
Differential Impact of Risk Factors for Cognitive Decline in Heterosexual and Sexual Minority Older Adults in England



Abstract
1. Introduction
- Two measures of SCD for memory and for global cognition (Aim 1);
- Two objective measures of cognitive decline in episodic and semantic memory (Aim 2).
2. Materials and Methods
2.1. Participant Sample
2.2. Sexual Orientation
2.3. Psycho-Social Risk Factors for Cognitive Decline
- Depressive symptoms were quantified by means of the Center for Epidemiologic Studies Depression Scale (CES-D) [32]. The CES-D includes 8 items to self-assess mood-related complaints in the previous week. Items were scored dichotomously (yes = 1; no = 0). The sum of all self-reported complaints resulted in a total score between 0 and 8 [33].
- Loneliness was self-assessed by means of the UCLA 3-Item Loneliness Scale [34]. This scale comprises three questions: “How often do you feel lack of companionship?”, “How often do you feel left out?” and “How often do you feel isolated from others?” Possible answers are (A) hardly ever, (B) some of the time and (C) often, corresponding to scores from 1 to 3, leading to a total loneliness score between 3 and 9.
- Participants’ marital status was coded as a binary variable to distinguish participants in a relationship from those who were not. At Wave 8, legal marital status was assessed by providing a series of response options: (A) single, that is, never married and never registered in a same-sex civil partnership; (B) married, first and only marriage or a civil partner in a registered same-sex civil partnership; (C) remarried, second or later marriage; (D) separated, but still legally married or (spontaneous only) in a same-sex civil partnership; (E) divorced or (spontaneous only) formerly in a same-sex civil partnership; (F) widowed or (spontaneous only) a surviving civil partner from a same-sex civil partnership. Due to small sample sizes across the sub-categories, marital status was operationalized as a binary variable to distinguish the participants currently in a relationship (Options B and C) from those not in a relationship for any reason (Options A, D, E and F).
- Socio-economic status (SES) was operationalised as quintiles of the total net non-pension wealth at the benefit unit level, in line with previous research [35]. Total net non-pension wealth has been extensively used as an index of SES because it captures current socio-economic circumstances and the wealth accumulated over the life course by older adults, associated with health outcomes [36,37].
2.4. Cognitive Outcome Measures
2.4.1. Subjective Cognitive Decline
2.4.2. Objectively Assessed Cognitive Decline
- A four-point measure (total score 0–4) assessing orientation to time (respondents were asked to provide (1) the day of the month, (2) the month, (3) the year and (4) the day of the week) [46].
- The word-list learning test [47] was used to assess how many words out of a list of 10 were recalled by participants both immediately after the reading (immediate recall, score 0–10) and after a delay of 5 min, during which the participants were asked other survey questions (delayed recall, score 0–10).
- The two measures assessing semantic memory were the following:
- Semantic fluency—animals [48] was used to assess the fluency of retrieval from the stored conceptual knowledge of a specific category of items. In particular, the participants were asked to report as many animals as they could in 60 s.
- Object and people naming was used to assess the participants’ conceptual knowledge by asking them to provide an answer to 5 definitions of either objects or people (score 0–5). This measure was adapted by combining and integrating items included in the telephone interview for cognitive status [49].
2.5. Statistical Analysis
3. Results
3.1. Between-Group Comparison of Socio-Demographic Characteristics and Risk Factors
3.2. Impact of Risk Factors on SCD in SMOAs and HOAs (Aim 1)
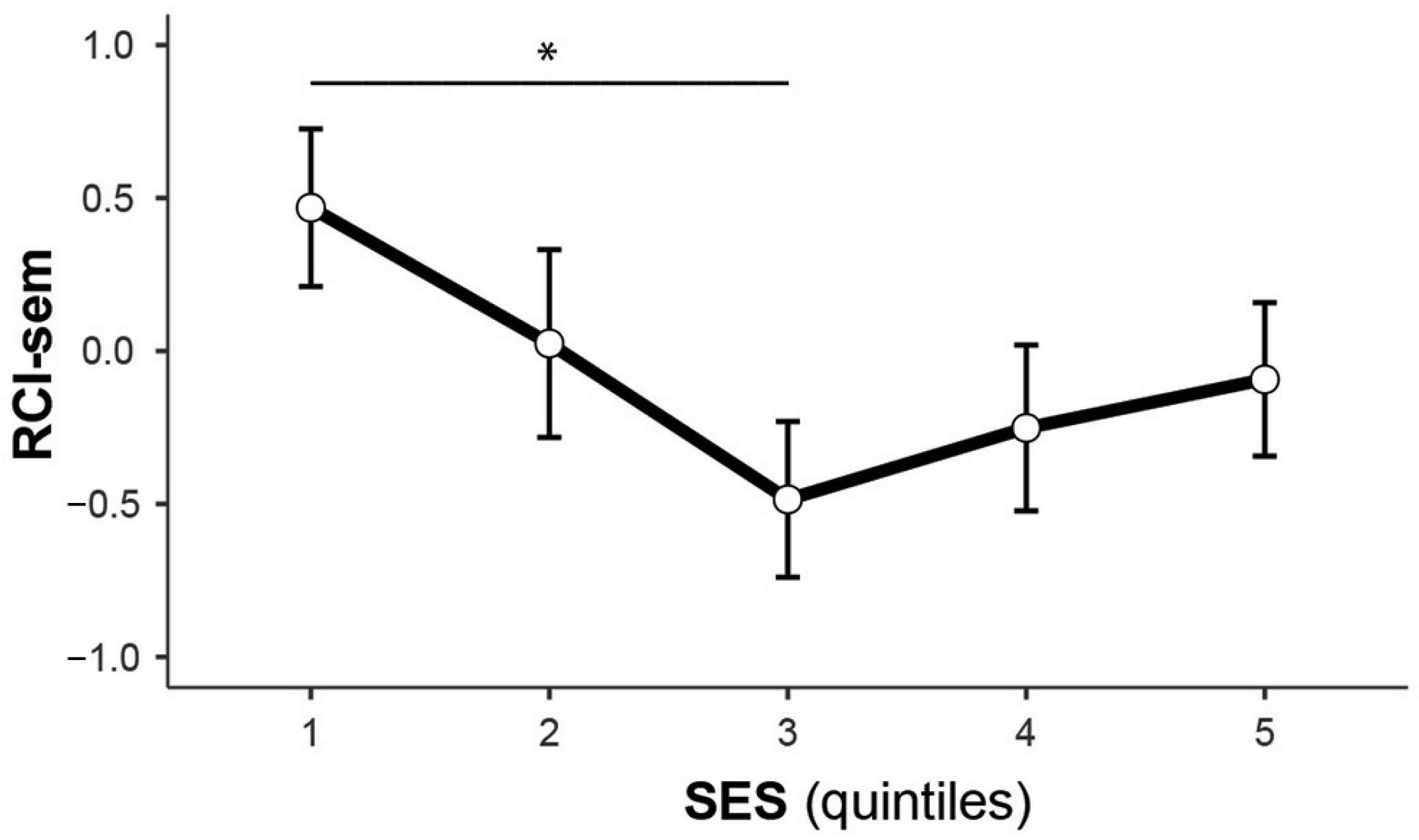
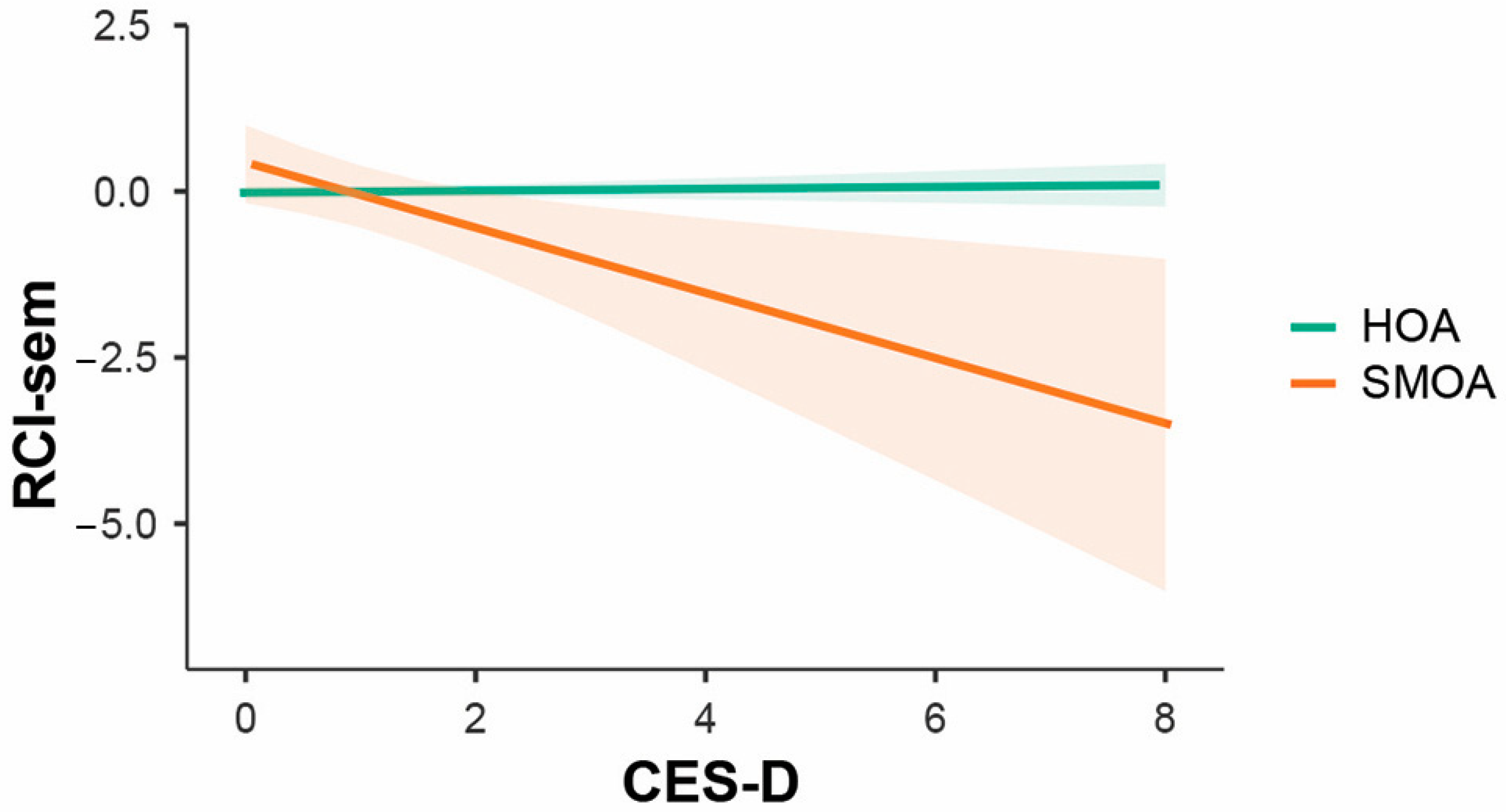
3.3. Impact of Risk Factors on Objective Cognitive Changes in SMOAs and HOAs (Aim 2)
3.4. Sensitivity Analysis in Matched Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Variable | HOA (n = 92) | SMOA (n = 92) | Test | p |
|---|---|---|---|---|
| Age (years) | 67.5 (8.2) | 67.5 (8.3) | 0.02 | 1.000 |
| Sex (M/F) a | 54.3/45.7 | 54.3/45.7 | 0.00 b | 1.000 |
| Education a | ||||
| No qualifications | 12.0 | 12.0 | 0.00 b | 1.000 |
| Level 1 | 12.0 | 12.0 | ||
| Level 2 | 22.8 | 22.8 | ||
| Level 3 | 16.3 | 16.3 | ||
| Level 4 | 12.0 | 12.0 | ||
| Level 5 | 1.1 | 1.1 | ||
| Level 6 | 23.9 | 23.9 | ||
| CES-D c | 0.0 (1) | 1.0 (1) | −0.80 d | 0.422 |
| Loneliness c | 3.0 (1) | 3.0 (3) | −2.05 d | 0.040 |
| Marital status (R/NR) a | 83.7/16.3 | 46.7/53.3 | 27.70 b | <0.001 |
| SES a | 4.44 b | 0.349 | ||
| Quintile 1 | 13.2 | 24.7 | ||
| Quintile 2 | 17.6 | 14.6 | ||
| Quintile 3 | 28.6 | 21.3 | ||
| Quintile 4 | 18.7 | 16.9 | ||
| Quintile 5 | 22.0 | 22.5 |
| SCD-mem | SCD-cog | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p | OR (95% CI) | p |
| SO (SMOA) | 5.48 (0.62, 53.74) | 0.132 | 1.71 (0.00, 9.73 × 1043) | 0.999 |
| Risk factors | ||||
| CES-D | 1.48 (1.13, 2.01) | 0.007 | 1.35 (0.98, 1.91) | 0.072 |
| Loneliness | 1.03 (0.79, 1.34) | 0.837 | 0.93 (0.58, 1.37) | 0.742 |
| Marital status (R) | 0.74 (0.32, 1.76) | 0.484 | 0.97 (0.31, 3.31) | 0.956 |
| SES (ref: Q1) | ||||
| Quintile 2 | 2.95 (0.85, 11.33) | 0.096 | 2.08 (0.45, 13.07) | 0.373 |
| Quintile 3 | 2.88 (0.93, 10.06) | 0.077 | 0.79 (0.12, 5.51) | 0.799 |
| Quintile 4 | 0.81 (0.20, 3.21) | 0.766 | 0.00 (0.00, 2.90 × 1015) | 0.991 |
| Quintile 5 | 2.46 (0.78, 8.73) | 0.140 | 1.41 (0.27, 9.30) | 0.690 |
| Interaction effects | ||||
| CES-D × SO | 1.09 (0.61, 1.93) | 0.778 | 0.99 (0.51, 1.95) | 0.966 |
| Loneliness × SO | 0.69 (0.40, 1.55) | 0.164 | 1.77 (0.81, 4.49) | 0.180 |
| Marital status × SO | 0.31 (0.05, 1.64) | 0.177 | 2.78 (0.24, 27.77) | 0.387 |
| SES × SO | ||||
| (Q2−Q1) × SO | 0.55 (0.04, 6.69) | 0.647 | 0.57 (0.01, 12.29) | 0.732 |
| (Q3−Q1) × SO | 1.06 (0.09, 10.66) | 0.961 | 0.20 (0.00, 5.74) | 0.382 |
| (Q4−Q1) × SO | 3.31 (0.21, 54.17) | 0.387 | 1.06 × 107 (0.00, 1.41 × 10196) | 0.992 |
| (Q5−Q1) × SO | 0.74 (0.06, 7.66) | 0.808 | 0.67 (0.06, 66.49) | 0.815 |
| RCI-epi | RCI-sem | |||
|---|---|---|---|---|
| Variable | β (95% CI) | p | β (95% CI) | p |
| SO (SMOA) | 0.90 (−0.40, 2.21) | 0.178 | −1.29 (−3.24, 0.70) | 0.199 |
| Risk factors | ||||
| CES-D | 0.00 (−0.16, 0.17) | 0.964 | −0.40 (−0.65, −0.16) | 0.002 |
| Loneliness | 0.04 (−0.12, 0.20) | 0.616 | 0.26 (0.03,0.50) | 0.030 |
| Marital status (R) | 0.23 (−0.28, 0.74) | 0.373 | −0.26 (−1.02, 0.50) | 0.504 |
| SES (ref: Q1) | ||||
| Quintile 2 | 0.29 (−0.45, 1.02) | 0.448 | −0.01 (−1.11, 1.10) | 0.994 |
| Quintile 3 | 0.40 (−0.27, 1.07) | 0.244 | −0.98 (−1.98, 0.03) | 0.058 |
| Quintile 4 | 0.32 (−0.39, 1.03) | 0.373 | −0.47 (−1.53, 0.59) | 0.383 |
| Quintile 5 | −0.02 (−0.71, 0.66) | 0.949 | −0.04 (−1.07, 0.99) | 0.941 |
| Interaction effects | ||||
| CES-D × SO | 0.11 (−0.21, 0.44) | 0.497 | −0.12 (−0.61, 0.37) | 0.637 |
| Loneliness × SO | 0.25 (−0.56, 0.07) | 0.123 | 0.27 (−0.20, 0.74) | 0.266 |
| Marital status × SO | −0.35 (−1.37, 0.67) | 0.500 | 0.02 (−1.50, 1.53) | 0.983 |
| SES × SO | ||||
| (Q2−Q1) × SO | −0.50 (−1.98, 0.97) | 0.506 | −1.93 (−4.13, 0.27) | 0.088 |
| (Q3−Q1) × SO | −0.36 (−1.71, 0.98) | 0.596 | −1.65 (−3.66, 0.36) | 0.109 |
| (Q4−Q1) × SO | −0.22 (−1.64, 1.20) | 0.760 | −1.59 (−3.71, 0.53) | 0.143 |
| (Q5−Q1) × SO | −1.54 (−2.91, −0.16) | 0.030 | −2.16 (−4.22, −0.11) | 0.041 |
References
- Adkins-Jackson, P.B.; George, K.M.; Besser, L.M.; Hyun, J.; Lamar, M.; Hill-Jarrett, T.G.; Bubu, O.M.; Flatt, J.D.; Heyn, P.C.; Cicero, E.C.; et al. The structural and social determinants of Alzheimer’s disease related dementias. Alzheimers Dement. 2023, 19, 3171–3185. [Google Scholar] [CrossRef] [PubMed]
- Rosendale, N.; Wong, J.O.; Flatt, J.D.; Whitaker, E. Sexual and gender minority health in neurology: A scoping review. JAMA Neurol. 2021, 78, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Manca, R.; Moreno, A.; Nicoletti, A.; Henderson, N.J.; Flatt, J.D. Neurocognitive health in LGBTQIA+ older adults: Current state of research and recommendations. Front. Hum. Neurosci. 2024, 18, 1394374. [Google Scholar] [CrossRef]
- Flatt, J.D.; Cicero, E.C. Advancing equity in Alzheimer’s disease and mental health research for LGBTQIA+ older adults. Nat. Ment. Health 2023, 1, 385–387. [Google Scholar] [CrossRef]
- Brown, M.J.; Patterson, R. Subjective cognitive decline among sexual and gender minorities: Results from a U.S. population-based sample. J. Alzheimers Dis. 2020, 73, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Hopper, S.; Hammond, N.G.; Taler, V.; Stinchcombe, A. Biopsychosocial correlates of subjective cognitive decline and related worry in the Canadian Longitudinal Study on Aging. Gerontology 2023, 69, 84–97. [Google Scholar] [CrossRef]
- Nelson, C.L.; Andel, R. Does sexual orientation relate to health and well-being? Analysis of adults 50+ years of age. Gerontologist 2020, 60, 1282–1290. [Google Scholar] [CrossRef]
- Flatt, J.D.; Cicero, E.C.; Lambrou, N.H.; Wharton, W.; Anderson, J.G.; Bouldin, E.D.; McGuire, L.C.; Taylor, C.A. Subjective cognitive decline higher among sexual and gender minorities in the United States, 2015–2018. Alzheimers Dement. 2021, 7, e12197. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen-Goldsen, K.I.; Jung, H.; Kim, H.; Petros, R.; Emlet, C. Disparities in subjective cognitive impairment by sexual orientation and gender in a national population based study of U.S. adults, 2013–2018. J. Aging Health 2022, 34, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Seelman, K.L. Differences in mental, cognitive, and functional health by sexual orientation among older women: Analysis of the 2015 Behavioral Risk Factor Surveillance System. Gerontologist 2019, 59, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Flatt, J.D.; Johnson, J.K.; Karpiak, S.E.; Seidel, L.; Larson, B.; Brennan-Ing, M. Correlates of subjective cognitive decline in lesbian, gay, bisexual, and transgender older adults. J. Alzheimers Dis. 2018, 64, 91–102. [Google Scholar] [CrossRef]
- Brown, M.J.; Amoatika, D.; Addo, P.N.O.; Kaur, A.; Haider, M.R.; Merrell, M.A.; Crouch, E. Childhood sexual trauma and subjective cognitive decline: An assessment of racial/ethnic and sexual orientation disparities. J. Appl. Gerontol. 2023, 42, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Barbee, H.; McKay, T. Do supportive work environments matter for minority aging? Work stress and subjective cognitive impairment among middle-age and older lesbian, gay, bisexual, transgender, and queer adults. Acta Psychol. 2023, 237, 103949. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen-Goldsen, K.; Petros, R.; Jung, H.H.; Kim, H. Sexual minority disparities in subjective cognitive impairment: Do they persist after accounting for psychological distress? J. Aging Health 2023, 35, 727–735. [Google Scholar] [CrossRef]
- Manca, R.; Venneri, A. A comparison of neurocognitive decline in older adults in same-sex and opposite-sex relationships. Curr. Alzheimer Res. 2020, 17, 1102–1114. [Google Scholar] [CrossRef]
- Manca, R.; Venneri, A. Minority stress and psychosocial influences on cognitive performance in sexual minority older adults. Innov. Aging 2023, 7, igad110. [Google Scholar] [CrossRef]
- Manca, R.; Correro, A.N.; Gauthreaux, K.; Flatt, J.D. Divergent patterns of cognitive deficits and structural brain alterations between older adults in mixed-sex and same-sex relationships. Front. Hum. Neurosci. 2022, 16, 909868. [Google Scholar] [CrossRef] [PubMed]
- Stinchcombe, A.; Hammond, N.G. Social determinants of memory change: A three-year follow-up of the Canadian Longitudinal Study on Aging (CLSA). Arch. Gerontol. Geriatr. 2023, 104, 104830. [Google Scholar] [CrossRef]
- Perales-Puchalt, J.; Gauthreaux, K.; Flatt, J.; Teylan, M.A.; Resendez, J.; Kukull, W.A.; Chan, K.C.; Burns, J.; Vidoni, E.D. Risk of dementia and mild cognitive impairment among older adults in same-sex relationships. Int. J. Geriatr. Psychiatry 2019, 34, 828–835. [Google Scholar] [CrossRef]
- Correro, A.N.; Gauthreaux, K.; Perales-Puchalt, J.; Chen, Y.; Chan, K.C.G.; Kukull, W.A.; Flatt, J.D. Cognitive aging with dementia, mild cognitive impairment, or no impairment: A comparison of same- and mixed-sex couples. J. Alzheimers Dis. 2023, 92, 109–128. [Google Scholar] [CrossRef]
- Hanes, D.W.; Clouston, S.A.P. Cognitive aging in same- and different-sex relationships: Comparing age of diagnosis and rate of cognitive decline in the Health and Retirement Study. Gerontology 2023, 69, 356–369. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.L.; MacCarthy, S.; Meads, C.; Massou, E.; Mant, J.; Saunders, A.M.; Elliott, M.N. Long-term conditions among sexual minority adults in England: Evidence from a cross-sectional analysis of responses to the English GP Patient Survey. BJGP Open 2021, 5, BJGPO.2021.0067. [Google Scholar] [CrossRef]
- Huo, S.; Rivier, C.A.; Clocchiatti-Tuozzo, S.; Renedo, D.; Sunmonu, N.A.; de Havenon, A.; Sarpong, D.F.; Rosendale, N.; Sheth, K.N.; Falcone, G.J. Brain Health Outcomes in Sexual and Gender Minority Groups: Results from the All of Us Research Program. Neurology 2024, 103, e209863. [Google Scholar] [CrossRef]
- Hsieh, N.; Liu, H.; Lai, W. Elevated risk of cognitive impairment among older sexual minorities: Do health conditions, health behaviors, and social connections matter? Gerontologist 2021, 61, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Hsieh, N.; Zhang, Z.; Zhang, Y.; Langa, K.M. Same-sex couples and cognitive impairment: Evidence from the Health and Retirement Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 1388–1399. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Correro, A.N.; Nielson, K.A. A review of minority stress as a risk factor for cognitive decline in lesbian, gay, bisexual, and transgender (LGBT) elders. J. Gay Lesbian Ment. Health 2020, 24, 2–19. [Google Scholar] [CrossRef] [PubMed]
- Rowan, G.A.; Frimpong, E.Y.; Li, M.; Chaudhry, S.; Radigan, M. Health disparities between older lesbian, gay, and bisexual adults and heterosexual adults in the public mental health system. Psychiatry Serv. 2022, 73, 39–45. [Google Scholar] [CrossRef]
- Fredriksen-Goldsen, K.I.; Kim, H.; Shui, C.; Bryan, A.E.B. Chronic health conditions and key health indicators among lesbian, gay, and bisexual older US adults, 2013–2014. Am. J. Public Health 2017, 107, 1332–1338. [Google Scholar] [CrossRef]
- Banks, J.; Batty, G.D.; Breedvelt, J.; Coughlin, K.; Crawford, R.; Marmot, M.; Nazroo, J.; Oldfield, Z.; Steel, N.; Steptoe, A.; et al. English Longitudinal Study of Ageing: Waves 0–9, 1998–2019, 37th ed.; Data Collection; UK Data Service: Colchester, UK, 2021; SN: 5050. [Google Scholar] [CrossRef]
- NatCen Social Research. English Longitudinal Study of Ageing: Wave 8, 2016–2017, Sexual Self-Completion Data: Special Licence Access, 2nd ed.; Data Collection; UK Data Service: Colchester, UK, 2021; SN: 8376. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- White, J.; Zaninotto, P.; Walters, K.; Kivimäki, M.; Demakakos, P.; Biddulph, J.; Kumari, M.; De Oliveira, C.; Gallacher, J.; Batty, G.D. Duration of depressive symptoms and mortality risk: The English Longitudinal Study of Ageing (ELSA). Br. J. Psychiatry 2016, 208, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A Short Scale for Measuring Loneliness in Large Surveys: Results From Two Population-Based Studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Malkowski, O.S.; Kanabar, R.; Western, M.J. Socio-economic status and trajectories of a novel multidimensional metric of Active and Healthy Ageing: The English Longitudinal Study of Ageing. Sci. Rep. 2023, 13, 6107. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.E.; Spiers, G.F.; Sinclair, D.R.; Kingston, A.; Hanratty, B. Characteristics of older unpaid carers in England: A study of social patterning from the English Longitudinal Study of Ageing. Age Ageing 2024, 53, afae049. [Google Scholar] [CrossRef]
- Demakakos, P.; Biddulph, J.P.; Bobak, M.; Marmot, M.G. Wealth and mortality at older ages: A prospective cohort study. J. Epidemiol. Community Health 2016, 70, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Liu, K.Y.; Costafreda, S.G.; Selbæk, G.; Alladi, S.; Ames, D.; Banerjee, S.; Burns, A.; Brayne, C.; et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet 2024, 404, 572–628. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Meyer, I.H. A Population Study of Health Status Among Sexual Minority Older Adults in Select U.S. Geographic Regions. Health Educ. Behav. 2019, 46, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Gorczynski, P.; Fasoli, F. Loneliness in sexual minority and heterosexual individuals: A comparative meta-analysis. J. Gay Lesbian Ment. Health 2022, 26, 112–129. [Google Scholar] [CrossRef]
- Gorman, B.K.; Oyarvide, Z. Sexual Orientation, Socioeconomic Status, and Healthy Aging. Generations 2018, 42, 56–60. [Google Scholar]
- Waite, S.; Denier, N. Gay Pay for Straight Work: Mechanisms Generating Disadvantage. Gend. Soc. 2015, 29, 561–588. [Google Scholar] [CrossRef]
- Park, D.C.; Lautenschlager, G.; Hedden, T.; Davidson, N.S.; Smith, A.D.; Smith, P.K. Models of visuospatial and verbal memory across the adult life span. Psychol. Aging 2002, 17, 299–320. [Google Scholar] [CrossRef] [PubMed]
- Marra, C.; Piccininni, C.; Masone Iacobucci, G.; Caprara, A.; Gainotti, G.; Costantini, E.M.; Callea, A.; Venneri, A.; Quaranta, D. Semantic Memory as an Early Cognitive Marker of Alzheimer’s Disease: Role of Category and Phonological Verbal Fluency Tasks. J. Alzheimers Dis. 2021, 81, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Wright, L.M.; De Marco, M.; Venneri, A. Verbal fluency discrepancies as a marker of the prehippocampal stages of Alzheimer’s disease. Neuropsychology 2023, 37, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.O.; Neal, S.R.; Peryer, G.; Sheehan, K.J.; Tan, M.P.; Myint, P.K. Orientation and verbal fluency in the English Longitudinal Study of Ageing: Modifiable risk factors for falls? Int. Psychogeriatr. 2019, 31, 1491–1498. [Google Scholar] [CrossRef]
- Ofstedal, M.B.; Fisher, G.G.; Herzhog, A.R. Documentation of Cognitive Functioning Measures in the Health and Retirement Study. 2005. Available online: https://hrsonline.isr.umich.edu/sitedocs/userg/dr-006.pdf (accessed on 30 January 2023).
- Woodcock, R.W.; McGrew, K.S.; Mather, N. Woodcock-Johnson III Tests of Achievement; Riverside: Rolling Meadows, IL, USA, 2007. [Google Scholar]
- Brandt, J.; Spencer, M.; Folstein, M. The Telephone Interview for Cognitive Status. Neuropsychiatry Neuropsychol. Behav. Neurol. 1988, 1, 111–117. [Google Scholar]
- Duff, K. Evidence-based indicators of neuropsychological change in the individual patient: Relevant concepts and methods. Arch. Clin. Neuropsychol. 2012, 27, 248–261. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.; Hu, H.; Ou, Y.; Bi, Y.; Ma, Y.; Tan, L.; Yu, J. Risk factors for subjective cognitive decline: The CABLE study. Transl. Psychiatry 2021, 11, 576. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, G.O.; Manning, L.; Kirn, D.; Klein, H.; Hampton, O.; Burke, O.; Buckley, R.; Rentz, D.; Sperling, R.; Marshall, G.A.; et al. Subjective Cognitive Decline in a Registry Sample: Relation to Psychiatric History, Loneliness, and Personality. J. Prev. Alzheimers Dis. 2022, 9, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Zullo, L.; Clark, C.; Gholam, M.; Castelao, E.; von Gunten, A.; Preisig, M.; Popp, J. Factors associated with subjective cognitive decline in dementia-free older adults-A population-based study. Int. J. Geriatr. Psychiatry 2021, 36, 1188–1196. [Google Scholar] [CrossRef]
- Kneale, D.; Henley, J.; Thomas, J.; French, R. Inequalities in older LGBT people’s health and care needs in the United Kingdom: A systematic scoping review. Ageing Soc. 2021, 41, 493–515. [Google Scholar] [CrossRef] [PubMed]
- Lara, E.; Caballero, F.F.; Rico-Uribe, L.A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef] [PubMed]
- Luchetti, M.; Terracciano, A.; Aschwanden, D.; Lee, J.H.; Stephan, Y.; Sutin, A.R. Loneliness is associated with risk of cognitive impairment in the Survey of Health, Ageing and Retirement in Europe. Int. J. Geriatr. Psychiatry 2020, 35, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Simons, R.L.; Ong, M.L.; Beach, S.R.H.; Lei, M.; Philibert, R.; Mielke, M.M. Direct and Indirect Effects of Socioeconomic Status and Discrimination on Subjective Cognitive Decline: A Longitudinal Study of African American Women. J. Gerontol. B Psychol. Sci. Soc. Sci. 2023, 78, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Zaninotto, P. Lower socioeconomic status and the acceleration of aging: An outcome-wide analysis. Proc. Natl. Acad. Sci. USA 2020, 117, 14911–14917. [Google Scholar] [CrossRef]
- Cadar, D.; Lassale, C.; Davies, H.; Llewellyn, D.J.; Batty, G.D.; Steptoe, A. Individual and Area-Based Socioeconomic Factors Associated With Dementia Incidence in England: Evidence From a 12-Year Follow-up in the English Longitudinal Study of Ageing. JAMA Psychiatry 2018, 75, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Hu, H.; Ou, Y.; Wang, Z.; Ma, Y.; Tan, L.; Yu, J. Socioeconomic Status and Risks of Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of 39 Prospective Studies. J. Prev. Alzheimers Dis. 2023, 10, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Craig, S.L.; Anderson, J.A.E.; Ross, L.E.; Muntaner, C. Sexual orientation and cognition in aging populations: Results from the Canadian Longitudinal Study on Aging. Acta Psychol. 2024, 242, 104117. [Google Scholar] [CrossRef]
- Bécares, L. Health and socio-economic inequalities by sexual orientation among older women in the United Kingdom: Findings from the UK Household Longitudinal Study. Ageing Soc. 2021, 41, 2416–2434. [Google Scholar] [CrossRef]
- Wu, Z.; Woods, R.L.; Wolfe, R.; Storey, E.; Chong, T.T.J.; Shah, R.C.; Orchard, S.G.; McNeil, J.J.; Murray, A.M.; Ryan, J. Trajectories of cognitive function in community-dwelling older adults: A longitudinal study of population heterogeneity. Alzheimers Dement. 2021, 13, e12180. [Google Scholar] [CrossRef] [PubMed]
- Correro, A.N.; Hinrichs, K.L.M.; Krishnan, M.C.; Cottingham, M.E.; Trittschuh, E.H.; Parmenter, B.A.; Kang, J.; Stelmokas, J. Neuropsychological assessment with lesbian, gay, bisexual, transgender, and queer/questioning (LGBTQ+) individuals: Practice, education, and training survey. Clin. Neuropsychol. 2022, 1–43. [Google Scholar] [CrossRef] [PubMed]
- Romanelli, R.J.; Rosenblatt, A.S.; Marcum, Z.A.; Flatt, J.D. Cognitive impairment in sexual and gender minority groups: A scoping review of the literature. LGBT Health 2023, 11, 178–192. [Google Scholar] [CrossRef] [PubMed]

| Variable | HOA (n = 4180) | SMOA (n = 92) | Test | p |
|---|---|---|---|---|
| Age (years) a | 67.0 (11) | 68.0 (12) | 0.33 b | 0.739 |
| Sex (M/F) c | 43.8/56.2 | 54.3/45.7 | 4.08 d | 0.043 |
| Education c | ||||
| No qualifications | 8.9 | 12.0 | 10.97 d | 0.089 |
| Level 1 | 11.4 | 12.0 | ||
| Level 2 | 34.1 | 22.8 | ||
| Level 3 | 12.3 | 16.3 | ||
| Level 4 | 14.8 | 12.0 | ||
| Level 5 | 2.9 | 1.1 | ||
| Level 6 | 15.6 | 23.9 | ||
| CES-D a | 0.0 (2) | 1.0 (1) | −0.66 b | 0.511 |
| Loneliness a | 3.0 (2) | 3.0 (3) | −1.86 b | 0.063 |
| Marital status (R/NR) c | 69.1/30.9 | 46.7/53.3 | 20.96 d | <0.001 |
| SES c | 3.15 d | 0.533 | ||
| Quintile 1 | 19.9 | 24.7 | ||
| Quintile 2 | 20.1 | 14.6 | ||
| Quintile 3 | 20.0 | 21.3 | ||
| Quintile 4 | 20.1 | 16.9 | ||
| Quintile 5 | 19.9 | 22.5 |
| SCD-mem | SCD-cog | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p | OR (95% CI) | p |
| Demographics | ||||
| SO (SMOA) | 1.70 (0.40, 7.27) | 0.468 | 0.35 (0.03, 2.87) | 0.356 |
| Age | 1.03 (1.02, 1.04) | <0.001 | 1.03 (1.02, 1.04) | <0.001 |
| Sex (F) | 1.07 (0.94, 1.22) | 0.320 | 0.91 (0.75, 1.11) | 0.366 |
| Education (ref: no qualifications) | ||||
| Level 1 | 1.08 (0.80, 1.44) | 0.618 | 1.22 (0.79, 1.88) | 0.374 |
| Level 2 | 1.09 (0.85, 1.40) | 0.477 | 1.44 (1.01, 2.09) | 0.047 |
| Level 3 | 1.07 (0.80, 1.43) | 0.663 | 1.50 (0.98, 2.30) | 0.062 |
| Level 4 | 1.37 (1.03, 1.82) | 0.030 | 1.28 (0.84, 1.96) | 0.261 |
| Level 5 | 1.24 (0.80, 1.91) | 0.325 | 1.14 (0.56, 2.19) | 0.694 |
| Level 6 | 1.35 (1.02, 1.79) | 0.039 | 1.78 (1.19, 2.71) | 0.006 |
| Risk factors | ||||
| CES-D | 1.38 (1.14, 1.72) | 0.002 | 1.35 (1.08, 1.73) | 0.011 |
| Loneliness | 0.95 (0.78, 1.13) | 0.587 | 1.16 (0.90, 1.48) | 0.246 |
| Marital status (R) | 0.75 (0.44, 1.23) | 0.262 | 1.55 (0.73, 3.41) | 0.259 |
| SES (ref: Q1) | ||||
| Quintile 2 | 1.37 (0.60, 3.20) | 0.458 | 1.20 (0.43, 3.41) | 0.713 |
| Quintile 3 | 1.70 (0.80, 3.80) | 0.180 | 0.56 (0.11, 1.95) | 0.394 |
| Quintile 4 | 1.23 (0.55, 2.76) | 0.601 | 0.81 (0.24, 2.51) | 0.720 |
| Quintile 5 | 1.29 (0.61, 2.82) | 0.510 | 0.91 (0.28, 2.83) | 0.873 |
| Interaction effects | ||||
| CES-D × SO | 1.35 (0.93, 2.09) | 0.137 | 1.08 (0.70, 1.78) | 0.727 |
| Loneliness × SO | 0.80 (0.55, 1.15) | 0.251 | 1.20 (0.72, 1.96) | 0.461 |
| Marital status × SO | 0.38 (0.13, 1.02) | 0.060 | 1.38 (0.31, 6.72) | 0.674 |
| SES × SO | ||||
| (Q2 − Q1) × SO | 2.01 (0.38, 10.99) | 0.410 | 1.84 (0.24, 14.71) | 0.551 |
| (Q3 − Q1) × SO | 2.72 (0.60, 13.63) | 0.205 | 0.41 (0.02, 4.97) | 0.513 |
| (Q4 − Q1) × SO | 1.50 (0.30, 7.47) | 0.613 | 1.03 (0.09, 9.74) | 0.980 |
| (Q5 − Q1) × SO | 2.46 (0.55, 11.73) | 0.244 | 1.42 (0.14, 13.52) | 0.754 |
| RCI-epi | RCI-sem | |||
|---|---|---|---|---|
| Variable | β (95% CI) | p | β (95% CI) | p |
| Demographics | ||||
| SO (SMOA) | 0.20 (−0.76, 1.16) | 0.678 | −1.23 (−2.57, 0.10) | 0.070 |
| Age | −0.01 (−0.02, −0.01) | <0.001 | −0.02 (−0.03, −0.02) | <0.001 |
| Sex (F) | 0.05 (−0.04, 0.015) | 0.283 | 0.03 (−0.10, 0.16) | 0.655 |
| Education (ref: no qualifications) | ||||
| Level 1 | −0.16 (−0.37, 0.04) | 0.123 | 0.14 (−0.15, 0.42) | 0.347 |
| Level 2 | −0.12 (−0.30, 0.05) | 0.168 | 0.10 (−0.15, 0.34) | 0.441 |
| Level 3 | −0.13 (−0.33, 0.08) | 0.230 | 0.15 (−0.14, 0.44) | 0.306 |
| Level 4 | −0.11 (−0.31, 0.10) | 0.305 | 0.19 (−0.09, 0.47) | 0.184 |
| Level 5 | −0.16 (−0.47, 0.15) | 0.306 | 0.08 (−0.35, 0.51) | 0.721 |
| Level 6 | −0.17 (−0.37, 0.03) | 0.093 | 0.05 (−0.23, 0.33) | 0.744 |
| Risk factors | ||||
| CES-D | 0.03 (−0.10, 0.15) | 0.680 | −0.24 (−0.41, −0.06) | 0.008 |
| Loneliness | −0.05 (−0.17, 0.07) | 0.455 | 0.19 (0.02, 0.36) | 0.026 |
| Marital status (R) | 0.21 (−0.32, 0.36) | 0.905 | −0.11 (−0.59, 0.36) | 0.643 |
| SES (ref: Q1) | ||||
| Quintile 2 | 0.09 (−0.46, 0.64) | 0.754 | −0.44 (−1.21, 0.32) | 0.258 |
| Quintile 3 | 0.14 (−0.38, 0.65) | 0.600 | −0.95 (−1.67, −0.24) | 0.009 |
| Quintile 4 | 0.10 (−0.42, 0.63) | 0.703 | −0.72 (−1.45, 0.01) | 0.053 |
| Quintile 5 | −0.35 (−0.86, 0.16) | 0.177 | −0.56 (−1.27, 0.15) | 0.123 |
| Interaction effects | ||||
| CES-D × SO | 0.03 (−0.23, 0.28) | 0.832 | −0.50 (−0.86, −0.15) | 0.005 |
| Loneliness × SO | −0.09 (−0.33, 0.15) | 0.482 | 0.42 (0.09, −0.75) | 0.014 |
| Marital status × SO | −0.04 (−0.73, 0.64) | 0.897 | −0.40 (−1.35, 0.55) | 0.413 |
| SES × SO | ||||
| (Q2 − Q1) × SO | −0.12 (−1.22, 0.99) | 0.834 | −1.08 (−2.61, 0.46) | 0.169 |
| (Q3 − Q1) × SO | 0.14 (−0.88, 1.17) | 0.783 | −1.74 (−3.17, −0.31) | 0.017 |
| (Q4 − Q1) × SO | 0.18 (−0.86, 1.23) | 0.738 | −1.35 (−2.80, 0.11) | 0.070 |
| (Q5 − Q1) × SO | −0.93 (−1.94, 0.09) | 0.075 | −1.29 (−2.71, 0.13) | 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manca, R.; Flatt, J.D.; Venneri, A. Differential Impact of Risk Factors for Cognitive Decline in Heterosexual and Sexual Minority Older Adults in England. Brain Sci. 2025, 15, 90. https://doi.org/10.3390/brainsci15010090
Manca R, Flatt JD, Venneri A. Differential Impact of Risk Factors for Cognitive Decline in Heterosexual and Sexual Minority Older Adults in England. Brain Sciences. 2025; 15(1):90. https://doi.org/10.3390/brainsci15010090
Chicago/Turabian StyleManca, Riccardo, Jason D. Flatt, and Annalena Venneri. 2025. "Differential Impact of Risk Factors for Cognitive Decline in Heterosexual and Sexual Minority Older Adults in England" Brain Sciences 15, no. 1: 90. https://doi.org/10.3390/brainsci15010090
APA StyleManca, R., Flatt, J. D., & Venneri, A. (2025). Differential Impact of Risk Factors for Cognitive Decline in Heterosexual and Sexual Minority Older Adults in England. Brain Sciences, 15(1), 90. https://doi.org/10.3390/brainsci15010090