Abstract
Background: Cognitive remediation therapy (CRT) for anorexia nervosa (AN) is an intervention specifically focused on addressing cognitive difficulties associated with the eating disorder. This systematic review of systematic reviews and meta-analysis aimed to provide a summary of the existing literature examining the efficacy of CRT in improving the neuropsychological, psychological, and clinical parameters of patients with AN. Methods: Systematic reviews and meta-analyses were sought in electronic databases, encompassing studies that explored the impact of CRT on AN. Three eligible reviews were identified based on the inclusion criteria. The Revised Assessment of Multiple SysTemAtic Reviews (R-AMSTAR) was employed to evaluate the methodological quality of the reviews, and all included reviews demonstrated satisfactory methodological quality with an R-AMSTAR score of ≥22. Relevant information was extracted from each review and qualitatively compiled. Results: Findings suggest that CRT can help people increase their awareness of cognitive styles and information processing and have a positive effect on patients’ responses to treatment. Conclusions: Further research is required to better understand its impact on other relevant outcomes, including psychological variables, to optimize the treatment’s benefits.
1. Introduction
Anorexia Nervosa (AN) is a severe and persistent eating disorder (ED) characterized by self-starvation, a reduction in body weight, and the perception of distorted body size and shape [1]. It is the leading cause of death among all mental health conditions, and an estimated 0.9% of women and 0.3% of men will experience AN at some point in their lifetime [2]. The available evidence for treating AN is limited [3,4] due to patients’ uncertainty toward change, drop-out rates of 20–40% [5], and low treatment acceptance [6].
In terms of clinical presentation, people with AN often focus on specific behaviors and routines, such as rigid rules [7]. Consequently, it is crucial to devise interventions that target the risk and maintenance aspects of AN rather than the core symptoms and concerns of the ED [8,9].
Particularly, neuropsychological research has highlighted two main cognitive deficits in AN, i.e., cognitive inflexibility (or limited set-shifting) [10] and intense attention to detail (or reduced central coherence) that indicate reduced executive and visual-constructive functions [11,12,13]. Reduced set-shifting refers to cognitive difficulties in shifting attentional control upon different tasks and in using different cognitive strategies as environmental circumstances change, while reducing central coherence involves intense focus on details rather than thinking in a holistic processing of information [14,15,16]. Among individuals with AN, both weak set-shifting and reduced central coherence are typically observed through obsessions with food, body image, weight, and compulsive actions like monitoring calories and exercising. Both set-shifting and weak central coherence could contribute to the development of AN [17] and could persist despite weight gain [18], thus contributing to diminished participation and compliance with treatment [19].
The difficulty of addressing AN has led to the conceptualization of novel approaches aimed at addressing these challenges, therefore fostering patients’ awareness of their cognitive styles and encouraging the adoption of alternative strategies.
In recent years, the evidence supporting cognitive remediation therapy (CRT) for AN has been growing [20,21]. CRT is a structured intervention delivered by paper-and-pencil or computer-based cognitive exercises centered on improving cognitive flexibility and holistic thinking. It directs its attention toward cognitive processes rather than emotional aspects, thus addressing cognitive function defects rather than the psychopathology of ED [22,23]. It is also aimed at increasing individuals’ motivation to change and overall quality of life [14,24,25,26,27,28,29,30].
However, the optimal use of CRT for AN treatment remains under exploration, and published systematic reviews and meta-analyses of CRT for AN reveal conflicting conclusions.
The present study aims to provide a summary of published systematic reviews and meta-analyses on the efficacy of CRT in improving cognitive flexibility, central coherence, set-shifting ability, motivation to change, and the quality of life in patients with anorexia nervosa.
2. Materials and Methods
This work was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [31]. The protocol for this study was registered with the International Prospective Register of Systematic Reviews (PROSPERO), nr. CRD42023459389. Trial Registration: PROSPERO ID CRD4202345938.
2.1. Literature Search
A systematic literature search of six databases (Scopus, PubMed, Google Scholar, PsychINFO, the Cochrane Library, and the Centre for Review and Dissemination—CRD) was conducted between 4 September and 31 October 2023. Under the PICO framework (Patient problem or population; Intervention; Comparison or control and Outcome) [32], the search strategies included the following terms: (anorexia) AND (cognitive remediation therapy) AND (flexibility OR central coherence OR set shifting OR body mass index-BMI) OR eating disorder OR motivation OR quality of life). Search terms were systematically combined by Boolean and truncation operators. The search syntax was modified as appropriate for each database.
2.2. Inclusion and Exclusion Criteria
Only systematic reviews and meta-analyses that met the following criteria were included: (1) people with AN, (2) explored the efficacy of cognitive remediation therapy in at least one cognitive/psychological domain (e.g., cognitive flexibility, central coherence, set-shifting ability, motivation to change, and quality of life), and (3) received a methodological quality score of 22 or higher in the Revised Assessment of Multiple SysTemAtic Reviews (R-AMSTAR) [33]. Studies were excluded if they (1) considered only biomedical outcomes. No limitations were set for language and year of publication, or for the age, gender, and ethnicity of the sample.
2.3. Selection Process
Two reviewers (G.M. and G.P.) independently screened the eligibility of the articles based on their titles, abstracts, and then their full texts. Disagreements were solved through discussion with a third researcher (D.M.C.). Furthermore, reference lists were manually examined for the possible inclusion of relevant records. The review team included at least one person with methodological expertise in conducting systematic reviews (G.P. and M.S.) and at least two experts on the topic under review (authors G.C. and D.M.C.) [34].
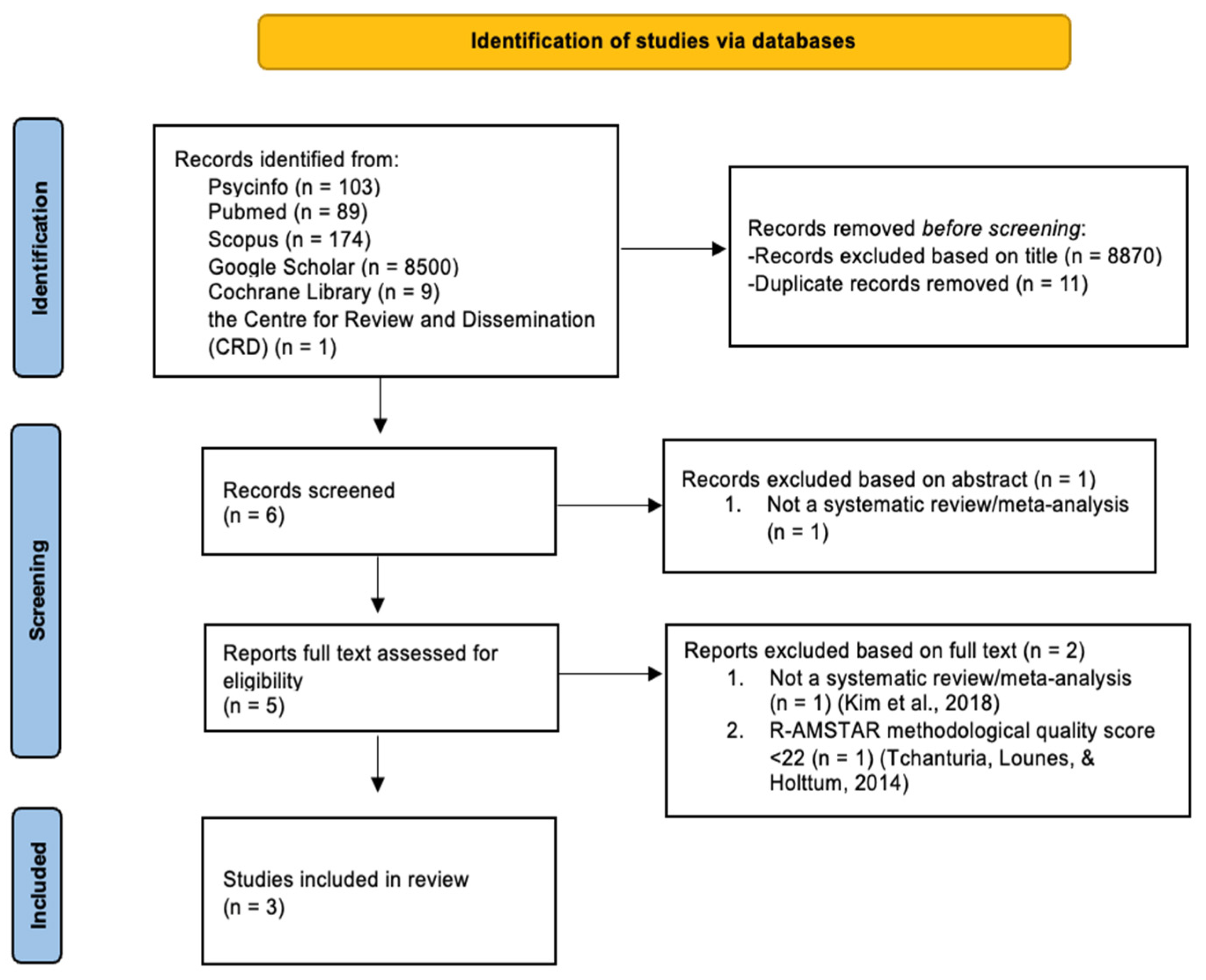
Following the PRISMA guidelines [35], the flowchart presented in Figure 1 provides step-by-step details of the study selection procedure.
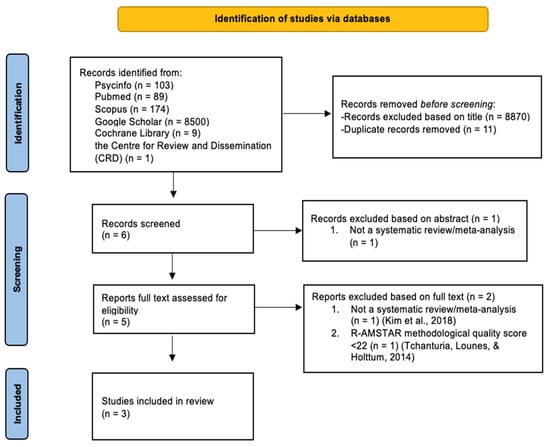
Figure 1.
The PRISMA flowchart [36,37].
2.4. Data Extraction
The following data were independently extracted by reviewers GM and GP, and any disagreements were resolved by consensus and consultation with a third researcher (author DMC): the author and year of publication, country, the aim of the review, the number of relevant included studies, study design, sample size, the age and gender of the participants, the duration of the intervention, format, and outcomes (Table 1).

Table 1.
Characteristics of included studies.
The extracted data were used to produce a narrative summary of the effects of CRT on improving the outcomes of people with AN.
2.5. The Assessment of the Risk of Bias
The R-AMSTAR checklist [33] was used to assess the methodological quality of the included systematic reviews and meta-analyses. It assesses the presence of 11 domains: 1. a priori design, 2. duplicate study selection and data extraction, 3. comprehensive literature exploration, 4. the incorporation of publication status as an inclusion criterion, 5. a list of included/excluded studies, 6. the attributes of included studies, 7. the evaluation of the scientific quality of selected studies, 8. the appropriate utilization of scientific quality in formulating conclusions, 9. the appropriate use of methodologies to combine study results, 10. the assessment of the potential publication bias, and 11. the inclusion of conflicts of interest. The score for each domain varies from 1 to 4, and the R-AMSTAR’s total scores range from 11 to 44. To include the reviews, a total score of 22 was mandatory. Two reviewers (G.M. and G.P.) evaluated the methodological quality of the selected reviews, and disagreements were resolved by a third researcher (D.M.C.) (Table 2).
Table 2.
Article Quality Assessment.
2.6. Data Analysis and Synthesis
Initially, reviews were examined, and pertinent details were extracted and documented. The outcomes from various reviews were combined using a qualitative summary to inform the efficacy of the treatment. A summary of quantitative results was not calculated from the meta-analyses that incorporated comparable studies due to the limitation that a meta-analysis of meta-analyses can only be conducted if the data from individual studies are not duplicated across multiple meta-analyses [34,39]. Indeed, seven [40,41,42,43,44,45,46] out of the 29 studies reviewed were included in more than one selected systematic review and meta-analysis (see Appendix A).
3. Results
3.1. Study Selection
A total of 8876 articles were initially identified: 11 were duplicates while 8871 records were excluded by reading their title and abstract. The full text of the remaining five articles was then screened, resulting in the exclusion of two records for the following reasons: (1) not a systematic review/meta-analysis [36] and (2) R-AMSTAR methodological quality score < 22 [37].
Three studies presenting a summary of evidence on the efficacy of CRT for AN entered this second-order review: one study aimed at conducting a systematic review of single case reports, case series, and RCTs [38]; Tchanturia et al., (2017) carried out a systematic review of single or multiple case studies and qualitative contributions [21], and a systematic review and meta-analysis of RCTs was conducted by Hagan et al. 2020 [20].
3.2. The Characteristics of the Included Studies
Table 1 provides a summary of the characteristics of each included review. All of the reviews examined the efficacy of CRT for patients with AN.
The total number of participants across reviews ranged from 303 [20] to 367 [21]. In terms of gender, two studies [20,38] included a higher proportion of female participants, while one study reported no gender information [21]. None of the selected contributions set any age-related inclusion criteria, and the ages of the participants ranged from 12 to 62 years in the reviews.
CRT treatments were delivered either individually or in groups, with a frequency ranging from one to three times per week and a total number of sessions ranging from 4 to 36.
In addition, the review by Dahlgren et al., (2014) also included studies providing family interventions and computer-assisted CRT [38].
3.3. The Methodological Quality of Included Reviews
The R-AMSTAR scores of the three included systematic reviews and meta-analyses (see Table 2) ranged from 25 [21,38] to 32 [20], with a mean score of 27.33 (SD = 4.04). The highest scores were assigned to Item #3 (Was a comprehensive literature search performed?) and Item #6 (Were the characteristics of the included studies provided?), in which all three systematic reviews and meta-analyses achieved the maximum.
Maximum scores were also obtained by Dahlgren et al., (2014) [38] in Item #5 (Was a list of studies—included and excluded—provided?), and by Hagan et al., (2020) [20] in Item #2 (Was there a duplicate study selection and data extraction?). In addition, minimum scores were given to Dahlgren et al., (2014) [38] and Tchanturia et al., (2017) [21] in Item #7 (Was the scientific quality of the included studies assessed and documented?) and Item #8 (Was the scientific quality of the included studies used appropriately in formulating conclusions?). Furthermore, Dahlgren et al., (2014) [38] received minimum scores in Item #2, Item #9 (Were the methods used to combine the findings of studies appropriate?), and Item #10 (Was the likelihood of publication bias assessed?), while Tchanturia et al., (2017) [21] received minimum scores in Item #4 (Was the status of publication—i.e., grey literature—used as an inclusion criterion?) and Item #11 (Was the conflict of interest included?). The highest scores across the selected systematic reviews and meta-analyses were for performing a comprehensive literature search (Item #3), and for providing the characteristics of the included studies (Item #6), the lowest scores were for documenting the scientific quality of the included studies (Item #7), and appropriately using the scientific quality of the included studies to formulate conclusions (Item #8).
3.4. Single Cases
Single-case studies focused on patients’ experiences with CRT. Taken together, results showed the potential of CRT in enhancing patients’ understanding of their thinking styles, regardless of the improvement in outcomes. For example, one of the included studies [47] reported no significant post-treatment changes in the participant’s neuropsychological profile. Still, the subject provided positive feedback and suggested that she had gained more awareness and self-reflection on her cognitive patterns. Furthermore, the respondent showed stable weight and decreased AN symptomatology at a 7-month follow-up.
3.5. Case Series
Different types of case series were reviewed. Studies [46,48,49,50,51,52] documented the applicability of CRT either in individual or group settings. Results also showed that CRT can be applied to patients with AN across ages and stages of the disease.
Case series studies, including the pre- and post-quantitative assessments of outcomes, were difficult to compare as they largely varied in terms of the age of the participants, treatment intensity, and assessment measures. However, patients received approximately the same number of CRT sessions [53,54,55]. The results showed a decrease after CRT treatment in depression and significant positive changes in the attention span among adults, but not in adolescents. For example, in a pre-post study, Dahlgren, et al., (2013) found significant changes in visuospatial memory and both processing and verbal fluency, but not in the executive functioning domain [46]. In another pre-post study [47], adolescent inpatients receiving CRT reported improvements in cognitive flexibility after the intervention, while their healthy counterparts who didn’t receive the intervention did not. No significant improvements were, instead, reported in central coherence. A subsequent follow-up study employing the same sample, together with additional participants, compared subjects with AN who received CRT with those who received no additional treatment [42]. Data were collected at the beginning and end of the intervention, as well as 6 months after treatment termination. No significant changes in neuropsychological and clinical measures were reported at follow-up, although the BMI increase in the CRT sample showed a noteworthy tendency.
A three-group uncontrolled trial comparing patients with severe AN receiving CRT to a group of patients receiving treatment as usual (TAU) plus CRT and a TAU condition showed that only participants assigned to the CRT groups had a post-treatment improvement in motivation to recover, set-shifting, central coherence, and switching task abilities [28].
Last, one-group pre-post studies observed significant improvements in set-shifting among patients with AN receiving CRT [44,56,57,58]. Still, while in Tchanturia et al., (2007) [57], self-reported flexibility was significantly higher post-CRT, no significant changes were reported in self-esteem or cognitive flexibility by Genders & Tchanturia (2010) [58].
3.6. Randomized Control Trials (RCTs)
Included RCTs [26,40,41,42,43,59] either reported significant changes in set-shifting and central coherence at the end of the CRT intervention or revealed non-significant improvements in the above-mentioned variables, depending on the outcome measures.
Specifically, an RCT comparing CRT and cognitive behavioral therapy (CBT) [43] showed increased set-shifting and central coherence abilities in patients receiving CRT, as well as lower dropout rates than their CBT counterparts. Still, no significant between-group differences were found for weight, BMI, or ED symptoms. Other RCTs [40,41], comparing CRT with nonspecific neurocognitive therapy (NNT) or TAU, found significant changes in cognitive flexibility and the quality of life related to ED in the CRT group. Dropout rates, instead, did not vary significantly, and no between-group differences were reported for BMI.
A single RCT [45] revealed improvements in caloric intake and eating-related anxiety in patients receiving exposure and response prevention therapy for AN (AN-EXRP) compared to the CRT group.
No pre-post within-group differences were found in anxiety, depression, obsessive-compulsive symptoms, or perfectionism in CRT groups [41,42,59].
3.7. Qualitative Studies
A few of the case studies included qualitative assessments of patients’ feedback, but only a single investigation was specifically intended to examine patient feedback letters after individual CRT [60]. Most of the participants reported a positive involvement in CRT and expressed that they had acquired knowledge about cognitive patterns and problem-solving techniques that could be used in everyday situations.
4. Discussion
To the best of our knowledge, this work represents the first attempt to summarize the state of the art on the efficacy of CRT for AN by conducting a systematic review of systematic reviews and meta-analyses on the topic. Throughout the selected systematic reviews and meta-analyses, the investigations consisted of RCTs, single case studies, case series, and qualitative evaluations. Inevitably, differences in methodology, delivery modality and setting, and outcome measures across studies posed important challenges in comparing and generalizing research findings. Still, these results have the potential to provide practical insight into the context of the implementation of CRT solutions for AN.
Specifically, regarding neuropsychological outcomes, results were contradictory for both central coherence and set-shifting abilities, the main cognitive domains targeted in the CRT intervention. Several studies found small to moderate improvements in central coherence among patients with AN who received CRT, while others reported no changes [41,42,43]. Also, small-to-moderate and moderate-to-large improvements in set-shifting abilities following CRT were observed, irrespective of the outcome measure [41,43].
Moreover, cognitive flexibility and executive functioning improved significantly following CRT across studies. However, the absence of further changes in cognitive flexibility after 6 months from treatment termination observed in Herbrich et al., (2017) suggests the need for a further exploration of the short- and long-term effects of CRT on neurocognitive domains [42].
Regarding psychological outcomes, Dingemans et al., (2014) [41], Herbrich et al., (2017) [42], and Lock et al., (2018) [59], found no significant differences in anxiety and depression symptoms at the end of the treatment in patients with AN undergoing CRT compared to patients who received TAU. Conversely, Dahlgren et al., (2013) [46] and Tchanturia et al., (2008) [54] identified a decrease in depressive symptoms in those who received CRT in their pre- and post-investigations. Furthermore, Diengemans et al., (2014) [41] and van Passel et al., (2020) [61] noted small to moderate improvements in ED-related quality of life. More research is needed to clarify these conflicting findings and investigate the influence of these comorbidities as moderators. Finally, no significant differences were detected in ED symptoms, both among adults and adolescents. Notably, Lock et al., (2013) [43] showed that CRT is not superior to CBT in alleviating symptoms related to ED, but it has an important effect on certain neurocognitive functions including cognitive flexibility and executive functioning.
Overall, these results point out the specific effect that CRT has on improving the neuropsychological functioning of patients with AN. Its effectiveness in enhancing the psychological well-being of such individuals, on the other hand, remains questionable—at least in the short term. This is not surprising, given the nature, characteristics, and goals of the intervention, which may represent an alternative-integrative approach to treatments focused on managing individuals’ emotional difficulties (e.g., CBT).
It is also interesting to note that, regardless of the statistical significance of the outcomes of the intervention, qualitative studies on the topic agree in suggesting that CRT is useful in promoting the understanding of AN patients about their thinking patterns and in enabling them to learn problem-solving techniques crucial for the autonomous management of their daily difficulties. Consistently, post-treatment improvements in motivation to change were observed. Increased awareness of one’s active role in problem resolution coupled with enhanced perceived self-efficacy, may have contributed to boosting individuals’ intrinsic motivation for treatment.
These considerations lead to the hypothesis that post-CRT, statistically significant improvements in neurological, psychological, and clinical outcomes are expected more in the long term than in the short term, as a result of the person’s continuous commitment to change. Studies with follow-ups extending beyond 12 months from the end of CRT treatment should be implemented to test this possibility.
Regarding clinical outcomes, most of the included studies did not report significant between-group differences in BMI and weight in individuals who received CRT treatment compared to TAU, but BMI decreased among those receiving CRT as reported in case studies. While weight gain is an expected outcome for individuals with AN participating in standard treatments with or without CRT integration, improved clinical parameters recognized by case studies reinforce the role of CRT in determining such an improvement.
Moreover, considering treatment delivery, individual CRT showed lower dropout rates and fostered a more positive patient-therapist alliance compared to group CRT [38]. This might be due to the fact that tasks assigned during group CRT were not perceived to be as relevant as in individual therapy [42,44], therefore they did not strengthen individuals’ motivation to change.
5. Strengths and Limitations
A notable strength of this contribution lies in the rigor of our data extraction and analysis process, which involved multiple researchers independently screening and scrutinizing the information, and the evaluation of the methodological quality of the included systematic reviews and meta-analyses. However, certain limitations must be considered. First, the variety in study design, sample characteristics (such as sample size and age, whether they were inpatients or outpatients), intervention methods (such as individual, family, or group therapy), treatment intensity, and the choice of outcome measures made it challenging to compare findings from the selected reviews and draw solid conclusions about the efficacy of CRT. Also, methodological flows and potential biases of the included studies as assessed by the R-AMSTAR checklist might have influenced the conclusions of the present work.
6. Suggestions and Implications for Future Research
The findings from this systematic review of systematic reviews and meta-analyses indicate that there is a need to implement research in CRT. First, future investigations aimed at testing and/or comparing different ways to deliver CRT should be carried out to better understand their specific advantages and disadvantages, and their effectiveness in improving cognitive, psychological, and clinical outcomes. This might include the testing of differences between individual or group therapy, but also the impact of computer-assisted CRT (CA-CRT) sessions on patients’ outcomes. Indeed, according to Brockmeyer (2013), CA-CRT might lead to increased awareness and the development of new thinking strategies but more studies should be conducted on the topic [40].
Moreover, the single report published on family CRT [62], showed a positive impact of the intervention in enhancing the understanding of how cognitive styles influence family dynamics and improving communication and cooperation among family members during treatments. Family CRT should, therefore, be further explored, also in integration with other therapeutic approaches.
Due to variations in outcome measures among the included records, the generalization of conclusions is complex, and future research might also consider employing more consistent outcome measures—especially concerning psychological outcomes.
Indeed, besides the fact that CRT mainly focuses on improving cognitive functioning, the evaluation of the impact that the intervention might have on emotional aspects is also relevant in future studies, which might also consider implementing and testing a specific CRT module about emotions.
Similarly, research comparing CRT with other treatment methods is limited, like the testing of the integrative impact of CRT on target outcomes. A broader range of comparative-integrative studies should, therefore, be further developed to help determine the role of CRT in the global treatment plan.
Moreover, since studies mainly focus on short-term effects, longitudinal studies would be crucial for understanding the long-term benefits of CRT on AN.
Overall, the selected studies support the feasibility of CRT across different ages and severity levels. However, it was not possible to explore how different types of patients respond to CRT. Future studies could focus more on individual differences, including the impact of age, severity of the disorder, and other relevant psychological and medical conditions on the effectiveness of CRT.
Specifically, knowledge is limited regarding the efficacy of CRT for adolescents diagnosed with AN. Since early engagement in treatment is associated with better outcomes [21], future studies should focus more on this age group.
7. Conclusions
Despite the findings from this systematic review of systematic reviews and meta-analyses revealing limited data, the present study suggests that CRT can help patients with AN become more aware of their cognitive styles and information processing and have a positive impact on treatment response. Some issues persist about CRT arrangements in regards to the intensity and duration needed to improve central coherence and set-shifting. Further research is needed to better understand CRT effects and how to maximize its unique benefits for the treatment of AN.
Author Contributions
Conceptualization, G.P.; methodology, M.S. and G.C.; formal analysis, M.S., G.M. and D.M.C.; data curation, G.P. and D.M.C.; writing—original draft preparation, G.M.; writing—review and editing, G.P., M.S. and D.M.C.; supervision, G.C.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available on request due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Target Studies Included in Each Selected Systematic Review/Meta-Analysis
| Dahlgren (2014) [38] | Hagan (2020) [20] | Tchanturia (2017) [21] | |
| Abbate-Daga (2012) [53] | X | ||
| Brockmeyer (2013) [40] | X | X | |
| Dahlgren (2013) [46] | X | X | |
| Davies (2005) [63] | X | ||
| Dingemans (2014) [41] | X | X | |
| Easter (2011) [52] | X | ||
| Genders (2010) [58] | X | ||
| Giombini (2016) [29] | X | ||
| Giombini (2017) [29] | X | ||
| Harrison (2018) [28] | X | ||
| Herbrich (2017) [42] | X | X | |
| Lask (2013) [62] | X | ||
| Lock (2013) [43] | X | X | |
| Lock (2018) [59] | X | ||
| Pitt (2010) [56] | X | ||
| Pretorius (2007) [64] | X | ||
| Pretorius (2012) [44] | X | X | |
| Sproch (2019) [26] | X | ||
| Steinglass (2014) [45] | X | X | |
| Tchanturia (2006) [65] | X | ||
| Tchanturia (2007) [57] | X | ||
| Tchanturia (2008) [54] | X | ||
| van Noort (2015) [47] | X | ||
| van Noort (2016) [66] | X | ||
| van Passel (2020) [61] | X | ||
| Whitney (2008) [51] | X | ||
| Wood (2011) [49] | X | ||
| Zuchova (2013) [50] | X |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- van Eeden, A.E.; van Hoeken, D.; Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Godier, L.R.; Park, R.J. Compulsivity in anorexia nervosa: A transdiagnostic concept. Front. Psychol. 2014, 5, 778. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G. Evidence-based treatment of anorexia nervosa. Int. J. Eat. Disord. 2005, 37, S26–S30. [Google Scholar] [CrossRef] [PubMed]
- Dejong, H.; Broadbent, H.; Schmidt, U. A systematic review of dropout from treatment in outpatients with anorexia nervosa. Int. J. Eat. Disord. 2012, 45, 635–647. [Google Scholar] [CrossRef] [PubMed]
- Halmi, K.A.; Agras, W.S.; Crow, S.; Mitchell, J.; Wilson, G.T.; Bryson, S.W.; Kraemer, H.C. Predictors of Treatment Acceptance and Completion in Anorexia Nervosa: Implications for Future Study Designs. Arch. Gen. Psychiatry 2005, 62, 776–781. [Google Scholar] [CrossRef]
- Di Lodovico, L.; Gorwood, P. The relationship between moderate to vigorous physical activity and cognitive rigidity in anorexia nervosa. Psychiatry Res. 2019, 284, 112703. [Google Scholar] [CrossRef]
- Murray, S.B.; Quintana, D.S.; Loeb, K.L.; Griffiths, S.; Le Grange, D. Treatment outcomes for anorexia nervosa: A systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 2019, 49, 535–544. [Google Scholar] [CrossRef]
- Zeeck, A.; Herpertz-Dahlmann, B.; Friederich, H.C.; Brockmeyer, T.; Resmark, G.; Hagenah, U.; Ehrlich, S.; Cuntz, U.; Zipfel, S.; Hartmann, A. Psychotherapeutic Treatment for Anorexia Nervosa: A Systematic Review and Network Meta-Analysis. Front. Psychiatry 2018, 9, 158. [Google Scholar] [CrossRef]
- Miles, S.; Gnatt, I.; Phillipou, A.; Nedeljkovic, M. Cognitive flexibility in acute anorexia nervosa and after recovery: A systematic review. Clin. Psychol. Rev. 2020, 81, 101905. [Google Scholar] [CrossRef]
- Dann, K.M.; Hay, P.; Touyz, S. Are poor set-shifting and central coherence associated with everyday function in anorexia nervosa? A systematic review. J. Eat. Disord. 2021, 9, 40. [Google Scholar] [CrossRef]
- Fuglset, T.S. Is set-shifting and central coherence in anorexia nervosa influenced by body mass index, anxiety or depression? A systematic review. BMC Psychiatry 2021, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Keegan, E.; Tchanturia, K.; Wade, T.D. Central coherence and set-shifting between nonunderweight eating disorders and anorexia nervosa: A systematic review and meta-analysis. Int. J. Eat. Disord. 2020, 54, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, T.; Febry, H.; Leiteritz-Rausch, A.; Wünsch-Leiteritz, W.; Leiteritz, A.; Friederich, H.-C. Cognitive flexibility, central coherence, and quality of life in anorexia nervosa. J. Eat. Disord. 2022, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Solmi, M.; Wade, T.D.; Byrne, S.; Del Giovane, C.; Fairburn, C.G.; Ostinelli, E.G.; De Crescenzo, F.; Johnson, C.; Schmidt, U.; Treasure, J.; et al. Comparative efficacy and acceptability of psychological interventions for the treatment of adult outpatients with anorexia nervosa: A systematic review and network meta-analysis. Lancet Psychiatry 2021, 8, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Smith, M.; Wright, D. Anorexia: A literature review of young people’s experiences of hospital treatment. Nurs. Child. Young-People 2020, 33, 10–17. [Google Scholar] [CrossRef]
- Fuglset, T.S. Set-shifting, central coherence and decision-making in individuals recovered from anorexia nervosa: A systematic review. J. Eat. Disord. 2019, 7, 22. [Google Scholar] [CrossRef]
- Tenconi, E.; Collantoni, E.; Meregalli, V.; Bonello, E.; Zanetti, T.; Veronese, A.; Meneguzzo, P.; Favaro, A. Clinical and Cognitive Functioning Changes After Partial Hospitalization in Patients with Anorexia Nervosa. Front. Psychiatry 2021, 12, 653506. [Google Scholar] [CrossRef]
- Tchanturia, K.; Harrison, A.; Davies, H.; Roberts, M.; Oldershaw, A.; Nakazato, M.; Stahl, D.; Morris, R.; Schmidt, U.; Treasure, J. Cognitive Flexibility and Clinical Severity in Eating Disorders. PLoS ONE 2011, 6, e20462. [Google Scholar] [CrossRef]
- Hagan, K.E.; Christensen, K.A.; Forbush, K.T. A preliminary systematic review and meta-analysis of randomized-controlled trials of cognitive remediation therapy for anorexia nervosa. Eat. Behav. 2020, 37, 101391. [Google Scholar] [CrossRef]
- Tchanturia, K.; Giombini, L.; Leppanen, J.; Kinnaird, E. Evidence for Cognitive Remediation Therapy in Young People with Anorexia Nervosa: Systematic Review and Meta-analysis of the Literature. Eur. Eat Disord. Rev. 2017, 25, 227–236. [Google Scholar] [CrossRef]
- Tchanturia, K.; Davies, H.; Reeder, C.; Wykes, T. Cognitive Remediation Programme for Anorexia Nervosa: A Manual for Practitioners; NHS Foundation Trust: London, UK, 2008. [Google Scholar]
- Dandil, Y.; Baillie, C.; Tchanturia, K. Cognitive Remediation Therapy as a Feasible Treatment for a Young Person with Anorexia Nervosa and Autism Spectrum Disorder Comorbidity: A Case Study. Clin. Case Stud. 2019, 19, 115–132. [Google Scholar] [CrossRef]
- Herbrich-Bowe, L.; Bentz, L.K.; Correll, C.U.; Kappel, V.; van Noort, B.M. Randomized controlled trial of cognitive remediation therapy in adolescent inpatients with anorexia nervosa: Neuropsychological outcomes. Eur. Eat. Disord. Rev. 2022, 30, 772–786. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, T.; Schmidt, H.; Leiteritz-Rausch, A.; Zimmermann, J.; Wünsch-Leiteritz, W.; Leiteritz, A.; Friederich, H.-C. Cognitive remediation therapy in anorexia nervosa—A randomized clinical trial. J. Consult. Clin. Psychol. 2021, 89, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Sproch, L.E.; Anderson, K.P.; Sherman, M.F.; Crawford, S.F.; Brandt, H.A. A randomized controlled trial of group cognitive remediation therapy for anorexia nervosa: Effects on set-shifting tasks for inpatient adults and adolescents. Int. J. Eat. Disord. 2019, 52, 1004–1014. [Google Scholar] [CrossRef]
- Alvarado-Sánchez, N.; Alvarez-Rayón, G.; Mancilla-Díaz, J.M. Cognitive remediation therapy in Mexico as a treatment for Anorexia Nervosa: A case study. Eat. Disord. 2019, 27, 230–252. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.; Stavri, P.; Ormond, L.; McEnemy, F.; Akyol, D.; Qureshi, A.; Al-Khairulla, H. Cognitive remediation therapy for adolescent inpatients with severe and complex anorexia nervosa: A treatment trial. Eur. Eat. Disord. Rev. 2018, 26, 230–240. [Google Scholar] [CrossRef]
- Giombini, L.; Moynihan, J.; Turco, M.; Nesbitt, S. Evaluation of individual cognitive remediation therapy (CRT) for the treatment of young people with anorexia nervosa. Eat. Weight Disord. 2017, 22, 667–673. [Google Scholar] [CrossRef]
- Tchanturia, K.; Larsson, E.; Brown, A. Benefits of group cognitive remediation therapy in anorexia nervosa: Case series. Neuropsychiatrie 2016, 30, 42–49. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; A Akl, E.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar]
- Kung, J.; Chiappelli, F.; Cajulis, O.O.; Avezova, R.; Kossan, G.; Chew, L.; Maida, C.A. From Systematic Reviews to Clinical Recommendations for Evidence-Based Health Care: Validation of Revised Assessment of Multiple Systematic Reviews (R-AMSTAR) for Grading of Clinical Relevance. Open Dent. J. 2010, 4, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Bahk, Y.-C.; Oh, H.; Lee, W.-H.; Lee, J.-S.; Choi, K.-H. Current Status of Cognitive Remediation for Psychiatric Disorders: A Review. Front. Psychiatry 2018, 9, 461. [Google Scholar] [CrossRef] [PubMed]
- Tchanturia, K.; Lounes, N.; Holttum, S. Cognitive Remediation in Anorexia Nervosa and Related Conditions: A Systematic Review. Eur. Eat. Disord. Rev. 2014, 22, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Lindvall Dahlgren, C.; Ro, O. A systematic review of cognitive remediation therapy for anorexia nervosa—Development, current state and implications for future research and clinical practice. J. Eat Disord. 2014, 2, 26. [Google Scholar] [CrossRef] [PubMed]
- Sorgente, A.; Pietrabissa, G.; Manzoni, G.M.; Re, F.; Simpson, S.; Perona, S.; Rossi, A.; Cattivelli, R.; Innamorati, M.; Jackson, J.B.; et al. Web-Based Interventions for Weight Loss or Weight Loss Maintenance in Overweight and Obese People: A Systematic Review of Systematic Reviews. J. Med. Internet Res. 2017, 19, e229. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, T.; Ingenerf, K.; Walther, S.; Wild, B.; Hartmann, M.; Herzog, W.; Bents, H.; Friederich, H. Training cognitive flexibility in patients with anorexia nervosa: A pilot randomized controlled trial of cognitive remediation therapy. Int. J. Eat. Disord. 2013, 47, 24–31. [Google Scholar] [CrossRef]
- Dingemans, A.E.; Danner, U.N.; Donker, J.M.; Aardoom, J.J.; Van Meer, F.; Tobias, K.; Van Elburg, A.A.; Van Furth, E.F. The effectiveness of cognitive remediation therapy in patients with a severe or enduring eating disorder: A randomized controlled trial. Psychother. Psychosom. 2014, 83, 29–36. [Google Scholar] [CrossRef]
- Herbrich, L.; van Noort, B.; Pfeiffer, E.; Lehmkuhl, U.; Winter, S.; Kappel, V. Follow-up Assessment of Cognitive Remediation Therapy in Adolescent Anorexia Nervosa: A Pilot Study. Eur. Eat. Disord. Rev. 2017, 25, 104–113. [Google Scholar] [CrossRef]
- Lock, J.; Agras, W.S.; Fitzpatrick, K.K.; Bryson, S.W.; Jo, B.; Tchanturia, K. Is outpatient cognitive remediation therapy feasible to use in randomized clinical trials for anorexia nervosa? Int. J. Eat. Disord. 2013, 46, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, N.; Dimmer, M.; Power, E.; Eisler, I.; Simic, M.; Tchanturia, K. Evaluation of a Cognitive Remediation Therapy Group for Adolescents with Anorexia Nervosa: Pilot Study. Eur. Eat. Disord. Rev. 2012, 20, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Steinglass, J.E.; Albano, A.M.; Simpson, H.B.; Wang, Y.; Zou, J.; Attia, E.; Walsh, B.T. Confronting fear using exposure and response prevention for anorexia nervosa: A randomized controlled pilot study. Int. J. Eat Disord. 2014, 47, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, C.L.; Lask, B.; Landrø, N.I.; Rø, Ø. Neuropsychological functioning in adolescents with anorexia nervosa before and after cognitive remediation therapy: A feasibility trial. Int. J. Eat Disord. 2013, 46, 576–581. [Google Scholar] [CrossRef] [PubMed]
- van Noort, B.M.; Pfeiffer, E.; Lehmkuhl, U.; Kappel, V. Cognitive Remediation Therapy for Children with Anorexia Nervosa. Z. Kinder Jugendpsychiatr Psychother. 2015, 43, 351–355. [Google Scholar] [CrossRef]
- Asch, M.; Esteves, J.; De Hautecloque, D.; Bargiacchi, A.; Le Heuzey, M.F.; Mouren, M.C.; Doyen, C. Cognitive remediation therapy for children and adolescents with anorexia nervosa in France: An exploratory study. Encephale 2014, 40, 240–246. [Google Scholar] [CrossRef]
- Wood, L.; Al-Khairulla, H.; Lask, B. Group cognitive remediation therapy for adolescents with anorexia nervosa. Clin. Child Psychol. Psychiatry 2011, 16, 225–231. [Google Scholar] [CrossRef]
- Zuchova, S.; Erler, T.; Papezova, H. Group cognitive remediation therapy for adult anorexia nervosa inpatients: First experiences. Eat. Weight Disord. 2013, 18, 269–273. [Google Scholar] [CrossRef]
- Whitney, J.; Easter, A.; Tchanturia, K. Service users’ feedback on cognitive training in the treatment of anorexia nervosa: A qualitative study. Int. J. Eat. Disord. 2008, 41, 542–550. [Google Scholar] [CrossRef]
- Easter, A.; Tchanturia, K. Therapists’ experiences of Cognitive Remediation Therapy for anorexia nervosa: Implications for working with adolescents. Clin. Child Psychol. Psychiatry 2011, 16, 233–246. [Google Scholar] [CrossRef]
- Abbate-Daga, G.; Buzzichelli, S.; Marzola, E.; Amianto, F.; Fassino, S. Effectiveness of cognitive remediation therapy (CRT) in anorexia nervosa: A case series. J. Clin. Exp. Neuropsychol. 2012, 34, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Tchanturia, K.; Davies, H.; Lopez, C.; Schmidt, U.; Treasure, J.; Wykes, T. Letter to the Editor: Neuropsychological task performance before and after cognitive remediation in anorexia nervosa: A pilot case-series. Psychol. Med. 2008, 38, 1371–1373. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, C.L.; Lask, B.; Landrø, N.I.; Rø, Ø. Developing and evaluating cognitive remediation therapy (CRT) for adolescents with anorexia nervosa: A feasibility study. Clin. Child Psychol. Psychiatry 2013, 19, 476–487. [Google Scholar] [CrossRef]
- Pitt, S.; Lewis, R.; Morgan, S.; Woodward, D. Cognitive remediation therapy in an outpatient setting: A case series. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2010, 15, e281–e286. [Google Scholar] [CrossRef] [PubMed]
- Tchanturia, K.; Davies, H.; Campbell, I.C. Cognitive remediation therapy for patients with anorexia nervosa: Preliminary findings. Ann. Gen. Psychiatry 2007, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Genders, R.; Tchanturia, K. Cognitive Remediation Therapy (CRT) for anorexia in group format: A pilot study. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2010, 15, e234–e239. [Google Scholar] [CrossRef]
- Lock, J.; Fitzpatrick, K.K.; Agras, W.S.; Weinbach, N.; Jo, B. Feasibility study combining art therapy or cognitive remediation therapy with family-based treatment for adolescent anorexia nervosa. Eur. Eat. Disord. Rev. 2018, 26, 62–68. [Google Scholar] [CrossRef]
- Giombini, L.; Nesbitt, S.; Waples, L.; Finazzi, E.; Easter, A.; Tchanturia, K. Young people’s experience of individual cognitive remediation therapy (CRT) in an inpatient eating disorder service: A qualitative study. Eat. Weight Disord. 2018, 23, 499–505. [Google Scholar] [CrossRef]
- van Passel, B.; Danner, U.N.; Dingemans, A.E.; Aarts, E.; Sternheim, L.C.; Becker, E.S.; van Elburg, A.A.; van Furth, E.F.; Hendriks, G.J.; Cath, D.C. Cognitive Remediation Therapy Does Not Enhance Treatment Effect in Obsessive-Compulsive Disorder and Anorexia Nervosa: A Randomized Controlled Trial. Psychother. Psychosom. 2020, 89, 228–241. [Google Scholar] [CrossRef]
- Lask, B.; Roberts, A. Family cognitive remediation therapy for anorexia nervosa. Clin. Child Psychol. Psychiatry 2013, 20, 207–217. [Google Scholar] [CrossRef]
- Davies, H.; Tchanturia, K. Cognitive remediation therapy as an intervention for acute anorexia nervosa: A case report. Eur. Eat. Disord. Rev. 2005, 13, 311–316. [Google Scholar] [CrossRef]
- Pretorius, N.; Tchanturia, K. Anorexia nervosa: How people think and how we address it in cognitive remediation therapy. Therapy 2007, 4, 423–432. [Google Scholar] [CrossRef]
- Tchanturia, K.; Whitney, J.; Treasure, J. Can cognitive exercises help treat anorexia nervosa? Eat. Weight. Disord. 2006, 11, e112–e116. [Google Scholar] [CrossRef] [PubMed]
- van Noort, B.M.; Kraus, M.K.A.; Pfeiffer, E.; Lehmkuhl, U.; Kappel, V. Neuropsychological and behavioural short-term effects of cognitive remediation therapy in adolescent anorexia nervosa: A pilot study. Eur. Eat. Disord. Rev. 2016, 24, 69–74. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).