1. Introduction
Epilepsy is a neurological disease that presents recurrent and unprovoked seizures [
1]. This disease affects the physical health of the patient. It can impact mental health and significantly decrease quality of life [
1,
2].
According to the World Health Organization (WHO), it is estimated that around 50 million people worldwide have epilepsy, with an annual diagnosis rate of approximately five million people [
3]. In the United States, the Center for Surveillance, Epidemiology, and Laboratory Services estimated that in 2010 2.3 million adults had active epilepsy, and that this number had increased to three million adults by 2015 [
4]. From January to September 2019, patients undergoing assessment or treatment for epilepsy accounted for 2,998,000 consultations in the medical units of the Mexican Institute of Social Security (IMSS) [
5]. In [
6], through the analysis of six epilepsy studies in Mexico, the prevalence rate was found to be between 3.9 and 42.2 cases per thousand inhabitants. The prevalence varied significantly by location.
The electroencephalogram (EEG) is one of the main tools used for the diagnosis of epilepsy. Manually analyzing EEG recordings is very time consuming; therefore, using computational tools for their analysis and characterization improves the diagnostic process [
7]. Several of the computational tools used to analyze EEG recordings are derived from the artificial intelligence field, including machine learning (ML) and deep learning (DL).
On the one hand, ML has been widely applied in epilepsy for seizure detection, differentiation of seizure states, and localization of seizure foci [
8]. Conversely, the use of DL techniques in epilepsy has increased regarding classification and prediction tasks [
9]. As mentioned by [
7], these DL techniques are usually reliant on nontransparent models.
In interesting work presented by [
10], the authors proposed novel representations, namely, the unigram ordinal pattern (UniOP) and bigram ordinal pattern (BiOP), to capture underlying dynamics in EEG time series for seizure detection. Their approach demonstrated high accuracy in discriminating between healthy and seizure states, outperforming existing methods. A recent work [
11] employed a combination of Variable-Frequency Complex Demodulation (VFCDM) and Convolutional Neural Networks (CNN) to discriminate between health, interictal, and ictal states using electroencephalogram (EEG) data then evaluating CNN performance through leave-one-subject-out cross-validation (LOSO CV), achieving consistently high accuracy rates between healthy and epileptic states.
Unfortunately, it is difficult to explain the decisions of a nontransparent model, and, as argued in [
12], explanations of the predictions are necessary to justify the reliability of the models. A solution to this problem can be found in the explainable artificial intelligence (XAI) field, which aims to produce justifications that facilitate the comprehension of a model’s functioning and of the rationale behind its decisions, allowing end users to trust the model [
13].
In the state of the art, several studies have explored the utilization of XAI for the analysis of EEG signals and the detection of seizures. In [
14], a deep neural network for seizure detection was designed. The model was subjected to adversarial training in order to acquire seizure representations from EEG signals. Additionally, an attention mechanism was implemented to assess the significance of individual EEG channels.
In [
15], the connectivity characteristics of EEG signals were estimated, then a set of neural networks was trained to detect seizures. The activation values of the neurons in the classifiers were utilized to estimate the relevance of the characteristics. The findings indicated that the relevance values varied for each subject.
In [
16], the authors discussed the application of DL algorithms for the diagnosis of epilepsy. In addition, the use of XAI to explain the model’s decisions was explored. Among the various XAI techniques evaluated, only attention pooling could extract the most significant segments from the signals. However, it was suggested that epileptographic patterns may be too complex to be captured using attention pooling.
Other XAI techniques, such as Shapley Additive Explanations (SHAP) [
17], have been employed for different tasks. One such task the classification of the pre-ictal and inter-ictal phases, as described in [
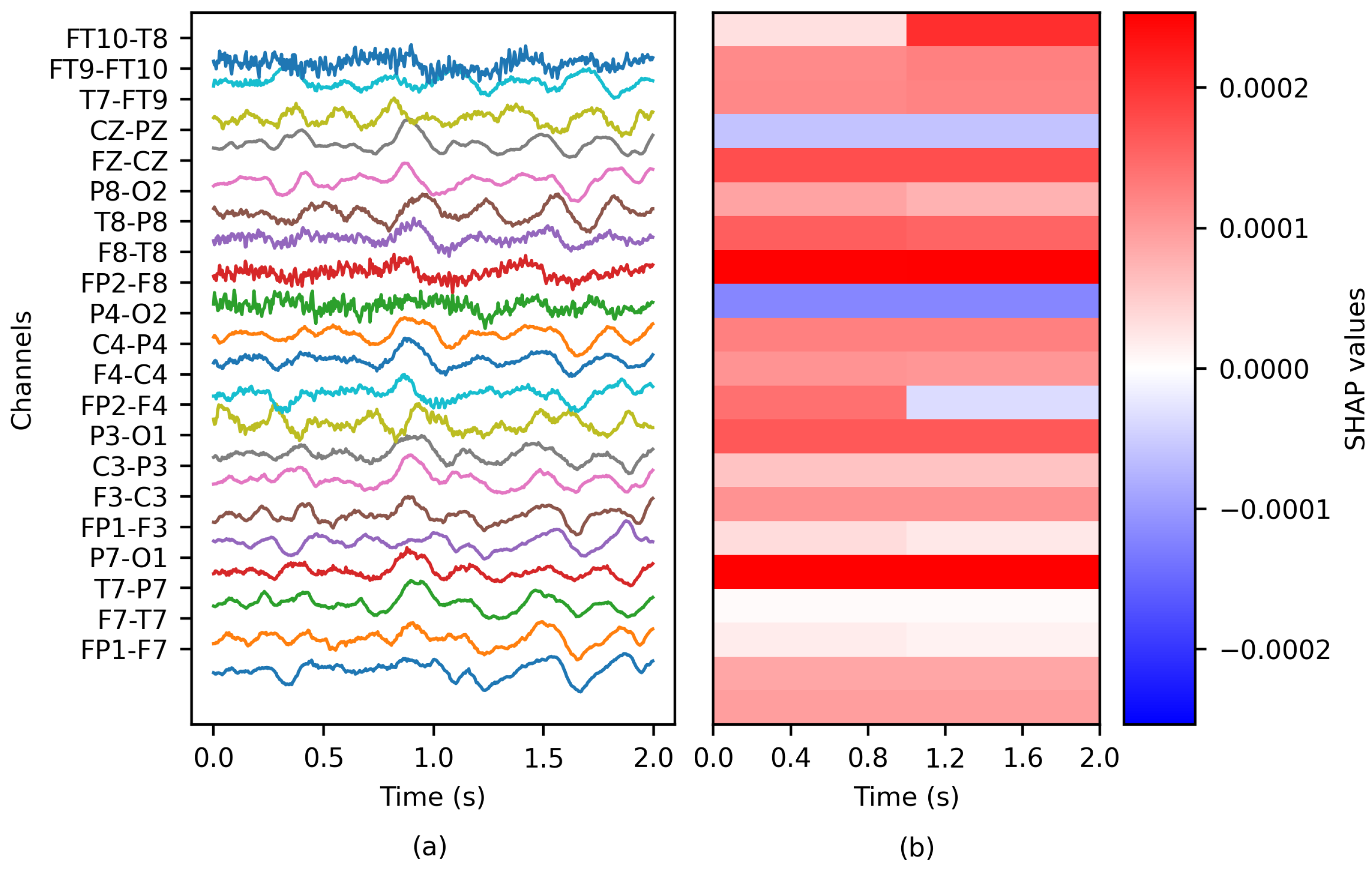
18], where the authors used SHAP to assess each EEG channel’s significance and demonstrated how this significance varied over time. Another task for which SHAP has been utilized was presented in [
19], where the detection of epileptic seizures from time–frequency domain transformations of EEG was studied using neural networks. Here, the task for SHAP was to visually identify the frequencies that contributed most to the classification.
In [
20], the authors proposed a system which uses a Bi-LSTM network for classification of normal and abnormal signals caused by epilepsy and the Layerwise Relevance Propagation (LRP) XAI method to explain the predictions of the network. The LRP method generates a relevance vector for the test input vector. The authors reported that these relevance values indicate the contribution of each datapoint of a signal, helping to classify signals into a particular class.
In another work, SHAP formed part of a methodology known as XAI4EEG developed for the detection of seizures and explanation of the model’s decisions [
21]. This technique consists of extracting the time and frequency features of EEG signals for classification by two convolutional neural networks, with SHAP implemented for explanation generation.
In [
22], the authors performed minor signal processing steps such as filtering, and used the discrete wavelet transform (DWT) to decompose the EEG signals and extract various eigenvalue features of the statistical time domain (STD) as linear and Fractal Dimension-based Nonlinear (FD-NL) features. Following this feature extraction step, the optimal features were identified through correlation coefficients with p-value and distance correlation analysis and classified using a Bagged Tree-Based Classifer (BTBC), followed by SHAP to provide the explanations.
Based on the understanding that DL models can identify patterns in epileptic EEG signals, are these patterns alone helpful? In addition, if we add transparency using XAI, could the explanations help to identify ictal EEG patterns?
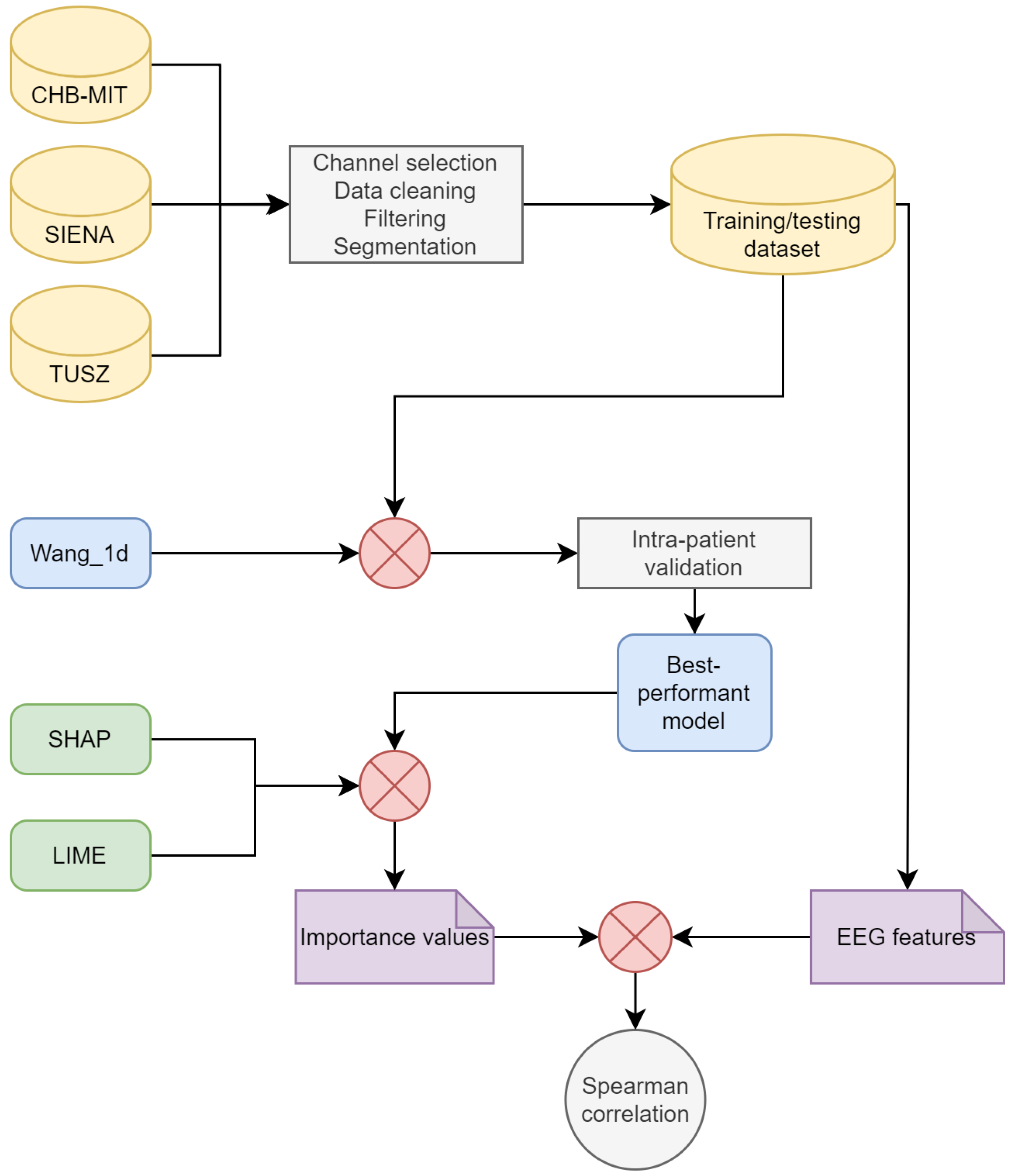
The main objective of this work is to evaluate the utility of explanations generated by XAI techniques such as SHAP and Local Interpretable Model-Agnostic Explanations (LIME) in identifying epileptiform patterns in EEG signals. The aim is to determine whether these explanations can enhance the understanding of deep learning (DL) models and assist in identifying ictal patterns in EEG signals. To achieve this, three EEG databases and a state-of-the-art DL model are utilized to evaluate the models’ performance under different training conditions. Moreover, EEG features are computed for each channel, and the Spearman’s rank correlation coefficient between these features and the importance values generated by XAI techniques is assessed. In summary, this study aims to highlight the complexity involved in identifying ictal patterns from DL models and to explore the role of transparency provided by XAI techniques in this process.
4. Discussion
This section presents a discussion of the results and their interpretation. In addition, the limitations of the present work and future research opportunities are addressed.
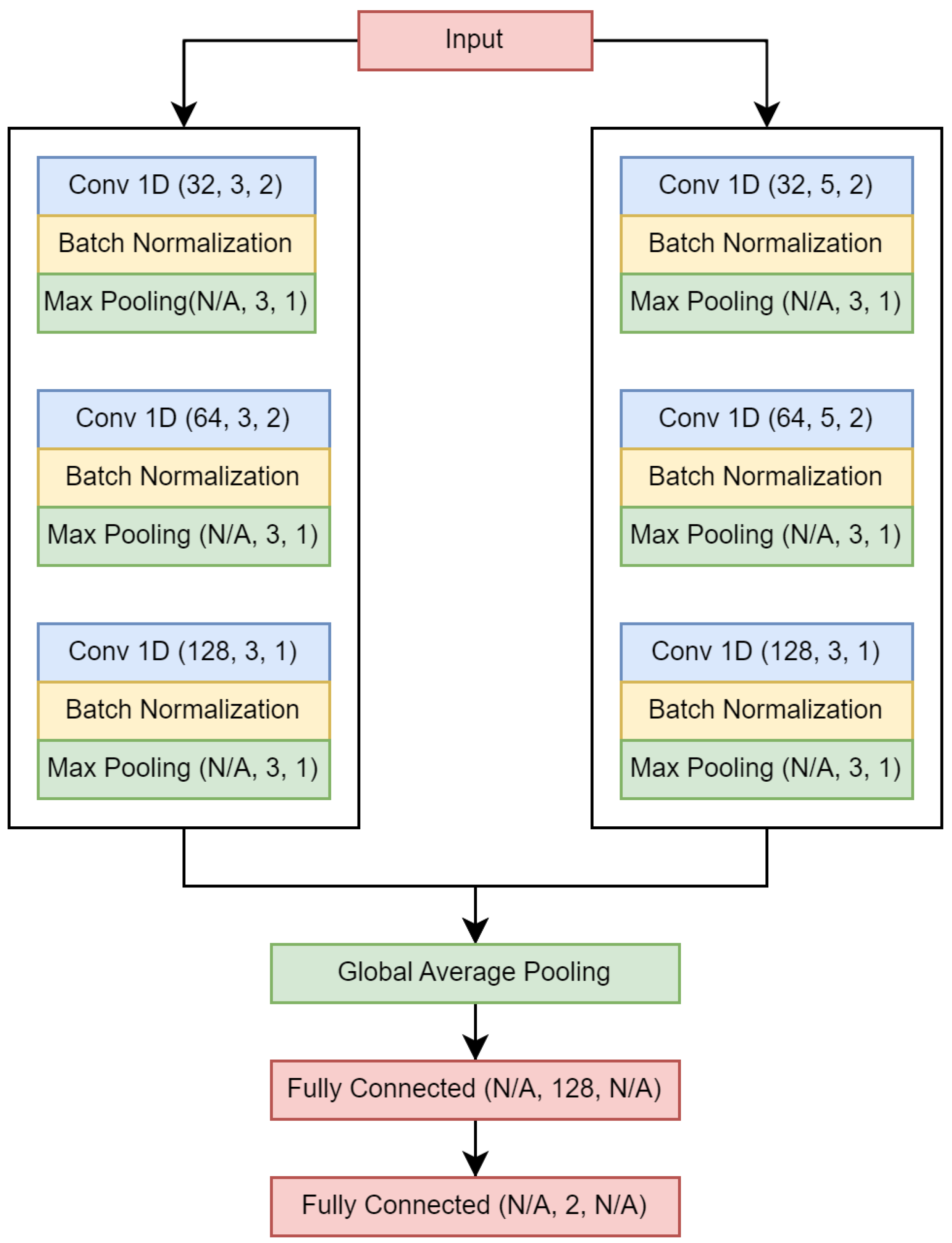
A state-of-the-art DL model was evaluated in this study, specifically, the one-dimensional convolutional neural network for seizure onset detection presented in [
30]. Despite aiming to select models that demonstrated high performance and rigor in their evaluation, it should be acknowledged that the search for models could have been more comprehensive.
In [
30], two databases were employed, namely, CHB-MIT [
23] and SWEC-ETHZ iEEG [
44], with the former being surface and the latter intracranial. Furthermore, the models were trained using an intra-patient approach. The results reported in [
30] using the CHB-MIT data showed mean sensitivity, specificity, and accuracy values of
,
, and
, respectively. In contrast, our study utilizing the same EEG dataset (see
Table 4) reported maximum sensitivity, specificity, and accuracy of
,
, and
, respectively, with significantly lower specificity. It is essential to consider the differences in data formation between [
30] and our work, such as the use of short-duration seizures, avoidance of seizure concatenation, and overlapping rates.
A brief overview of similar studies conducted using comparable methodologies is presented next. In [
45], a sensitivity of
was reported for intra-patient models; this was achieved by applying a convolutional neural network in conjunction with a long short-term memory network. In [
46], the authors employed inter-patient models using only the CHB-MIT database, and reported mean values of
,
, and
for sensitivity, specificity, and accuracy, respectively. In [
47], the authors trained patient-specific convolutional neural networks and reported values of
and
for sensitivity and the area under the curve, respectively. In [
48], the authors utilized a neural network called ScoreNet, achieving a sensitivity of
and specificity of
. Finally, an accuracy of
was obtained by [
14], who trained inter-patient models using an adversarial neural network. Among the mentioned works, ref. [
45,
46,
47,
48] used the CHB-MIT database, while [
14] used the TUH EEG Seizure Corpus. However, there are other works that have reported better performance in terms of accuracy, such as [
11] for advanced epilepsy detection by applying VFCDM and CNN, who achieved consistently high accuracy rates between healthy and epileptic states. However, their results were obtained for the Bonn database, which contains only five patients with epilepsy. In our work exploring the importance of EEG channels in detecting epileptic seizures, we have identified that database and training conditions can affect classifier performance.
Regarding the work presented in [
10], the authors selected three EEG datasets, one of which was the publicly available Bonn dataset, to demonstrate that their method outperformed several state-of-the-art methods. A second dataset was used to show the good generalization ability of their proposed method, and a third dataset to demonstrate that their method is suitable for large-scale datasets. In our work, we selected three EEG datasets to train and evaluate the models under different conditions of overlap between EEG data windows.
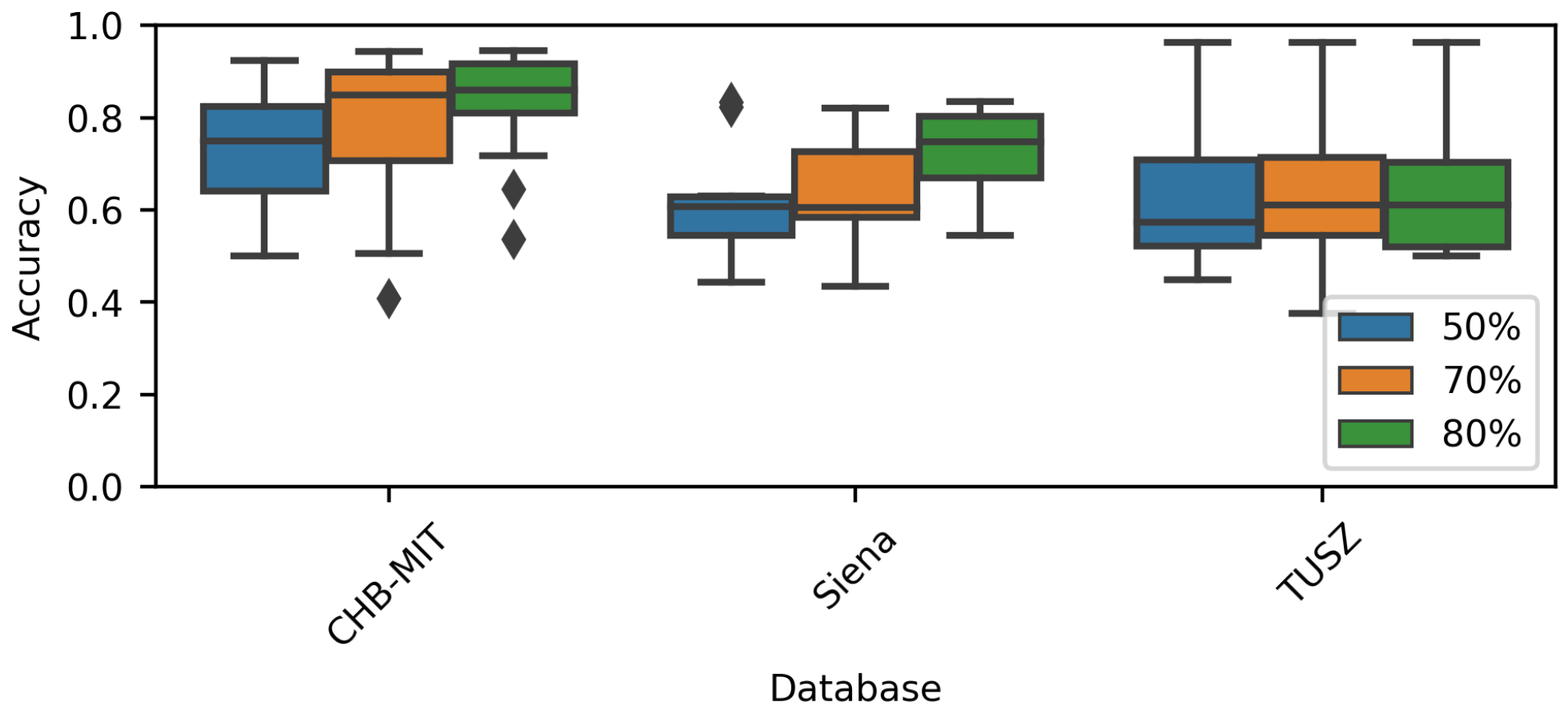
One of the goals of the present research was to understand how the training conditions can impact a model’s performance. First, the results showed that a model’s sensitivity and specificity can vary noticeably based on the EEG dataset. For example, the overall specificity for CHB-MIT models was more significant than for the rest of the models (see
Figure 5). Accordingly, any ML model used to detect seizures should be evaluated across diverse EEG datasets.
The differences in performance can be explained by the differences between the EEG datasets, such as the EEG channels, sampling frequency, patient demographics, and epilepsy characteristics. Second, it was observed that an overlap during training impacts the model’s performance. During this research, the overlap was applied to the ictal instances to address class imbalances. In addition, the largest class (non-ictal) was subsampled to generate a balanced dataset.
Our results showed that the more significant the overlap applied to the ictal class, the higher the accuracy. It should be noted that a significant overlap implies that the training dataset size has increased. An exception is the TUSZ dataset;
Table 4 shows an increase in overall accuracy for the TUSZ models, although the increase is not significant.
Our work can be compared to similar state-of-the-art works with the primary objective of automatically detecting seizures by applying machine learning methods to EEG signals and incorporating explainable artificial intelligence techniques to enhance the interpretability of the models used in seizure detection. First, we have the work presented in [
20]; the authors proposed a system which uses a Bi-LSTM network to classify normal and abnormal signals caused by epilepsy, achieving an accuracy of 87.25% on the Bonn dataset. They used the Layerwise Relevance Propagation (LRP) XAI method to explain the predictions of their network. LRP generates a relevance vector containing relevance values to indicate the contribution of a signal in particular class. However, as stated by the authors, many points in the relevance vector were missed; thus, this implementation of the LRP method requires further improvement to generate more accurate results. In [
22], the main difference with our work is in the feature extraction step. They reported an accuracy of 99.6% on the Bonn dataset, and their explanations were over the features rather than the signal morphology (time series). In our work, we chose a state-of-the-art deep learning model for seizure detection and three EEG databases. The developed models were trained and evaluated under different conditions and the classifiers with the best performance were selected. SHAP and LIME were then employed to estimate the importance value of each EEG channel. To measure the similarity between the explanations and the epileptic signals, we computed the Spearman’s rank correlation coefficient between the EEG features of epileptic signals (time series) and the importance values. Another important difference between these works are the data sources. In [
20,
22], the authors used an open access dataset published by researchers at Bonn University containing intracranial EEG recordings from a total number of ten subjects, of whom five were healthy volunteers and the other five were epilepsy patients. Compared to our work, in which three databases were tested, previous works have used a limited dataset in order to evaluate their algorithms. Furthermore, studies employing the Bonn dataset used intracranial instead of scalp EEG recordings.
The interpretability of classification models used in the medical field is crucial, as mentioned by [
12,
49]; although the number of XAI algorithms is significant, not all algorithms can be applied to time series. Compared to other fields, the interpretation of time series in this field is usually not intuitive, and requires domain knowledge [
13,
50]. In the present work, SHAP and LIME, which are both agnostic and local methods, were applied. SHAP has previously been used for EEG signals; selected use cases are displayed in
Table 7.
In light of the capacity of XAI methods to identify information relevant to the classifier, it may be possible to identify discriminating ictal patterns in high-importance regions (e.g., large SHAP values would match large STD values). As XAI aims to provide transparency, understandable ictal patterns would be preferable.
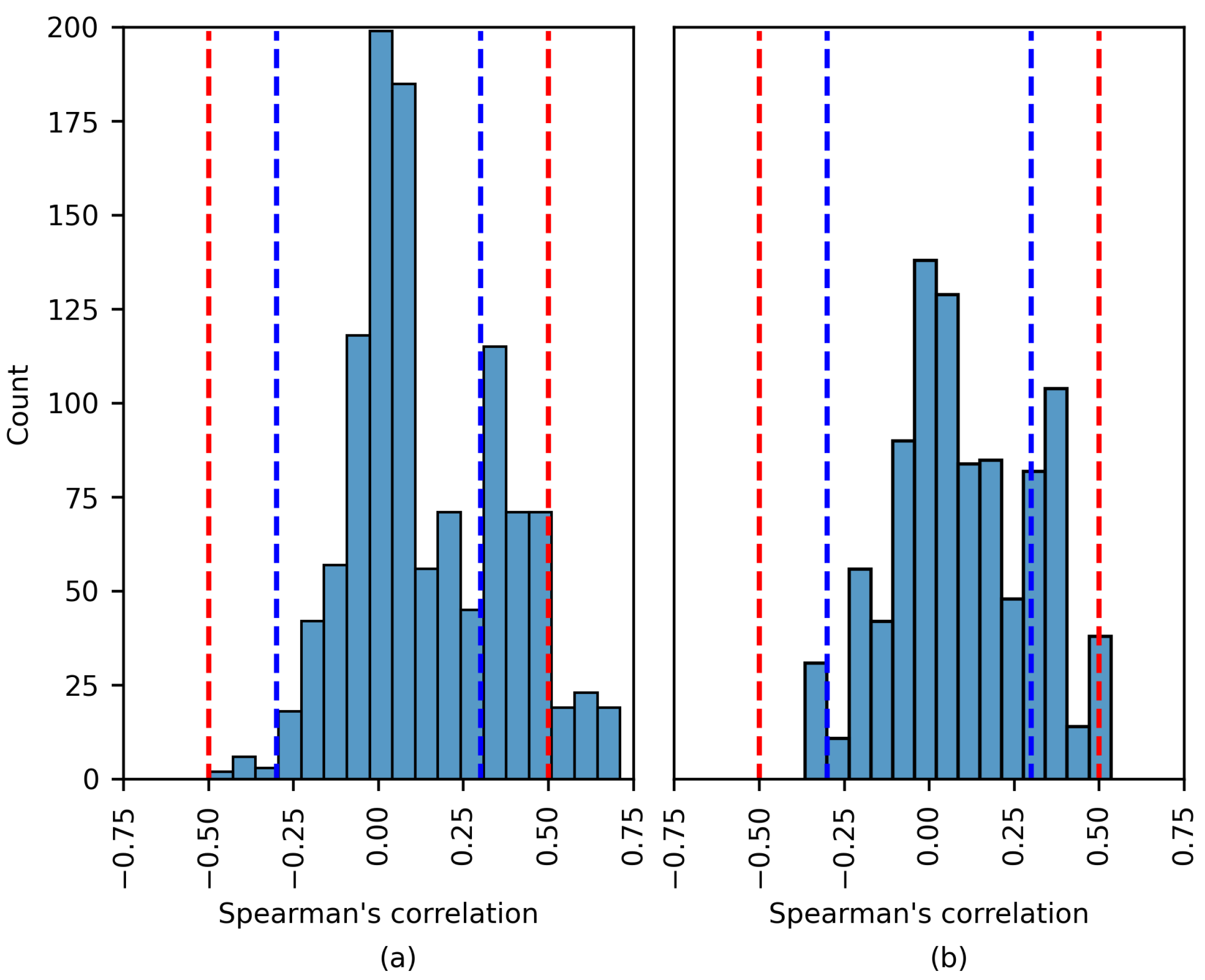
In line with the above, the Spearman’s rank correlation coefficient between the XAI-generated importance values and the EEG features was computed. As previously stated, this coefficient measures the strength of a monotonic relationship.
As deduced from the results, the strength of the relationship was low and negligible even for high-performing models. The most remarkable cases are described in
Table 6. It was observed that experiments resulting in a moderate correlation did not present high accuracy; therefore, a larger correlation coefficient does not imply better performance. The only exception was patient 4456 (TUSZ dataset).
To the best of the authors’ knowledge, there is no similar study in the state of the art; hence, the comparison was complex. However, the difficulties in obtaining epileptic EEG patterns have been described in previous works, e.g., [
15,
18]. It is relevant to mention that while several previously published works have included XAI to increase the transparency, they did not apply a pattern/explanation evaluation stage.
In addition to the above, the following limitations must be considered: the applied XAI methods, the small set of EEG features, and the chosen classification model. Although more extensive experiments could be performed to search for correlation patterns, alternative approaches must be considered. These are outlined below.
In [
55], the classification of seizure and non-seizure states was performed. Random forest showed the best accuracy among the evaluated classification models. Bidirectional network graphs and the lifespan of homology classes were computed to characterize the EEG windows. SHAP was implemented to provide model transparency. The use of EEG features as model inputs provided an initial foundation for transparency, contrary to the raw EEG signals.
In [
56], the classification of eight seizure types was addressed. A deep neural network was used for classification and raw EEG windows were used as model inputs. SHAP and topographic maps were applied for transparency. Notably, network activation was used to plot the topographic maps. This technique adds a spatial feature to the XAI explanations, which may indeed be helpful for medical staff.
Additionally, seizure prediction was addressed in [
57]. A list of univariate linear features was estimated from EEG recordings. Support vector machine, logistic regression, and CNN were applied during classification. A diverse set of techniques was used to provide explainability, e.g., SHAP, LIME and partial dependency plots. Importantly, the explanations were evaluated by humans (data scientists and clinicians).
Finally, there are a number of limitations in the present work. First, even though a deeper literature revision was performed, modeling the three datasets using several architectures is required to measure the effect of architecture variations. Second, it would be interesting to group the information by several different conditions (for example, on the basis of seizure type, sex, and age, among others) in order to evaluate their effects on detection of ictal patterns. Third, as the use of the Spearman correlation constrains the search to monotonic relations, different nonlinear metrics should be used.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}