
Non-Invasive Monitoring of Cerebral Edema Using Ultrasonic Echo Signal Features and Machine Learning



Abstract
1. Introduction
2. Literature Review
2.1. Research Related to Cerebral Edema Monitoring
2.2. Research Related to Ultrasonic Echo Features and Machine Learning
3. Materials and Methods
3.1. Experimental Animals and Grouping
3.2. Cerebral Ischemia Model
3.3. Assessment of Neurological Deficits
3.4. Analysis of Cerebral Infarction Volume
3.5. Assessment of Histology
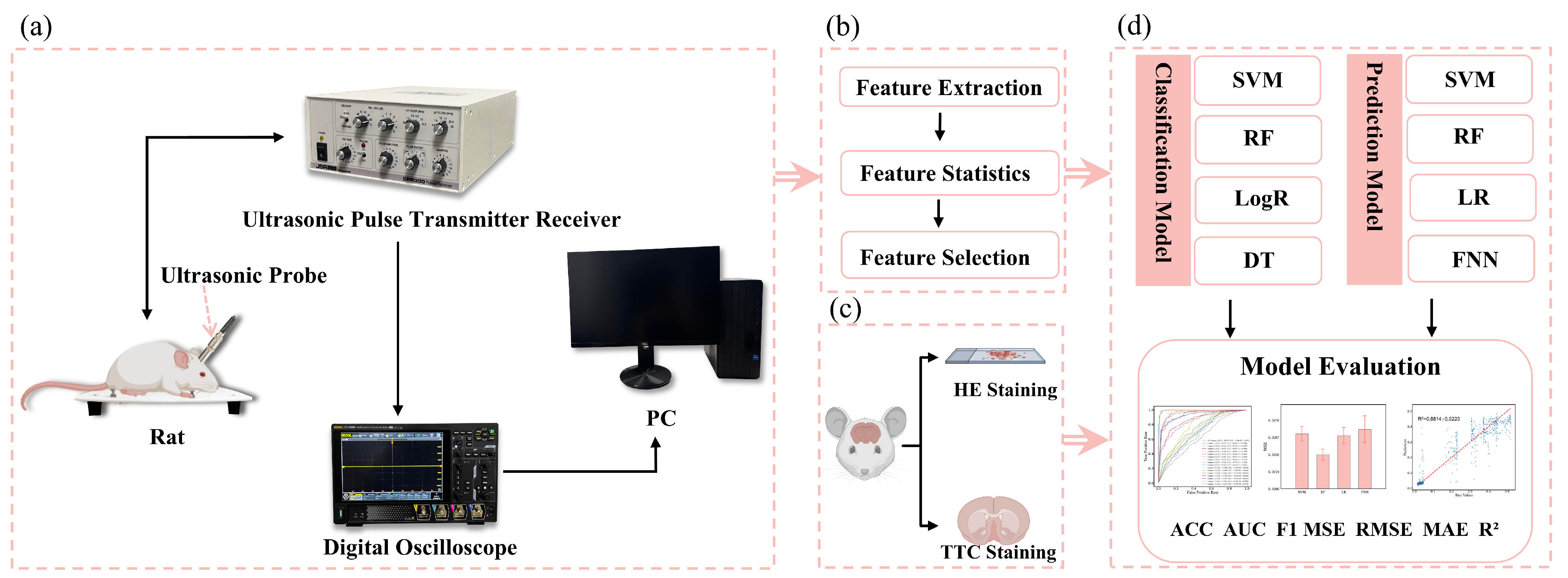
3.6. Ultrasonic Echo Signal Acquisition
3.7. Feature Parameter Extraction
3.8. Classification of Cerebral Edema and Model Evaluation
3.9. Prediction of Cerebral Infarction Volume Ratio and Model Evaluation
3.10. Statistical Analysis
4. Results
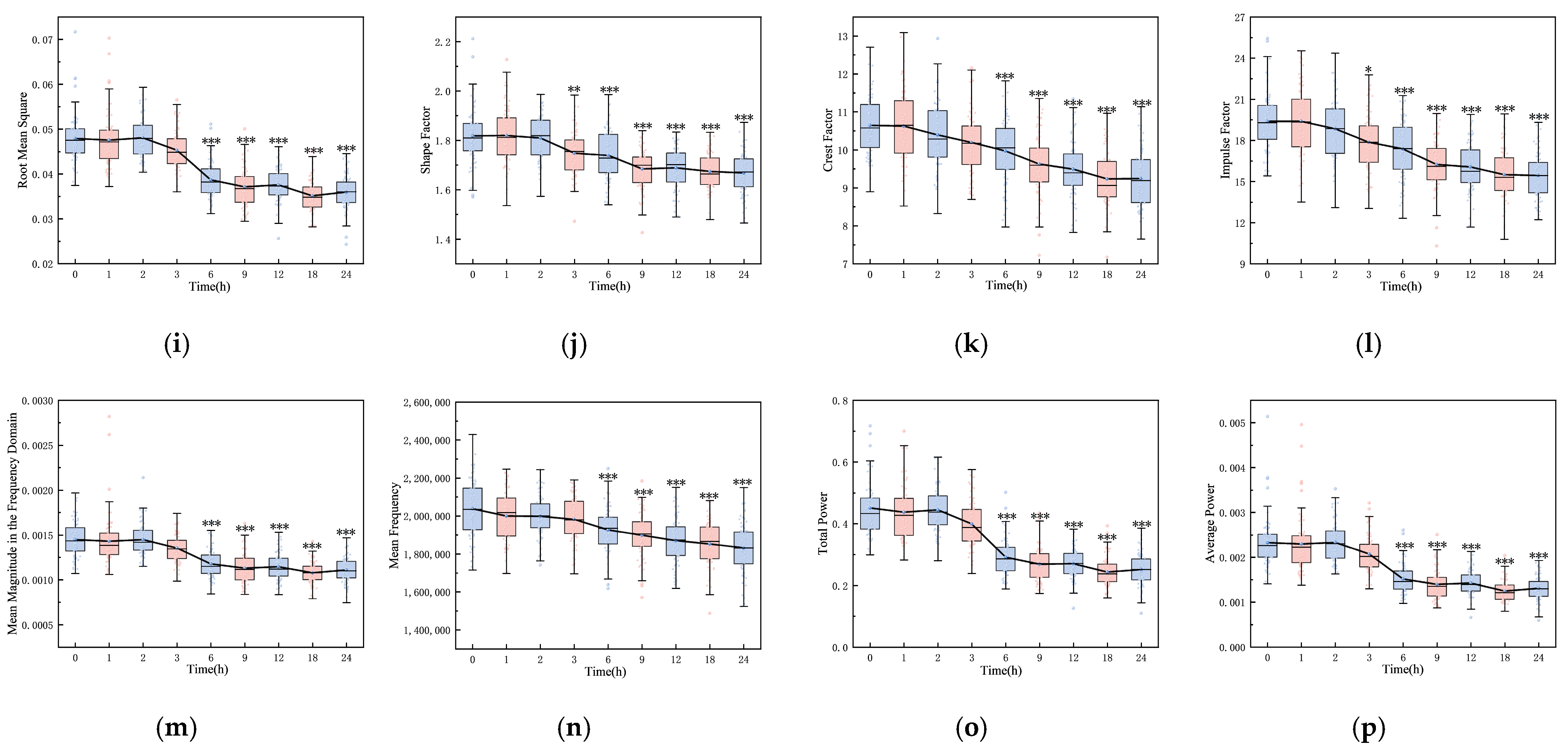
4.1. Changes to Features over Time
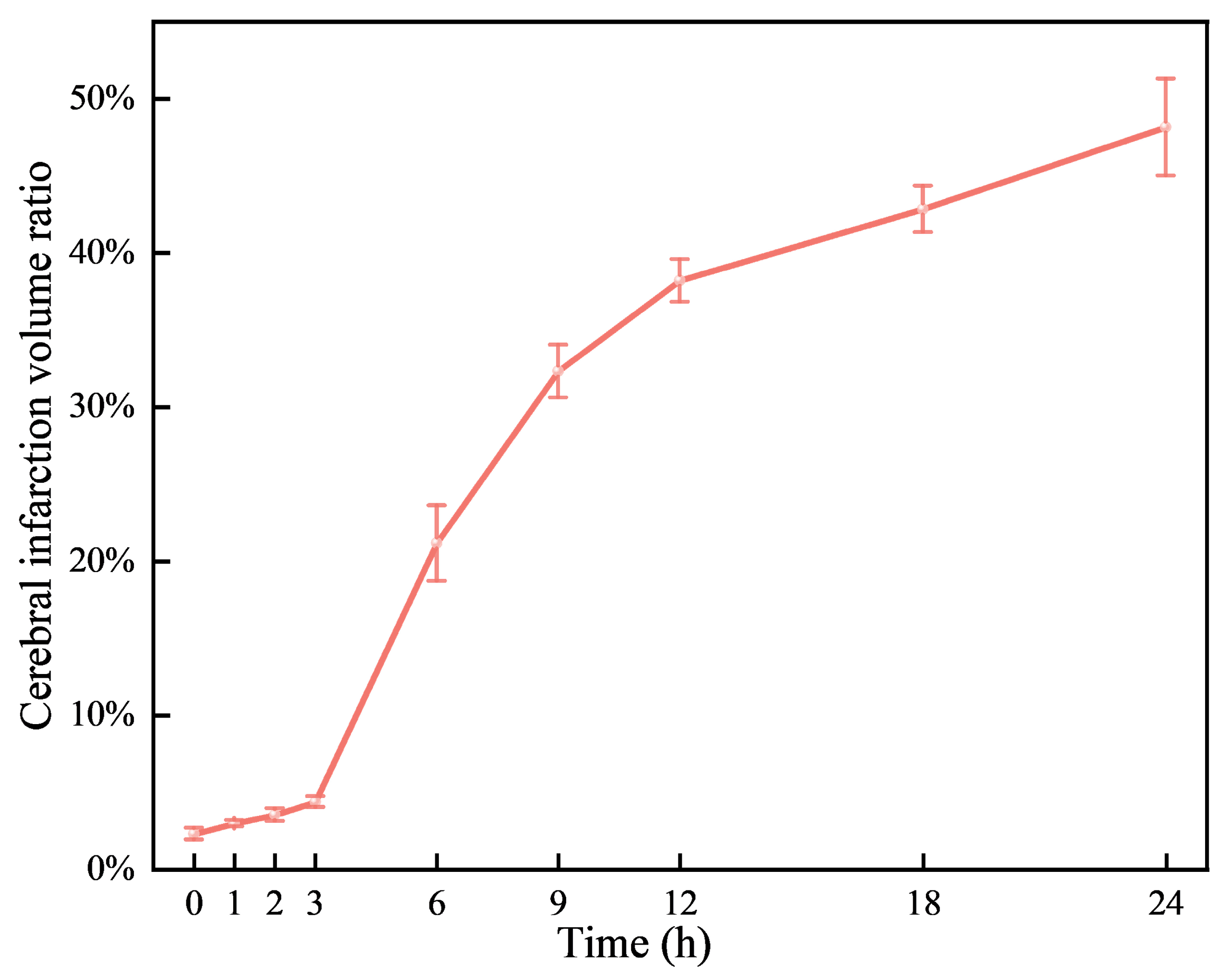
4.2. Volume Ratio of Cerebral Infarction over Time
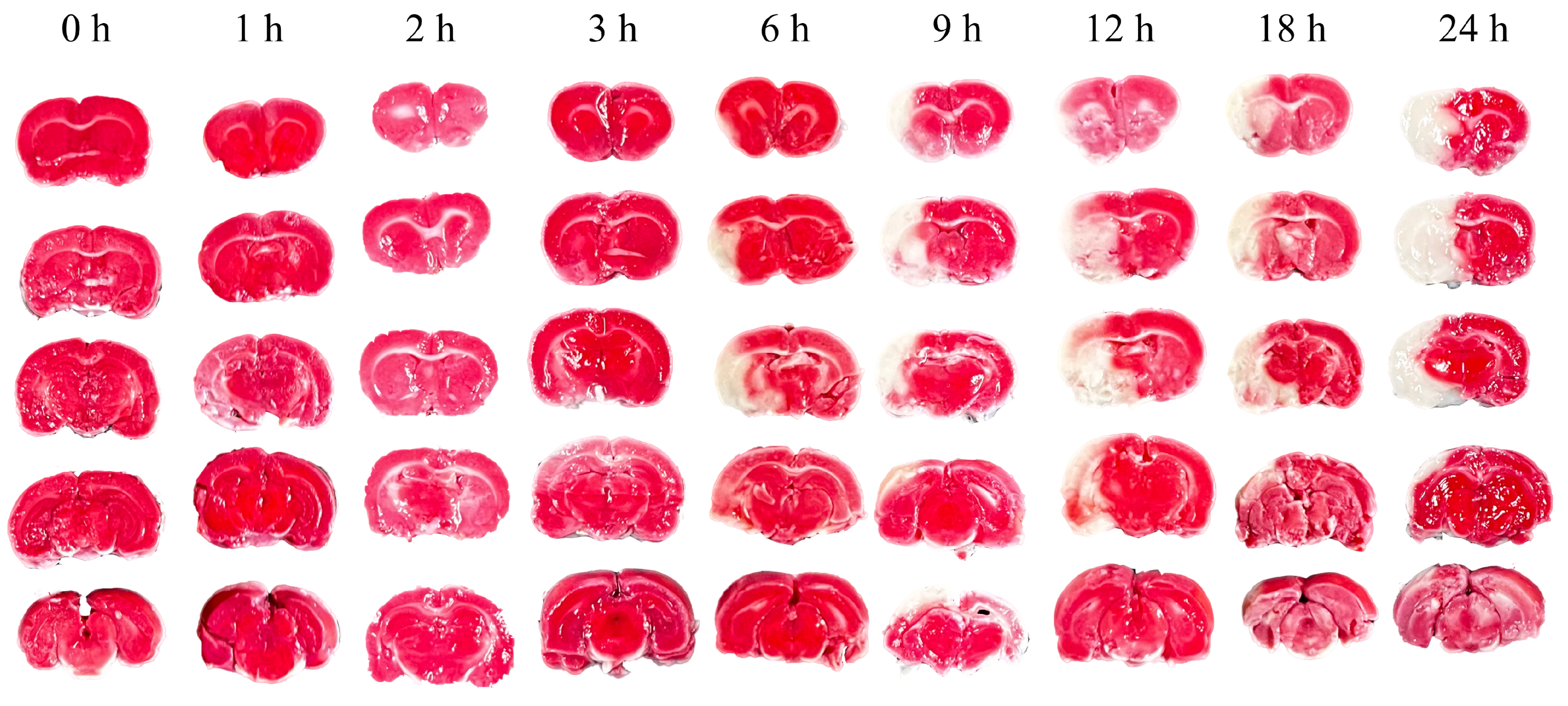
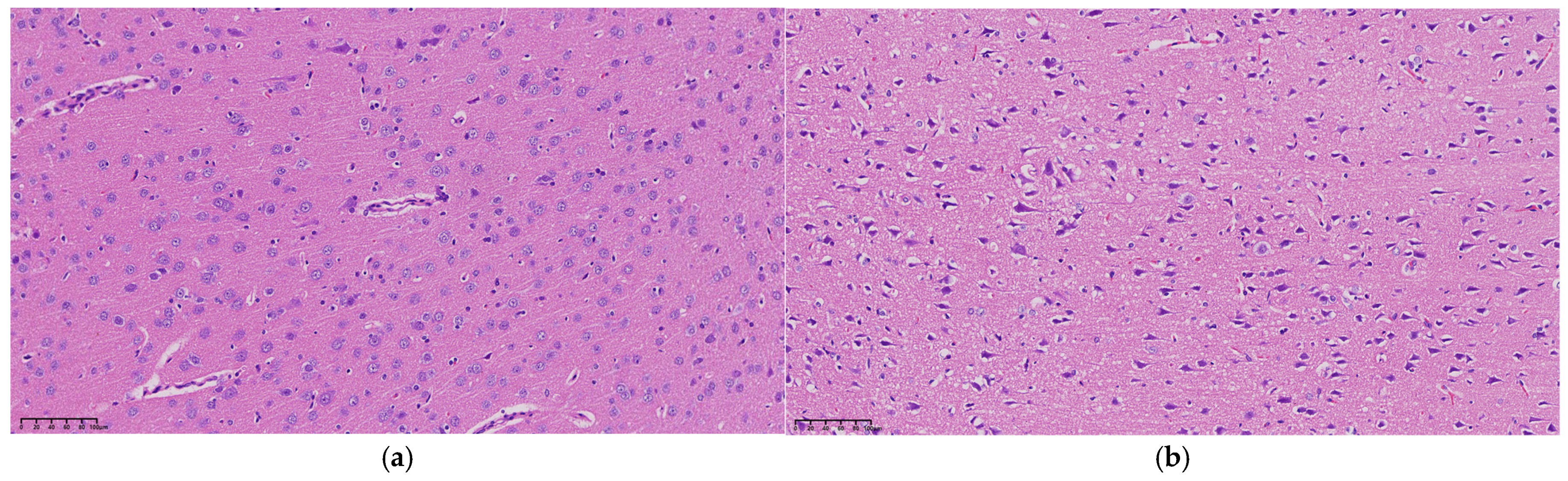
4.3. Pathological Morphology at Different Times
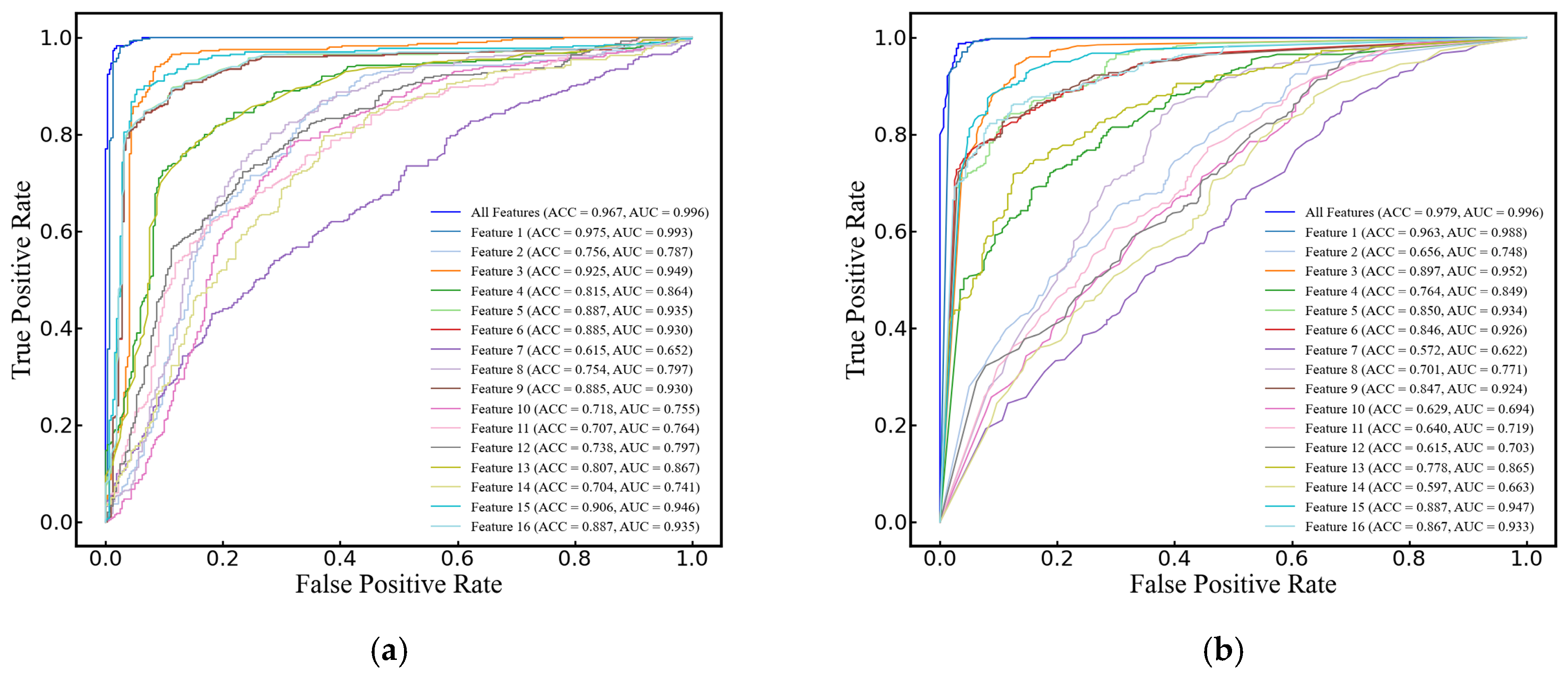
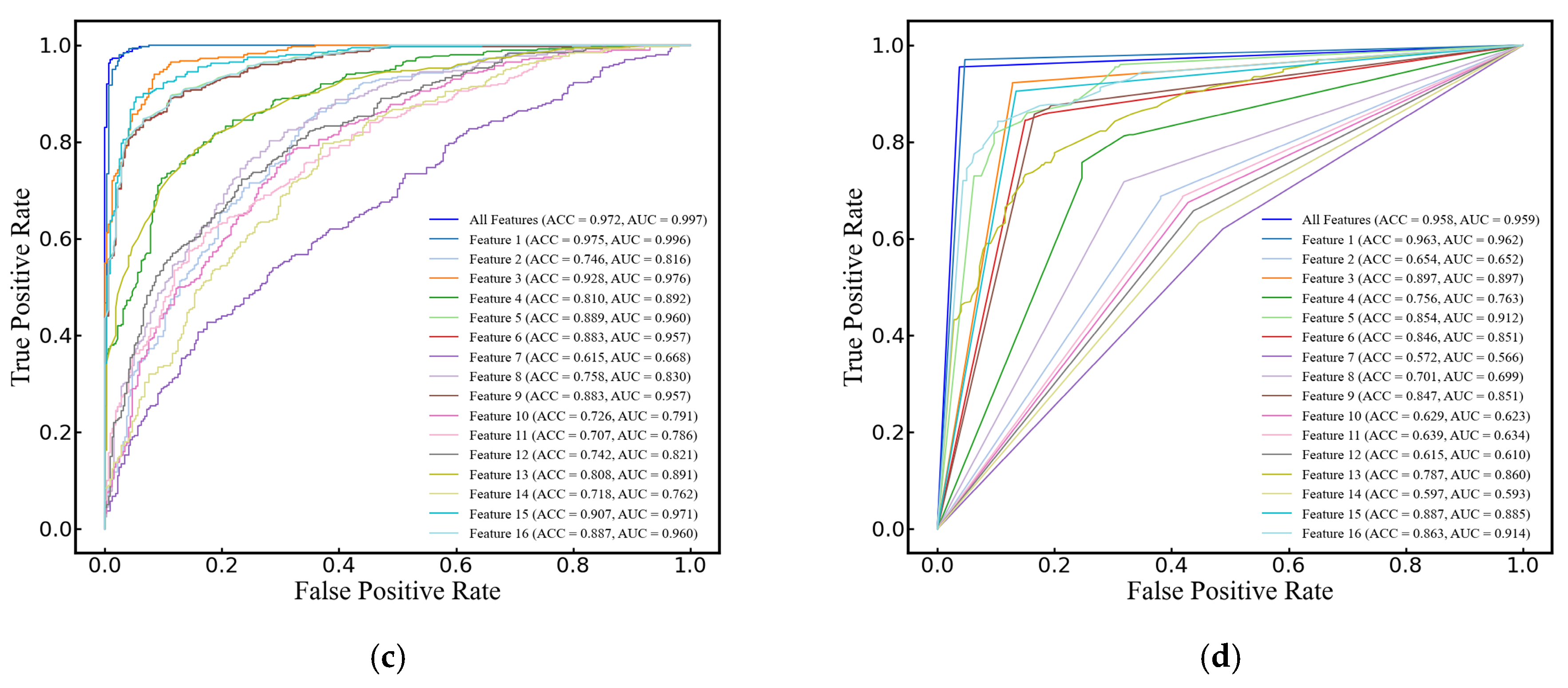
4.4. Cerebral Edema Classification
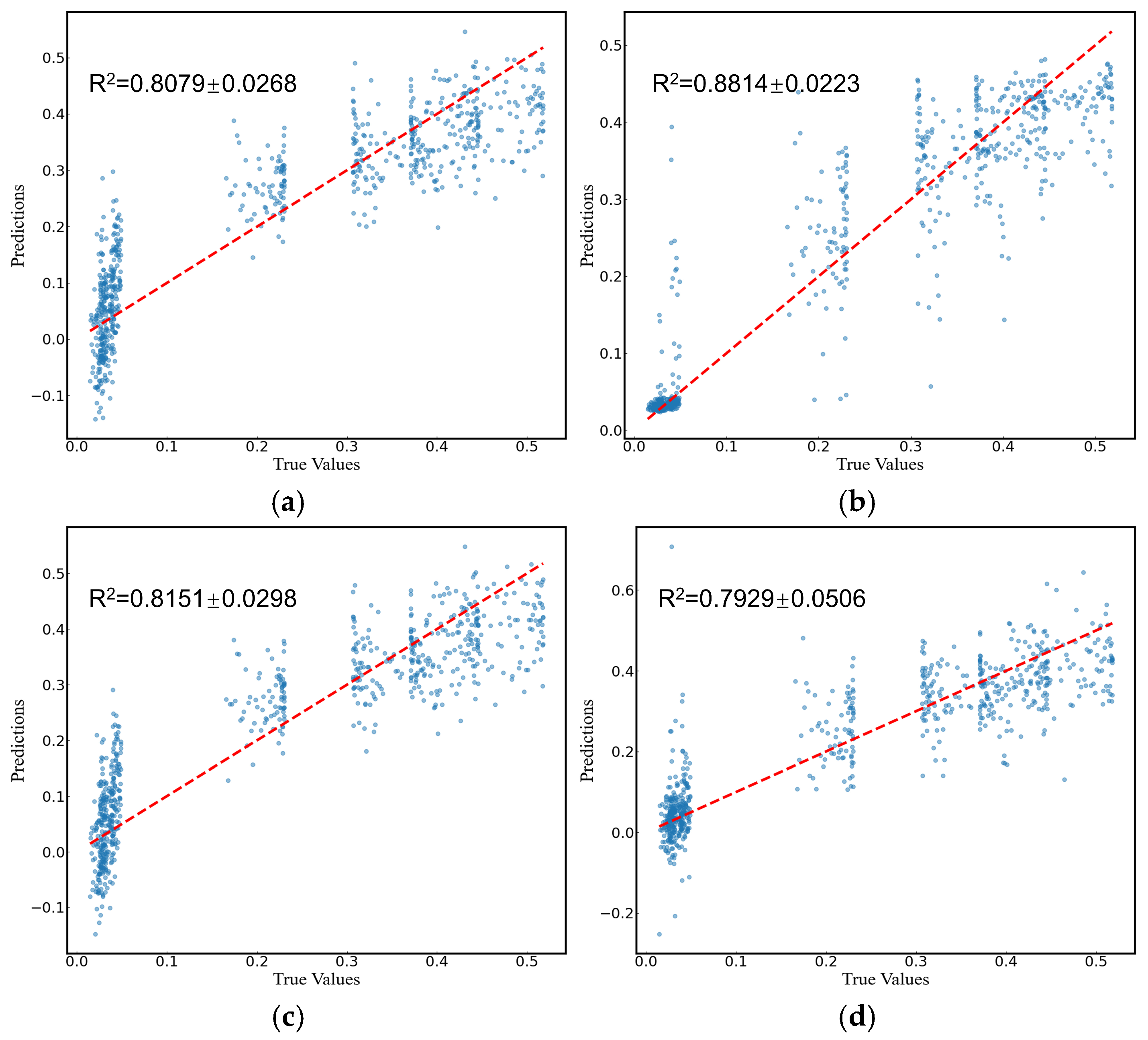
4.5. Prediction of Cerebral Infarction Volume Ratio
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liotta, E.M. Management of cerebral edema, brain compression, and intracranial pressure. CONTINUUM Lifelong Learn. Neurol. 2021, 27, 1172–1200. [Google Scholar] [CrossRef]
- Stocchetti, N.; Maas, A.I. Traumatic intracranial hypertension. N. Engl. J. Med. 2014, 370, 2121–2130. [Google Scholar] [CrossRef]
- Han, W.; Song, Y.; Rocha, M.; Shi, Y. Ischemic brain edema: Emerging cellular mechanisms and therapeutic approaches. Neurobiol. Dis 2023, 178, 106029. [Google Scholar] [CrossRef] [PubMed]
- Stokum, J.A.; Gerzanich, V.; Simard, J.M. Molecular pathophysiology of cerebral edema. J. Cereb. Blood Flow Metab. 2016, 36, 513–538. [Google Scholar] [CrossRef] [PubMed]
- Sulhan, S.; Lyon, K.A.; Shapiro, L.A.; Huang, J.H. Neuroinflammation and blood–brain barrier disruption following traumatic brain injury: Pathophysiology and potential therapeutic targets. J. Neurosci. Res. 2020, 98, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Jha, R.M.; Kochanek, P.M.; Simard, J.M. Pathophysiology and treatment of cerebral edema in traumatic brain injury. Neuropharmacology 2019, 145, 230–246. [Google Scholar] [CrossRef]
- Hawryluk, G.W.; Citerio, G.; Hutchinson, P.; Kolias, A.; Meyfroidt, G.; Robba, C.; Stocchetti, N.; Chesnut, R. Intracranial pressure: Current perspectives on physiology and monitoring. Intensive Care Med. 2022, 48, 1471–1481. [Google Scholar] [CrossRef]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N. Guidelines for the management of severe traumatic brain injury. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef]
- Lietke, S.; Zausinger, S.; Patzig, M.; Holtmanspötter, M.; Kunz, M. CT-Based Classification of Acute Cerebral Edema: Association with Intracranial Pressure and Outcome. J. Neuroimaging 2020, 30, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Wang, L.; Xu, C.; Li, L.; Gao, G.; Dong, X. Real-time imaging of subarachnoid hemorrhage in piglets with electrical impedance tomography. Physiol. Meas. 2010, 31, 1229. [Google Scholar] [CrossRef]
- Hackett, P.; Yarnell, P.; Weiland, D.; Reynard, K. Acute and evolving MRI of high-altitude cerebral edema: Microbleeds, edema, and pathophysiology. Am. J. Neuroradiol. 2019, 40, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Thiagarajah, J.R.; Papadopoulos, M.C.; Verkman, A. Noninvasive early detection of brain edema in mice by near-infrared light scattering. J. Neurosci. Res. 2005, 80, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.-L.; Jin, G.; Bai, Z.-L.; Chen, J.-B.; Li, M.-W.; Li, G.; Zhuang, W.; Liu, Y.-N.; Qin, M.-X. Twenty-four-hour real-time continuous monitoring of acute focal cerebral ischemia in rabbits based on magnetic inductive phase shift. BioMed. Eng. OnLine 2020, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Goffi, A.; Geeraerts, T.; Cardim, D.; Via, G.; Czosnyka, M.; Park, S.; Sarwal, A.; Padayachy, L.; Rasulo, F. Brain ultrasonography: Methodology, basic and advanced principles and clinical applications. A narrative review. Intensive Care Med. 2019, 45, 913–927. [Google Scholar] [CrossRef]
- Maurer, M.; Shambal, S.; Berg, D.; Woydt, M.; Hofmann, E.; Georgiadis, D.; Lindner, A.; Becker, G. Differentiation between intracerebral hemorrhage and ischemic stroke by transcranial color-coded duplex-sonography. Stroke 1998, 29, 2563–2567. [Google Scholar] [CrossRef]
- Motuel, J.; Biette, I.; Srairi, M.; Mrozek, S.; Kurrek, M.M.; Chaynes, P.; Cognard, C.; Fourcade, O.; Geeraerts, T. Assessment of brain midline shift using sonography in neurosurgical ICU patients. Crit. Care 2014, 18, 676. [Google Scholar] [CrossRef]
- Bowler, A.L.; Pound, M.P.; Watson, N.J. A review of ultrasonic sensing and machine learning methods to monitor industrial processes. Ultrasonics 2022, 124, 106776. [Google Scholar] [CrossRef]
- Wang, X.; Guan, S.; Hua, L.; Wang, B.; He, X. Classification of spot-welded joint strength using ultrasonic signal time-frequency features and PSO-SVM method. Ultrasonics 2019, 91, 161–169. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, X. Research on laser ultrasonic surface defect identification based on a support vector machine. Sci. Prog. 2021, 104, 00368504211059038. [Google Scholar] [CrossRef]
- Moradi, M.; Mousavi, P.; Siemens, D.; Sauerbrei, E.; Isotalo, P.; Boag, A.; Abolmaesumi, P. Discrete Fourier analysis of ultrasound RF time series for detection of prostate cancer. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 1339–1342. [Google Scholar]
- Liao, Z.; Zhang, Y.; Li, Z.; He, B.; Lang, X.; Liang, H.; Chen, J. Classification of red blood cell aggregation using empirical wavelet transform analysis of ultrasonic radiofrequency echo signals. Ultrasonics 2021, 114, 106419. [Google Scholar] [CrossRef]
- Uniyal, N.; Eskandari, H.; Abolmaesumi, P.; Sojoudi, S.; Gordon, P.; Warren, L.; Rohling, R.N.; Salcudean, S.E.; Moradi, M. Ultrasound RF time series for classification of breast lesions. IEEE Trans. Med. Imaging 2014, 34, 652–661. [Google Scholar] [CrossRef]
- Mörlein, D.; Rosner, F.; Brand, S.; Jenderka, K.-V.; Wicke, M. Non-destructive estimation of the intramuscular fat content of the longissimus muscle of pigs by means of spectral analysis of ultrasound echo signals. Meat Sci. 2005, 69, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Schmid-Elsaesser, R.; Zausinger, S.; Hungerhuber, E.; Baethmann, A.; Reulen, H.-J. A critical reevaluation of the intraluminal thread model of focal cerebral ischemia: Evidence of inadvertent premature reperfusion and subarachnoid hemorrhage in rats by laser-Doppler flowmetry. Stroke 1998, 29, 2162–2170. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, J. Experimental studies of ischemic brain edema. 1. A new experimental model of cerebral embolism in rats in which recirculation can be introduced in the ischemic area. Jpn. J. Stroke 1986, 8, 1–8. [Google Scholar] [CrossRef]
- Longa, E.Z.; Weinstein, P.R.; Carlson, S.; Cummins, R. Reversible middle cerebral artery occlusion without craniectomy in rats. stroke 1989, 20, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Swanson, R.A.; Morton, M.T.; Tsao-Wu, G.; Savalos, R.A.; Davidson, C.; Sharp, F.R. A semiautomated method for measuring brain infarct volume. J. Cereb. Blood Flow Metab. 1990, 10, 290–293. [Google Scholar] [CrossRef]
- Al Shalabi, L.; Shaaban, Z.; Kasasbeh, B. Data mining: A preprocessing engine. J. Comput. Sci. 2006, 2, 735–739. [Google Scholar] [CrossRef]
- Kreft, B.; Tzschätzsch, H.; Shahryari, M.; Haffner, P.; Braun, J.; Sack, I.; Streitberger, K.-J. Noninvasive Detection of Intracranial Hypertension by Novel Ultrasound Time-Harmonic Elastography. Investig. Radiol. 2022, 57, 77–84. [Google Scholar] [CrossRef]
- Zhou, S.; Gao, X.; Park, G.; Yang, X.; Qi, B.; Lin, M.; Huang, H.; Bian, Y.; Hu, H.; Chen, X. Transcranial volumetric imaging using a conformal ultrasound patch. Nature 2024, 629, 810–818. [Google Scholar] [CrossRef]
- Winkler, E.A.; Minter, D.; Yue, J.K.; Manley, G.T. Cerebral edema in traumatic brain injury: Pathophysiology and prospective therapeutic targets. Neurosurg. Clin. 2016, 27, 473–488. [Google Scholar] [CrossRef]
- Zhu, L.; He, W.; Wu, J. Experimental Study of the Influence of Elastic Medium Deformation on Ultrasonic Propagation Characteristics. J. Exp. Mech. 2014, 29, 26–32. [Google Scholar]
- Fadhel, M.N.; Berndl, E.S.; Strohm, E.M.; Kolios, M.C. High-frequency acoustic impedance imaging of cancer cells. Ultrasound Med. Biol. 2015, 41, 2700–2713. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Yoshida, K.; Maruyama, H.; Mamou, J.; Yamaguchi, T. Acoustic impedance analysis with high-frequency ultrasound for identification of fatty acid species in the liver. Ultrasound Med. Biol. 2017, 43, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Yi, Y.; Meng, Y.; Lv, G.; Jiang, X.; Wu, Y.; Yang, W.; Yao, Y.; Xu, H.; Bu, W. Self-enhanced acoustic impedance difference strategy for detecting the acidic tumor microenvironment. ACS Nano 2022, 16, 4217–4227. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Chen, R.; Yang, L.; Zhang, G.; Li, W.; Zhao, Z.; Xu, C.; Dong, X.; Fu, F. Electrical impedance changes at different phases of cerebral edema in rats with ischemic brain injury. BioMed Res. Int. 2018, 2018, 9765174. [Google Scholar] [CrossRef]
- Chen, J.; Li, G.; Liang, H.; Zhao, S.; Sun, J.; Qin, M. An amplitude-based characteristic parameter extraction algorithm for cerebral edema detection based on electromagnetic induction. BioMed Eng. OnLine 2021, 20, 74. [Google Scholar] [CrossRef]
- Zhang, Y.; Qi, X.; Li, W.; Wan, M.; Ning, X.; Hu, J. Research on the classification of early-stage brain edema by combining intrinsic optical signal imaging and laser speckle contrast imaging. J. Biophotonics 2024, 17, e202300394. [Google Scholar] [CrossRef]
- Kuts, R.; Frank, D.; Gruenbaum, B.F.; Grinshpun, J.; Melamed, I.; Knyazer, B.; Tarabrin, O.; Zvenigorodsky, V.; Shelef, I.; Zlotnik, A. A novel method for assessing cerebral edema, infarcted zone and blood-brain barrier breakdown in a single post-stroke rodent brain. Front. Neurosci. 2019, 13, 1105. [Google Scholar] [CrossRef]
- Shigeno, T.; Brock, M.; Shigeno, S.; Fritschka, E.; Cervós-Navarro, J. The determination of brain water content: Microgravimetry versus drying-weighing method. J. Neurosurg. 1982, 57, 99–107. [Google Scholar] [CrossRef]
- Keep, R.F.; Hua, Y.; Xi, G. Brain water content: A misunderstood measurement? Transl. Stroke Res. 2012, 3, 263–265. [Google Scholar] [CrossRef]
- Chadha, G.S.; Panambilly, A.; Schwung, A.; Ding, S.X. Bidirectional deep recurrent neural networks for process fault classification. ISA Trans. 2020, 106, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Quddus, A.; Zandi, A.S.; Prest, L.; Comeau, F.J. Using long short term memory and convolutional neural networks for driver drowsiness detection. Accid. Anal. Prev. 2021, 156, 106107. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Formula | Feature | Formula |
|---|---|---|---|
| Maximum | Impulse factor | ||
| Minimum | Crest factor | ||
| Mean | Mean magnitude in the frequency domain | ||
| Peak-to-Peak | Centroid frequency | ||
| Average | Mean squared frequency | ||
| Variance | Variance frequency | ||
| Standard deviation | Frequency variance | ||
| Kurtosis | Mean frequency | ||
| Skewness | Total power | ||
| Root mean square | Average power | ||
| Shape factor | Peak frequency |
| Model | ACC | AUC | F1 |
|---|---|---|---|
| SVM | 0.967 ± 0.034 | 0.996 ± 0.007 | 0.971 ± 0.029 |
| RF | 0.979 ± 0.019 | 0.996 ± 0.005 | 0.982 ± 0.017 |
| LogR | 0.972 ± 0.030 | 0.997 ± 0.005 | 0.975 ± 0.026 |
| DT | 0.958 ± 0.021 | 0.959 ± 0.022 | 0.962 ± 0.018 |
| Model | MSE | RMSE | MAE | R2 |
|---|---|---|---|---|
| SVM | 0.0061 ± 0.0008 | 0.0782 ± 0.0048 | 0.0632 ± 0.0054 | 0.8079 ± 0.0268 |
| RF | 0.0038 ± 0.0006 | 0.0612 ± 0.0046 | 0.0379 ± 0.0035 | 0.8814 ± 0.0223 |
| LR | 0.0059 ± 0.0009 | 0.0766 ± 0.0056 | 0.0616 ± 0.0056 | 0.8151 ± 0.0298 |
| FNN | 0.0066 ± 0.0015 | 0.0808 ± 0.0091 | 0.0577 ± 0.0066 | 0.7929 ± 0.0506 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.; Yang, Y.; Zhou, Y. Non-Invasive Monitoring of Cerebral Edema Using Ultrasonic Echo Signal Features and Machine Learning. Brain Sci. 2024, 14, 1175. https://doi.org/10.3390/brainsci14121175
Yang S, Yang Y, Zhou Y. Non-Invasive Monitoring of Cerebral Edema Using Ultrasonic Echo Signal Features and Machine Learning. Brain Sciences. 2024; 14(12):1175. https://doi.org/10.3390/brainsci14121175
Chicago/Turabian StyleYang, Shuang, Yuanbo Yang, and Yufeng Zhou. 2024. "Non-Invasive Monitoring of Cerebral Edema Using Ultrasonic Echo Signal Features and Machine Learning" Brain Sciences 14, no. 12: 1175. https://doi.org/10.3390/brainsci14121175
APA StyleYang, S., Yang, Y., & Zhou, Y. (2024). Non-Invasive Monitoring of Cerebral Edema Using Ultrasonic Echo Signal Features and Machine Learning. Brain Sciences, 14(12), 1175. https://doi.org/10.3390/brainsci14121175