Decision-Making and Risk-Propensity Changes during and after the COVID-19 Pandemic Lockdown

 , ,
, ,  ,
,  ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Cognitive Tasks
2.3. Questionnaires
2.4. Procedure
2.5. Statistical Analyses
3. Results
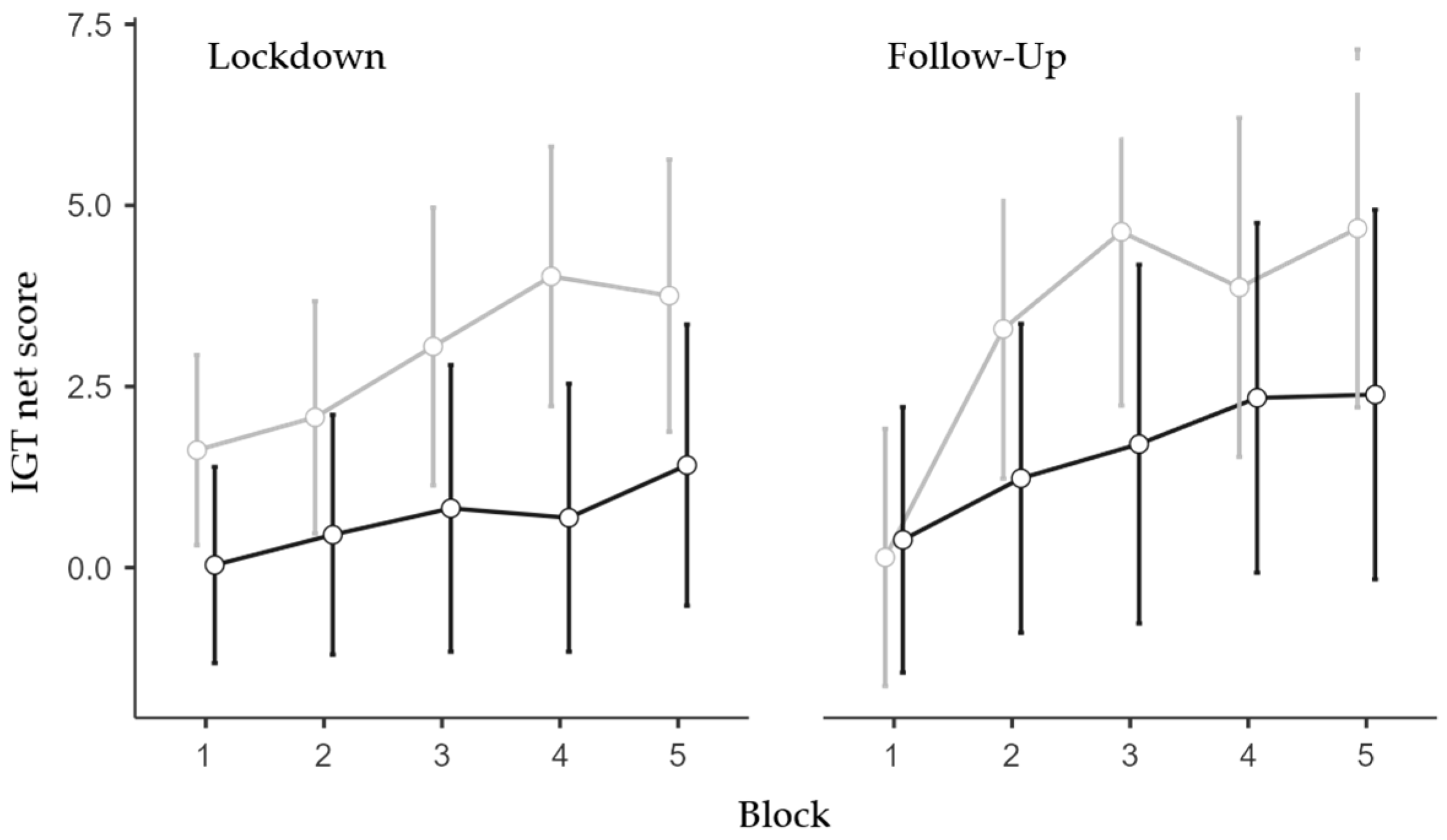
3.1. Iowa Gambling Task
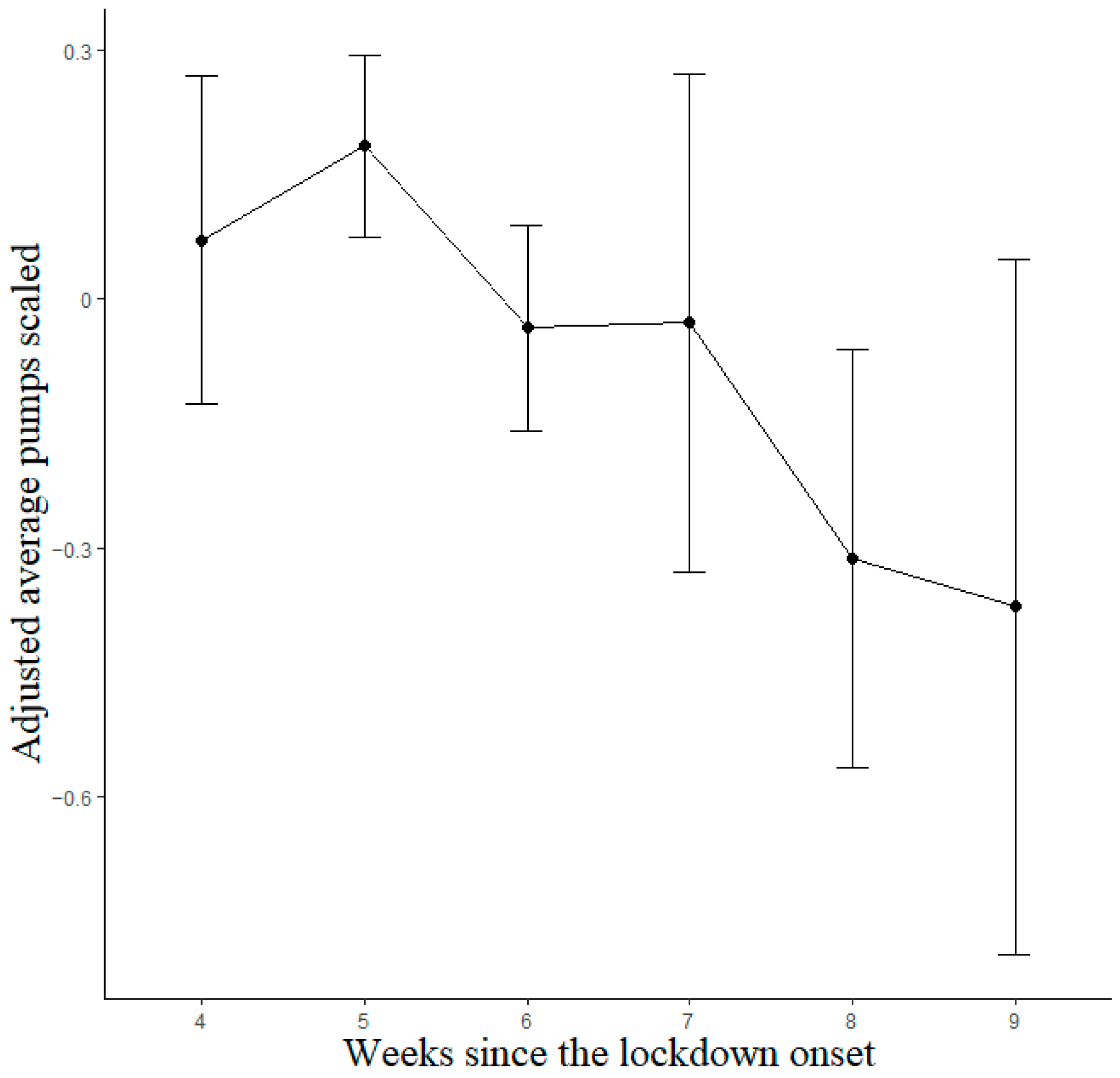
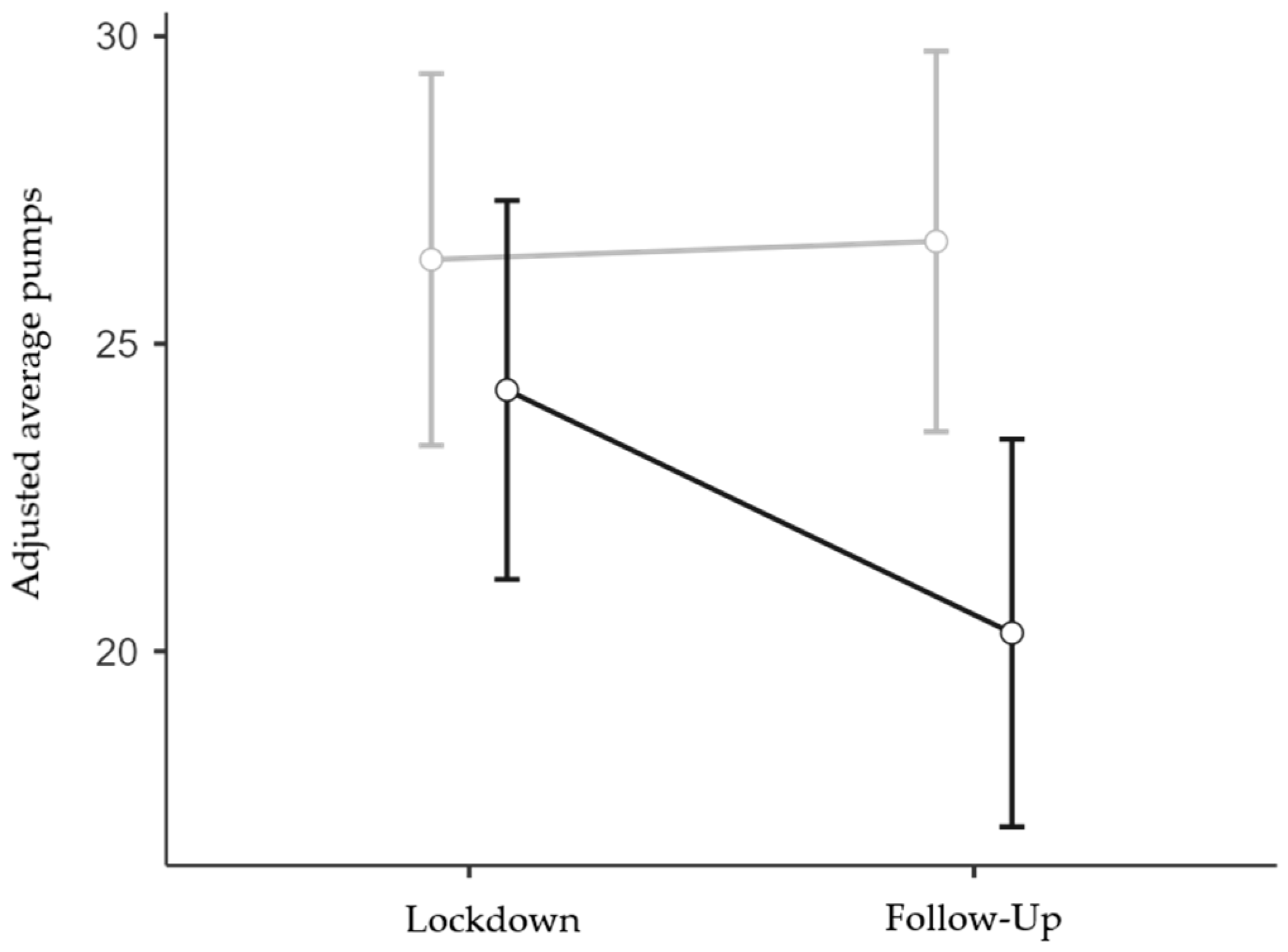
3.2. Balloon Analogue Risk Task
3.3. Category Switch Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Materials and Methods
Appendix A.1. Iowa Gambling Task
Appendix A.2. Balloon Analogue Risk Task
Appendix A.3. Category Switch Task
Appendix A.4. Impact of Event Scale
Appendix A.5. State-Trait Anxiety Inventory
Appendix A.6. Perceived Stress Scale
Appendix A.7. Statistical Analyses
Appendix B. Results
Appendix B.1. Iowa Gambling Task
Appendix B.2. Category Switch Task

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BART Adj. Avg. Pumps | IGT Net Score | |||||
|---|---|---|---|---|---|---|
| β | CI | p | β | CI | p | |
| (p boot) | (p boot) | |||||
| Intercept | −0.08 | −0.22–0.05 | 0.234 | −0.04 | −0.12–0.05 | 0.435 |
| (0.114) | (0.116) | |||||
| Week [linear] | −0.44 | −0.88–−0.00 | 0.049 | −0.12 | −0.41–0.18 | 0.44 |
| (<0.01) | (0.039) | |||||
| Week [quadratic] | −0.12 | −0.29–0.05 | 0.168 | −0.02 | −0.14–0.09 | 0.723 |
| (0.424) | (0.762) | |||||
| Week [cubic] | 0.09 | −0.03–0.22 | 0.154 | 0.04 | −0.04–0.13 | 0.312 |
| (0.395) | (0.369) | |||||
| Week [4th degree] | −0.01 | −0.14–0.12 | 0.906 | −0.04 | −0.13–0.05 | 0.392 |
| (0.938) | (0.379) | |||||
| Week [5th degree] | 0.13 | −0.03–0.30 | 0.117 | −0.02 | −0.13–0.09 | 0.73 |
| (0.309) | (0.724) | |||||
| Previous sessions | 0.32 | 0.16–0.47 | <0.001 | 0.15 | 0.05–0.25 | 0.004 |
| (<0.001) | (<0.001) | |||||
| Block [linear] | -- | -- | -- | 0.24 | 0.20–0.29 | <0.001 |
| (<0.001) | ||||||
| Block [quadratic] | -- | -- | -- | −0.04 | −0.09–0.00 | 0.078 |
| (0.164) | ||||||
| Block [cubic] | -- | -- | -- | −0.02 | −0.07–0.02 | 0.342 |
| (0.428) | ||||||
| Block [4th degree] | -- | -- | -- | 0.02 | −0.03–0.06 | 0.492 |
| (0.518) | ||||||
| Age | -- | -- | -- | −0.09 | −0.15–−0.04 | <0.001 |
| (<0.001) | ||||||
| CST Switch Cost | CST N-2 Rep. Cost | |||||
|---|---|---|---|---|---|---|
| β | SE | p | β | SE | p | |
| (p boot) | (p boot) | |||||
| Intercept | 0.06 | −0.08–0.20 | 0.417 | 0.1 | −0.04–0.23 | 0.154 |
| (0.259) | (00.077) | |||||
| Week [linear] | 0.11 | −0.37–0.59 | 0.656 | 0.43 | −0.05–0.92 | 0.077 |
| (0.414) | (<0.01) | |||||
| Week [quadratic] | 0.08 | −0.13–0.29 | 0.451 | 0.04 | −0.24–0.31 | 0.798 |
| (0.577) | (00.804) | |||||
| Week [cubic] | −0.22 | −0.38–−0.07 | 0.005 | 0.07 | −0.14–0.28 | 0.497 |
| (0.044) | (00.502) | |||||
| Week [4th degree] | 0.03 | −0.13–0.19 | 0.693 | 0.03 | −0.17–0.23 | 0.744 |
| (0.724) | (00.724) | |||||
| Week [5th degree] | 0.13 | −0.08–0.34 | 0.217 | 0.01 | −0.26–0.27 | 0.956 |
| (0.32) | (00.956) | |||||
| Previous sessions | −0.26 | −0.43–−0.10 | 0.002 | −0.21 | −0.38–−0.04 | 0.016 |
| (<0.001) | (<0.001) | |||||
| Age | 0.13 | 0.05–0.21 | 0.001 | -- | -- | -- |
| (<0.001) | ||||||
References
- Czeisler, M.É.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, M.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; et al. Mental Health, Substance Use, and Suicidal Ideation During the COVID-19 Pandemic—United States, June 24–30 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Sher, L. COVID-19, Anxiety, Sleep Disturbances and Suicide. Sleep Med. 2020, 70, 124. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, V.; Gorgoni, M.; Scarpelli, S.; Zivi, P.; Sdoia, S.; Mari, E.; Fraschetti, A.; Ferlazzo, F.; Giannini, A.M.; De Gennaro, L. COVID-19 Lockdown and Poor Sleep Quality: Not the Whole Story. J. Sleep Res. 2021, 30, e13368. [Google Scholar] [CrossRef]
- Alfonsi, V.; Gorgoni, M.; Scarpelli, S.; Zivi, P.; Sdoia, S.; Mari, E.; Quaglieri, A.; Ferlazzo, F.; Giannini, A.M.; De Gennaro, L. Changes in Sleep Pattern and Dream Activity across and after the COVID-19 Lockdown in Italy: A Longitudinal Observational Study. J. Sleep Res. 2022, 31, e13500. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, C.; Musetti, A.; Zenesini, C.; Palagini, L.; Scarpelli, S.; Quattropani, M.C.; Lenzo, V.; Freda, M.F.; Lemmo, D.; Vegni, E.; et al. Poor Sleep Quality and Its Consequences on Mental Health During the COVID-19 Lockdown in Italy. Front. Psychol. 2020, 11, 574475. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 Lockdown on Sleep Quality in University Students and Administration Staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Miniati, M.; Marzetti, F.; Palagini, L.; Marazziti, D.; Orrù, G.; Conversano, C.; Gemignani, A. Eating Disorders Spectrum During the COVID Pandemic: A Systematic Review. Front. Psychol. 2021, 12, 663376. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized Anxiety Disorder, Depressive Symptoms and Sleep Quality during COVID-19 Outbreak in China: A Web-Based Cross-Sectional Survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Tang, F.; Liang, J.; Zhang, H.; Kelifa, M.M.; He, Q.; Wang, P. COVID-19 Related Depression and Anxiety among Quarantined Respondents. Psychol. Health 2021, 36, 164–178. [Google Scholar] [CrossRef]
- Quaglieri, A.; Lausi, G.; Fraschetti, A.; Burrai, J.; Barchielli, B.; Pizzo, A.; Cordellieri, P.; De Gennaro, L.; Gorgoni, M.; Ferlazzo, F.; et al. “Stay at Home” in Italy during the COVID-19 Outbreak: A Longitudinal Study on Individual Well-Being among Different Age Groups. Brain Sci. 2021, 11, 993. [Google Scholar] [CrossRef]
- Kar, P.; Tomfohr-Madsen, L.; Giesbrecht, G.; Bagshawe, M.; Lebel, C. Alcohol and Substance Use in Pregnancy during the COVID-19 Pandemic. Drug Alcohol Depend. 2021, 225, 108760. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 and Violence against Women: What the Health Sector/System Can Do, April 7th 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID Stress Syndrome: Concept, Structure, and Correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef]
- Arnsten, A.F.T. Stress Signalling Pathways That Impair Prefrontal Cortex Structure and Function. Nat. Rev. Neurosci. 2009, 10, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Schoofs, D.; Preuß, D.; Wolf, O.T. Psychosocial Stress Induces Working Memory Impairments in an N-Back Paradigm. Psychoneuroendocrinology 2008, 33, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Shields, G.S.; Sazma, M.A.; Yonelinas, A.P. The Effects of Acute Stress on Core Executive Functions: A Meta-Analysis and Comparison with Cortisol. Neurosci. Biobehav. Rev. 2016, 68, 651–668. [Google Scholar] [CrossRef]
- Baddeley, A.D. Selective Attention and Performance in Dangerous Environments. Br. J. Psychol. 1972, 63, 537–546. [Google Scholar] [CrossRef]
- Chajut, E.; Algom, D. Selective Attention Improves under Stress: Implications for Theories of Social Cognition. J. Pers. Soc. Psychol. 2003, 85, 231–248. [Google Scholar] [CrossRef]
- Payne, J.; Bettman, J.; Johnson, E. Adaptive Strategy Selection in Decision Making. J. Exp. Psychol. Learn. Mem. Cogn. 1988, 14, 534–552. [Google Scholar] [CrossRef]
- Schwabe, L.; Wolf, O.T. Stress-Induced Modulation of Instrumental Behavior: From Goal-Directed to Habitual Control of Action. Behav. Brain Res. 2011, 219, 321–328. [Google Scholar] [CrossRef]
- Schwabe, L.; Wolf, O.T. Stress and Multiple Memory Systems: From ‘Thinking’ to ‘Doing’. Trends Cogn. Sci. 2013, 17, 60–68. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, H.; Damasio, A.R. Emotion, Decision Making and the Orbitofrontal Cortex. Cereb. Cortex 2000, 10, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Damasio, A.R.; Everitt, B.J.; Bishop, D.; Roberts, A.C.; Robbins, T.W.; Weiskrantz, L. The Somatic Marker Hypothesis and the Possible Functions of the Prefrontal Cortex. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 1996, 351, 1413–1420. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to Future Consequences Following Damage to Human Prefrontal Cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Simonovic, B.; Stupple, E.; Gale, M.; Sheffield, D. Sweating the Small Stuff: A Meta-Analysis of Skin Conductance on the Iowa Gambling Task. Cogn. Affect. Behav. Neurosci. 2019, 19, 1097–1112. [Google Scholar] [CrossRef]
- Overman, W.; Pierce, A. Iowa Gambling Task with Non-Clinical Participants: Effects of Using Real + Virtual Cards and Additional Trials. Front. Psychol. 2013, 4, 935. [Google Scholar] [CrossRef]
- van Honk, J.; Schutter, D.J.L.G.; Hermans, E.J.; Putman, P. Low Cortisol Levels and the Balance between Punishment Sensitivity and Reward Dependency. NeuroReport 2003, 14, 1993–1996. [Google Scholar] [CrossRef] [PubMed]
- Preston, S.D.; Buchanan, T.W.; Stansfield, R.B.; Bechara, A. Effects of Anticipatory Stress on Decision Making in a Gambling Task. Behav. Neurosci. 2007, 121, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, V.; Tasca, I.; Giannetto, N.; Mangano, G.R.; Turriziani, P.; Oliveri, M. Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown. Behav. Sci. 2021, 11, 167. [Google Scholar] [CrossRef]
- Brand, M.; Recknor, E.C.; Grabenhorst, F.; Bechara, A. Decisions under Ambiguity and Decisions under Risk: Correlations with Executive Functions and Comparisons of Two Different Gambling Tasks with Implicit and Explicit Rules. J. Clin. Exp. Neuropsychol. 2007, 29, 86–99. [Google Scholar] [CrossRef]
- Ingram, J.; Hand, C.J.; Maciejewski, G. Social Isolation during COVID-19 Lockdown Impairs Cognitive Function. Appl. Cogn. Psychol. 2021, 35, 935–947. [Google Scholar] [CrossRef]
- Starcke, K.; Brand, M. Decision Making under Stress: A Selective Review. Neurosci. Biobehav. Rev. 2012, 36, 1228–1248. [Google Scholar] [CrossRef]
- Lejuez, C.W.; Read, J.P.; Kahler, C.W.; Richards, J.B.; Ramsey, S.E.; Stuart, G.L.; Strong, D.R.; Brown, R.A. Evaluation of a Behavioral Measure of Risk Taking: The Balloon Analogue Risk Task (BART). J. Exp. Psychol. Appl. 2002, 8, 75–84. [Google Scholar] [CrossRef]
- Lighthall, N.R.; Mather, M.; Gorlick, M.A. Acute Stress Increases Sex Differences in Risk Seeking in the Balloon Analogue Risk Task. PLoS ONE 2009, 4, e6002. [Google Scholar] [CrossRef] [PubMed]
- Bourne, L.E.; Yaroush, R.A. Stress and Cognition: A Cognitive Psychological Perspective; National Aeronautics and Space Administration Ames Research Center: Moffett Field, CA, USA, 2003.
- Lighthall, N.R.; Sakaki, M.; Vasunilashorn, S.; Nga, L.; Somayajula, S.; Chen, E.Y.; Samii, N.; Mather, M. Gender Differences in Reward-Related Decision Processing under Stress. Soc. Cogn. Affect. Neurosci. 2012, 7, 476–484. [Google Scholar] [CrossRef]
- Morgado, P.; Sousa, N.; Cerqueira, J. The Impact of Stress in Decision Making in the Context of Uncertainty. J. Neurosci. Res. 2015, 93, 839–847. [Google Scholar] [CrossRef]
- Otto, A.R.; Raio, C.M.; Chiang, A.; Phelps, E.A.; Daw, N.D. Working-Memory Capacity Protects Model-Based Learning from Stress. Proc. Natl. Acad. Sci. USA 2013, 110, 20941–20946. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, A.J.; Delgado, M.R. Acute Stress Modulates Risk Taking in Financial Decision Making. Psychol. Sci. 2009, 20, 278–283. [Google Scholar] [CrossRef]
- Starcke, K.; Brand, M. Effects of Stress on Decisions under Uncertainty: A Meta-Analysis. Psychol. Bull. 2016, 142, 909–933. [Google Scholar] [CrossRef] [PubMed]
- van den Bos, R.; Harteveld, M.; Stoop, H. Stress and Decision-Making in Humans: Performance Is Related to Cortisol Reactivity, Albeit Differently in Men and Women. Psychoneuroendocrinology 2009, 34, 1449–1458. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C. Perceived Social Isolation and Cognition. Trends Cogn. Sci. 2009, 13, 447–454. [Google Scholar] [CrossRef]
- Kandasamy, N.; Hardy, B.; Page, L.; Schaffner, M.; Graggaber, J.; Powlson, A.S.; Fletcher, P.C.; Gurnell, M.; Coates, J. Cortisol Shifts Financial Risk Preferences. Proc. Natl. Acad. Sci. USA 2014, 111, 3608–3613. [Google Scholar] [CrossRef]
- Baradell, J.G.; Klein, K. Relationship of Life Stress and Body Consciousness to Hypervigilant Decision Making. J. Pers. Soc. Psychol. 1993, 64, 267–273. [Google Scholar] [CrossRef]
- Lenow, J.K.; Constantino, S.M.; Daw, N.D.; Phelps, E.A. Chronic and Acute Stress Promote Overexploitation in Serial Decision Making. J. Neurosci. 2017, 37, 5681–5689. [Google Scholar] [CrossRef] [PubMed]
- Soares, J.M.; Sampaio, A.; Ferreira, L.M.; Santos, N.C.; Marques, F.; Palha, J.A.; Cerqueira, J.J.; Sousa, N. Stress-Induced Changes in Human Decision-Making Are Reversible. Transl. Psychiatry 2012, 2, e131. [Google Scholar] [CrossRef]
- Mari, E.; Fraschetti, A.; Lausi, G.; Pizzo, A.; Baldi, M.; Paoli, E.; Giannini, A.M.; Avallone, F. Forced Cohabitation during Coronavirus Lockdown in Italy: A Study on Coping, Stress and Emotions among Different Family Patterns. J. Clin. Med. 2020, 9, 3906. [Google Scholar] [CrossRef]
- Aiello, J.R.; DeRisi, D.T.; Epstein, Y.M.; Karlin, R.A. Crowding and the Role of Interpersonal Distance Preference. Sociometry 1977, 40, 271–282. [Google Scholar] [CrossRef]
- Evans, G.W.; Wener, R.E. Crowding and Personal Space Invasion on the Train: Please Don’t Make Me Sit in the Middle. J. Environ. Psychol. 2007, 27, 90–94. [Google Scholar] [CrossRef]
- Suedfeld, P. Extreme and unusual environments. In Handbook of Environmental Psychology; Stokols, D., Altman, I., Eds.; Wiley: New York, NY, USA, 1987; Volume 1, pp. 863–887. [Google Scholar]
- Sandal, G.M.; Leon, G.R.; Palinkas, L. Human Challenges in Polar and Space Environments. Rev. Environ. Sci. Biotechnol. 2006, 5, 281–296. [Google Scholar] [CrossRef]
- Zivi, P.; De Gennaro, L.; Ferlazzo, F. Sleep in Isolated, Confined, and Extreme (ICE): A Review on the Different Factors Affecting Human Sleep in ICE. Front. Neurosci. 2020, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, M.; Martinent, G.; Suedfeld, P.; Gaudino, M. Assessing Psychological Adaptation during Polar Winter-Overs: The Isolated and Confined Environments Questionnaire (ICE-Q). J. Environ. Psychol. 2019, 65, 101317. [Google Scholar] [CrossRef]
- Suedfeld, P.; Steel, G.D. The Environmental Psychology of Capsule Habitats. Annu. Rev. Psychol. 2000, 51, 227–253. [Google Scholar] [CrossRef]
- Abeln, V.; MacDonald-Nethercott, E.; Piacentini, M.F.; Meeusen, R.; Kleinert, J.; Strueder, H.K.; Schneider, S. Exercise in Isolation- A Countermeasure for Electrocortical, Mental and Cognitive Impairments. PLoS ONE 2015, 10, e0126356. [Google Scholar] [CrossRef]
- Nicolas, M.; Weiss, K. Stress and Recovery Assessment during Simulated Microgravity: Effects of Exercise during a Long-Term Head-down Tilt Bed Rest in Women. J. Environ. Psychol. 2009, 29, 522–528. [Google Scholar] [CrossRef]
- Van Cutsem, J.; Abeln, V.; Schneider, S.; Keller, N.; Diaz-Artiles, A.; Ramallo, M.A.; Dessy, E.; Pattyn, N.; Ferlazzo, F.; Torre, G.G.D.L. The Impact of the COVID-19 Lockdown on Human Psychology and Physical Activity; a Space Analogue Research Perspective. Int. J. Astrobiol. 2022, 21, 32–45. [Google Scholar] [CrossRef]
- Leon, G.R.; Sandal, G.M.; Larsen, E. Human Performance in Polar Environments. J. Environ. Psychol. 2011, 31, 353–360. [Google Scholar] [CrossRef]
- Nicolas, M.; Sandal, G.M.; Weiss, K.; Yusupova, A. Mars-105 Study: Time-Courses and Relationships between Coping, Defense Mechanisms, Emotions and Depression. J. Environ. Psychol. 2013, 35, 52–58. [Google Scholar] [CrossRef]
- Nicolas, M.; Suedfeld, P.; Weiss, K.; Gaudino, M. Affective, Social, and Cognitive Outcomes During a 1-Year Wintering in Concordia. Environ. Behav. 2016, 48, 1073–1091. [Google Scholar] [CrossRef]
- Sandal, G.M.; van deVijver, F.J.R.; Smith, N. Psychological Hibernation in Antarctica. Front. Psychol. 2018, 9, 2235. [Google Scholar] [CrossRef]
- Bishop, S.L. Evaluating Teams in Extreme Environments: From Issues to Answers. Aviat. Space Environ. Med. 2004, 75, C14–C21. [Google Scholar]
- Kanas, N. Psychosocial Issues Affecting Crews during Long-Duration International Space Missions. Acta Astronaut. 1998, 42, 339–361. [Google Scholar] [CrossRef]
- John Paul, F.U.; Mandal, M.K.; Ramachandran, K.; Panwar, M.R. Cognitive Performance during Long-Term Residence in a Polar Environment. J. Environ. Psychol. 2010, 30, 129–132. [Google Scholar] [CrossRef]
- Pagel, J.I.; Choukèr, A. Effects of Isolation and Confinement on Humans-Implications for Manned Space Explorations. J. Appl. Physiol. 2016, 120, 1449–1457. [Google Scholar] [CrossRef]
- Strangman, G.E.; Sipes, W.; Beven, G. Human Cognitive Performance in Spaceflight and Analogue Environments. Aviat. Space Environ. Med. 2014, 85, 1033–1048. [Google Scholar] [CrossRef]
- van Baarsen, B.; Ferlazzo, F.; Ferravante, D.; Smit, J.; Pligt, J.; Duijn, M. The Effects of Extreme Isolation on Loneliness and Cognitive Control Processes: Analyses of the Lodgead Data Obtained during the Mars105 and the Mars520 Studies. Proc. Int. Astronaut. Congr. IAC 2012, 1, 19–26. [Google Scholar]
- Evans, I.E.M.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social Isolation and Cognitive Function in Later Life: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2019, 70, S119–S144. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Miyake, A.; Young, S.E.; DeFries, J.C.; Corley, R.P.; Hewitt, J.K. Individual Differences in Executive Functions Are Almost Entirely Genetic in Origin. J. Exp. Psychol. Gen. 2008, 137, 201. [Google Scholar] [CrossRef]
- Mayr, U.; Kliegl, R. Differential Effects of Cue Changes and Task Changes on Task-Set Selection Costs. J. Exp. Psychol. Learn. Mem. Cogn. 2003, 29, 362–372. [Google Scholar] [CrossRef]
- Mayr, U.; Keele, S.W. Changing Internal Constraints on Action: The Role of Backward Inhibition. J. Exp. Psychol. Gen. 2000, 129, 4–26. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; De Gennaro, L.; Di Paolo, M.C.; Solano, L. The Impact of Event Scale: Validation of an Italian Version. J. Psychosom. Res. 2003, 55, 389–393. [Google Scholar] [CrossRef]
- Pedrabissi, L.; Santinello, M. Verifica Della Validità Dello STAI Forma Y Di Spielberger. Giunti Organ. Spec. 1989, 191–192, 11–14. [Google Scholar]
- Mondo, M.; Sechi, C.; Cabras, C. Psychometric Evaluation of Three Versions of the Italian Perceived Stress Scale. Curr. Psychol. 2021, 40, 1884–1892. [Google Scholar] [CrossRef]
- Guenther, B.; Galizzi, M.M.; Sanders, J.G. Heterogeneity in Risk-Taking During the COVID-19 Pandemic: Evidence From the UK Lockdown. Front. Psychol. 2021, 12, 643653. [Google Scholar] [CrossRef]
- Harrison, G.W.; Hofmeyr, A.; Kincaid, H.; Monroe, B.; Ross, D.; Schneider, M.; Swarthout, J.T. Subjective Beliefs and Economic Preferences during the COVID-19 Pandemic. Exp. Econ. 2022, 25, 795–823. [Google Scholar] [CrossRef]
- Friedel, E.; Sebold, M.; Kuitunen-Paul, S.; Nebe, S.; Veer, I.M.; Zimmermann, U.S.; Schlagenhauf, F.; Smolka, M.N.; Rapp, M.; Walter, H.; et al. How Accumulated Real Life Stress Experience and Cognitive Speed Interact on Decision-Making Processes. Front. Hum. Neurosci. 2017, 11, 302. [Google Scholar] [CrossRef]
- Park, H.; Lee, D.; Chey, J. Stress Enhances Model-Free Reinforcement Learning Only after Negative Outcome. PLoS ONE 2017, 12, e0180588. [Google Scholar] [CrossRef]
- Petzold, A.; Plessow, F.; Goschke, T.; Kirschbaum, C. Stress Reduces Use of Negative Feedback in a Feedback-Based Learning Task. Behav. Neurosci. 2010, 124, 248–255. [Google Scholar] [CrossRef]
- Porcelli, A.J.; Delgado, M.R. Stress and Decision Making: Effects on Valuation, Learning, and Risk-Taking. Curr. Opin. Behav. Sci. 2017, 14, 33–39. [Google Scholar] [CrossRef]
- Simonovic, B.; Stupple, E.J.N.; Gale, M.; Sheffield, D. Performance Under Stress: An Eye-Tracking Investigation of the Iowa Gambling Task (IGT). Front. Behav. Neurosci. 2018, 12, 217. [Google Scholar] [CrossRef]
- Starcke, K.; Agorku, J.D.; Brand, M. Exposure to Unsolvable Anagrams Impairs Performance on the Iowa Gambling Task. Front. Behav. Neurosci. 2017, 11, 114. [Google Scholar] [CrossRef] [PubMed]
- Haucke, M.; Golde, S.; Saft, S.; Hellweg, R.; Liu, S.; Heinzel, S. The Effects of Momentary Loneliness and COVID-19 Stressors on Hypothalamic–Pituitary Adrenal (HPA) Axis Functioning: A Lockdown Stage Changes the Association between Loneliness and Salivary Cortisol. Psychoneuroendocrinology 2022, 145, 105894. [Google Scholar] [CrossRef]
- de Kloet, E.R.; Joëls, M.; Holsboer, F. Stress and the Brain: From Adaptation to Disease. Nat. Rev. Neurosci. 2005, 6, 463–475. [Google Scholar] [CrossRef]
- Northoff, G.; Grimm, S.; Boeker, H.; Schmidt, C.; Bermpohl, F.; Heinzel, A.; Hell, D.; Boesiger, P. Affective Judgment and Beneficial Decision Making: Ventromedial Prefrontal Activity Correlates with Performance in the Iowa Gambling Task. Hum. Brain Mapp. 2006, 27, 572–587. [Google Scholar] [CrossRef]
- Li, X.; Lu, Z.-L.; D’Argembeau, A.; Ng, M.; Bechara, A. The Iowa Gambling Task in FMRI Images. Hum. Brain Mapp. 2010, 31, 410–423. [Google Scholar] [CrossRef] [PubMed]
- Andolina, D.; Maran, D.; Valzania, A.; Conversi, D.; Puglisi-Allegra, S. Prefrontal/Amygdalar System Determines Stress Coping Behavior Through 5-HT/GABA Connection. Neuropsychopharmacology 2013, 38, 2057–2067. [Google Scholar] [CrossRef]
- Reimann, M.; Bechara, A. The Somatic Marker Framework as a Neurological Theory of Decision-Making: Review, Conceptual Comparisons, and Future Neuroeconomics Research. J. Econ. Psychol. 2010, 31, 767–776. [Google Scholar] [CrossRef]
- Noel, P.; Cork, C.; White, R.G. Social Capital and Mental Health in Post-Disaster/Conflict Contexts: A Systematic Review. Disaster Med. Public Health Prep. 2018, 12, 791–802. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using Social and Behavioural Science to Support COVID-19 Pandemic Response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Lenth, R.V.; Buerkner, P.; Herve, M.; Love, J.; Miguez, F.; Riebl, H.; Singmann, H. Emmeans: Estimated Marginal Means, Aka Least-Squares Means. Am. Stat. 2022, 34, 216–221. [Google Scholar]
- Zhang, L.; Wang, K.; Zhu, C.; Yu, F.; Chen, X. Trait Anxiety Has Effect on Decision Making under Ambiguity but Not Decision Making under Risk. PLoS ONE 2015, 10, e0127189. [Google Scholar] [CrossRef]




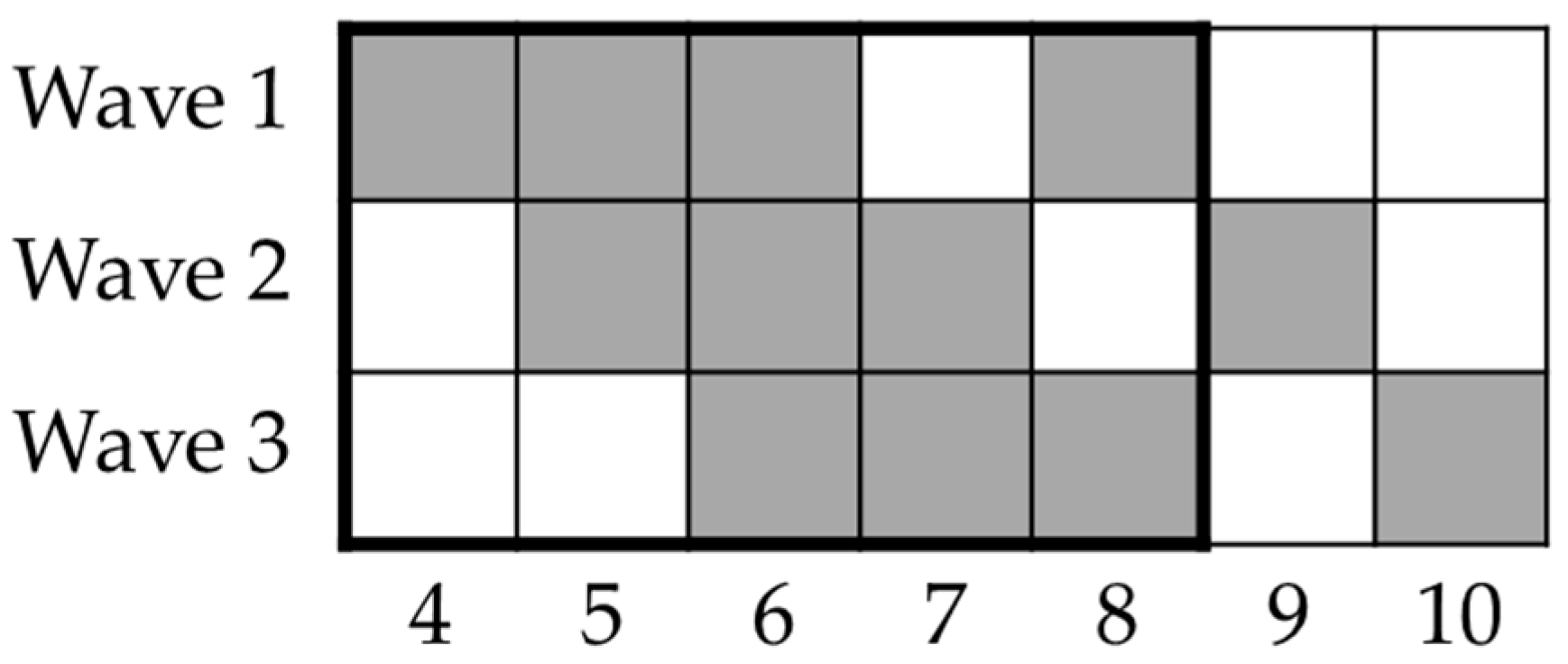
| Week | BART | IGT | CST |
|---|---|---|---|
| 4 | N = 408 | N = 402 | N = 386 |
| 124 m, 284 f | 122 m, 280 f | 114 m, 272 f | |
| Age M 32.57 SD 14.33 | Age M 32.42 SD 14.24 | Age M 32.29 SD 14.20 | |
| 5 | N = 314 | N = 310 | N = 301 |
| 96 m, 218 f | 94 m, 216 f | 89 m, 212 f | |
| Age M 33.03 SD 14.67 | Age M 33.13 SD 14.75 | Age M 32.73 SD 14.57 | |
| 6 | N = 292 | N = 292 | N = 286 |
| 91 m, 201 f | 91 m, 201 f | 87 m, 199 f | |
| Age M 34.20 SD 15.17 | Age M 34.10 SD 15.11 | Age M 34.04 SD 15.07 | |
| 7 | N = 27 | N = 27 | N = 26 |
| 7 m, 20 f | 7 m, 20 f | 6 m, 20 f | |
| Age M 39.11 SD 15.57 | Age M 39.11 SD 15.57 | Age M 39.69 SD 15.58 | |
| 8 | N = 200 | N = 200 | N = 195 |
| 62 m, 138 f | 63 m, 137 f | 58 m, 137 f | |
| Age M 33.32 SD 14.77 | Age M 33.17 SD 14.75 | Age M 32.92 SD 14.62 | |
| 9 | N = 24 | N = 25 | N = 25 |
| 4 m, 20 f | 4 m, 21 f | 4 m, 21 f | |
| Age M 31.42 SD 15.15 | Age M 31.00 SD 14.98 | Age M 31.00 SD 14.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zivi, P.; Sdoia, S.; Alfonsi, V.; Gorgoni, M.; Mari, E.; Quaglieri, A.; De Gennaro, L.; Giannini, A.M.; Ferlazzo, F. Decision-Making and Risk-Propensity Changes during and after the COVID-19 Pandemic Lockdown. Brain Sci. 2023, 13, 793. https://doi.org/10.3390/brainsci13050793
Zivi P, Sdoia S, Alfonsi V, Gorgoni M, Mari E, Quaglieri A, De Gennaro L, Giannini AM, Ferlazzo F. Decision-Making and Risk-Propensity Changes during and after the COVID-19 Pandemic Lockdown. Brain Sciences. 2023; 13(5):793. https://doi.org/10.3390/brainsci13050793
Chicago/Turabian StyleZivi, Pierpaolo, Stefano Sdoia, Valentina Alfonsi, Maurizio Gorgoni, Emanuela Mari, Alessandro Quaglieri, Luigi De Gennaro, Anna Maria Giannini, and Fabio Ferlazzo. 2023. "Decision-Making and Risk-Propensity Changes during and after the COVID-19 Pandemic Lockdown" Brain Sciences 13, no. 5: 793. https://doi.org/10.3390/brainsci13050793
APA StyleZivi, P., Sdoia, S., Alfonsi, V., Gorgoni, M., Mari, E., Quaglieri, A., De Gennaro, L., Giannini, A. M., & Ferlazzo, F. (2023). Decision-Making and Risk-Propensity Changes during and after the COVID-19 Pandemic Lockdown. Brain Sciences, 13(5), 793. https://doi.org/10.3390/brainsci13050793