
Dysautonomia in Alzheimer’s Disease: A Systematic Review

 ,
,  , , , , , , and
, , , , , , and 
Abstract
1. Introduction
2. Materials and Methods
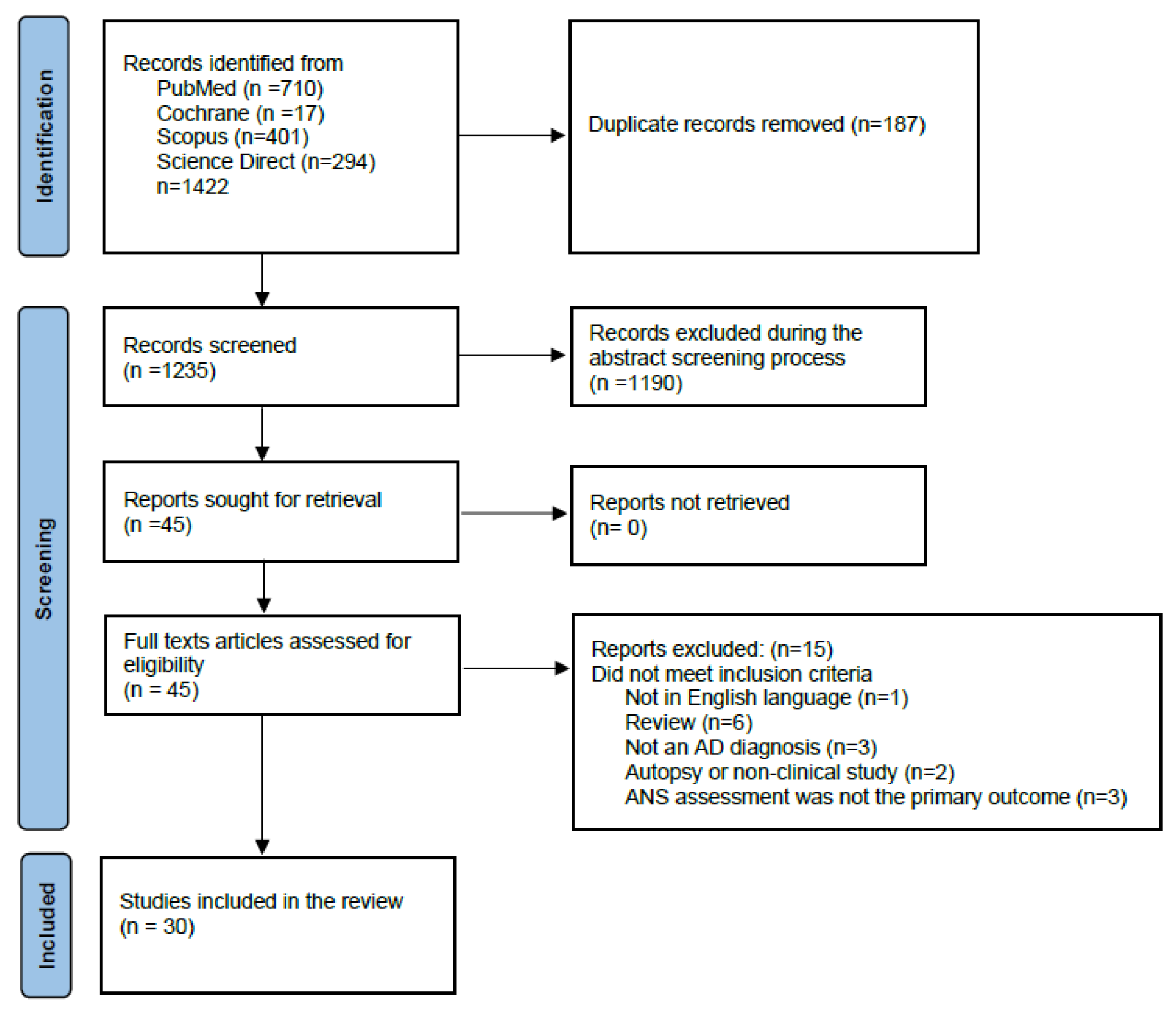
2.1. Review of the Literature
2.2. Inclusion Criteria
- 1.
- All types of observational studies were included: case-control studies, cohort studies, cross-sectional studies, and retrospective studies
- 2.
- A diagnosis of Alzheimer’s disease was a prerequisite
- 3.
- Studies including patients suffering from dementias other than AD were considered when sufficient data on AD were provided
- 4.
- Primary outcome assessment of autonomic dysfunction with specific measurement tools
2.3. Exclusion Criteria
- 1.
- Reviews (systematic or other) and meta-analyses
- 2.
- Animal studies
- 3.
- Autopsy studies with no clinical correlation to dysautonomia
- 4.
- Studies including patients suffering from diseases that may affect the autonomic nervous system (e.g., diabetes mellitus, amyloidosis etc.)
2.4. Data Extraction
2.5. Risk of Bias
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Tools of Assessment
3.2.1. HRV
3.2.2. OH
3.2.3. PPH
3.2.4. SSR
3.2.5. TILT TEST
3.2.6. 123. I-MIBG
3.2.7. Serum /CSF Norepinephrine
3.2.8. Deep Breathing
3.2.9. BR
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DSM | American Psychiatric Association’s Diagnostic and Statistical Manual |
| AD | Alzheimer’s disease |
| PD | Parkinson’s disease |
| COMPASS | Composite Autonomic Symptom Score |
| HRV | heart rate variability |
| LF | low frequency |
| HF | high frequency |
| VLF | very low frequency |
| TSP | total spectral power |
| ANS | autonomic nervous system |
| BPV | blood pressure variability |
| RRIV | R-R interval variation |
| ECG | electrocardiogram |
| OH | orthostatic hypotension |
| PPH | postprandial hypotension |
| BR | baroreflex |
| SSR | Sympathetic Skin Response |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| HC | healthy controls |
| VAD | vascular dementia |
| MCI | mild cognitive impairment |
| DLB | dementia with Lewy bodies |
| PDD | Parkinson’s disease dementia |
| MMSE | Mini Mental State Examination |
| CAMCOG | Cambridge Cognition Examination |
| GDS | Global Deterioration Scale |
| FAB | frontal assessment battery |
| NE | norepinephrine |
References
- Global Status Report on the Public Health Response to Dementia—Exec Summary.Pdf. Available online: https://www.who.int/publications/i/item/9789240033245 (accessed on 24 February 2025).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; 2022. Available online: https://psychiatryonline.org/pb-assets/dsm/update/DSM-5-TR_Neurocognitive-Disorders-Supplement_2022_APA_Publishing.pdf (accessed on 24 February 2025).
- 2024 Alzheimer’s Disease Facts and Figures. J. Alzheimers Dement. 2024, 20, 3708–3821. [CrossRef]
- Jorm, A.F.; Jolley, D. The Incidence of Dementia: A Meta-Analysis. Neurology 1998, 51, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Ishii, M.; Iadecola, C. Metabolic and Non-Cognitive Manifestations of Alzheimer’s Disease: The Hypothalamus as Both Culprit and Target of Pathology. Cell Metab. 2015, 22, 761–776. [Google Scholar] [CrossRef]
- Raudino, F. Non-Cognitive Symptoms and Related Conditions in the Alzheimer’s Disease: A Literature Review. Neurol. Sci. 2013, 34, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Arkin, S.; Mahendra, N. Insight in Alzheimer’s Patients: Results of a Longitudinal Study Using Three Assessment Methods. Am. J. Alzheimers Dis. Other Dement. 2001, 16, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Kato, S. Depression-Dementia Medius: Between Depression and the Manifestation of Dementia Symptoms. Psychogeriatrics 2011, 11, 177–182. [Google Scholar] [CrossRef]
- Kang, J.Y.; Lee, J.S.; Kang, H.; Lee, H.-W.; Kim, Y.K.; Jeon, H.J.; Chung, J.-K.; Lee, M.C.; Cho, M.J.; Lee, D.S. Regional Cerebral Blood Flow Abnormalities Associated with Apathy and Depression in Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2012, 26, 217–224. [Google Scholar] [CrossRef]
- Wuwongse, S.; Chang, R.C.-C.; Law, A.C.K. The Putative Neurodegenerative Links between Depression and Alzheimer’s Disease. Prog. Neurobiol. 2010, 91, 362–375. [Google Scholar] [CrossRef]
- Braak, H.; Braak, E. Neuropathological Stageing of Alzheimer-Related Changes. Acta Neuropathol. 1991, 82, 239–259. [Google Scholar] [CrossRef]
- Iadecola, C. The Overlap Between Neurodegenerative and Vascular Factors in the Pathogenesis of Dementia. Acta Neuropathol. 2010, 120, 287–296. [Google Scholar] [CrossRef]
- Wiesmann, M.; Kiliaan, A.J.; Claassen, J.A.H.R. Vascular Aspects of Cognitive Impairment and Dementia. J. Cereb. Blood Flow. Metab. 2013, 33, 1696–1706. [Google Scholar] [CrossRef]
- Claassen, J.A.H.R.; Jansen, R.W.M.M. Cholinergically Mediated Augmentation of Cerebral Perfusion in Alzheimer’s Disease and Related Cognitive Disorders: The Cholinergic-Vascular Hypothesis. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Van Beek, A.H.E.A.; Claassen, J.A.H.R. The Cerebrovascular Role of the Cholinergic Neural System in Alzheimer’s Disease. Behav. Brain Res. 2011, 221, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Femminella, G.D.; Rengo, G.; Komici, K.; Iacotucci, P.; Petraglia, L.; Pagano, G.; de Lucia, C.; Canonico, V.; Bonaduce, D.; Leosco, D.; et al. Autonomic Dysfunction in Alzheimer’s Disease: Tools for Assessment and Review of the Literature. J. Alzheimers Dis. 2014, 42, 369–377. [Google Scholar] [CrossRef]
- Berrios, G.E.; Campbell, C.; Politynska, B.E. Autonomic Failure, Depression and Anxiety in Parkinson’s Disease. Br. J. Psychiatry 1995, 166, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Sletten, D.M.; Suarez, G.A.; Low, P.A.; Mandrekar, J.; Singer, W. COMPASS 31: A Refined and Abbreviated Composite Autonomic Symptom Score. Mayo Clin. Proc. 2012, 87, 1196–1201. [Google Scholar] [CrossRef]
- Malliani, A.; Pagani, M.; Lombardi, F.; Cerutti, S. Cardiovascular Neural Regulation Explored in the Frequency Domain. Circulation 1991, 84, 482–492. [Google Scholar] [CrossRef]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R.E.; et al. Heart Rate Variability: Standards of Measurement, Physiological Interpretation and Clinical Use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Mackay, J.D.; Page, M.M.; Cambridge, J.; Watkins, P.J. Diabetic Autonomic Neuropathy. The Diagnostic Value of Heart Rate Monitoring. Diabetologia 1980, 18, 471–478. [Google Scholar] [CrossRef]
- Bellelli, G.; Pezzini, A.; Bianchetti, A.; Trabucchi, M. Increased Blood Pressure Variability May Be Associated with Cognitive Decline in Hypertensive Elderly Subjects with No Dementia. Arch. Intern. Med. 2002, 162, 483–484. [Google Scholar] [CrossRef]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-Regulation, Adaptation, and Health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef] [PubMed]
- de Heus, R.A.A.; Tzourio, C.; Lee, E.J.L.; Opozda, M.; Vincent, A.D.; Anstey, K.J.; Hofman, A.; Kario, K.; Lattanzi, S.; Launer, L.J.; et al. Association Between Blood Pressure Variability With Dementia and Cognitive Impairment: A Systematic Review and Meta-Analysis. Hypertension 2021, 78, 1478–1489. [Google Scholar] [CrossRef] [PubMed]
- Persson, A.; Solders, G. R-R Variations, a Test of Autonomic Dysfunction. Acta Neurol. Scand. 1983, 67, 285–293. [Google Scholar] [CrossRef]
- Parry, S.W.; Reeve, P.; Lawson, J.; Shaw, F.E.; Davison, J.; Norton, M.; Frearson, R.; Kerr, S.; Newton, J.L. The Newcastle Protocols 2008: An Update on Head-up Tilt Table Testing and the Management of Vasovagal Syncope and Related Disorders. Heart 2009, 95, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Mellingsæter, M.R.; Wyller, T.B.; Ranhoff, A.H.; Bogdanovic, N.; Wyller, V.B. Reduced Sympathetic Response to Head-up Tilt in Subjects with Mild Cognitive Impairment or Mild Alzheimer’s Dementia. Dement. Geriatr. Cogn. Disord. Extra 2015, 5, 107–115. [Google Scholar] [CrossRef]
- de Heus, R.A.A.; de Jong, D.L.K.; Rijpma, A.; Lawlor, B.A.; Olde Rikkert, M.G.M.; Claassen, J.A.H.R. Orthostatic Blood Pressure Recovery Is Associated With the Rate of Cognitive Decline and Mortality in Clinical Alzheimer’s Disease. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 2169–2176. [Google Scholar] [CrossRef]
- Allan, L.M.; Ballard, C.G.; Allen, J.; Murray, A.; Davidson, A.W.; McKeith, I.G.; Kenny, R.A. Autonomic Dysfunction in Dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 671–677. [Google Scholar] [CrossRef]
- Siennicki-Lantz, A.; Lilja, B.; Elmståhl, S. Orthostatic Hypotension in Alzheimer’s Disease: Result or Cause of Brain Dysfunction? Aging Clin. Exp. Res. 1999, 11, 155–160. [Google Scholar] [CrossRef]
- Jansen, R.W.; Lipsitz, L.A. Postprandial Hypotension: Epidemiology, Pathophysiology, and Clinical Management. Ann. Intern. Med. 1995, 122, 286–295. [Google Scholar] [CrossRef]
- Meel-van den Abeelen, A.S.S.; Lagro, J.; Gommer, E.D.; Reulen, J.P.H.; Claassen, J.A.H.R. Baroreflex Function Is Reduced in Alzheimer’s Disease: A Candidate Biomarker? Neurobiol. Aging 2013, 34, 1170–1176. [Google Scholar] [CrossRef]
- Vetrugno, R.; Liguori, R.; Cortelli, P.; Montagna, P. Sympathetic Skin Response: Basic Mechanisms and Clinical Applications. Clin. Auton. Res. 2003, 13, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Negami, M.; Maruta, T.; Takeda, C.; Adachi, Y.; Yoshikawa, H. Sympathetic Skin Response and Heart Rate Variability as Diagnostic Tools for the Differential Diagnosis of Lewy Body Dementia and Alzheimer’s Disease: A Diagnostic Test Study. BMJ Open 2013, 3, e001796. [Google Scholar] [CrossRef]
- Toru, S.; Kanouchi, T.; Yokota, T.; Yagi, Y.; Machida, A.; Kobayashi, T. Utility of Autonomic Function Tests to Differentiate Dementia with Lewy Bodies and Parkinson Disease with Dementia from Alzheimer Disease. Eur. Neurol. 2018, 79, 27–32. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Haglund, M.; Heyman, I.; Javanshiri, K. Progressive QTc Prolongation and Reduced Heart Rate Variability in Dementia with Lewy Bodies Compared to Alzheimer’s Disease. Park. Relat. Disord. 2024, 122, 106947. [Google Scholar] [CrossRef]
- Nair, S.S.; Govindankutty, M.M.; Balakrishnan, M.; Prasad, K.; Sathyaprabha, T.N.; Udupa, K. Investigation of Autonomic Dysfunction in Alzheimer’s Disease-A Computational Model-Based Approach. Brain Sci. 2023, 13, 1322. [Google Scholar] [CrossRef] [PubMed]
- Omoya, R.; Miyajima, M.; Ohta, K.; Suzuki, Y.; Aoki, A.; Fujiwara, M.; Watanabe, T.; Yoshida, N.; Suwa, H.; Kawara, T.; et al. Heart Rate Response to Orthostatic Challenge in Patients with Dementia with Lewy Bodies and Alzheimer’s Disease. Psychogeriatrics 2021, 21, 62–70. [Google Scholar] [CrossRef]
- Kim, M.S.; Yoon, J.H.; Hong, J.M. Early Differentiation of Dementia with Lewy Bodies and Alzheimer’s Disease: Heart Rate Variability at Mild Cognitive Impairment Stage. Clin. Neurophysiol. 2018, 129, 1570–1578. [Google Scholar] [CrossRef] [PubMed]
- Kasanuki, K.; Iseki, E.; Fujishiro, H.; Ando, S.; Sugiyama, H.; Kitazawa, M.; Chiba, Y.; Sato, K.; Arai, H. Impaired Heart Rate Variability in Patients with Dementia with Lewy Bodies: Efficacy of Electrocardiogram as a Supporting Diagnostic Marker. Park. Relat. Disord. 2015, 21, 749–754. [Google Scholar] [CrossRef]
- de Vilhena Toledo, M.A.; Junqueira, L.F. Cardiac Autonomic Modulation and Cognitive Status in Alzheimer’s Disease. Clin. Auton. Res. 2010, 20, 11–17. [Google Scholar] [CrossRef]
- Allan, L.M.; Kerr, S.R.J.; Ballard, C.G.; Allen, J.; Murray, A.; McLaren, A.T.; Kenny, R.A. Autonomic Function Assessed by Heart Rate Variability Is Normal in Alzheimer’s Disease and Vascular Dementia. Dement. Geriatr. Cogn. Disord. 2005, 19, 140–144. [Google Scholar] [CrossRef]
- Zulli, R.; Nicosia, F.; Borroni, B.; Agosti, C.; Prometti, P.; Donati, P.; De Vecchi, M.; Romanelli, G.; Grassi, V.; Padovani, A. QT Dispersion and Heart Rate Variability Abnormalities in Alzheimer’s Disease and in Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 2135–2139. [Google Scholar] [CrossRef] [PubMed]
- Giubilei, F.; Strano, S.; Imbimbo, B.P.; Tisei, P.; Calcagnini, G.; Lino, S.; Frontoni, M.; Santini, M.; Fieschi, C. Cardiac Autonomic Dysfunction in Patients with Alzheimer Disease: Possible Pathogenetic Mechanisms. Alzheimer Dis. Assoc. Disord. 1998, 12, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Aharon-Peretz, J.; Harel, T.; Revach, M.; Ben-Haim, S.A. Increased Sympathetic and Decreased Parasympathetic Cardiac Innervation in Patients with Alzheimer’s Disease. Arch. Neurol. 1992, 49, 919–922. [Google Scholar] [CrossRef]
- Franceschi, M.; Ferini-Strambi, L.; Minicucci, F.; Sferrazza-Papa, A.; Smirne, S. Signs of Cardiac Autonomic Dysfunction during Sleep in Patients with Alzheimer’s Disease. Gerontology 1986, 32, 327–334. [Google Scholar] [CrossRef]
- Freidenberg, D.L.; Shaffer, L.E.T.; Macalester, S.; Fannin, E.A. Orthostatic Hypotension in Patients with Dementia: Clinical Features and Response to Treatment. Cogn. Behav. Neurol. 2013, 26, 105–120. [Google Scholar] [CrossRef] [PubMed]
- van Beek, A.H.E.A.; Sijbesma, J.C.; Olde Rikkert, M.G.M.; Claassen, J.A.H.R. Galantamine Does Not Cause Aggravated Orthostatic Hypotension in People with Alzheimer’s Disease. J. Am. Geriatr. Soc. 2010, 58, 409–410. [Google Scholar] [CrossRef]
- Idiaquez, J.; Rios, L.; Sandoval, E. Postprandial Hypotension in Alzheimer’s Disease. Clin. Auton. Res. 1997, 7, 119–120. [Google Scholar] [CrossRef]
- Szili-Török, T.; Kálmán, J.; Paprika, D.; Dibó, G.; Rózsa, Z.; Rudas, L. Depressed Baroreflex Sensitivity in Patients with Alzheimer’s and Parkinson’s Disease. Neurobiol. Aging 2001, 22, 435–438. [Google Scholar] [CrossRef]
- Pascualy, M.; Petrie, E.C.; Brodkin, K.; Peskind, E.R.; Wilkinson, C.W.; Raskind, M.A. Hypothalamic Pituitary Adrenocortical and Sympathetic Nervous System Responses to the Cold Pressor Test in Alzheimer’s Disease. Biol. Psychiatry 2000, 48, 247–254. [Google Scholar] [CrossRef]
- Elrod, R.; Peskind, E.R.; DiGiacomo, L.; Brodkin, K.I.; Veith, R.C.; Raskind, M.A. Effects of Alzheimer’s Disease Severity on Cerebrospinal Fluid Norepinephrine Concentration. Am. J. Psychiatry 1997, 154, 25–30. [Google Scholar] [CrossRef]
- Vitiello, B.; Veith, R.C.; Molchan, S.E.; Martinez, R.A.; Lawlor, B.A.; Radcliffe, J.; Hill, J.L.; Sunderland, T. Autonomic Dysfunction in Patients with Dementia of the Alzheimer Type. Biol. Psychiatry 1993, 34, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Raskind, M.A.; Peskind, E.R.; Halter, J.B.; Jimerson, D.C. Norepinephrine and MHPG Levels in CSF and Plasma in Alzheimer’s Disease. Arch. Gen. Psychiatry 1984, 41, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewska-Pniewska, B.; Gawel, M.; Szmidt-Salkowska, E.; Kepczynska, K.; Nojszewska, M. Clinical and Functional Assessment of Dysautonomia and Its Correlation in Alzheimer’s Disease. Am. J. Alzheimers Dis. Other Dement. 2012, 27, 592–599. [Google Scholar] [CrossRef]
- Wang, S.J.; Liao, K.K.; Fuh, J.L.; Lin, K.N.; Wu, Z.A.; Liu, C.Y.; Liu, H.C. Cardiovascular Autonomic Functions in Alzheimer’s Disease. Age Ageing 1994, 23, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Elmståhl, S.; Petersson, M.; Lilja, B.; Samuelsson, S.M.; Rosén, I.; Bjunö, L. Autonomic Cardiovascular Responses to Tilting in Patients with Alzheimer’s Disease and in Healthy Elderly Women. Age Ageing 1992, 21, 301–307. [Google Scholar] [CrossRef]
- Allan, L.; McKeith, I.; Ballard, C.; Kenny, R.A. The Prevalence of Autonomic Symptoms in Dementia and Their Association with Physical Activity, Activities of Daily Living and Quality of Life. Dement. Geriatr. Cogn. Disord. 2006, 22, 230–237. [Google Scholar] [CrossRef]
- Allan, L.M.; Ballard, C.G.; Rowan, E.N.; Kenny, R.A. Incidence and Prediction of Falls in Dementia: A Prospective Study in Older People. PLoS ONE 2009, 4, e5521. [Google Scholar] [CrossRef]
- Checklist_for_Analytical_Cross_Sectional_Studies.Pdf. Available online: https://jbi.global/sites/default/files/2020-08/Checklist_for_Analytical_Cross_Sectional_Studies.pdf (accessed on 3 March 2025).
- JBI Critical Appraisal Tools|JBI. Available online: https://jbi.global/critical-appraisal-tools (accessed on 22 February 2025).
- Idiaquez, J.; Roman, G.C. Autonomic Dysfunction in Neurodegenerative Dementias. J. Neurol. Sci. 2011, 305, 22–27. [Google Scholar] [CrossRef]
- da Silva, V.P.; Ramalho Oliveira, B.R.; Tavares Mello, R.G.; Moraes, H.; Deslandes, A.C.; Laks, J. Heart Rate Variability Indexes in Dementia: A Systematic Review with a Quantitative Analysis. Curr. Alzheimer Res. 2018, 15, 80–88. [Google Scholar] [CrossRef]
- Cheng, Y.-C.; Huang, Y.-C.; Huang, W.-L. Heart Rate Variability in Patients with Dementia or Neurocognitive Disorders: A Systematic Review and Meta-Analysis. Aust. N. Z. J. Psychiatry 2022, 56, 16–27. [Google Scholar] [CrossRef]
- Masters, M.C.; Morris, J.C.; Roe, C.M. “Noncognitive” Symptoms of Early Alzheimer Disease. Neurology 2015, 84, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Selles, M.C.; Oliveira, M.M.; Ferreira, S.T. Brain Inflammation Connects Cognitive and Non-Cognitive Symptoms in Alzheimer’s Disease. J. Alzheimers Dis. 2018, 64, S313–S327. [Google Scholar] [CrossRef] [PubMed]
- Forester, B.P.; Oxman, T.E. Measures to Assess the Noncognitive Symptoms of Dementia in the Primary Care Setting. Prim. Care Companion J. Clin. Psychiatry 2003, 5, 158–163. [Google Scholar] [PubMed]
- Wang, X.; Cheng, Z. Cross-Sectional Studies: Strengths, Weaknesses, and Recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical Diagnosis of Alzheimer’s Disease: Report of the NINCDS-ADRDA Work Group under the Auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef]
- Paradowski, B.; Bilińska, M.; Koszewicz, M.; Pokryszko, A. Ocena czynności układu sercowo-naczyniowego i potowydzielniczego u chorych na chorobe Alzheimera [Evaluation of cardiovascular and sudomotor functions in Alzheimer’s disease]. Pol Merkur Lek. 1999, 7, 180–184. (In Polish) [Google Scholar] [PubMed]
- Tulbă, D.; Cozma, L.; Popescu, B.O.; Davidescu, E.I. Dysautonomia in Alzheimer’s Disease. Medicina 2020, 56, 337. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Elia, A.; Fossati, S. Autonomic nervous system and cardiac neuro-signaling pathway modulation in cardiovascular disorders and Alzheimer’s disease. Front. Physiol. 2023, 14, 1060666. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kenny, R.A.; Kalaria, R.; Ballard, C. Neurocardiovascular instability in cognitive impairment and dementia. Ann. N. Y. Acad. Sci. 2002, 977, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, A.R.; Larrick, J.W. The Danger of Being Too Sympathetic: Norepinephrine in Alzheimer’s Disease and Graying of Hair. Rejuvenation Res. 2020, 23, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Royall, D.R.; Gao, J.H.; Kellogg, D.L., Jr. Insular Alzheimer’s disease pathology as a cause of “age-related” autonomic dysfunction and mortality in the non-demented elderly. Med. Hypotheses 2006, 67, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Nashiro, K.; Yoo, H.J.; Cho, C.; Kim, A.J.; Nasseri, P.; Min, J.; Dahl, M.J.; Mercer, N.; Choupan, J.; Choi, P.; et al. Heart rate and breathing effects on attention and memory (HeartBEAM): Study protocol for a randomized controlled trial in older adults. Trials 2024, 25, 190. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, C.R.; Yang, C.Y.; Sharma, D.; Chen, T.H.; Huang, X.Q.; Hung, T.M.; Kuo, T.B.J.; Jou, J.H. Associations between Sleep Duration and Autonomic Nervous System Regulation in Patients with Probable Alzheimer’s Disease: A Cross-Sectional Pilot Study. Clocks Sleep 2024, 6, 533–545. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gan, J.; Liu, S.; Wang, X.D.; Hu, W.; Lv, Y.; Niu, J.; Meng, X.; Chen, Y.; Shi, Z.; Ji, Y. The Association Between Hyperhidrosis and Dementia: A Community-Based Research. J. Alzheimers Dis. 2021, 84, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Ren, P.; Wang, X.; Anthony, M.; Tadin, D.; Heffner, K.L. Cortical thickness is associated with altered autonomic function in cognitively impaired and non-impaired older adults. J. Physiol. 2017, 595, 6969–6978. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fotiou, D.F.; Stergiou, V.; Tsiptsios, D.; Lithari, C.; Nakou, M.; Karlovasitou, A. Cholinergic deficiency in Alzheimer’s and Parkinson’s disease: Evaluation with pupillometry. Int. J. Psychophysiol. 2009, 73, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Mendez, M.F.; Kaiser, N.; Jimenez, E.; Mather, M.; Shapira, J.S. Skin conductance levels may reflect emotional blunting in behavioral variant frontotemporal dementia. J. Neuropsychiatry Clin. Neurosci. 2014, 26, 227–232. [Google Scholar] [CrossRef]
- Deutsch, C.K.; Patnaik, P.P.; Greco, F.A. Is There a Characteristic Autonomic Response During Outbursts of Combative Behavior in Dementia Patients? J. Alzheimers Dis. Rep. 2021, 5, 389–394. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mendez, M.F.; Fong, S.S.; Ashla, M.M.; Jimenez, E.E.; Carr, A.R. Skin Conduction Levels Differentiate Frontotemporal Dementia From Alzheimer’s Disease. J. Neuropsychiatry Clin. Neurosci. 2018, 30, 208–213. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| No | Study | Sample Size | AGE Mean (SD) | Sex (F%) | MMSE GDS, FAB CAMCOG | Clinical Dysautonomia | Test | Findings | Comments |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Haglund et al., 2024 [37] | 18 AD 18 DLB | 62.6 (6.2) 64.6 (9.3) | (61) (28.5) | 5% OH | HRV | DLB < AD | Unknown clinical significance | |
| 2 | Nair et al., 2023 [38] | 20 AD 20 HC | Age matched | gender matched | No information | HRV | AD < HC LF/HF AD > HC | Sympathetic/parasympathetic balance disorder | |
| 3 | Omoya et al., 2020 [39] | 29 AD 26 DLB 25 HC | 81.2 (6.4) 78.3 (8.1) 77.2 (5.4) | (65.5) (53.8) (68) | 18.7 (4.7) 17.4 (7.2) 28.8 (1.0) | No information | HRV | LF DLB < AD late HRR (Hmax − H180) AD < HC | AD exhibited differences from HC but not as large as in DLB |
| 4 | Kim et al., 2018 [40] | 32 AD 23 DLB 36 HC | 70.1 (6.3) 70.6 (5.2) 68.4 (6.4) | (56.3) | 24.7 (2.8) 25.0 (2.4) 26.6 (1.9) | No information | HRV | AD = HC | HRV negatively correlated with verbal memory HRV can discriminate DLB-AD at the MCI stage |
| 5 | Kasanuki et al., 2015 [41] | 30 AD 30 DLB 20 HC | 79.8 (5.6) 79.9 (4.7) 77.2 (4.8) | (50) (46.6) (50) | 20.5 (4.2) 18.0 (4.2) 30.0 (0.7) | Constipation, orthostatic dizziness, urinary incontinence, increased sweating | HRV | DLB < AD | HRV can differentiate DLB-AD |
| 6 | Toledo and Junqueira, 2010 [42] | 22 AD | 79.6 (1.4) | (90.9) | No information | HRV | HF-positive correlation, LF-negative correlation with cognitive performance | Severe cognitive deficiency →lower parasympathetic/higher cardiac sympathetic modulation. | |
| 7 | Allan et al., 2005 [43] | 14 AD 20 VAD 80 HC | 77.2 (6.2) 81.4 (5.0) 75.7 (5.7) | (71.4) (33.3) (50) | 18.4 (4.3) 18.6 (6.1) 28.5 (1.6) | No information | HRV | AD = VAD = HC | Insensitive to detect minor changes Sensitive for clinically significant dysautonomia |
| 8 | Zulli et al., 2005 [44] | 33 AD 39 MCI 29 HC | 72.1 (8.2) 70.0 (7.2) 69.8 (5.3) | (60.6) (58.9) (65.5) | 19.0 (4.3) 27.4 (1.8) 28.8 (1.3) | No information | HRV | AD < MCI/HC | Correlated with the degree of cognitive impairment |
| 9 | Giubilei et al., 1998 [45] | 12 AD 10 HC | 65.7 (6.2) | (58.3) | 18.4 (3.6) | No information | HRV | AD < HC | Treatment caused changes similar to those observed in controls |
| 10 | Aharon-Peretz et al., 1992 [46] | 20 AD 7 HC | 71.3 (8.2) 65 (2.4) | 18.35 (3.18) | No information | HRV | AD < HC LF/HF AD > HC | Hypersympathetic, hypoparasympathetic state. | |
| 11 | Allan et al., 2007 [29] | 39 AD 29 VAD 27 DLB 37 PDD 38 HC | 79 (6) 80 (6) 75 (7) 72 (5) 76 (7) | (56) (30) (43) (42) (53) | autonomic neuropathy 13% | HRV OH | →AD = HC →AD ≠ HC (prevalence) | Autonomic functions unimpaired except OH | |
| 12 | Franceschi et al., 1986 [47] | 16 AD 7 HC | 62.2 (4.1) 59.6 (2.5) | (50) (42.8) | No information | HRV body movement related | Rmb AD < HC Rs/w AD = HC | Sympathetic cardiac dysfunction during sleep Unknown clinical importance | |
| 13 | Freidenberg et al., 2013 [48] | 188 | 80.8 (7.7) | OH | 40% OH (prevalence) | Mental and motor fluctuations related to OH not traditional signs | |||
| 14 | van Beek et al., 2010 [49] | 21 AD 20 HC | NO INF | No information | OH | AD > HC | Enhanced sympathetic tone Increased orthostatic tolerance | ||
| 15 | Siennicki-Lantz et al., 1999 [30] | 12 AD 15 HC | 82.6 (3.8) 81.8 (3.5) | (100) (100) | No information | OH | AD = HC 33% OH | AD with OH had significantly lower CBF frontal/parieto-frontal regions, compared with AD without OH | |
| 16 | Idiaquez et al., 1997 [50] | 10 AD 23 HC | 73.9 (6.4) 71.5 (6.4) | (70) (47.8) | 14.5 (5.85) 27.2 (1.6) | No associated symptoms | PPH | AD > HC | Sympathetic dysfunction— BP instability of central origin |
| 17 | Meel-van den Abeelen et al., 2012 [32] | 18 AD 11 MCI 19 HC | 72 (6) 74 (9) 75 (3) | (61.1) (54.5) (26.3) | 22 (5) 25 (3) 29(5) | No information | BR | AD < HC | Not known significance |
| 18 | Szili-Török et al., 2001 [51] | 24 AD 23 PD 22 HC | 72.3 (7.2) 65 (9.3) 70 (6.6) | (60.8) (54.2) (68.2) | 19 (6.5) 27.5 (2) 29 (0.9) | No information | BR | AD/PD < HC | Unclear significance in neurological disorders |
| 19 | Pascualy et al., 2000 [52] | 9 AD 9 HC | 76 (2) 76 (1) | (55.5) (55.5) | 17 (1) 29 (1) | No information | Basal NE (CPT) responses to 1-min | Basal NE AD > HC NE (CPT) AD = HC | increased HPA axis responsiveness to CPT |
| 20 | Elrod et al., 1997 [53] | 74 AD 42 HC 54 HC | 69 (6) 68 (7) 26 (3) | (24.3) (38) (0) | 18 (4) | No information | NE in CSF | Advanced AD > moderate AD/HC | Contribute to cognitive deficits and agitated behaviors |
| 21 | Vitiello et al., 1993 [54] | 60 AD 20 HC | 65.5 (8) 64.7 (9.4) | (53.3) (50) | 4.6 (1.0) 0 | No information | NE OH | →AD = HC →AD < HC (systolic BP) | More evident in depressed AD |
| 22 | Raskind et al., 1984 [55] | 9 AD 7AD 6 HC | 68 (8) 61 (6) 67 (10) | (0) (0) (0) | Advanced moderate | No information | NE in plasma/CSF | Advanced AD > moderate AD/HC | Contribute to agitation, sleep disturbance |
| 23 | Toru et al., 2018 [35] | 59 AD 56 DLB 37 PDD | 77.6 (6.9) 77.6 (6.5) 77.6 (6.6) | (62.7) (55) (59.4) | 19.2 (5.7) 19.0 (9.3) 19.1 (7.2) | 18.6% 100% 100% | SSR HUTiltTest NE 123I-MIBG | →AD ≠ DLB PDD →AD ≠ DLB PDD →AD > DLB/PDD →AD > DLB/PDD | SSR was the best marker of autonomic dysfunction for distinguishing DLB/PDD from AD |
| 24 | Negami et al., 2013 [34] | 20 AD 20 DLB | 78.5 (5.0) 78.7 (6.9) | (50) (50) | 19.3 (3.6) 19.2 (4.8) | No information | SSRamp HRV 123I-MIBG | →DLB < AD →DLB < AD →DLB < AD | SSR showed the most significant difference |
| 25 | Zakrzewska-Pniewska et al., 2012 [56] | 54 AD 37 HC | 73.1 (6.3) 47.3 (16.4) | (57.4) (56.7) | Mild in 66% | SSR RRIV | →AD = HC →AD < HC | Subclinical dysautonomia associated with cardiovascular dysfunction | |
| 26 | Wang et al., 1994 [57] | 23 AD 23 HC | 70.7 (6.7) 70.8 (6.9) | (56.5) (39.1) | 10.0 (6.9) | No information | SSR RRIV OH | →AD = HC →AD < HC →AD = HC | Mildly impaired vagal parasympathetic functions. |
| 27 | Mellingsæter et al., 2015 [27] | 14 AD 48 HC | 73.6 (5.7) 72 (6) | (50) (50) | 24.8 (2.4) | No information | TILT | AD ≠ HC | Poorer sympathetic response to orthostatic stress |
| 28 | Elmståhl et al., 1992 [58] | 24 AD 54 HC | 85 (5.3) | (100) | No information | TILT TEST DEEP BREATHING | →AD ≠ HC →AD = HC | Imbalance of ANS Degeneration of cholinergic nuclei of Meynert | |
| 29 | Allan et al., 2006 [59] | 40 AD 46 PDD 32 DLB 38 VAD 42 HC | 78 (5.6) 72 (5.7) 75 (7.1) 79 (5.9) 76 (6.7) | (55) (39) (41) (29) (48) | 59 (14.5) 64 (16.3) 60 (15.0 62 (18.3) 94 (4.7) | Mucosal dryness urinary symptoms, constipation, postural dizziness | Autonomic symptom scale | AD = HC DLB PDD ≠ AD/HC | No clinically significant dysautonomia in AD |
| 30 | Allan et al., 2009 [60] | 38 AD 40 PDD 30 DLB 32 VAD 39 HC | 79 (5.8) 72 (6.0) 76 (7.1) 79 (6.2) 75 (6.4) | (52.6) (35) (40) (27.1) (46.2) | 59 (15) 64 (16) 59 (15) 64 (18) 94 (4.7) | Symptomatic orthostatic hypotension dizziness, lightheadedness, unsteadiness or presyncope Ewing’s battery | Ewing’s battery Falls incidence | AD/VAD = HC | Higher incidence of falls in all dementia types than HC. PDD/DLB at higher risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadopoulou, M.; Stefanou, M.-I.; Bakola, E.; Moschovos, C.; Athanasaki, A.; Tsigkaropoulou, E.; Michopoulos, I.; Paraskevas, G.P.; Gournellis, R.; Tsivgoulis, G. Dysautonomia in Alzheimer’s Disease: A Systematic Review. Brain Sci. 2025, 15, 502. https://doi.org/10.3390/brainsci15050502
Papadopoulou M, Stefanou M-I, Bakola E, Moschovos C, Athanasaki A, Tsigkaropoulou E, Michopoulos I, Paraskevas GP, Gournellis R, Tsivgoulis G. Dysautonomia in Alzheimer’s Disease: A Systematic Review. Brain Sciences. 2025; 15(5):502. https://doi.org/10.3390/brainsci15050502
Chicago/Turabian StylePapadopoulou, Marianna, Maria-Ioanna Stefanou, Eleni Bakola, Christos Moschovos, Athanasia Athanasaki, Evdoxia Tsigkaropoulou, Ioannis Michopoulos, George P. Paraskevas, Rossetos Gournellis, and Georgios Tsivgoulis. 2025. "Dysautonomia in Alzheimer’s Disease: A Systematic Review" Brain Sciences 15, no. 5: 502. https://doi.org/10.3390/brainsci15050502
APA StylePapadopoulou, M., Stefanou, M.-I., Bakola, E., Moschovos, C., Athanasaki, A., Tsigkaropoulou, E., Michopoulos, I., Paraskevas, G. P., Gournellis, R., & Tsivgoulis, G. (2025). Dysautonomia in Alzheimer’s Disease: A Systematic Review. Brain Sciences, 15(5), 502. https://doi.org/10.3390/brainsci15050502