Abstract
Facing an unrelenting rise in dementia cases worldwide, researchers are exploring non-pharmacological ways to ameliorate cognitive decline in later life. Twenty older adults completed assessments before and after a single bout of interactive physical and cognitive exercise, by playing a neuro-exergame that required pedaling and steering to control progress in a tablet-based video game tailored to impact executive function (the interactive Physical and Cognitive Exercise System; iPACES v2). This study explored the cognitive and biomarker outcomes for participants with mild cognitive impairment (MCI) and normative older adults after 20 min of pedal-to-play exercise. Neuropsychological and salivary assessments were performed pre- and post-exercise to assess the impact. Repeated-measures ANOVAs revealed significant interaction effects, with MCI participants experiencing greater changes in executive function and alpha-amylase levels than normative older adults; within-group changes were also significant. This study provides further data regarding cognitive effects and potential mechanisms of action for exercise as an intervention for MCI.
1. Introduction
1.1. Dementia Epidemic and Mild Cognitive Impairment (MCI)
Aging can be characterized by cognitive changes such as executive function deterioration; however, these changes can occur earlier in life in those who develop Alzheimer’s disease (AD) and related dementias [1]. There is a dementia epidemic that poses a serious risk to the older population, as the incidence of dementia is expected to reach 152.8 million by 2050 [2]. This is concerning for the older adult population because there are serious limitations in the clinical treatment of Alzheimer’s and dementia, as there is no specific cure for the disorder, and pharmacological treatments have limited effects on dementia progression [3,4,5]. Therefore, researchers worldwide must focus on the development of non-pharmacological treatments, such as exercise, to delay the progression of cognitive decline toward dementia. One possible way to delay the onset of cognitive decline toward dementia [6] is to intervene early, in the prodromal phase of mild cognitive impairment (MCI), to ameliorate deficits in affected cognitive domains. The potential to delay the onset of dementia could reduce the prevalence of dementia [7]; a delay by one year could prevent close to 10 million cases of AD by 2050 [8].
While behavioral interventions may not reverse cognitive decline, there is evidence that physical activity can reduce the risk of dementia onset [9,10,11] or slow progression [7,12]. Unfortunately, many older adults do not exercise [13]. Therefore, researchers are developing innovative methods to engage older adults in physical exercise, such as virtual reality or video games that incorporate exercise (exergames; [14]), as well as exergames that may help older adults to reap the benefits of exercise by prospectively targeting neuropsychological functions such as executive function (neuro-exergame; [15]). A recent review shows that a behavioral intervention consisting of physical and mental exercise has the potential to improve executive control and global cognition in MCI patients [16]. This present study aims to replicate and extend a prior finding that a single bout of interactive neuro-exergaming, an integrated physical and cognitive exercise intervention, could produce enhanced cognitive benefits in the executive function domain [17]. Moreover, this study measured changes in biomarkers that are associated with cognitive improvements [17].
1.2. Physical Exercise and Cognition Change
Recent and prior meta-analyses [12,18,19,20] have found evidence demonstrating that physical activity can improve cognitive function in later life. More specifically, some studies have found that physical exercise can offer small benefits to executive function in older adults [21,22,23,24]. However, recent reviews have found little evidence in the relationship between physical exercise and cognitive benefits in the literature [25,26]. Nevertheless, some reviews have explored the effect of physical exercise on neurocognitive disorders with the goal of improving cognitive function [18,27,28,29]. Studies have explored the use of physical exercise to achieve cognitive improvements in MCI individuals [30,31,32]. There is evidence that supports the notion that physical activity benefits cognition, especially in the executive function domain, among those in the MCI population [20,33,34,35]. Recent reviews strongly encourage larger randomized controlled trials (RCTs) in the MCI population, where physical activity interventions can explore the broader neuropathology of cognitive decline [16,36,37].
Researchers have used different cognitive and exercise interventions to study the effects of exercise in the older adult population [12]. The current study focuses on the MCI population as opposed to more progressed forms of Alzheimer’s disease and related dementias, because the activation of the exercise-induced neurobiological mechanisms has led to greater cognitive improvements in the MCI population [4,38,39]. Many studies have shown that exercise benefits cognition—for example, in the executive function domain, in MCI patients [30,31,32,33,35,40]. Compared to various exercise interventions, aerobic exercise has maintained a medium effect size on global cognition in the MCI population [34], and acute aerobic exercise can benefit executive function in the older adult population [41] Ultimately, physical exercise has been shown to be a reliable method to bring about cognitive improvements in the Alzheimer’s and MCI population [42].
Given that most older adults do not exercise at adequate levels, researchers have used exergaming as a motivation for exercise, hoping that an engaging exergame would stimulate consistent exercise toward proper dosing to maximize the cognitive benefits of physical exercise [43]. It was hypothesized that over three months, older adults pedaling a stationary bike along a virtual reality pathway [43] would experience greater cognitive benefits than those who were assigned to the traditional stationary bike. Analyses showed that the cybercycle condition yielded cognitive benefits as hypothesized, as the cybercycle condition yielded a 23% decreased risk of developing MCI [43]. In the end, it was found that the improvements were not due to the dose of exercise: it appeared that the combined physical and cognitive exercise yielded a synergistic effect on cognition, leading to enhanced improvements [43]. The interactive Physical and Cognitive Exercise System (iPACES v1) was developed in an attempt to maximize the neuropsychological benefit that might be derived from combined mental and physical exercise, not simply utilizing a “dual-task” paradigm (e.g., pedaling while playing a separate, non-interactive game) but rather emphasizing interactivity, where pedaling controls on-screen movement and where steering is involved in intentionally designed mental processing tasks that also adaptively impact the physical exercise, i.e., a neuro-exergame [44].
Current theories suggest that the cognitive benefits of physical exercise can be attributed to multiple neurobiological mechanisms that promote neuroplasticity and neurogenesis in the brain [45]. Prior animal research showed that physical exercise and mental exercise activate different neurobiological mechanisms, as physical exercise promotes neurogenesis and mental exercise promotes neuronal survival [46,47,48]. Additionally, human research has shown that physical and mental exercise induce different structural and functional differences in the brain [49]. Studies have revealed various biomarkers correlated with changes in cognition that are indicative of the broader physiological mechanisms [50]. One biomarker, Brain-Derived Neurotrophic Factor (BDNF), is hypothesized to be activated by physical exercise, which is associated with blood flow improvements and neuronal growth [51]. The current iPACES study intended to investigate the enhanced cognitive benefits of interactive cognitive and physical exercise and measure certain biomarkers that may be associated with the underlying neurological biochemical and cellular changes associated with cognitive decline.
1.3. Cognitive Training and Cognitive Decline
The surprising findings of the cybercycle study [43] have influenced researchers to investigate the possibility that the cognitive training component has some synergistic effect with physical exercise. Despite our own skepticism, recent guidelines from the American Academy of Neurology [52] state that clinicians should recommend cognitive interventions over pharmacological interventions for MCI patients [52]. Prior meta-analyses indicate that cognitive training interventions do produce effects in the older adult population [17,53,54,55,56,57]. Additionally, prior studies have shown that cognitive interventions alone, such as interactive computer tasks, yield cognitive improvements in older adults [58,59,60,61].
However, researchers have raised concerns regarding the validity of the literature concerning cognitive interventions. One Cochrane review of 11 RCTs revealed no significant benefits from cognitive training [62]. Critics question the cognitive training intervention literature regarding the transfer and generalization of effects to overall cognitive functioning and everyday tasks from cognitive training tasks [32,63,64]. A review of the literature on cognitive training devices found that studies reported significant findings with several limitations, weakening the validity of the tests [56,57,65,66,67]. Furthermore, a critique of the literature has found further limitations, including reporting, generalizability, and more, that weaken the enthusiasm surrounding the findings [62,68,69,70,71,72]. Given the controversy regarding the cognitive benefits resulting from cognitive training alone, it is possible that one can reap the benefits of cognitive training when it is integrated with other interventions, such as physical activity, because of the activation of additional neurobiological mechanisms. Thus, researchers are investigating the benefits of interventions that integrate cognitive training with interventions such as physical exercise.
1.4. Mental and Physical Exercise Combination (Interactive/Neuro-Exergaming) and Cognitive Decline
Research has recently begun to understand the interaction between physical and mental exercise, specifically the physiological mechanisms induced by physical exercise that lead to greater cognitive improvements. When physical exercise is combined with cognitive training, the resulting impact may allow the brain to experience greater cognitive benefits. Many reviews have shown the added cognitive benefits of interventions where physical exercise is combined with mental exercise [73,74,75,76,77,78,79,80,81]. Many theories have offered neurobiological explanations for the combined effects of physical and exercise training [77]; however, more technological innovations are needed to explore the physiological impact and effects, specifically in the MCI population [82].
There is a vast amount of literature that covers the cognitive effects of different types of multimodal interventions: (1) combined interventions, where physical and cognitive exercise components are administered sequentially [57,79,83,84,85,86,87]; (2) dual-task interventions, where the components are administered as separate types of tasks at the same time [88,89,90,91,92,93,94,95]; and (3) interactive interventions, a specialized form of exergaming, in which the actions in one component directly affect the other synergistically [15,17,44,96,97,98,99,100,101,102,103].
The theory that integrated (mental + physical exercise) cognitive interventions slow the decline in cognition in older adults with MCI has led to an increase in RCTs. Meta-analyses and reviews explore the synergistic effects of different combinations of mental and physical exercise [76,82,104,105]. Combined interventions have yielded cognitive benefits in the older adult population, specifically in the domains of executive function and memory [34,35,46,48,49,53,54], as well as in global cognition [59]. A recent meta-analysis looked at four studies that included MCI samples and reported that combined interventions were more effective than dual-task interventions [104]. However, some studies have shown that when combined interventions are compared to physical and cognitive interventions alone, they do not produce significantly greater cognitive improvements [78,85,88,100,106].
Dual-task or simultaneous interventions have led to improved cognition in older adults with a variety of exercise activities [82,91,94,107,108,109,110,111]. A recent meta-analysis revealed that integrated physical and cognitive exercise interventions produced significant improvements in cognitive performance, and simultaneous physical and cognitive interventions were superior to combined interventions [73]. Recent reviews of the literature on the cognitive benefits of interactive exergaming have shown that there is evidence of a cognitive improvement [15,76,98,99,112,113,114,115,116]. There remains little research that compares the cognitive and neurobiological outcomes of simultaneous/interactive and sequential interventions, but it is still hypothesized that interactive interventions have a synergistic effect [15,17,43,44,82,102,103,117].
Researchers evaluated the effects of various interactive physical and mental exercise combinations in a recent six-month RCT called the Aerobic and Cognitive Exercise Study (ACES) for MCI [44]. Participants were assigned to three conditions: (1) exer-tour (pedaling along a virtual scenic bike path; (2) exer-score (pedaling through an interactive game involving dragons and coins; (3) game-only (no pedaling). Analyses revealed an increase in executive function after 6 months of exercising in both the exer-tour and exer-score samples [44]. However, the study had several limitations: the lack of portability of the commercial grade equipment, which made the intervention experience difficult for the MCI participants; the lack of flexibility in the game to adapt to various cognitive abilities and target specific cognitive domains; and the lack of a reliable method to measure “mental exercise” behaviors [44]. To overcome these limitations, Anderson-Hanley et al. developed a portable neuro-exergame, iPACES v1, that was launched and found to be feasible for MCI participants in subsequent studies [43,103]. The second iteration (iPACES v2) of the neuro-exergame was launched in a three-month RCT, where analyses showed that executive function improved in the MCI participants [15]. The present study aims to add evidence to support the use of the iPACES neuro-exergame as an interactive physical and mental exercise intervention to induce cognitive improvements in the MCI population.
1.5. Single-Bout Exercise Intervention and Cognitive Performance
The growing field of various exercise interventions has primarily focused on studying the effects in long-term settings. There is a lack of research surrounding the efficacy of a single session of a physical exercise intervention. Meta-analyses have shown that a single bout of exercise (i.e., less than 60 min) can provide a noticeable improvement in executive function [41,118,119]. Studies have shown that a single bout of exercise can improve cognitive performance in children and younger adults [120,121]. Early studies compared cognitive performance in older adults to that in younger adults and found that acute bouts of aerobic exercise significantly improved executive function and cognitive performance in older adults [118,122]. Many researchers have studied the effects of single-bout exercise on the domains of working memory and inhibitory control [118,123]; additionally, researchers have examined the impact on memory [124,125]. New research looks at how a single-bout exercise session affects different components of executive function, such as cognitive flexibility and task-switching ability [126]. Additionally, a few studies have explored the effects of a single bout of exercise on biomarkers associated with neural growth. An acute bout of aerobic exercise has been shown to increase the serum levels of BDNF, a neurotrophic factor correlated with neural growth [127,128]. Researchers evaluated the effects of a single exercise bout of interactive exergaming in a pilot study of the iPACES v1, and analyses found a significant increase in executive function, represented by increases in performance on neuropsychological tasks, among older adults post-intervention [17]. This study is a partial replication and extension, expanding the investigation to include potential biomarkers linked to cognitive benefits.
1.6. Neurobiological Mechanism and Markers of Cognitive Changes
It has been hypothesized that an interactive exergaming intervention can produce greater cognitive benefits due to the synergistic interaction between physical exercise and cognitive stimulation. The research focuses on connecting mental processes to the physiological pathways triggered by exercise, as revealed by measurable changes in particular biomarkers, such as BDNF and IGF-1 [103]. Multiple neurobiological mechanisms are activated by physical exercise, including the regulation of the production and uptake of certain central and peripheral growth factors, which promote synaptic plasticity and improvements in cognition [45].
The following is a summary of the current understanding of the role of several of these factors as they relate to cognitive function and dementia. For example, physical exercise has been shown to yield increases in BDNF, which is linked to enhanced plasticity [45,88,129,130,131,132,133,134]. BDNF has been implicated as a neuroprotective growth factor, and it is part of a cascade that promotes neuronal plasticity [45]. However, the use of BDNF as a biomarker attributed to exercise has been quite controversial, with inconsistencies reported in various studies [135]. Insulin-Like Growth Factor (IGF-1) has been discovered to play a variable role in the exercise-induced mechanism that promotes neuroplasticity [45,132,136,137,138]. IGF-1 has been shown to increase with exercise [127,136,139,140,141], and decreased IGF-1 has been associated with decreased cognition [142,143]. BDNF and IGF-1 participate in intertwining pathways that ultimately lead to neurogenesis and improved learning [45].
Many studies have studied cortisol and its role in the stress response mechanism that is triggered by exercise. Cortisol, a glucocorticoid hormone involved in the human stress response [144,145], has been highlighted in individuals with cognitive decline as it can cross the blood–brain barrier and affect pathology and cognition [146,147,148]. Studies show that high concentrations of cortisol are linked to changes in cognition in patients with Alzheimer’s and other dementias [144,149,150,151,152,153]. Prior studies have explored the association between cognitive improvements in MCI and changes in cortisol [154]. It was found that cortisol decreased with improvements in executive function in the MCI population [15]. More research is needed to understand the physiological interaction between the stress response and cognitive improvements in MCI. Additionally, salivary alpha-amylase is another biomarker of the human stress response and has been shown to increase in the face of acute stress, making it a viable biomarker to explore in MCI populations [155]. This study contributes to the limited literature on the role of salivary alpha-amylase in the stress response triggered by physical exercise.
1.7. A Priori Hypotheses
- Executive function will improve after a single-bout intervention of interactive neuro-exergaming [17].
- Improvements in cognition will be correlated with changes in the salivary biomarkers as follows:
- Cortisol will be negatively correlated [15];
- Alpha-amylase will be positively correlated [155];
- IGF-1 will be positively correlated [15].
- MCI participants will experience a greater improvement in cognitive performance than normative older adults [103].
2. Materials and Methods
2.1. Participants
Participants were enrolled at multiple sites in the Northeastern United States and the study protocol was approved by the IRBs at the relevant institutions. Older adults, aged 50+, were invited to voluntarily participate in a single bout of neuro-exergaming on the tablet-based interactive Physical and Cognitive Exercise System (iPACES v2). Over two years, participants were recruited from an academic neuropsychology lab, independent senior residences, and a physical therapy center. Various recruitment methods were used, including outreach emails by the administrators of programs, the posting of flyers, and demonstrations of the game at senior living communities.
Criteria used to screen participants included physical or mental impairments that would hinder the participant’s ability to complete or understand the cognitive tests, pedal an under-desk elliptical, or play an interactive memory game. Participants were screened using the Impaired Decision-Making Capacity (IDMC) test, a structured interview that ensures that the appropriate consent can be obtained (IDMC; Veteran’s Health Administration Handbook), and they provided informed consent (if applicable; alternatively, they were co-signed by a surrogate or legally appointed representative per the IDMC).
The participants who completed the single bout were 20 females and 13 males (see Table 1).

Table 1.
Demographics for the iPACES single-bout intervention.
The mean age of the participants was 72.8 (SD = 10.7), the mean level of education was 16.1 years (SD = 2.4), the mean body mass index was 25.9 (SD = 3.3), the average cognitive status was in the normative range (24.7, MoCA > 23; with 10 meeting the screening criteria for MCI, MoCA ≤ 23) [156], and one individual self-reported a multiethnic background (see Table 1).
Thirty-three participants completed the 20-min single bout of exercise using the under-desk elliptical and the interactive iPACESv2 game (two participants reported parkinsonism; however, their slight tremors did not impede the neuropsychological exercise or evaluation; see Figure 1 and Table 2).
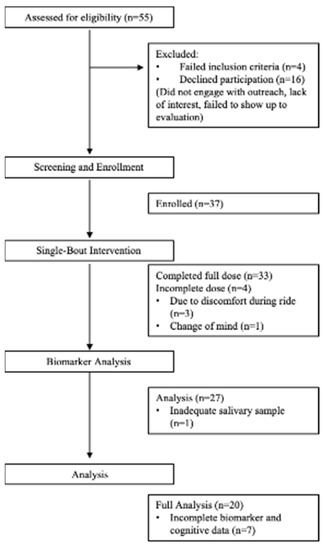
Figure 1.
CONSORT flow diagram: enrollment, progress, and analysis throughout the single-bout intervention.
Table 2.
Biomarker and cognitive outcomes for the iPACES single-bout intervention.
Of the 33 participants, 27 participants were able to provide complete salivary samples, which were used for the neurobiological marker analysis (see Results). Of the 27 participants, 20 participants were included in the pre/post comparative assessments, while seven participants had to be excluded due to incomplete data (either administration error in recording or due to participant factors such as difficulty completing a test). Thus, a total of 20 participants were able to be included in the final analysis, and, of those, five met the screening criteria for MCI.
2.2. Procedures
After participants expressed interest in participating in the study, they were screened by a research associate over the telephone or in person using the IDMC structured interview. A time and location were scheduled for the evaluation, in which participants reviewed and signed an informed consent form. Participants completed a demographic form, including age, height, weight, marital status, computer use, and exercise history. During the evaluation, participants completed a neuropsychological battery before and after the exercise intervention, to understand the change in cognitive performance. Saliva samples were collected before and after the exercise intervention using the passive drool technique, to be stored for Enzyme-Linked Immunosorbent Assay (ELISA) analysis to investigate the biomarker correlations relating the changes in cognition to exercise, as described further below. Upon completion of the intervention, participants were asked to complete an “exit” survey questionnaire in which they evaluated the exergaming intervention and experience.
2.3. Measures
2.3.1. Neuropsychological Evaluation
The purpose of this intervention was to investigate the correlation between physical exercise and the improvement of executive function. Previous literature has shown that executive function is the major domain that improves due to exercise and exergaming [12,15,17,41,44,59,67,75,93,103,108,109,115]. Executive function refers to higher-order mental processing that is responsible for the coordination and execution of attention and behavior when faced with multiple stimuli that require working memory, inhibition, and cognitive flexibility [157]. These traits are essential for older adults to maintain independence in later life. A battery of neuropsychological assessments was administered to collect data on various aspects of executive function, including the Stroop task, to assess the changes before and after the single-bout intervention.
2.3.2. Cognitive Measures
The Stroop task (40-item format) is an executive function measure that has been used with high validity and reliability in clinical and research studies [158,159,160,161,162]. In Stroop A, participants stated the colors of blocks printed in line on a page; in Stroop B, participants stated the color words printed in black ink; in Stroop C, participants stated the color of the ink and the color words were printed on the page. In Stroop C, some of the color words were congruent (same color ink as the color word) and some were incongruent (different color ink and word), so this required participants to ignore distractor stimuli and allowed for the analysis of effortful inhibition. In the study, both the paper Stroop and an electronic version of the Stroop through an application called Brain Baseline were administered to each patient [15,159].
The Congruent Correct–Incongruent Incorrect metric (CCII; [15,163]) is an executive measure scaling technique that was applied to the electronic Brain Baseline Stroop task. The CCII metric is the percentage of correct congruent responses minus the percentage of incorrect incongruent responses (II; [15]). The objective of the CCII metric is to measure the strength of mental processing by comparing the ability to correctly respond to easier stimuli with incorrect performance when responding to different stimuli. The electronic Brain Baseline Stroop data were used to compute the CCII metric and yielded proportions ranging from −1 to 1.
The Alzheimer’s Disease Assessment Scale (ADAS) Word Recall Task [164] is a verbal memory task used to evaluate short-term memory through immediate recall [165] and long-term memory through delayed recall [166]. In the first three trials, participants verbally read a list of 10 words displayed to them on cards with the following immediate recall. After completing 10 min of another neuropsychological task, participants were asked to recall the list of words again for delayed recall. Different word lists were used for the pre and post assessments. This task was conducted using the Quizlet app on the iPad.
The Montreal Cognitive Assessment (MoCA; [167]) was used to assess the cognitive function of the participants. The test assesses multiple cognitive domains via delayed word recall, a clock drawing task, digit repetition, color trails, and more. This test has been validated and is commonly used as a cognitive screen in clinical research [167]. The scores can be used to categorize participants within various dementia to normative ranges, where scores above 26 are normal, scores below 17 represent an Alzheimer’s-type dementia, and scores between these values represent an MCI condition [167]. However, a recent meta-analysis of 304 studies showed that a cutoff of score of 23 (MCI < 23) had better diagnostic accuracy [156]. An electronic version of the MoCA was used on the iPad.
2.3.3. Biological Measures
Saliva samples were collected from all participants that were willing and able to offer saliva through passive drool before and after the single-bout intervention. The samples were placed on ice at −80 °C and then analyzed in triplicate for concentrations of cortisol (Cohen Biochemistry lab protocol), alpha-amylase (alpha-amylase saliva ELISA, BioVendor, Brno, Czech Republic), and IGF-1 (Human IGF1 SimpleStep ELISA Kit, Abcam, Cambridge, UK). Protein concentrations in the saliva samples were measured using the bicinchoninic (BCA) assay (Pierce™ BCA Protein Assay Kit, Thermo Fisher, Waltham, MA, USA). Measurements of the salivary biomarkers were normalized to the total protein concentrations.
2.4. Intervention
The interactive physical and cognitive exercise neuro-exergame was designed by the Healthy Aging and Neuropsychology Lab at Union College to target executive function and was initially programmed for a touch-screen PC tablet (iPACES v1) [17]. Version 2 (iPACES v2) of the game used in this study, called Memory Lane, was created through a collaboration between the lab and a software company, 1st Playable Productions in Troy, NY, to improve the playability and to create an iOS app for the iPad [15]. To complete the neuro-exergaming interactive operation and track the necessary vitals for analysis, multiple Bluetooth-enabled devices were integrated into the software: a heart rate monitor ring on the finger (Hammacher Schlemmer Lifewell); a cadence meter to track the pedaling motion (Polar Global Cadence Sensor Bluetooth Smart), and an under-desk elliptical pedaler (Stamina 55-1610 InMotion E1000 Elliptical Trainer).
The iPACES intervention using the Memory Lane game required participants to use an iPad Air 2, an under-desk elliptical, and a heart rate monitor ring. The iPACES Memory Lane neuro-exergame (v2) was played on the iPad [15]. The heart rate ring was used to monitor the heart rate so that participants could reach their target heart rate during their single bout of exercise [168]. The information taken from the memory game was their total score, minutes pedaled, and average heart rate.
The iPACES Memory Lane game was designed to model a real-life scenario along with the intention of testing and challenging executive function by the simulation of riding a bike along a virtual bike path to complete a list of errands [15]. Participants used the iPad as a steering wheel by tilting the device left and right to “steer” through a virtual bike path. Participants were asked to complete a 20-min exercise session, excluding 1–3 min at the beginning to assimilate to the game. Participants were given instructions for the game, starting with how to follow and steer through a simulation of a virtual bike down a road. When the participants pedaled the under-desk elliptical, the virtual bike moved on the screen at the speed at which the participants were pedaling. The cognitive aspect of the game involved a word list memory task in which participants were instructed to remember words presented to them at the beginning of the path. Within the game, participants navigated through forks in the virtual road, where they had to choose the correct destination based on a list of locations (from the words on the list) presented at the beginning. This task targets the executive function abilities; therefore, the iPACES game is classified as a neuro-exergame [44]. When the participants correctly followed the order of locations, they were instructed to follow the bike path in reverse order. The participants could monitor the total time that they exercised, their total distance traveled, and their current heart rate on the screen. Participants were alerted if they chose an incorrect word. After the intervention, participants completed questionnaires regarding performance during and after the exercise, followed by the second set of neuropsychological assessments.
3. Results
Description of Results
Paired t-tests revealed significant changes in salivary alpha-amylase (p = 0.01) and executive function, measured by the CCII ratio (p = 0.04). A repeated-measures ANOVA was conducted to measure the change in alpha-amylase and executive function, measured by the CCII ratio, in the MCI and normative groups. A significant improvement was found in salivary alpha-amylase and the CCII measure of executive function after the single-bout iPACES intervention [F(2,17) = 9.09, p = 0.002]. A univariate ANOVA was conducted to measure the change in salivary alpha-amylase and executive function, measured by the CCII ratio, in the MCI and normative groups. A greater increase in salivary alpha-amylase was found in MCI participants compared to normative participants [F(1,17) = 13.8, p = 0.002] see Figure 2.
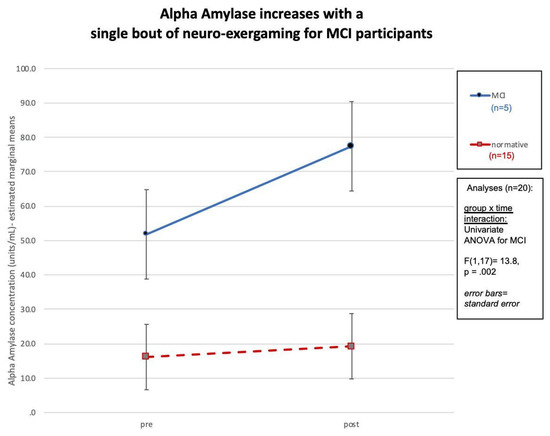
Figure 2.
Change in salivary alpha-amylase among the MCI and normative participants, with a significant increase in alpha-amylase among the MCI participants.
In addition, a greater increase in executive function, measured using the CCII ratio, was found in MCI participants compared to normative participants [F(1,17) = 4.8, p = 0.04], see Figure 3.
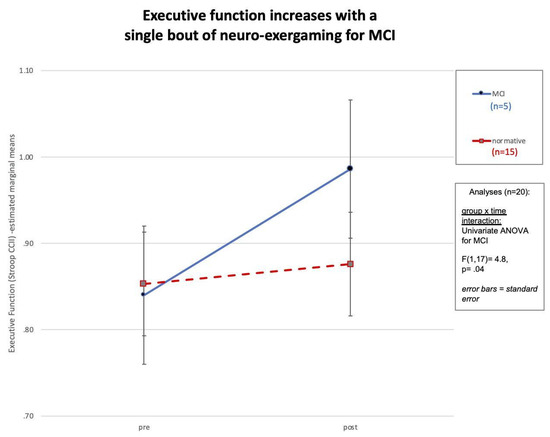
Figure 3.
Change in executive function among the MCI and normative participants, with a significant increase in executive function among the MCI participants.
Furthermore, a negative correlation was found between the change in salivary alpha-amylase and MoCA, with age as a covariate (r = −0.64, p = 0.002).
4. Discussion
This study is a replication and extension of an earlier feasibility trial that explored whether a single bout of interactive physical and cognitive exercise can yield enhanced cognitive benefits compared to independent physical or mental exercise [17]. The synergistic effects of aerobic exercise and cognitive training have been explored in the older adult population with MCI, and this population has previously demonstrated improvements in short-term and long-term neuropsychological abilities [15,17,44,82,102,103]. The current results were derived from 20 older adults who completed assessments before and after a single bout of pedaling-to-play the iPACES neuro-exergame. The purpose of this study was to explore the cognitive and neurobiological effects of a single session of a combined interactive physical and mental exercise intervention, pedaling an under-desk elliptical that controlled progress in a video game. A battery of neuropsychological tests was used to assess changes in executive function, and salivary samples were used to measure changes in neurobiological markers. The results affirm the a priori hypothesis, revealing a significant change in salivary alpha-amylase and executive function, measured using the CCII ratio, amongst the entire group. These findings are important given the varied literature regarding the cognitive effects of a single bout of exercise and provide further evidence of the possible utility of exergaming for MCI patients. The significant increase in salivary alpha-amylase is an intriguing finding, as it provides further evidence that exercise, herein neuro-exergaming, activates the noradrenergic system, which, to our knowledge, has only been reported in one other previous study [155]. The noradrenergic response has been linked to cognitive and memory improvements and can be the focus of future interventions [155]. However, to our knowledge, this is only the second paper studying alpha-amylase in this way. Neither the Segal et al. (2012) [155] nor this study has determined the physiological mechanisms underlying the cognitive changes. Furthermore, this finding reveals that the MCI population may experience stress during the intervention, and additional research is needed to clarify the role of physiological arousal, stress over the challenge, or other factors in elevating alpha-amylase. Continuing research and development in iPACES is aimed at future versions of neuro-exergaming that will make it an enjoyable experience that allows for the maximum cognitive benefits for both challenged (MCI) and higher functioning, normative participants.
Results revealed a significant increase in executive function, measured using the CCII ratio, and salivary alpha-amylase in both the MCI and normative populations. The increases in both salivary alpha-amylase and executive function were greater in the MCI group compared to the normative group. Additionally, the increase in salivary alpha-amylase was found to have a significant negative correlation with the MoCA scores, as individuals with lower MoCA scores were found to experience the greatest change in salivary alpha-amylase. This suggests that the participants with lower cognitive baselines were more likely to experience increases in cognitive markers, evidence for an increase in cognition. This evidence supports the idea of interventions targeting the MCI/intermediate stage of cognitive decline, because the MCI population can experience improvements in cognitive abilities. This phenomenon is possible because those with MCI may still possess the physiological components to obtain the benefits of the activation of the exercise-induced mechanisms that promote neuroplasticity. Furthermore, future research should include measurements of the neurotrophic and neuroprotective growth factors, such as BDNF and VEGF, that are implicated in the mechanism that promotes neural growth [45], to verify that neurogenesis takes place after a single bout of the iPACES intervention.
An important strength in this study was the use of salivary biomarkers as indicators of cognitive improvement. Different biomarkers have now been implicated in several intertwined neurobiological mechanisms that appear to be activated by physical exercise [45], but further research is needed to determine the role of physical, cognitive, and other factors in the process. The ability to quantitatively measure various salivary biomarkers that suggest cognitive improvements will be beneficial in future exergaming interventions because it is non-invasive and simple, compared to serum-based or cerebrospinal biomarkers. Exergaming interventions have evolved to facilitate greater compliance in the MCI/older adult population, as seen in the switch from the stationary bike “cybercycle” [43,44] to an in-home, portable neuro-exergame [17,103]. A practice such as the spinal tap for cerebrospinal fluid to determine beta-amyloid protein levels may not be practical in the older adult population [169]; therefore, the practice of measuring salivary biomarkers will be important in further exergaming interventions. Classical Alzheimer’s biomarkers such as beta-amyloid have been detected using salivary analysis [170,171,172,173]. There is immense potential for further studies to identify and quantitatively determine certain biomarkers that could allow researchers to construct a framework for the broad neurobiological mechanisms. Furthermore, more studies are exploring biomarkers in serum, cerebrospinal fluid, and imaging in patients with MCI, such as microRNA [174]; thus, it would be beneficial to expand the biomarker analysis in future trials to study the exergaming-induced effects.
Another important strength in this study was the neuro-exergame utilizing the iPACES platform, where an iPad can be paired with an under-desk elliptical. The video game component of the iPACES platform provides adequate motivation and attention for older adults to achieve the recommended levels of exercise necessary to improve cognitive health [15,103]. One purpose of the game is to model a real-life, naturalistic situation of a journey in one’s neighborhood to complete a set of errands and then retrace one’s path to return “home,” and it models the independence that is often eroded by progressive cognitive decline. The concept of this game raises the question of how the cognitive benefits of the video game cognitive training manifest in the participants, and, if it can be generalized to “real life”, whether we can conclude that they can maintain or regain qualities diminished due to underlying Alzheimer’s disease or related dementias. Further research in a larger cohort of participants is needed to understand how a long-term neuro-exergame intervention might affect activities of daily living, as this would shed light on how interactive exergaming targeting the executive function domain can affect one’s overall quality of life and cognitive trajectory. A larger, long-term trial might affirm that interactive neuro-exergaming can produce enhanced cognitive benefits and slow the progression of cognitive decline.
One limitation of the study was the lack of reliability of the technology to measure the heart rate reliably. Data were not obtained for the heart rate measurements because the heart rate device did not function consistently to produce continuous heart rate measurements. Prior research has shown that when participants reach their target heart rate, they can maximize the benefits of physical activity [168]. The fact that the findings were significant- even if not every participant was able to fully sustain their target heart rate or, by inference, achieve the targeted dose of the neuro-exergame- suggests that even a single bout experienced in a naturalistic way, including such variability, may be potent. In this light, the findings may even be more generalizable to a naturalistic environment wherein such variability would be expected. Nonetheless, the more precise measurement and integration of heart rate data would seem likely to boost the significance in future studies. Future trials should include a more reliable system, such as using an axial heart rate system measurement, that can be integrated with the Apple iOS platform to measure adequate vitals throughout the exercise session.
While this study yielded promising findings, some additional limitations might have affected the results. A larger sample size would help to increase the statistical power, identify any outliers and smaller effects, and improve the generalizability of the results when there is a more diverse group that allows for better analysis of the covariates (age, gender, race, education, etc.). Another weakness was that the most common cognitive measure to evaluate the participants for MCI across subsamples was the MoCA, already noted above as a brief screening tool. Additional testing to discern the type and degree of MCI and more specific cognitive challenges could be useful in elucidating more specific benefits or areas for the adaptation of this intervention (e.g., amnestic MCI (aMCI), wherein memory deficits predominate). Future studies should include a breadth of neuropsychological measures to better characterize the patients and a larger sample to allow sufficient additional categorization. Additionally, future studies should pursue a detailed analyses to determine whether there is variability in changes in executive function and salivary markers in response to pedal-n-play exercise as with iPACES. In addition, data regarding the forward/backward learning task in iPACES that targets executive function were not recorded; therefore, future research should quantify these data. This pursuit will provide further insight into the cognitive functioning of the participants, such as how long a word list one can recall in a single-bout session, how many attempts are required for a participant to finish the minimum word list, whether they ever reach maximum word list, and the time taken. Moreover, the participants in this study were primarily European Americans with a generally high level of education and socioeconomic status, so further research must include a more diverse sample, which will help to clarify how iPACES is effective over a broader group of individuals. Furthermore, the limitations of the equipment do not yet allow for the customization of iPACES, and some older adults experienced difficulties with the apparatus and could not fulfill the expected length of the intervention. Future research studies must include various setups with the equipment that allow for adaptability to the participants, which will allow them to perform the intervention in suitable conditions and achieve the full potential of the intervention.
The iPACES exergame has great potential for future use in delaying cognitive decline for MCI patients. While there are pharmacological options to treat cognitive decline, behavioral interventions are an alternative that will revolutionize the treatment of Alzheimer’s disease. Future research should explore the effectiveness of the neuro-exergaming in both short-term and long-term settings and illustrate the neuropsychological and neurobiological outcomes of the intervention. The long-term goal of the iPACES platform is to understand the target amount of neuro-exergaming needed to provide substantial cognitive improvements. The overarching goal of this research should be to uncover and model the exercise-induced neurobiological mechanisms that lead to neural growth, because this would allow clinicians to understand which biological markers to identify when treating the cognitive decline. Future research using the iPACES platform should be undertaken in conjunction with imaging or another form of neurobiological marker measurement, because this would allow for the identification of additional biomarkers indicative of cognitive improvements. The field of non-invasive treatments for the cognitive decline associated with Alzheimer’s disease is growing, and research must continue to clarify the effects of novel behavioral interventions among the MCI population. Ultimately, this may lead to accrued evidence that would encourage clinicians to use behavioral interventions to help ameliorate cognitive impairment.
5. Conclusions
This partial replication and extension study revealed that a single bout of a neuro-exergame can induce cognitive improvements and biomarker changes in patients with mild cognitive impairment. Significant increases in biomarkers such as salivary alpha-amylase suggest that this type of exercise can activate neurobiological mechanisms that, in other research, have been linked to neurogenesis, thus providing an indication of a linking mechanism. The improvement in executive function is encouraging and suggests exercise-induced benefits to neurological function. While each of these findings is not entirely new (e.g., the cognitive benefits of exercise are well established, and biomarkers as a possible mechanism are increasingly being revealed [12]), this study provides encouraging new evidence at the intersection of these fields of investigation and takes the research a step further. Older adults, including those with MCI, may obtain a cognitive benefit from an exercise paradigm that is tailored to target a specific cognitive function through an interactive experience, such as executive function, as prospectively designed in iPACES. Furthermore, this may be done more conveniently than in previous protocols, using a simple, portable, and cost-effective exercise intervention that can be implemented in-home for older adults. Interventions such as the iPACES neuro-exergame need additional longer-term investigation to verify that they can be utilized, and further adapted and refined, as a meaningful intervention to curb cognitive decline in patients with prodromal Alzheimer’s disease or related dementias.
Author Contributions
Conceptualization: K.N., A.P., K.W., J.S., B.C. and C.A.-H.; methodology: K.N., A.P., K.W., J.S., B.C. and C.A.-H.; formal analysis: K.N., A.P., K.W., J.S., B.C. and C.A.-H.; investigation: K.N., A.P., K.W., J.S. and I.F.; resources: S.C., C.S., B.C. and C.A.-H.; data curation: K.N., A.P., K.W., J.S., B.C. and C.A.-H.; writing—original draft preparation: K.N., A.P., K.W., J.S. and C.A.-H.; writing—review and editing: K.N., A.P., K.W., J.S., I.F. and C.A.-H.; visualization: K.N.; supervision: S.C., C.S., B.C. and C.A.-H.; project administration: S.C., C.S., B.C. and C.A.-H.; funding acquisition: K.N., A.P., K.W., J.S. and C.A.-H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by student and faculty research grants from Union College, NY, and Grant R15AG042109 from the National Institute on Aging.
Institutional Review Board Statement
This study was conducted in accordance with Union College’s Human Subjects Review Committee.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. Results were previously presented at the Annual Meeting of the Eastern Psychological Association in 2020. The following is the citation. “Nath, K., Puleio, A., Michielli, M., Voelm, C., Alberts, K., Wall, K., Duff, A., Hanley, C., Rogers, C., Cohen, B. & Anderson-Hanley, C. (2020). Biomarker and cognitive improvements after a single bout of Interactive Cognitive and Physical Exercise (iPACES v2.75): Results of a multi-site pilot study” [175].
Acknowledgments
Michela Michielli, Carli Voellm, Kylie Alberts, Sarah McErlean, Adelaide Graham, Autumn Duff, Ciara Hanley. Special thanks to all participants from Kingsway, Prestwick Chase, Schaffer Heights, and Union College’s Adult Lifelong Learning (UCALL).
Conflicts of Interest
The research herein was conducted as part of student theses (A.P., J.S., K.W.) and summer research projects (A.P., K.N.) funded by Union College student and faculty research grants and the Beckman Foundation’s Scholar Program (K.N., C.A.H.), and conducted through the Healthy Aging and Neuropsychology Lab at Union College under the mentorship of C.A.H. The funders had no role in the design of the study (e.g., in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results). This research (including design, data collection, analysis, and write-up) was largely completed prior to the NIA grant (R44 AG071063), which is funding follow-up research conducted by the spin-off, pre-revenue/pre-investment company, iPACES LLC. Subsequent to the research reported herein, K.N. and I.F. later worked as NIA-grant-funded research assistants for the company. C.A.H. is on the faculty at Union College and the inventor of the iPACES patent owned by Union College, where the game was created, which is now licensed to the company, where C.A.H. is also lead PI and part owner.
References
- Kirova, A.-M.; Bays, R.B.; Lagalwar, S. Working Memory and Executive Function Decline across Normal Aging, Mild Cognitive Impairment, and Alzheimer’s Disease. BioMed Res. Int. 2015, 2015, 748212. [Google Scholar] [CrossRef] [PubMed]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T.; et al. Estimation of the Global Prevalence of Dementia in 2019 and Forecasted Prevalence in 2050: An Analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Hansen, R.A.; Gartlehner, G.; Lohr, K.N.; Kaufer, D.I. Functional Outcomes of Drug Treatment in Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Drugs Aging 2007, 24, 155–167. [Google Scholar] [CrossRef]
- Ahlskog, J.E.; Geda, Y.E.; Graff-Radford, N.R.; Petersen, R.C. Physical Exercise as a Preventive or Disease-Modifying Treatment of Dementia and Brain Aging. Mayo Clin. Proc. 2011, 86, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Schneider, L.S.; Mangialasche, F.; Andreasen, N.; Feldman, H.; Giacobini, E.; Jones, R.; Mantua, V.; Mecocci, P.; Pani, L.; Winblad, B.; et al. Clinical Trials and Late-Stage Drug Development for Alzheimer’s Disease: An Appraisal from 1984 to 2014. J. Intern. Med. 2014, 275, 251–283. [Google Scholar] [CrossRef]
- Korczyn, A.D.; Vakhapova, V. The Prevention of the Dementia Epidemic. J. Neurol. Sci. 2007, 257, 2–4. [Google Scholar] [CrossRef]
- Larson, E.B. Prospects for Delaying the Rising Tide of Worldwide, Late-Life Dementias. Int. Psychogeriatr. 2010, 22, 1196–1202. [Google Scholar] [CrossRef]
- Brookmeyer, R.; Johnson, E.; Ziegler-Graham, K.; Arrighi, H.M. Forecasting the Global Burden of Alzheimer’s Disease. Alzheimer’s Dement. 2007, 3, 186–191. [Google Scholar] [CrossRef]
- Heyn, P.; Abreu, B.C.; Ottenbacher, K.J. The Effects of Exercise Training on Elderly Persons with Cognitive Impairment and Dementia: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2004, 85, 1694–1704. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be Smart, Exercise Your Heart: Exercise Effects on Brain and Cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Kramer, A.F.; Colcombe, S. Fitness Effects on the Cognitive Function of Older Adults: A Meta-Analytic Study—Revisited. Perspect. Psychol. Sci. 2018, 13, 213–217. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical Activity and Public Health in Older Adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sport. Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef]
- Read, J.L.; Shortell, S.M. Interactive Games to Promote Behavior Change in Prevention and Treatment. JAMA 2011, 305, 1704. [Google Scholar] [CrossRef]
- Wall, K.; Stark, J.; Schillaci, A.; Saulnier, E.; McLaren, E.; Striegnitz, K.; Cohen, B.; Arciero, P.; Kramer, A.; Anderson-Hanley, C. The Enhanced Interactive Physical and Cognitive Exercise System (iPACESTM v2.0): Pilot Clinical Trial of an In-Home IPad-Based Neuro-Exergame for Mild Cognitive Impairment (MCI). J. Clin. Med. 2018, 7, 249. [Google Scholar] [CrossRef]
- Cui, M.Y.; Lin, Y.; Sheng, J.Y.; Zhang, X.; Cui, R.J. Exercise Intervention Associated with Cognitive Improvement in Alzheimer’s Disease. Neural Plast. 2018, 2018, 9234105. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Maloney, M.; Barcelos, N.; Striegnitz, K.; Kramer, A. Neuropsychological Benefits of Neuro-Exergaming for Older Adults: A Pilot Study of an Interactive Physical and Cognitive Exercise System (IPACES). J. Aging Phys. Act. 2017, 25, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.; Kramer, A.F. Fitness Effects on the Cognitive Function of Older Adults: A Meta-Analytic Study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Rathore, A.; Lom, B. The Effects of Chronic and Acute Physical Activity on Working Memory Performance in Healthy Participants: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Syst. Rev. 2017, 6, 124. [Google Scholar] [CrossRef] [PubMed]
- Biazus-Sehn, L.F.; Schuch, F.B.; Firth, J.; de Souza Stigger, F. Effects of Physical Exercise on Cognitive Function of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Arch. Gerontol. Geriatr. 2020, 89, 104048. [Google Scholar] [CrossRef]
- Chen, F.-T.; Etnier, J.L.; Chan, K.-H.; Chiu, P.-K.; Hung, T.-M.; Chang, Y.-K. Effects of Exercise Training Interventions on Executive Function in Older Adults: A Systematic Review and Meta-Analysis. Sport. Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef]
- Diamond, A.; Ling, D.S. Aerobic-Exercise and Resistance-Training Interventions Have Been among the Least Effective Ways to Improve Executive Functions of Any Method Tried Thus Far. Dev. Cogn. Neurosci. 2019, 37, 100572. [Google Scholar] [CrossRef] [PubMed]
- Gasquoine, P.G.; Chen, P.-Y. Effect of Physical Exercise on Popular Measures of Executive Function in Older, Nonclinical, Participants of Randomized Controlled Trials: A Meta-Analytic Review. Appl. Neuropsychol. Adult 2022, 29, 203–211. [Google Scholar] [CrossRef]
- De Souto Barreto, P.; Demougeot, L.; Vellas, B.; Rolland, Y. Exercise Training for Preventing Dementia, Mild Cognitive Impairment, and Clinically Meaningful Cognitive Decline: A Systematic Review and Meta-Analysis. J. Gerontol. Ser. A 2018, 73, 1504–1511. [Google Scholar] [CrossRef]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise Programs for People with Dementia. Cochrane Database Syst. Rev. 2015, 2015, CD006489. [Google Scholar] [CrossRef]
- Young, J.; Angevaren, M.; Rusted, J.; Tabet, N. Aerobic Exercise to Improve Cognitive Function in Older People without Known Cognitive Impairment. Cochrane Database Syst. Rev. 2015, 2015, CD005381. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.F.; Hahn, S.; Cohen, N.J.; Banich, M.T.; McAuley, E.; Harrison, C.R.; Chason, J.; Vakil, E.; Bardell, L.; Boileau, R.A.; et al. Ageing, Fitness and Neurocognitive Function. Nature 1999, 400, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Carlson, M.C.; Fillit, H.; Greenough, W.T.; Kramer, A.; Rebok, G.W. From Bedside to Bench: Does Mental and Physical Activity Promote Cognitive Vitality in Late Life? Sci. Aging Knowl. Environ. 2006, 2006, pe21. [Google Scholar] [CrossRef]
- Angevaren, M.; Aufdemkampe, G.; Verhaar, H.J.J.; Aleman, A.; Vanhees, L. Physical Activity and Enhanced Fitness to Improve Cognitive Function in Older People without Known Cognitive Impairment. Cochrane Database Syst. Rev. 2008, 2008, CD005381. [Google Scholar] [CrossRef]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of Aerobic Exercise on Mild Cognitive Impairment: A Controlled Trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef]
- Geda, Y.E.; Roberts, R.O.; Knopman, D.S.; Christianson, T.J.H.; Pankratz, V.S.; Ivnik, R.J.; Boeve, B.F.; Tangalos, E.G.; Petersen, R.C.; Rocca, W.A. Physical Exercise, Aging, and Mild Cognitive Impairment: A Population-Based Study. Arch. Neurol. 2010, 67, 80–86. [Google Scholar] [CrossRef]
- Martin, M.; Clare, L.; Altgassen, A.M.; Cameron, M.H.; Zehnder, F. Cognition-Based Interventions for Healthy Older People and People with Mild Cognitive Impairment. Cochrane Database Syst. Rev. 2011, 2011, CD006220. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic Exercise Ameliorates Cognitive Function in Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Br. J. Sport Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Song, D.; Yu, D.S.F.; Li, P.W.C.; Lei, Y. The Effectiveness of Physical Exercise on Cognitive and Psychological Outcomes in Individuals with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2018, 79, 155–164. [Google Scholar] [CrossRef]
- Hess, N.C.; Dieberg, G.; McFarlane, J.R.; Smart, N.A. The Effect of Exercise Intervention on Cognitive Performance in Persons at Risk of, or with, Dementia: A Systematic Review and Meta-Analysis. Healthy Aging Res. 2014, 3, 3. [Google Scholar]
- Mistridis, P.; Krumm, S.; Monsch, A.U.; Berres, M.; Taylor, K.I. The 12 Years Preceding Mild Cognitive Impairment Due to Alzheimer’s Disease: The Temporal Emergence of Cognitive Decline. J. Alzheimer’s Dis. 2015, 48, 1095–1107. [Google Scholar] [CrossRef]
- Meng, Q.; Lin, M.-S.; Tzeng, I.-S. Relationship between Exercise and Alzheimer’s Disease: A Narrative Literature Review. Front. Neurosci. 2020, 14, 131. [Google Scholar] [CrossRef]
- Kramer, A.F.; Erickson, K.I. Capitalizing on Cortical Plasticity: Influence of Physical Activity on Cognition and Brain Function. Trends Cogn. Sci. 2007, 11, 342–348. [Google Scholar] [CrossRef]
- Teixeira, C.V.L.; Rezende, T.J.; Weiler, M.; Nogueira, M.H.; Campos, B.M.; Pegoraro, L.F.; Vicentini, J.E.; Scriptore, G.; Cendes, F.; Balthazar, M.L. Relation between Aerobic Fitness and Brain Structures in Amnestic Mild Cognitive Impairment Elderly. Age 2016, 38, 51. [Google Scholar] [CrossRef][Green Version]
- Gates, N.; Fiatarone Singh, M.A.; Sachdev, P.S.; Valenzuela, M. The Effect of Exercise Training on Cognitive Function in Older Adults with Mild Cognitive Impairment: A Meta-Analysis of Randomized Controlled Trials. Am. J. Geriatr. Psychiatry 2013, 21, 1086–1097. [Google Scholar] [CrossRef] [PubMed]
- Ludyga, S.; Gerber, M.; Brand, S.; Holsboer-Trachsler, E.; Pühse, U. Acute Effects of Moderate Aerobic Exercise on Specific Aspects of Executive Function in Different Age and Fitness Groups: A Meta-Analysis: Moderate Exercise and Executive Function. Psychophysiology 2016, 53, 1611–1626. [Google Scholar] [CrossRef]
- Liang, J.-H.; Xu, Y.; Lin, L.; Jia, R.-X.; Zhang, H.-B.; Hang, L. Comparison of Multiple Interventions for Older Adults with Alzheimer Disease or Mild Cognitive Impairment. Medicine 2018, 97, e10744. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F.; et al. Exergaming and Older Adult Cognition. Am. J. Prev. Med. 2012, 42, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The Aerobic and Cognitive Exercise Study (ACES) for Community-Dwelling Older Adults with or At-Risk for Mild Cognitive Impairment (MCI): Neuropsychological, Neurobiological and Neuroimaging Outcomes of a Randomized Clinical Trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.-A. Exercise Builds Brain Health: Key Roles of Growth Factor Cascades and Inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef]
- Van Praag, H.; Kempermann, G.; Gage, F.H. Neural Consequences of Environmental Enrichment. Nat. Rev. Neurosci. 2000, 1, 191–198. [Google Scholar] [CrossRef]
- Van Praag, H.; Shubert, T.; Zhao, C.; Gage, F.H. Exercise Enhances Learning and Hippocampal Neurogenesis in Aged Mice. J. Neurosci. 2005, 25, 8680–8685. [Google Scholar] [CrossRef] [PubMed]
- Van Praag, H. Neurogenesis and Exercise: Past and Future Directions. Neuromol. Med. 2008, 10, 128–140. [Google Scholar] [CrossRef]
- Suo, C.; Singh, M.F.; Gates, N.; Wen, W.; Sachdev, P.; Brodaty, H.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Singh, N.; et al. Therapeutically Relevant Structural and Functional Mechanisms Triggered by Physical and Cognitive Exercise. Mol. Psychiatry 2016, 21, 1633–1642. [Google Scholar] [CrossRef]
- Kirk-Sanchez, N.; McGough, E. Physical Exercise and Cognitive Performance in the Elderly: Current Perspectives. Clin. Interv. Aging 2013, 9, 51–62. [Google Scholar] [CrossRef]
- Rasmussen, P.; Brassard, P.; Adser, H.; Pedersen, M.V.; Leick, L.; Hart, E.; Secher, N.H.; Pedersen, B.K.; Pilegaard, H. Evidence for a Release of Brain-Derived Neurotrophic Factor from the Brain during Exercise: Brain-Derived Neurotrophic Factor Release during Exercise. Exp. Physiol. 2009, 94, 1062–1069. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice Guideline Update Summary: Mild Cognitive Impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Papp, K.V.; Walsh, S.J.; Snyder, P.J. Immediate and Delayed Effects of Cognitive Interventions in Healthy Elderly: A Review of Current Literature and Future Directions. Alzheimer’s Dement. 2009, 5, 50–60. [Google Scholar] [CrossRef]
- Anguera, J.A.; Boccanfuso, J.; Rintoul, J.L.; Al-Hashimi, O.; Faraji, F.; Janowich, J.; Kong, E.; Larraburo, Y.; Rolle, C.; Johnston, E.; et al. Video Game Training Enhances Cognitive Control in Older Adults. Nature 2013, 501, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Li, K.Z.H.; Lindenberger, U.; Freund, A.M.; Baltes, P.B. Walking While Memorizing: Age-Related Differences in Compensatory Behavior. Psychol. Sci. 2001, 12, 230–237. [Google Scholar] [CrossRef]
- Toril, P.; Reales, J.M.; Ballesteros, S. Video Game Training Enhances Cognition of Older Adults: A Meta-Analytic Study. Psychol. Aging 2014, 29, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yu, J.-T.; Wang, H.-F.; Tan, C.-C.; Meng, X.-F.; Tan, L. Non-Pharmacological Interventions for Patients with Mild Cognitive Impairment: A Meta-Analysis of Randomized Controlled Trials of Cognition-Based and Exercise Interventions. J. Alzheimer’s Dis. 2014, 42, 663–678. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros, S.; Prieto, A.; Mayas, J.; Toril, P.; Pita, C.; Ponce de León, L.; Reales, J.M.; Waterworth, J. Brain Training with Non-Action Video Games Enhances Aspects of Cognition in Older Adults: A Randomized Controlled Trial. Front. Aging Neurosci. 2014, 6, 277. [Google Scholar] [CrossRef]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S.G. A Review of Physical and Cognitive Interventions in Aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef]
- Corbett, A.; Owen, A.; Hampshire, A.; Grahn, J.; Stenton, R.; Dajani, S.; Burns, A.; Howard, R.; Williams, N.; Williams, G.; et al. The Effect of an Online Cognitive Training Package in Healthy Older Adults: An Online Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2015, 16, 990–997. [Google Scholar] [CrossRef]
- Mowszowski, L.; Lampit, A.; Walton, C.C.; Naismith, S.L. Strategy-Based Cognitive Training for Improving Executive Functions in Older Adults: A Systematic Review. Neuropsychol. Rev. 2016, 26, 252–270. [Google Scholar] [CrossRef]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive Training and Cognitive Rehabilitation for Persons with Mild to Moderate Dementia of the Alzheimer’s or Vascular Type: A Review. Alzheimers Res. 2013, 5, 35. [Google Scholar] [CrossRef]
- Simons, D.J.; Boot, W.R.; Charness, N.; Gathercole, S.E.; Chabris, C.F.; Hambrick, D.Z.; Stine-Morrow, E.A.L. Do “Brain-Training” Programs Work? Psychol. Sci. Public Interest 2016, 17, 103–186. [Google Scholar] [CrossRef] [PubMed]
- Reijnders, J.; van Heugten, C.; van Boxtel, M. Cognitive Interventions in Healthy Older Adults and People with Mild Cognitive Impairment: A Systematic Review. Ageing Res. Rev. 2013, 12, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Willis, S.L.; Tennstedt, S.L.; Marsiske, M.; Ball, K.; Elias, J.; Koepke, K.M.; Morris, J.N.; Rebok, G.W.; Unverzagt, F.W.; Stoddard, A.M.; et al. Long-Term Effects of Cognitive Training on Everyday Functional Outcomes in Older Adults. JAMA 2006, 296, 2805. [Google Scholar] [CrossRef]
- Karr, J.E.; Areshenkoff, C.N.; Rast, P.; Garcia-Barrera, M.A. An Empirical Comparison of the Therapeutic Benefits of Physical Exercise and Cognitive Training on the Executive Functions of Older Adults: A Meta-Analysis of Controlled Trials. Neuropsychology 2014, 28, 829–845. [Google Scholar] [CrossRef]
- Huntley, J.D.; Gould, R.L.; Liu, K.; Smith, M.; Howard, R.J. Do Cognitive Interventions Improve General Cognition in Dementia? A Meta-Analysis and Meta-Regression. BMJ Open 2015, 5, e005247. [Google Scholar] [CrossRef]
- Owen, A.M.; Hampshire, A.; Grahn, J.A.; Stenton, R.; Dajani, S.; Burns, A.S.; Howard, R.J.; Ballard, C.G. Putting Brain Training to the Test. Nature 2010, 465, 775–778. [Google Scholar] [CrossRef]
- Van Muijden, J.; Band, G.P.H.; Hommel, B. Online Games Training Aging Brains: Limited Transfer to Cognitive Control Functions. Front. Hum. Neurosci. 2012, 6, 221. [Google Scholar] [CrossRef]
- Redick, T.S.; Shipstead, Z.; Harrison, T.L.; Hicks, K.L.; Fried, D.E.; Hambrick, D.Z.; Kane, M.J.; Engle, R.W. No Evidence of Intelligence Improvement after Working Memory Training: A Randomized, Placebo-Controlled Study. J. Exp. Psychol. Gen. 2013, 142, 359–379. [Google Scholar] [CrossRef]
- Boot, W.R.; Kramer, A.F. The Brain-Games Conundrum: Does Cognitive Training Really Sharpen the Mind? Cerebrum 2014, 2014, 15. [Google Scholar]
- Zokaei, N.; MacKellar, C.; Čepukaitytė, G.; Patai, E.Z.; Nobre, A.C. Cognitive Training in the Elderly: Bottlenecks and New Avenues. J. Cogn. Neurosci. 2017, 29, 1473–1482. [Google Scholar] [CrossRef]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical Activity to Improve Cognition in Older Adults: Can Physical Activity Programs Enriched with Cognitive Challenges Enhance the Effects? A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act 2018, 15, 63. [Google Scholar] [CrossRef]
- Constans, A.; Pin-barre, C.; Temprado, J.-J.; Decherchi, P.; Laurin, J. Influence of Aerobic Training and Combinations of Interventions on Cognition and Neuroplasticity after Stroke. Front. Aging Neurosci. 2016, 8, 164. [Google Scholar] [CrossRef]
- Diamond, A. Effects of Physical Exercise on Executive Functions: Going beyond Simply Moving to Moving with Thought. Ann. Sport. Med. Res. 2015, 2, 1011. [Google Scholar]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The More the Better? A Meta-Analysis on Effects of Combined Cognitive and Physical Intervention on Cognition in Healthy Older Adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Geda, Y.E.; Silber, T.C.; Roberts, R.O.; Knopman, D.S.; Christianson, T.J.H.; Pankratz, V.S.; Boeve, B.F.; Tangalos, E.G.; Petersen, R.C. Computer Activities, Physical Exercise, Aging, and Mild Cognitive Impairment: A Population-Based Study. Mayo Clin. Proc. 2012, 87, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.; Verdile, G.; Sohrabi, H.; Campbell, A.; Putland, E.; Cheetham, C.; Dhaliwal, S.; Weinborn, M.; Maruff, P.; Darby, D.; et al. A Combination of Physical Activity and Computerized Brain Training Improves Verbal Memory and Increases Cerebral Glucose Metabolism in the Elderly. Transl. Psychiatry 2014, 4, e487. [Google Scholar] [CrossRef]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive Effects of Combined Cognitive and Physical Exercise Training on Cognitive Function in Older Adults with Mild Cognitive Impairment or Dementia: A Meta-Analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef]
- Styliadis, C.; Kartsidis, P.; Paraskevopoulos, E.; Ioannides, A.A.; Bamidis, P.D. Neuroplastic Effects of Combined Computerized Physical and Cognitive Training in Elderly Individuals at Risk for Dementia: An ELORETA Controlled Study on Resting States. Neural Plast. 2015, 2015, 172192. [Google Scholar] [CrossRef]
- Edwards, M.; Loprinzi, P. Experimental Effects of Acute Exercise and Meditation on Parameters of Cognitive Function. J. Clin. Med. 2018, 7, 125. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros, S.; Voelcker-Rehage, C.; Bherer, L. Editorial: Cognitive and Brain Plasticity Induced by Physical Exercise, Cognitive Training, Video Games, and Combined Interventions. Front. Hum. Neurosci. 2018, 12, 169. [Google Scholar] [CrossRef] [PubMed]
- Barnes, D.E.; Santos-Modesitt, W.; Poelke, G.; Kramer, A.F.; Castro, C.; Middleton, L.E.; Yaffe, K. The Mental Activity and Exercise (MAX) Trial. JAMA Intern. Med. 2013, 173, 797. [Google Scholar] [CrossRef]
- Fiatarone Singh, M.A.; Gates, N.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. The Study of Mental and Resistance Training (SMART) Study—Resistance Training and/or Cognitive Training in Mild Cognitive Impairment: A Randomized, Double-Blind, Double-Sham Controlled Trial. J. Am. Med. Dir. Assoc. 2014, 15, 873–880. [Google Scholar] [CrossRef]
- Law, L.L.F.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of Combined Cognitive and Exercise Interventions on Cognition in Older Adults with and without Cognitive Impairment: A Systematic Review. Ageing Res. Rev. 2014, 15, 61–75. [Google Scholar] [CrossRef]
- Rahe, J.; Becker, J.; Fink, G.R.; Kessler, J.; Kukolja, J.; Rahn, A.; Rosen, J.B.; Szabados, F.; Wirth, B.; Kalbe, E. Cognitive Training with and without Additional Physical Activity in Healthy Older Adults: Cognitive Effects, Neurobiological Mechanisms, and Prediction of Training Success. Front. Aging Neurosci. 2015, 7, 187. [Google Scholar] [CrossRef] [PubMed]
- Lipardo, D.S.; Aseron, A.M.C.; Kwan, M.M.; Tsang, W.W. Effect of Exercise and Cognitive Training on Falls and Fall-Related Factors in Older Adults with Mild Cognitive Impairment: A Systematic Review. Arch. Phys. Med. Rehabil. 2017, 98, 2079–2096. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, S.; Schumacher, V. The Interplay between Cognitive and Motor Functioning in Healthy Older Adults: Findings from Dual-Task Studies and Suggestions for Intervention. Gerontology 2011, 57, 239–246. [Google Scholar] [CrossRef]
- De Coelho, F.G.M.; Andrade, L.P.; Pedroso, R.V.; Santos-Galduroz, R.F.; Gobbi, S.; Costa, J.L.R.; Gobbi, L.T.B. Multimodal Exercise Intervention Improves Frontal Cognitive Functions and Gait in Alzheimer’s Disease: A Controlled Trial: Exercise, Cognitive Functions and Gait. Geriatr. Gerontol. Int. 2013, 13, 198–203. [Google Scholar] [CrossRef]
- Forte, R.; Boreham, C.; Leite, J.; De Vito, G.; Brennan, L.; Gibney, E.; Pesce, C. Enhancing Cognitive Functioning in the Elderly: Multicomponent vs Resistance Training. Clin. Interv. Aging 2013, 2013, 19–27. [Google Scholar] [CrossRef]
- Theill, N.; Schumacher, V.; Adelsberger, R.; Martin, M.; Jäncke, L. Effects of Simultaneously Performed Cognitive and Physical Training in Older Adults. BMC Neurosci. 2013, 14, 103. [Google Scholar] [CrossRef]
- Bherer, L. Cognitive Plasticity in Older Adults: Effects of Cognitive Training and Physical Exercise: Cognitive Plasticity in Older Adults. Ann. N. Y. Acad. Sci. 2015, 1337, 12682. [Google Scholar] [CrossRef]
- Eggenberger, P.; Wolf, M.; Schumann, M.; de Bruin, E.D. Exergame and Balance Training Modulate Prefrontal Brain Activity during Walking and Enhance Executive Function in Older Adults. Front. Aging Neurosci. 2016, 8, 66. [Google Scholar] [CrossRef]
- Yokoyama, H.; Okazaki, K.; Imai, D.; Yamashina, Y.; Takeda, R.; Naghavi, N.; Ota, A.; Hirasawa, Y.; Miyagawa, T. The Effect of Cognitive-Motor Dual-Task Training on Cognitive Function and Plasma Amyloid β Peptide 42/40 Ratio in Healthy Elderly Persons: A Randomized Controlled Trial. BMC Geriatr. 2015, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Desjardins-Crepeau, L.; Berryman, N.; Fraser, S.; Vu, T.T.M.; Kergoat, M.-J.; Li, K.; Bosquet, L.; Bherer, L. Effects of Combined Physical and Cognitive Training on Fitness and Neuropsychological Outcomes in Healthy Older Adults. Clin. Interv. Aging 2016, 11, 1287–1299. [Google Scholar] [CrossRef]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of Interactive Physical-Activity Video-Game Training on Physical and Cognitive Function in Older Adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef]
- González-Palau, F.; Franco, M.; Bamidis, P.; Losada, R.; Parra, E.; Papageorgiou, S.G.; Vivas, A.B. The Effects of a Computer-Based Cognitive and Physical Training Program in a Healthy and Mildly Cognitive Impaired Aging Sample. Aging Ment. Health 2014, 18, 838–846. [Google Scholar] [CrossRef]
- Schoene, D.; Valenzuela, T.; Lord, S.R.; de Bruin, E.D. The Effect of Interactive Cognitive-Motor Training in Reducing Fall Risk in Older People: A Systematic Review. BMC Geriatr. 2014, 14, 107. [Google Scholar] [CrossRef] [PubMed]
- Bamidis, P.D.; Fissler, P.; Papageorgiou, S.G.; Zilidou, V.; Konstantinidis, E.I.; Billis, A.S.; Romanopoulou, E.; Karagianni, M.; Beratis, I.; Tsapanou, A.; et al. Gains in Cognition through Combined Cognitive and Physical Training: The Role of Training Dosage and Severity of Neurocognitive Disorder. Front. Aging Neurosci. 2015, 7, 152. [Google Scholar] [CrossRef]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of Combined Physical and Cognitive Training on Cognition: A Systematic Review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Liu, H.-H.; Zhu, X.-T.; Meng, T.; Li, H.-J.; Zuo, X.-N. Action Video Game Training for Healthy Adults: A Meta-Analytic Study. Front. Psychol. 2016, 7, 907. [Google Scholar] [CrossRef]
- Stanmore, E.; Stubbs, B.; Vancampfort, D.; de Bruin, E.D.; Firth, J. The Effect of Active Video Games on Cognitive Functioning in Clinical and Non-Clinical Populations: A Meta-Analysis of Randomized Controlled Trials. Neurosci. Biobehav. Rev. 2017, 78, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Stark, J.; Wall, K.M.; VanBrakle, M.; Michel, M.; Maloney, M.; Barcelos, N.; Striegnitz, K.; Cohen, B.; Kramer, A.F. The Interactive Physical and Cognitive Exercise System (IPACES™): Effects of a 3-Month in-Home Pilot Clinical Trial for Mild Cognitive Impairment and Caregivers. Clin. Interv. Aging 2018, 13, 1565–1577. [Google Scholar] [CrossRef] [PubMed]
- Bruderer-Hofstetter, M.; Rausch-Osthoff, A.-K.; Meichtry, A.; Münzer, T.; Niedermann, K. Effective Multicomponent Interventions in Comparison to Active Control and No Interventions on Physical Capacity, Cognitive Function and Instrumental Activities of Daily Living in Elderly People with and without Mild Impaired Cognition—A Systematic Review and Network Meta-Analysis. Ageing Res. Rev. 2018, 45, 1–14. [Google Scholar] [CrossRef]
- Joubert, C.; Chainay, H. Aging Brain: The Effect of Combined Cognitive and Physical Training on Cognition as Compared to Cognitive and Physical Training Alone—A Systematic Review. Clin. Interv. Aging 2018, 13, 1267–1301. [Google Scholar] [CrossRef]
- Van het Reve, E.; de Bruin, E.D. Strength-Balance Supplemented with Computerized Cognitive Training to Improve Dual Task Gait and Divided Attention in Older Adults: A Multicenter Randomized-Controlled Trial. BMC Geriatr. 2014, 14, 134. [Google Scholar] [CrossRef] [PubMed]
- Hiyamizu, M.; Morioka, S.; Shomoto, K.; Shimada, T. Effects of Dual Task Balance Training on Dual Task Performance in Elderly People: A Randomized Controlled Trial. Clin. Rehabil. 2012, 26, 58–67. [Google Scholar] [CrossRef]
- Kayama, H.; Okamoto, K.; Nishiguchi, S.; Yamada, M.; Kuroda, T.; Aoyama, T. Effect of a Kinect-Based Exercise Game on Improving Executive Cognitive Performance in Community-Dwelling Elderly: Case Control Study. J. Med. Internet Res. 2014, 16, e61. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, N.; Shah, N.; Cohen, K.; Hogan, M.J.; Mulkerrin, E.; Arciero, P.J.; Cohen, B.D.; Kramer, A.F.; Anderson-Hanley, C. Aerobic and Cognitive Exercise (ACE) Pilot Study for Older Adults: Executive Function Improves with Cognitive Challenge While Exergaming. J. Int. Neuropsychol. Soc. 2015, 21, 768–779. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Tanigawa, T.; Sekiyama, K.; Kawagoe, T.; Suzuki, M.; Yoshikawa, S.; Abe, N.; Otsuka, Y.; Nakai, R.; et al. A 12-Week Physical and Cognitive Exercise Program Can Improve Cognitive Function and Neural Efficiency in Community-Dwelling Older Adults: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1355–1363. [Google Scholar] [CrossRef]
- León, J.; Ureña, A.; Bolaños, M.J.; Bilbao, A.; Oña, A. A Combination of Physical and Cognitive Exercise Improves Reaction Time in Persons 61–84 Years Old. J. Aging Phys. Act. 2015, 23, 72–77. [Google Scholar] [CrossRef]
- Smith, G.E. Healthy Cognitive Aging and Dementia Prevention. Am. Psychol. 2016, 71, 268–275. [Google Scholar] [CrossRef]
- Barry, G.; Galna, B.; Rochester, L. The Role of Exergaming in Parkinson’s Disease Rehabilitation: A Systematic Review of the Evidence. J. NeuroEng. Rehabil. 2014, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.-Y.; Scherer, Y.K.; Montgomery, C.A. Effects of Using Nintendo Wii™ Exergames in Older Adults: A Review of the Literature. J. Aging Health 2015, 27, 379–402. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.F.; You, T.; Leveille, S.G. Potential Benefits of Exergaming for Cognition and Dual-Task Function in Older Adults: A Systematic Review. J. Aging Phys. Act. 2016, 24, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Zilidou, V.I.; Konstantinidis, E.I.; Romanopoulou, E.D.; Karagianni, M.; Kartsidis, P.; Bamidis, P.D. Investigating the Effectiveness of Physical Training through Exergames: Focus on Balance and Aerobic Protocols. In Proceedings of the 2016 1st International Conference on Technology and Innovation in Sports, Health and Wellbeing (TISHW), Vila Real, Portugal, 1–3 December 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–6. [Google Scholar] [CrossRef]
- Fissler, P.; Küster, O.; Schlee, W.; Kolassa, I.-T. Novelty Interventions to Enhance Broad Cognitive Abilities and Prevent Dementia. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2013; Volume 207, pp. 403–434. [Google Scholar] [CrossRef]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The Effects of Acute Exercise on Cognitive Performance: A Meta-Analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef]
- Lambourne, K.; Tomporowski, P. The Effect of Exercise-Induced Arousal on Cognitive Task Performance: A Meta-Regression Analysis. Brain Res. 2010, 1341, 12–24. [Google Scholar] [CrossRef]
- Hillman, C.H.; Pontifex, M.B.; Raine, L.B.; Castelli, D.M.; Hall, E.E.; Kramer, A.F. The Effect of Acute Treadmill Walking on Cognitive Control and Academic Achievement in Preadolescent Children. Neuroscience 2009, 159, 1044–1054. [Google Scholar] [CrossRef]
- Nanda, B.; Balde, J.; Manjunatha, S. The Acute Effects of a Single Bout of Moderate-Intensity Aerobic Exercise on Cognitive Functions in Healthy Adult Males. J. Clin. Diagn. Res. JCDR 2013, 7, 1883. [Google Scholar] [CrossRef]
- Kamijo, K.; Hayashi, Y.; Sakai, T.; Yahiro, T.; Tanaka, K.; Nishihira, Y. Acute Effects of Aerobic Exercise on Cognitive Function in Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64B, 356–363. [Google Scholar] [CrossRef]
- Li, L.; Men, W.-W.; Chang, Y.-K.; Fan, M.-X.; Ji, L.; Wei, G.-X. Acute Aerobic Exercise Increases Cortical Activity during Working Memory: A Functional MRI Study in Female College Students. PLoS ONE 2014, 9, e99222. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Roig, M.; Tomporowski, P.D.; Javadi, A.; Kelemen, W.L. Effects of acute exercise on memory: Considerations of exercise intensity, post-exercise recovery period and aerobic endurance. Mem. Cognit. 2023, 51, 1011–1026. [Google Scholar] [CrossRef] [PubMed]
- Labban, J.D.; Etnier, J.L. Effects of acute exercise on long-term memory. Res. Q. Exerc. Sport 2011, 82, 712–721. [Google Scholar] [CrossRef] [PubMed]
- Heath, M.; Shukla, D. A Single Bout of Aerobic Exercise Provides an Immediate “Boost” to Cognitive Flexibility. Front. Psychol. 2020, 11, 1106. [Google Scholar] [CrossRef]
- Tsai, C.-L.; Pai, M.-C.; Ukropec, J.; Ukropcová, B. Distinctive Effects of Aerobic and Resistance Exercise Modes on Neurocognitive and Biochemical Changes in Individuals with Mild Cognitive Impairment. Curr. Alzheimer Res. 2019, 16, 316–332. [Google Scholar] [CrossRef] [PubMed]
- Devenney, K.E.; Guinan, E.M.; Kelly, Á.M.; Mota, B.C.; Walsh, C.; Olde Rikkert, M.; Schneider, S.; Lawlor, B. Acute High-Intensity Aerobic Exercise Affects Brain-Derived Neurotrophic Factor in Mild Cognitive Impairment: A Randomised Controlled Study. BMJ Open Sport Exerc. Med. 2019, 5, e000499. [Google Scholar] [CrossRef]
- Knaepen, K.; Goekint, M.; Heyman, E.M.; Meeusen, R. Neuroplasticity—Exercise-Induced Response of Peripheral Brain-Derived Neurotrophic Factor: A Systematic Review of Experimental Studies in Human Subjects. Sport. Med. 2010, 40, 765–801. [Google Scholar] [CrossRef]
- Leckie, R.L.; Oberlin, L.E.; Voss, M.W.; Prakash, R.S.; Szabo-Reed, A.; Chaddock-Heyman, L.; Phillips, S.M.; Gothe, N.P.; Mailey, E.; Vieira-Potter, V.J.; et al. BDNF Mediates Improvements in Executive Function Following a 1-Year Exercise Intervention. Front. Hum. Neurosci. 2014, 8, 985. [Google Scholar] [CrossRef]
- Vaughan, S.; Wallis, M.; Polit, D.; Steele, M.; Shum, D.; Morris, N. The Effects of Multimodal Exercise on Cognitive and Physical Functioning and Brain-Derived Neurotrophic Factor in Older Women: A Randomised Controlled Trial. Age Ageing 2014, 43, 623–629. [Google Scholar] [CrossRef]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Liu, C.S.; Sherman, C.; Chan, S.; Lanctôt, K.L. The Effect of Exercise Training on Resting Concentrations of Peripheral Brain-Derived Neurotrophic Factor (BDNF): A Meta-Analysis. PLoS ONE 2016, 11, e0163037. [Google Scholar] [CrossRef]
- Maass, A.; Düzel, S.; Brigadski, T.; Goerke, M.; Becke, A.; Sobieray, U.; Neumann, K.; Lövdén, M.; Lindenberger, U.; Bäckman, L.; et al. Relationships of Peripheral IGF-1, VEGF and BDNF Levels to Exercise-Related Changes in Memory, Hippocampal Perfusion and Volumes in Older Adults. NeuroImage 2016, 131, 142–154. [Google Scholar] [CrossRef]
- Canton-Martínez, E.; Rentería, I.; García-Suárez, P.C.; Moncada-Jiménez, J.; Machado-Parra, J.P.; Lira, F.S.; Johnson, D.K.; Jiménez-Maldonado, A. Concurrent Training Increases Serum Brain-Derived Neurotrophic Factor in Older Adults Regardless of the Exercise Frequency. Front. Aging Neurosci. 2022, 14, 791698. [Google Scholar] [CrossRef]
- De Rondão, C.A.M.; Mota, M.P.; Oliveira, M.M.; Peixoto, F.; Esteves, D. Multicomponent Exercise Program Effects on Fitness and Cognitive Function of Elderlies with Mild Cognitive Impairment: Involvement of Oxidative Stress and BDNF. Front. Aging Neurosci. 2022, 14, 950937. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Prakash, R.S.; Erickson, K.I.; Basak, C.; Chaddock, L.; Kim, J.S.; Alves, H.; Heo, S.; Szabo, A.N.; White, S.M.; et al. Plasticity of Brain Networks in a Randomized Intervention Trial of Exercise Training in Older Adults. Front. Aging Neurosci. 2010, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.M.; Peiffer, J.J.; Martins, R.N. Multiple Effects of Physical Activity on Molecular and Cognitive Signs of Brain Aging: Can Exercise Slow Neurodegeneration and Delay Alzheimer’s Disease? Mol. Psychiatry 2013, 18, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.; Baktir, M.A.; Srivatsan, M.; Salehi, A. Neuroprotective Effects of Physical Activity on the Brain: A Closer Look at Trophic Factor Signaling. Front. Cell. Neurosci. 2014, 8, 170. [Google Scholar] [CrossRef] [PubMed]
- Rojas Vega, S.; Knicker, A.; Hollmann, W.; Bloch, W.; Strüder, H.K. Effect of Resistance Exercise on Serum Levels of Growth Factors in Humans. Horm. Metab. Res. 2010, 42, 982–986. [Google Scholar] [CrossRef]
- Bellar, D.; Glickman, E.L.; Juvancic-Heltzel, J.; Gunstad, J. Serum Insulin like Growth Factor-1 Is Associated with Working Memory, Executive Function and Selective Attention in a Sample of Healthy, Fit Older Adults. Neuroscience 2011, 178, 133–137. [Google Scholar] [CrossRef]
- Stein, A.M.; da Silva, T.M.V.; de Coelho, F.G.M.; Rueda, A.V.; Camarini, R.; Galduróz, R.F.S. Acute Exercise Increases Circulating IGF-1 in Alzheimer’s Disease Patients, but Not in Older Adults without Dementia. Behav. Brain Res. 2021, 396, 112903. [Google Scholar] [CrossRef]
- Dik, M.G.; Pluijm, S.M.F.; Jonker, C.; Deeg, D.J.H.; Lomecky, M.Z.; Lips, P. Insulin-like Growth Factor I (IGF-I) and Cognitive Decline in Older Persons. Neurobiol. Aging 2003, 24, 573–581. [Google Scholar] [CrossRef]
- Al-Delaimy, W.K.; Von Muhlen, D.; Barrett-Connor, E. Insulinlike Growth Factor-1, Insulinlike Growth Factor Binding Protein-1, and Cognitive Function in Older Men and Women: IGF-1 and Cognitive Function. J. Am. Geriatr. Soc. 2009, 57, 1441–1446. [Google Scholar] [CrossRef]
- Lara, V.P.; Caramelli, P.; Teixeira, A.L.; Barbosa, M.T.; Carmona, K.C.; Carvalho, M.G.; Fernandes, A.P.; Gomes, K.B. High Cortisol Levels Are Associated with Cognitive Impairment No-Dementia (CIND) and Dementia. Clin. Chim. Acta 2013, 423, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Tortosa-Martínez, J.; Manchado, C.; Cortell-Tormo, J.M.; Chulvi-Medrano, I. Exercise, the Diurnal Cycle of Cortisol and Cognitive Impairment in Older Adults. Neurobiol. Stress 2018, 9, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; Maheu, F.; Tu, M.; Fiocco, A.; Schramek, T.E. The Effects of Stress and Stress Hormones on Human Cognition: Implications for the Field of Brain and Cognition. Brain Cogn. 2007, 65, 209–237. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.; Lange, C.; Huijbers, W. Plasma Cortisol Is Associated with Cerebral Hypometabolism across the Alzheimer’s Disease Spectrum. Neurobiol. Aging 2019, 84, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Kline, S.A.; Mega, M.S. Stress-Induced Neurodegeneration: The Potential for Coping as Neuroprotective Therapy. Am. J. Alzheimers Dis. Other Demen. 2020, 35, 153331752096087. [Google Scholar] [CrossRef]
- Lupien, S.J.; de Leon, M.; de Santi, S.; Convit, A.; Tarshish, C.; Nair, N.P.V.; Thakur, M.; McEwen, B.S.; Hauger, R.L.; Meaney, M.J. Cortisol Levels during Human Aging Predict Hippocampal Atrophy and Memory Deficits. Nat. Neurosci. 1998, 1, 69–73. [Google Scholar] [CrossRef]
- Lupien, S.J.; Nair, N.P.V.; Briére, S.; Maheu, F.; Tu, M.T.; Lemay, Μ.; McEwen, B.S.; Meaney, M.J. Increased Cortisol Levels and Impaired Cognition in Human Aging: Implication for Depression and Dementia in Later Life. Rev. Neurosci. 1999, 10, 117–140. [Google Scholar] [CrossRef] [PubMed]
- Csernansky, J.G.; Dong, H.; Fagan, A.M.; Wang, L.; Xiong, C.; Holtzman, D.M.; Morris, J.C. Plasma Cortisol and Progression of Dementia in Subjects with Alzheimer-Type Dementia. Am. J. Psychiatry 2006, 163, 2164–2169. [Google Scholar] [CrossRef]
- Lara, J.; Cooper, R.; Nissan, J.; Ginty, A.T.; Khaw, K.-T.; Deary, I.J.; Lord, J.M.; Kuh, D.; Mathers, J.C. A Proposed Panel of Biomarkers of Healthy Ageing. BMC Med. 2015, 13, 222. [Google Scholar] [CrossRef]
- Antypa, D.; Basta, M.; Vgontzas, A.; Zaganas, I.; Panagiotakis, S.; Vogiatzi, E.; Kokosali, E.; Simos, P. The Association of Basal Cortisol Levels with Episodic Memory in Older Adults Is Mediated by Executive Function. Neurobiol. Learn. Mem. 2022, 190, 107600. [Google Scholar] [CrossRef]
- Tortosa-Martínez, J.; Clow, A.; Caus-Pertegaz, N.; González-Caballero, G.; Abellán-Miralles, I.; Saenz, M.J. Exercise Increases the Dynamics of Diurnal Cortisol Secretion and Executive Function in People with Amnestic Mild Cognitive Impairment. J. Aging Phys. Act. 2015, 23, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Segal, S.K.; Cotman, C.W.; Cahill, L.F. Exercise-Induced Noradrenergic Activation Enhances Memory Consolidation in Both Normal Aging and Patients with Amnestic Mild Cognitive Impairment. J. Alzheimer’s Dis. 2012, 32, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Carson, N.; Leach, L.; Murphy, K.J. A Re-Examination of Montreal Cognitive Assessment (MoCA) Cutoff Scores: Re-Examination of MoCA Cutoff Scores. Int. J. Geriatr. Psychiatry 2018, 33, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Want to Optimize Executive Functions and Academic Outcomes? Simple, Just Nourish the Human Spirit. Minn. Symp. Child Psychol. Ser. 2014, 37, 205–232. [Google Scholar]
- Strauss, E.; Sherman, E.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary, 3rd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Lee, H.; Baniqued, P.L.; Cosman, J.; Mullen, S.; McAuley, E.; Severson, J.; Kramer, A.F. Examining Cognitive Function across the Lifespan Using a Mobile Application. Comput. Hum. Behav. 2012, 28, 1934–1946. [Google Scholar] [CrossRef]
- Van der Elst, W.; Van Boxtel, M.P.J.; Van Breukelen, G.J.P.; Jolles, J. The Stroop Color-Word Test: Influence of Age, Sex, and Education; and Normative Data for a Large Sample Across the Adult Age Range. Assessment 2006, 13, 62–79. [Google Scholar] [CrossRef]
- Ettenhofer, M.L.; Hambrick, D.Z.; Abeles, N. Reliability and Stability of Executive Functioning in Older Adults. Neuropsychology 2006, 20, 607–613. [Google Scholar] [CrossRef]
- Houx, P.J. Testing Cognitive Function in Elderly Populations: The PROSPER Study. J. Neurol. Neurosurg. Psychiatry 2002, 73, 385–389. [Google Scholar] [CrossRef]
- Lesh, T.A.; Westphal, A.J.; Niendam, T.A.; Yoon, J.H.; Minzenberg, M.J.; Ragland, J.D.; Solomon, M.; Carter, C.S. Proactive and Reactive Cognitive Control and Dorsolateral Prefrontal Cortex Dysfunction in First Episode Schizophrenia. NeuroImage Clin. 2013, 2, 590–599. [Google Scholar] [CrossRef]
- Mohs, R.C.; Knopman, D.; Petersen, R.C.; Ferris, S.H.; Ernesto, C.; Grundman, M.; Sano, M.; Bieliauskas, L.; Geldmacher, D.; Clark, C.; et al. Development of Cognitive Instruments for Use in Clinical Trials of Antidementia Drugs: Additions to the Alzheimer’s Disease Assessment Scale That Broaden Its Scope. The Alzheimer’s Disease Cooperative Study. Alzheimer Dis. Assoc. Disord. 1997, 11 (Suppl. S2), S13–S21. [Google Scholar] [CrossRef]
- Harrison, J.; Minassian, S.L.; Jenkins, L.; Black, R.S.; Koller, M.; Grundman, M. A Neuropsychological Test Battery for Use in Alzheimer Disease Clinical Trials. Arch. Neurol. 2007, 64, 1323. [Google Scholar] [CrossRef] [PubMed]
- Podhorna, J.; Krahnke, T.; Shear, M.; Harrison, J.E. for the Alzheimer’s Disease Neuroimaging Initiative. Alzheimer’s Disease Assessment Scale–Cognitive Subscale Variants in Mild Cognitive Impairment and Mild Alzheimer’s Disease: Change over Time and the Effect of Enrichment Strategies. Alzheimer’s Res. Ther. 2016, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment: MOCA: A Brief Screening Tool for MCI. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Mullen, S.P.; Szabo, A.N.; White, S.M.; Wójcicki, T.R.; Mailey, E.L.; Gothe, N.P.; Olson, E.A.; Voss, M.; Erickson, K.; et al. Self-Regulatory Processes and Exercise Adherence in Older Adults. Am. J. Prev. Med. 2011, 41, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Menendez-Gonzalez, M. Routine Lumbar Puncture for the Early Diagnosis of Alzheimer’s Disease. Is It Safe? Front. Aging Neurosci. 2014, 6, 65. [Google Scholar]
- Bermejo-Pareja, F.; Antequera, D.; Vargas, T.; Molina, J.A.; Carro, E. Saliva Levels of Abeta1-42 as Potential Biomarker of Alzheimer’s Disease: A Pilot Study. BMC Neurol. 2010, 10, 108. [Google Scholar] [CrossRef]
- Sabbagh, M.N.; Shi, J.; Lee, M.; Arnold, L.; Al-Hasan, Y.; Heim, J.; McGeer, P. Salivary Beta Amyloid Protein Levels Are Detectable and Differentiate Patients with Alzheimer’s Disease Dementia from Normal Controls: Preliminary Findings. BMC Neurol. 2018, 18, 155. [Google Scholar] [CrossRef]
- Lee, M.; Guo, J.-P.; Kennedy, K.; McGeer, E.G.; McGeer, P.L. A Method for Diagnosing Alzheimer’s Disease Based on Salivary Amyloid-β Protein 42 Levels. J. Alzheimer’s Dis. 2016, 55, 1175–1182. [Google Scholar] [CrossRef]
- McGeer, P.L.; Guo, J.P.; Lee, M.; Kennedy, K.; McGeer, E.G. Alzheimer’s Disease Can Be Spared by Nonsteroidal Anti-Inflammatory Drugs. J. Alzheimer’s Dis. 2018, 62, 1219–1222. [Google Scholar] [CrossRef]
- Sheinerman, K.S.; Toledo, J.B.; Tsivinsky, V.G.; Irwin, D.; Grossman, M.; Weintraub, D.; Hurtig, H.I.; Chen-Plotkin, A.; Wolk, D.A.; McCluskey, L.F.; et al. Circulating Brain-Enriched MicroRNAs as Novel Biomarkers for Detection and Differentiation of Neurodegenerative Diseases. Alzheimer’s Res. Ther. 2017, 9, 89. [Google Scholar] [CrossRef]
- Nath, K.; Puleio, A.; Michielli, M.; Voelm, C.; Alberts, K.; Wall, K.; Duff, A.; Hanley, C.; Rogers, C.; Cohen, B.; et al. Biomarker and cognitive improvements after a single bout of Interactive Cognitive and Physical Exercise (iPACES v2.75): Results of a multi-site pilot study. In Proceedings of the The 33rd Annual Steinmetz Symposium, Schenectady, NY, USA, 22–24 May 2020. [Google Scholar]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).