
Depression and Pseudodementia: Decoding the Intricate Bonds in an Italian Outpatient Setting


 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessment Scales
2.3. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Patients
3.2. Psychopathological and Neurocognitive Features
3.3. Correlations between Depressive and Cognitive Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiloh, L.G. Pseudo-dementia. Acta Psychiatr. Scand. 1961, 37, 336–351. [Google Scholar] [CrossRef]
- Burns, A.; Jolley, D. Pseudodementia: History, mystery and positivity. In Troublesome Disguises: Managing Challenging Disorders in Psychiatry, 2nd ed.; Bhugra, D., Malhi, G.S., Eds.; John Wiley & Sons: Oxford, UK, 2015; pp. 218–230. [Google Scholar] [CrossRef]
- Sekhon, S.; Marwaha, R. Depressive Cognitive Disorders. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Šimić, G.; Babić Leko, M.; Wray, S.; Harrington, C.R.; Delalle, I.; Jovanov-Milosevic, N.; Bažadona, D.; Buée, L.; de Silva, R.; Di Giovanni, G.; et al. Monoaminergic neuropathology in Alzheimer’s disease. Prog. Neurobiol. 2017, 151, 101–138. [Google Scholar] [CrossRef]
- Marazziti, D.; Consoli, G.; Picchetti, M.; Carlini, M.; Faravelli, L. Cognitive impairment in major depression. Eur. J. Pharmacol. 2010, 626, 83–86. [Google Scholar] [CrossRef]
- Cole, M.G.; Dendukuri, N. Risk factors for depression among elderly community subjects: A systematic review and meta-analysis. Am. J. Psychiatry 2003, 160, 1147–1156. [Google Scholar] [CrossRef]
- Weyerer, S.; Eifflaender-Gorfer, S.; Köhler, L.; Jessen, F.; Maier, W.; Fuchs, A.; Pentzek, M.; Kaduszkiewicz, H.; Bachmann, C.; Angermeyer, M.C.; et al. Prevalence and risk factors for depression in non-demented primary care attenders aged 75 years and older. J. Affect. Disord. 2008, 111, 153–163. [Google Scholar] [CrossRef]
- Hegeman, J.M.; Kok, R.M.; van der Mast, R.C.; Giltay, E.J. Phenomenology of depression in older compared with younger adults: Meta-analysis. Br. J. Psychiatry 2012, 200, 275–281. [Google Scholar] [CrossRef]
- Sözeri-Varma, G. Depression in the elderly: Clinical features and risk factors. Aging Dis. 2012, 3, 465–471. [Google Scholar]
- Hashem, A.H.; Nasreldin, M.; Gomaa, M.A.; Khalaf, O.O. Late versus early-onset depression in elderly patients: Vascular risk and cognitive impairment. Curr. Aging Sci. 2017, 10, 211–216. [Google Scholar] [CrossRef]
- Savard, R.J.; Rey, A.C.; Post, R.M. Halstead-Reitan Category Test in bipolar and unipolar affective disorders: Relationship to age and phase of illness. J. Nerv. Ment. Dis. 1980, 168, 297–304. [Google Scholar] [CrossRef]
- Mormont, C. The influence of age and depression on intellectual and memory performances. Acta Psychiatr. Belg. 1984, 84, 127–134. [Google Scholar]
- Rubinow, D.R.; Post, R.M.; Savard, R.; Gold, P.W. Cortisol hypersecretion and cognitive impairment in depression. Arch. Gen. Psychiatry 1984, 41, 279–283. [Google Scholar] [CrossRef]
- Castaneda, A.E.; Tuulio-Henriksson, A.; Marttunen, M.; Suvisaari, J.; Lönnqvist, J. A review on cognitive impairments in depressive and anxiety disorders with a focus on young adults. J. Affect. Disord. 2008, 106, 1–27. [Google Scholar] [CrossRef]
- Pisljar, M.; Pirtosek, Z.; Repovs, G.; Grgic, M. Executive dysfunction in late-onset depression. Psychiatr. Danub. 2008, 20, 231–235. [Google Scholar]
- Jarema, M.; Dudek, D.; Czernikiewicz, A. Dysfunkcje poznawcze w depresji—Niedoszacowany objaw czy nowy wymiar? [Cognitive dysfunctions in depression—Underestimated symptom or new dimension?]. Psychiatr. Pol. 2014, 48, 1105–1116. [Google Scholar] [CrossRef]
- Barch, D.M.; D’Angelo, G.; Pieper, C.; Wilkins, C.H.; Welsh-Bohmer, K.; Taylor, W.; Garcia, K.S.; Gersing, K.; Doraiswamy, P.M.; Sheline, Y.I. Cognitive improvement following treatment in late-life depression: Relationship to vascular risk and age of onset. Am. J. Geriatr. Psychiatry 2012, 20, 682–690. [Google Scholar] [CrossRef]
- Jost, B.C.; Grossberg, G.T. The evolution of psychiatric symptoms in Alzheimer’s disease: A natural history study. J. Am. Geriatr. Soc. 1996, 44, 1078–1081. [Google Scholar] [CrossRef]
- Alexopoulos, G.S.; Meyers, B.S.; Young, R.C.; Campbell, S.; Silbersweig, D.; Charlson, M. ‘Vascular depression’ hypothesis. Arch. Gen. Psychiatry 1997, 54, 915–922. [Google Scholar] [CrossRef]
- Butters, M.A.; Young, J.B.; Lopez, O.; Aizenstein, H.J.; Mulsant, B.H.; Reynolds, C.F., 3rd; DeKosky, S.T.; Becker, J.T. Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin. Neurosci. 2008, 10, 345–357. [Google Scholar] [CrossRef]
- Heser, K.; Tebarth, F.; Wiese, B.; Eisele, M.; Bickel, H.; Köhler, M.; Mösch, E.; Weyerer, S.; Werle, J.; König, H.H.; et al. Age of major depression onset, depressive symptoms, and risk for subsequent dementia: Results of the German study on Ageing, Cognition, and Dementia in primary care patients (AgeCoDe). Psychol. Med. 2013, 43, 1597–1610. [Google Scholar] [CrossRef]
- Kessing, L.V. Depression and the risk for dementia. Curr. Opin. Psychiatry 2012, 25, 457–461. [Google Scholar] [CrossRef]
- Lin, W.C.; Hu, L.Y.; Tsai, S.J.; Yang, A.C.; Shen, C.C. Depression and the risk of vascular dementia: A population-based retrospective cohort study. Int. J. Geriatr. Psychiatry 2017, 32, 556–563. [Google Scholar] [CrossRef]
- Reijnders, J.S.; Ehrt, U.; Weber, W.E.; Aarsland, D.; Leentjens, A.F. A systematic review of prevalence studies of depression in Parkinson’s disease. Mov. Disord. 2008, 23, 183–313. [Google Scholar] [CrossRef]
- Enache, D.; Winblad, B.; Aarsland, D. Depression in dementia: Epidemiology, mechanisms, and treatment. Curr. Opin. Psychiatry 2011, 24, 461–472. [Google Scholar] [CrossRef]
- Kitching, D. Depression in dementia. Aust. Prescr. 2015, 38, 209–211. [Google Scholar] [CrossRef]
- Cherbuin, N.; Kim, S.; Anstey, K.J. Dementia risk estimates associated with measures of depression: A systematic review and meta-analysis. BMJ Open 2015, 5, e008853. [Google Scholar] [CrossRef]
- Almeida, O.P.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L. Depression as a modifiable factor to decrease the risk of dementia. Transl. Psychiatry 2017, 7, e1117. [Google Scholar] [CrossRef]
- Oude Voshaar, R.C.; Dimitriadis, M.; vandenBrink, R.H.S.; Aprahamian, I.; Borges, M.K.; Marijnissen, R.M.; Hoogendijk, E.O.; Rhebergen, D.; Jeuring, H.W. A 6-year prospective clinical cohort study on the bidirectional association between frailty and depressive disorder. Int. J. Geriatr. Psychiatry 2021, 36, 1699–1707. [Google Scholar] [CrossRef]
- Mirza, S.S.; Wolters, F.J.; Swanson, S.A.; Koudstaal, P.J.; Hofman, A.; Tiemeier, H.; Ikram, M.A. 10-year trajectories of depressive symptoms and risk of dementia: A population-based study. Lancet Psychiatry 2016, 3, 628–635. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Dugravot, A.; Fournier, A.; Abell, J.; Ebmeier, K.; Kivimäki, M.; Sabia, S. Trajectories of depressive symptoms before diagnosis of dementia: A 28-year follow-up study. JAMA Psychiatry 2017, 74, 712–718. [Google Scholar] [CrossRef]
- Voros, V.; Martin Gutierrez, D.; Alvarez, F.; Boda-Jorg, A.; Kovacs, A.; Tenyi, T.; Fekete, S.; Osvath, P. The impact of depressive mood and cognitive impairment on quality of life of the elderly. Psychogeriatrics 2020, 20, 271–277. [Google Scholar] [CrossRef]
- Bonfiglio, V.; Umegaki, H.; Kuzuya, M. Quality of life in cognitively impaired older adults. Geriatr. Gerontol. Int. 2019, 19, 999–1005. [Google Scholar] [CrossRef]
- Sousa, M.F.; Santos, R.L.; Arcoverde, C.; Simões, P.; Belfort, T.; Adler, I.; Leal, C.; Dourado, M.C. Quality of life in dementia: The role of non-cognitive factors in the ratings of people with dementia and family caregivers. Int. Psychogeriat. 2013, 25, 1097–1105. [Google Scholar] [CrossRef]
- Peavy, G.M.; Salmon, D.P.; Jacobson, M.W.; Hervey, A.; Gamst, A.C.; Wolfson, T.; Patterson, T.L.; Goldman, S.; Mills, P.J.; Khandrika, S.; et al. Effects of chronic stress on memory decline in cognitively normal and mildly impaired older adults. Am. J. Psychiatry 2009, 166, 1384–1391. [Google Scholar] [CrossRef]
- Byers, A.L.; Yaffe, K. Depression and risk of developing dementia. Nat. Rev. Neurol. 2011, 7, 323–331. [Google Scholar] [CrossRef]
- Taylor, W.D.; McQuoid, D.R.; Payne, M.E.; Zannas, A.S.; MacFall, J.R.; Steffens, D.C. Hippocampus atrophy and the longitudinal course of late-life depression. Am. J. Geriatr. Psychiatry 2014, 22, 1504–1512. [Google Scholar] [CrossRef]
- Eisch, A.J.; Petrik, D. Depression and hippocampal neurogenesis: A road to remission? Science 2012, 338, 72–75. [Google Scholar] [CrossRef]
- Stern, Y.; Gurland, B.; Tatemichi, T.K.; Tang, M.X.; Wilder, D.; Mayeux, R. Influence of education and occupation on the incidence of Alzheimer’s disease. JAMA 1994, 271, 1004–1010. [Google Scholar] [CrossRef]
- Kaszniak, A.W. Neuropsychological consultation to geriatricians: Issues in the assessment of memory complaints. Clin. Neuropsychol. 1987, 1, 35–46. [Google Scholar] [CrossRef]
- Liebermann-Jordanidis, H.; Roheger, M.; Folkerts, A.K.; Alfter, A.; Krohm, F.; Adams, A.; Kalbe, E. A systematic review on prognostic factors and models for changes in quality of life and depressive symptoms after multi-domain cognitive training in healthy older adults: Who benefits? Int. J. Geriatr. Psychiatry 2023, 38, e5923. [Google Scholar] [CrossRef]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2020. [Google Scholar]
- Wells, C.E. Pseudodementia. Am. J. Psychiatry 1979, 136, 895–900. [Google Scholar] [CrossRef]
- Sachdev, P.S.; Reutens, S. The nondepressive pseudodementias. In Dementia: Presentations, Differential Diagnosis, and Nosology, 2nd ed.; Emery, V.O.B., Oxman, T.E., Eds.; The Johns Hopkins University Press: Baltimore, MD, USA, 2003; pp. 417–443. [Google Scholar]
- Marazziti, D. Psicofarmacoterapia Clinica, VI ed.; Giovanni Fioriti Editore: Roma, Italy, 2020. [Google Scholar]
- Reynolds, C.F., 3rd; Kupfer, D.J.; Houck, P.R.; Hoch, C.C.; Stack, J.A.; Berman, S.A.; Zimmer, B. Reliable discrimination of elderly depressed and demented patients by electroencephalographic sleep data. Arch. Gen. Psychiatry 1998, 45, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, D.; Wertman, E.; Bentin, S. Passive listening and task related P300 measurement for the evaluation of dementia and pseudodementia. Clin. Electroencephalogr. 1991, 22, 102–107. [Google Scholar] [CrossRef]
- Cho, M.J.; Lyoo, I.K.; Lee, D.W.; Kwon, J.S.; Lee, J.S.; Lee, D.S.; Jung, J.K.; Lee, M.C. Brain single photon emission computed tomography findings in depressive pseudodementia patients. J. Affect. Disord. 2002, 69, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Abas, M.A.; Sahakian, B.J.; Levy, R. Neuropsychological deficits and CT scan changes in elderly depressives. Psychol. Med. 1990, 20, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Connors, M.H.; Quinto, L.; Brodaty, H. Longitudinal outcomes of patients with pseudodementia: A systematic review. Psychol. Med. 2019, 49, 727–737. [Google Scholar] [CrossRef]
- Alexopoulos, G.S. Pharmacotherapy for late-life depression. J. Clin. Psychiatry 2011, 72, e04. [Google Scholar] [CrossRef]
- Bottino, C.M.; Barcelos-Ferreira, R.; Ribeiz, S.R. Treatment of depression in older adults. Curr. Psychiatry Rep. 2012, 14, 289–297. [Google Scholar] [CrossRef]
- Katona, C.; Hansen, T.; Olsen, C.K. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Int. Clin. Psychopharmacol. 2012, 27, 215–223. [Google Scholar] [CrossRef]
- Taylor, W.D. Clinical practice. Depression in the elderly. N. Engl. J. Med. 2014, 371, 1228–1236. [Google Scholar] [CrossRef]
- Perini, G.; Cotta Ramusino, M.; Sinforiani, E.; Bernini, S.; Petrachi, R.; Costa, A. Cognitive impairment in depression: Recent advances and novel treatments. Neuropsychiatr. Dis. Treat. 2019, 15, 1249–1258. [Google Scholar] [CrossRef]
- Voros, V.; Fekete, S.; Tenyi, T.; Rihmer, Z.; Szili, I.; Osvath, P. Untreated depressive symptoms significantly worsen quality of life in old age and may lead to the misdiagnosis of dementia: A cross-sectional study. Ann. Gen. Psychiatry 2020, 19, 52. [Google Scholar] [CrossRef] [PubMed]
- Bartels, C.; Wagner, M.; Wolfsgruber, S.; Ehrenreich, H.; Schneider, A.; Alzheimer’s Disease Neuroimaging Initiative. Impact of SSRI therapy on risk of conversion from mild cognitive impairment to Alzheimer’s dementia in individuals with previous depression. Am. J. Psychiatry 2018, 175, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Koesters, M.; Ostuzzi, G.; Guaiana, G.; Breilmann, J.; Barbui, C. Vortioxetine for depression in adults. Cochrane Database Syst. Rev. 2017, 7, CD011520. [Google Scholar] [CrossRef] [PubMed]
- Kodesh, A.; Sandin, S.; Reichenberg, A.; Rotstein, A.; Pedersen, N.L.; Ericsson, M.; Karlsson, I.K.; Davidson, M.; Levine, S.Z. Exposure to antidepressant medication and the risk of incident dementia. Am. J. Geriatr. Psychiatry 2019, 27, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Solomonov, N.; Alexopoulos, G.S. Do antidepressants increase the risk of dementia? Am. J. Geriatr. Psychiatry 2019, 27, 1189–1191. [Google Scholar] [CrossRef]
- American Psychiatric Association. DSM-5. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–57. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Pfeiffer, E. A short psychiatric evaluation schedule: A new 15-item monotonic scale indicative of functional psychiatric disorder. In Brain Function in Old Age; Hoffmeister, F., Müller, C., Eds.; Springer: Berlin/Heilderberg, Germany, 1979; pp. 228–236. [Google Scholar] [CrossRef]
- Alexopoulos, G.S.; Abrams, R.C.; Young, R.C.; Shamoian, C.A. Cornell Scale for Depression in Dementia. Biol. Psychiatry 1988, 23, 271–284. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Pozzoli, S.; De Carlo, V.; Madonna, D. Depression, dementia, and pseudodementia. In Clinical Cases in Psychiatry: Integrating Translational Neuroscience Approaches; Altamura, A., Brambilla, P., Eds.; Springer International Publishing: Berlin/Heilderberg, Germany, 2019; pp. 171–188. [Google Scholar] [CrossRef]
- Pozzi, F.E.; Licciardo, D.; Musarra, M.; Jonghi-Lavarini, L.; Crivellaro, C.; Basso, G.; Appollonio, I.; Ferrarese, C. Depressive pseudodementia with reversible AD-like brain hypometabolism: A case report and a review of the literature. J. Pers. Med. 2022, 12, 1665. [Google Scholar] [CrossRef]
- Padovani, A.; Antonini, A.; Barone, P.; Bellelli, G.; Fagiolini, A.; Ferini Strambi, L.; Sorbi, S.; Stocchi, F. Exploring depression in Alzheimer’s disease: An Italian Delphi Consensus on phenomenology, diagnosis, and management. Neurol. Sci. 2023. [Google Scholar] [CrossRef]
- Nobili, F.; Arbizu, J.; Bouwman, F.; Drzezga, A.; Agosta, F.; Nestor, P.; Walker, Z.; Boccardi, M.; EANM-EAN Task Force for the Prescription of FDG-PET for Dementing Neurodegenerative Disorders. European Association of Nuclear Medicine and European Academy of Neurology recommendations for the use of brain 18F-fluorodeoxyglucose positron emission tomography in neurodegenerative cognitive impairment and dementia: Delphi consensus. Eur. J. Neurol. 2018, 25, 1201–1217. [Google Scholar] [CrossRef]
- Rybakowski, J.K.; Nawacka, D.; Kiejna, A. One-year course of the first vs. multiple episodes of depression—Polish naturalistic study. Eur. Psychiatry 2004, 19, 258–263. [Google Scholar] [CrossRef]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef]
- Nyer, M.; Kasckow, J.; Fellows, I.; Lawrence, E.C.; Goldhan, S.; Solorzano, E.; Zisook, S. The relationship of marital status and clinical characteristics in middle-aged and older patients with schizophrenia and depressive symptoms. Ann. Clin. Psychiatry 2010, 22, 172–179. [Google Scholar]
- Santarelli, E.; Cottone, F. Leaving home, family support and intergenerational ties in Italy: Some regional differences. Demogr. Res. 2009, 21, 1–12. [Google Scholar] [CrossRef]
- Van Gelder, B.M.; Tijhuis, M.; Kalmijn, S.; Giampaoli, S.; Nissinen, A.; Kromhout, D. Marital status and living situation during a 5-year period are associated with a subsequent 10-year cognitive decline in older men: The FINE Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, 213–219. [Google Scholar] [CrossRef]
- Bjelland, I.; Krokstad, S.; Mykletun, A.; Dahl, A.A.; Tell, G.S.; Tambs, K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 2008, 66, 1334–1345. [Google Scholar] [CrossRef] [PubMed]
- Lövdén, M.; Fratiglioni, L.; Glymour, M.M.; Lindenberger, U.; Tucker-Drob, E.M.T. Education and cognitive functioning across the life span. Psychol. Sci. Public Interest 2020, 21, 6–41. [Google Scholar] [CrossRef]
- Patria, B. The longitudinal effects of education on depression: Finding from the Indonesian national survey. Front. Public Health 2022, 10, 1017995. [Google Scholar] [CrossRef]
- Bowman, S.; McKinstry, C.; Howie, L.; McGorry, P. Expanding the search for emerging mental ill health to safeguard student potential and vocational success in high school: A narrative review. Early Interv. Psychiatry 2020, 14, 655–676. [Google Scholar] [CrossRef]
- Grasdalsmoen, M.; Eriksen, H.R.; Lønning, K.J.; Sivertsen, B. Physical exercise, mental health problems, and suicide attempts in university students. BMC Psychiatry 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Berg, S.; Dellasega, C. The Use of psychoactive medications and cognitive function in older adults. J. Aging Health 1996, 8, 136–149. [Google Scholar] [CrossRef]
- Oh, E.S.; Rosenberg, P.B.; Rattinger, G.B.; Stuart, E.A.; Lyketsos, C.G.; Leoutsakos, J.S. Psychotropic medication and cognitive, functional, and neuropsychiatric outcomes in Alzheimer’s Disease (AD). J. Am. Geriatr. Soc. 2021, 69, 955–963. [Google Scholar] [CrossRef]
- Chen, A.T.; Nasrallah, H.A. Neuroprotective effects of the second generation antipsychotics. Schizophr. Res. 2019, 208, 1–7. [Google Scholar] [CrossRef]
- Leentjens, A.F.; Van den Akker, M.; Metsemakers, J.F.; Lousberg, R.; Verhey, F.R. Higher incidence of depression preceding the onset of Parkinson’s disease: A register study. Mov. Disord. 2003, 18, 414–418. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N (%) | ||
|---|---|---|
| Diagnosis | Depressive disorder | 33 (57.9%) |
| Bipolar disorder | 24 (42.1%) | |
| Number of episodes | First episode | 25 (43.9%) |
| Multiple episodes | 32 (56.1%) | |
| Family history of psychiatric disorder | None | 38 (66.7%) |
| Positive | 19 (33.3%) | |
| Psychiatric comorbidity | None | 50 (87.7%) |
| Panic disorder | 4 (7%) | |
| Generalized anxiety disorder | 3 (5.3%) | |
| Neurological disease | None | 52 (91.2%) |
| Stroke, chorea, Parkinson’s disease, essential tremor | 5 (8.8%) | |
| Medical illness | None | 22 (38.6%) |
| One medical disease | 35 (61.4%) | |
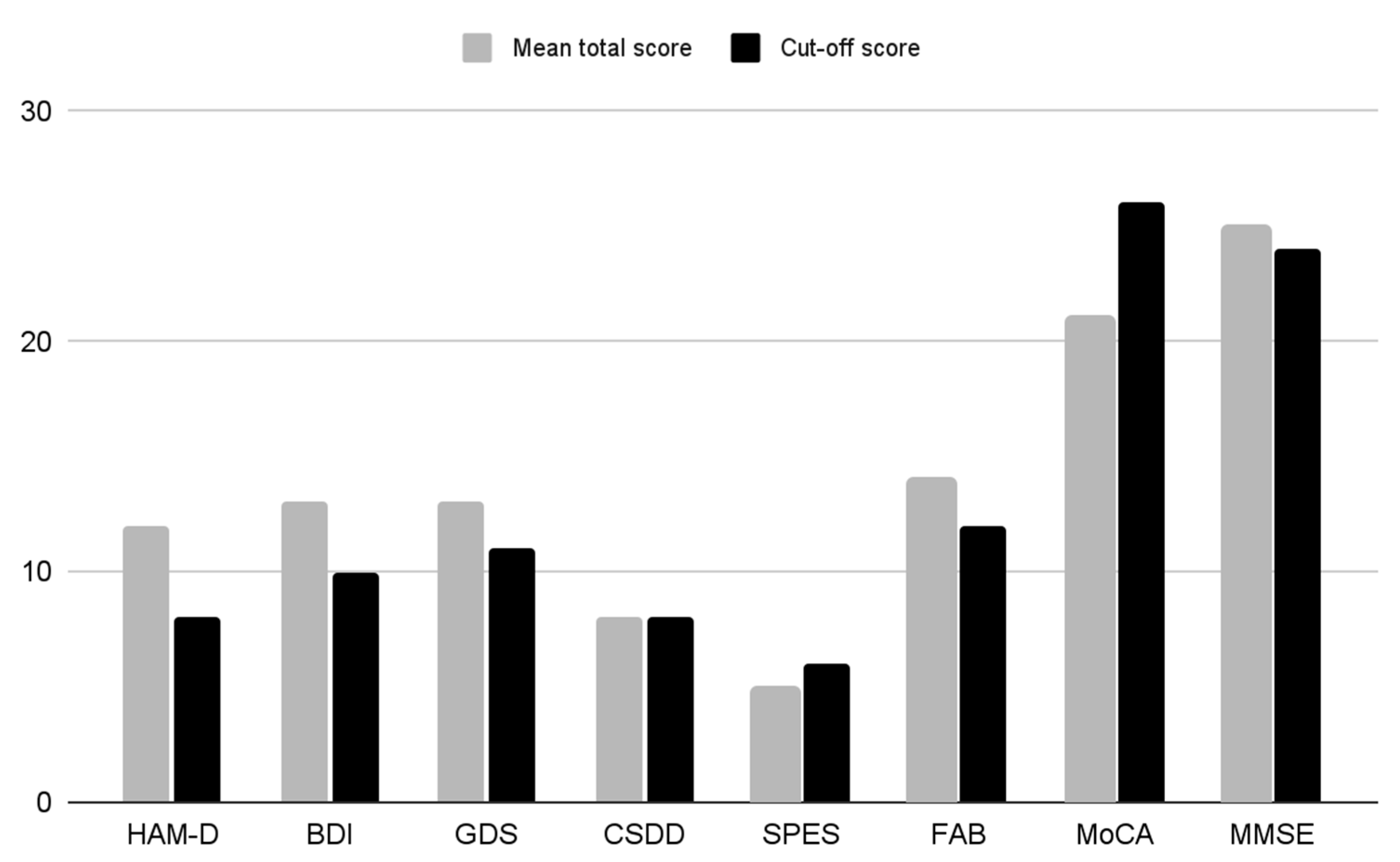
| Scale | Mean Total Score ± SD | Cut-Off Score |
|---|---|---|
| HAM-D | 12.18 ± 6.33 | ≥8 |
| BDI | 12.79 ± 9.89 | ≥10 |
| GDS | 12.69 ± 8.25 | ≥11 |
| CSDD | 8.35 ± 6.25 | ≥8 |
| SPES | 5.75 ± 3.82 | ≥6 |
| FAB | 14.12 ± 3.92 | <12.03 |
| MoCA | 21.30 ± 4.86 | <26 |
| MMSE | 25.06 ± 4.20 | ≤24 |
| Panel a | |||||||||
| BDI | GDS | CSDD | |||||||
| r | p | r | p | r | p | ||||
| HAM-D | 0.77 | <0.01 | 0.68 | <0.01 | 0.70 | <0.01 | |||
| BDI | 0.77 | <0.01 | 0.73 | <0.01 | |||||
| GDS | 0.67 | <0.01 | |||||||
| Panel b | |||||||||
| FAB | MMSE | ||||||||
| r | p | r | p | ||||||
| MoCA | 0.75 | <0.01 | 0.52 | <0.01 | |||||
| FAB | 0.33 | <0.01 | |||||||
| Panel c | |||||||||
| FAB | MoCA | MMSE | |||||||
| r | p | r | p | r | p | ||||
| HAM-D | 0.29 | <0.01 | ns | ns | ns | ns | |||
| BDI | 0.26 | <0.01 | ns | ns | ns | ns | |||
| CSDD | 0.34 | <0.01 | ns | ns | ns | ns | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buccianelli, B.; Marazziti, D.; Arone, A.; Palermo, S.; Simoncini, M.; Carbone, M.G.; Massoni, L.; Violi, M.; Dell’Osso, L. Depression and Pseudodementia: Decoding the Intricate Bonds in an Italian Outpatient Setting. Brain Sci. 2023, 13, 1200. https://doi.org/10.3390/brainsci13081200
Buccianelli B, Marazziti D, Arone A, Palermo S, Simoncini M, Carbone MG, Massoni L, Violi M, Dell’Osso L. Depression and Pseudodementia: Decoding the Intricate Bonds in an Italian Outpatient Setting. Brain Sciences. 2023; 13(8):1200. https://doi.org/10.3390/brainsci13081200
Chicago/Turabian StyleBuccianelli, Beatrice, Donatella Marazziti, Alessandro Arone, Stefania Palermo, Marly Simoncini, Manuel Glauco Carbone, Leonardo Massoni, Miriam Violi, and Liliana Dell’Osso. 2023. "Depression and Pseudodementia: Decoding the Intricate Bonds in an Italian Outpatient Setting" Brain Sciences 13, no. 8: 1200. https://doi.org/10.3390/brainsci13081200
APA StyleBuccianelli, B., Marazziti, D., Arone, A., Palermo, S., Simoncini, M., Carbone, M. G., Massoni, L., Violi, M., & Dell’Osso, L. (2023). Depression and Pseudodementia: Decoding the Intricate Bonds in an Italian Outpatient Setting. Brain Sciences, 13(8), 1200. https://doi.org/10.3390/brainsci13081200