Reduces Threat-Induced Modulation of Amygdala Connectivity. NeuroImage Clin. 2016, 11, 53–60. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Leech, R.; Williams, T.M.; Erritzoe, D.; Abbasi, N.; Bargiotas, T.; Hobden, P.; Sharp, D.J.; Evans, J.; Feilding, A.; et al. Implications for Psychedelic-Assisted Psychotherapy: Functional Magnetic Resonance Imaging Study with Psilocybin. Br. J. Psychiatry 2012, 200, 238–244. [Google Scholar] [CrossRef]
- Goodwin, G.M.; Aaronson, S.T.; Alvarez, O.; Arden, P.C.; Baker, A.; Bennett, J.C.; Bird, C.; Blom, R.E.; Brennan, C.; Brusch, D.; et al. Single-Dose Psilocybin for a Treatment-Resistant Episode of Major Depression. N. Engl. J. Med. 2022, 387, 1637–1648. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; O’Donnell, M.L.; Creamer, M.; McFarlane, A.C.; Clark, C.R.; Silove, D. The Psychiatric Sequelae of Traumatic Injury. Am. J. Psychiatry 2010, 167, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.T.; Danforth, A.; Daroff, R.; Stauffer, C.; Ekman, E.; Agin-Liebes, G.; Trope, A.; Boden, M.T.; Dilley, J.; Mitchell, J.; et al. Psilocybin-Assisted Group Therapy for Demoralized Older Long-Term AIDS Survivor Men: An Open-Label Safety and Feasibility Pilot Study. eClinicalMedicine 2020, 27, 100538. [Google Scholar] [CrossRef]
- Yerubandi, A.; Thomas, J.E.; Alam Bhuiya, N.M.M.; Harrington, C.; Zapata, L.V.; Caballero, J. Acute Adverse Effects of Therapeutic Doses of Psilocybin: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2024, 7, e245960. [Google Scholar] [CrossRef]
- Carbonaro, T.M.; Bradstreet, M.P.; Barrett, F.S.; MacLean, K.A.; Jesse, R.; Johnson, M.W.; Griffiths, R.R. Survey Study of Challenging Experiences after Ingesting Psilocybin Mushrooms: Acute and Enduring Positive and Negative Consequences. J. Psychopharmacol. 2016, 30, 1268–1278. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.W.; Sewell, R.A.; Griffiths, R.R. Psilocybin Dose-Dependently Causes Delayed, Transient Headaches in Healthy Volunteers. Drug Alcohol. Depend. 2012, 123, 132–140. [Google Scholar] [CrossRef]
- Bogenschutz, M.P.; Forcehimes, A.A.; Pommy, J.A.; Wilcox, C.E.; Barbosa, P.; Strassman, R.J. Psilocybin-Assisted Treatment for Alcohol Dependence: A Proof-of-Concept Study. J. Psychopharmacol. 2015, 29, 289–299. [Google Scholar] [CrossRef]
- Johnson, M.W.; Garcia-Romeu, A.; Griffiths, R.R. Long-Term Follow-up of Psilocybin-Facilitated Smoking Cessation. Am. J. Drug Alcohol. Abus. 2017, 43, 55–60. [Google Scholar] [CrossRef]
- Ding, K.; Gupta, P.K.; Diaz-Arrastia, R. Epilepsy after Traumatic Brain Injury. In Translational Research in Traumatic Brain Injury; Laskowitz, D., Grant, G., Eds.; CRC Press/Taylor and Francis Group: Boca Raton, FL, USA, 2016; Chapter 14. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326716/ (accessed on 5 May 2025).
- Soto-Angona, Ó.; Fortea, A.; Fortea, L.; Martínez-Ramírez, M.; Santamarina, E.; Gil López, F.J.; Knudsen, G.M.; Ona, G. Do Classic Psychedelics Increase the Risk of Seizures? A Scoping Review. Eur. Neuropsychopharmacol. 2024, 85, 35–42. [Google Scholar] [CrossRef]
- Esterov, D.; Greenwald, B.D. Autonomic Dysfunction after Mild Traumatic Brain Injury. Brain Sci. 2017, 7, 100. [Google Scholar] [CrossRef]
- Price, L.; Wilson, C.; Grant, G. Blood–Brain Barrier Pathophysiology following Traumatic Brain Injury. In Translational Research in Traumatic Brain Injury; Laskowitz, D., Grant, G., Eds.; CRC Press/Taylor and Francis Group: Boca Raton, FL, USA, 2016; Chapter 4. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326726/ (accessed on 5 May 2025).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmer, C.; Ferber, A.T.; Greenwald, B.D. The Potential Role of Psilocybin in Traumatic Brain Injury Recovery: A Narrative Review. Brain Sci. 2025, 15, 572. https://doi.org/10.3390/brainsci15060572
Palmer C, Ferber AT, Greenwald BD. The Potential Role of Psilocybin in Traumatic Brain Injury Recovery: A Narrative Review. Brain Sciences. 2025; 15(6):572. https://doi.org/10.3390/brainsci15060572
Chicago/Turabian StylePalmer, Charles, Ally T. Ferber, and Brian D. Greenwald. 2025. "The Potential Role of Psilocybin in Traumatic Brain Injury Recovery: A Narrative Review" Brain Sciences 15, no. 6: 572. https://doi.org/10.3390/brainsci15060572
APA StylePalmer, C., Ferber, A. T., & Greenwald, B. D. (2025). The Potential Role of Psilocybin in Traumatic Brain Injury Recovery: A Narrative Review. Brain Sciences, 15(6), 572. https://doi.org/10.3390/brainsci15060572