
Image Findings as Predictors of Fall Risk in Patients with Cerebrovascular Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Methods
2.2. Clinical Assessments
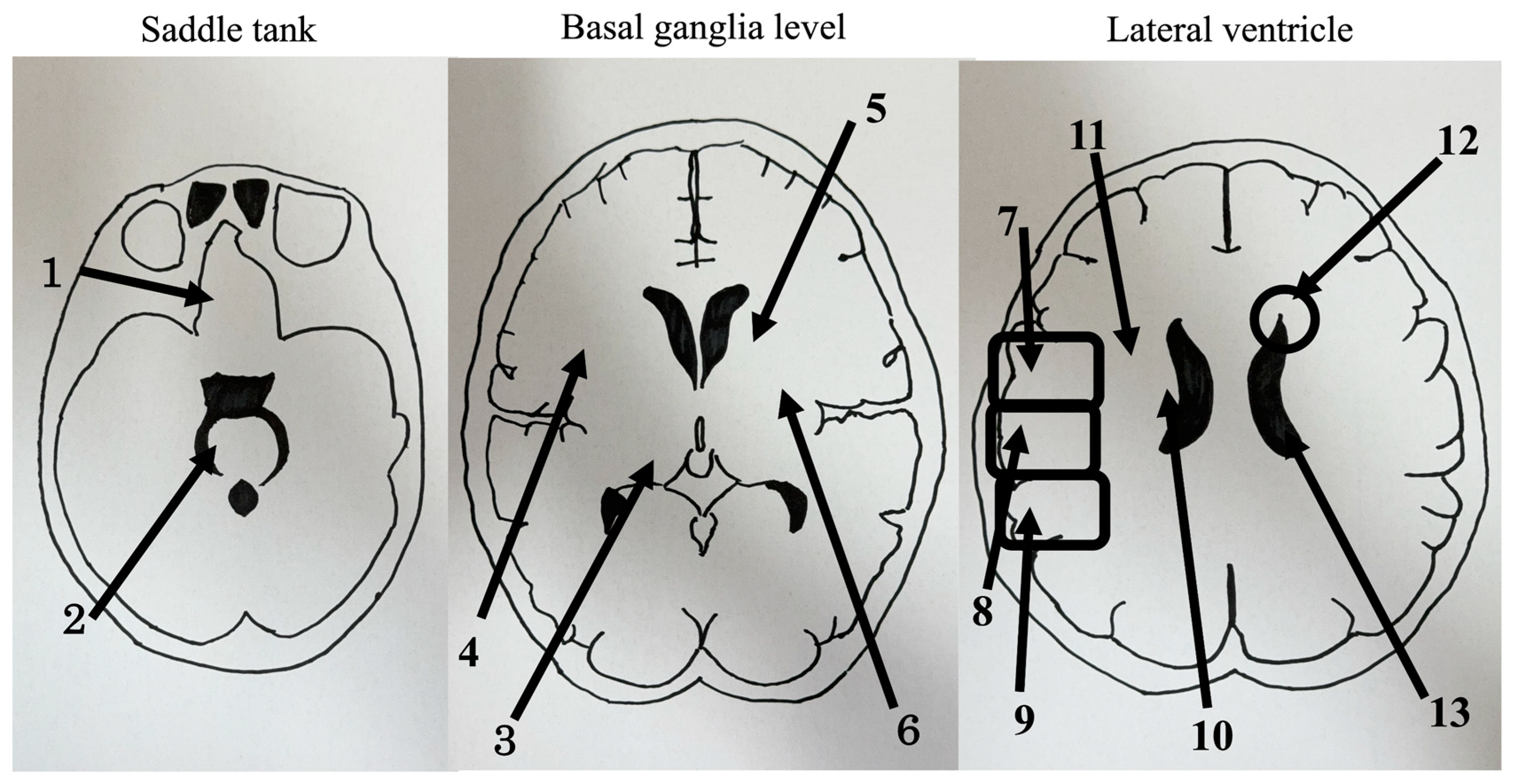
2.2.1. CT
2.2.2. Functional Independence Measure (FIM)
2.2.3. Mini-Mental State Examination (MMSE)
2.2.4. Functional Ambulation Categories (FAC)
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Logistic Regression Analysis
3.3. Logistic Regression Analysis Classified into Cerebral Hemorrhage and Cerebral Infarction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ang, G.C.; Low, S.L.; How, C.H. Approach to falls among the elderly in the community. Singap. Med. J. 2020, 61, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Kamel, M.H.; Abdulmajeed, A.A.; Ismail, S.E.S. Risk factors of falls among elderly living in urban Suez-Egypt. Pan Afr. Med. J. 2013, 14, 26. [Google Scholar] [CrossRef] [PubMed]
- Jewell, V.D.; Capistran, K.; Flecky, K.; Qi, Y.; Fellman, S. Prediction of falls in acute care using the Morse Fall Risk Scale. Occup. Ther. Health Care 2020, 34, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Gibson, M.J.; Andres, R.O.; Isaacs, B.; Radebaugh, T.; WormPetersen, J. The prevention of falls in later life. A report of the Kellogg International Work Group on the prevention of falls by the elderly. Dan. Med. Bull. 1987, 34 (Suppl. 4), 1–24. [Google Scholar]
- Smith, A.A.; Silva, A.O.; Rodrigues, R.A.; Moreira, M.A.; Nogueira, J.A.; Tura, L.F. Assessment of risk of falls in elderly living at home. Rev. Lat. Am. Enferm. 2017, 25, e2754. [Google Scholar] [CrossRef] [PubMed]
- Moreland, J.; Richardson, J.; Chan, D.; O’Neill, J.; Bellissimo, A.; Grum, R.M.; Shanks, L. Evidence-based guidelines for the secondary prevention of falls in older adults. Gerontology 2003, 49, 93–116. [Google Scholar] [CrossRef] [PubMed]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef]
- Moon, H.I.; Pyun, S.B.; Tae, W.S.; Kwon, H.K. Neural substrates of lower extremity motor, balance, and gait function after supratentorial stroke using voxel-based lesion symptom mapping. Neuroradiology 2016, 58, 723–731. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Kojima, G.; Masud, T.; Kendrick, D.; Morris, R.; Gawler, S.; Treml, J.; Iliffe, S. Does the timed up and go test predict future falls among British community-dwelling older people? Prospective cohort study nested within a randomised controlled trial. BMC Geriatr. 2015, 15, 38. [Google Scholar] [CrossRef]
- Beauchet, O.; Fantino, B.; Allali, G.; Muir, S.W.; Montero-Odasso, M.; Annweiler, C. Timed Up and Go test and risk of falls in older adults: A systematic review. J. Nutr. Health Aging 2011, 15, 933–938. [Google Scholar] [CrossRef]
- Silsupadol, P.; Siu, K.C.; Shumway-Cook, A.; Woollacott, M.H. Training of balance under single- and dual-task conditions in older adults with balance impairment. Phys. Ther. 2006, 86, 269–281. [Google Scholar] [CrossRef]
- Verma, R.; Arya, K.N.; Sharma, P.; Garg, R.K. Understanding gait control in post-stroke: Implications for management. J. Bodyw. Mov. Ther. 2012, 16, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.A.; Van Puymbroeck, M.; Altenburger, P.A.; Miller, K.K.; Combs, S.A.; Page, S.J. Balance is associated with quality of life in chronic stroke. Top. Stroke Rehabil. 2013, 20, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Hertanu, J.S.; Demopoulos, J.T.; Yang, W.C.; Calhoun, W.F.; Fenigstein, H.A. Stroke rehabilitation: Correlation and prognostic value of computerized tomography and sequential functional assessments. Arch. Phys. Med. Rehabil. 1984, 65, 505–508. [Google Scholar]
- Lee, K.B.; Kim, J.S.; Hong, B.Y.; Sul, B.; Song, S.; Sung, W.J.; Hwang, B.Y.; Lim, S.H. Brain lesions affecting gait recovery in stroke patients. Brain Behav. 2017, 7, e00868. [Google Scholar] [CrossRef]
- Koch, G.; Bonni, S.; Casula, E.P.; Iosa, M.; Paolucci, S.; Pellicciari, M.C.; Cinnera, A.M.; Ponzo, V.; Maiella, M.; Picazio, S.; et al. Effect of cerebellar stimulation on gait and balance recovery in patients with hemiparetic stroke: A randomized clinical trial. JAMA Neurol. 2019, 76, 170–178. [Google Scholar] [CrossRef]
- Lamb, S.E.; Ferrucci, L.; Volapto, S.; Fried, L.P.; Guralnik, J.M. Women’s Health and Aging Study. Risk factors for falling in home-dwelling older women with stroke: The Women’s Health and Aging Study. Stroke 2003, 34, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Hyndman, D.; Ashburn, A.; Stack, E. Fall events among people with stroke living in the community: Circumstances of falls and characteristics of fallers. Arch. Phys. Med. Rehabil. 2002, 83, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Kwon, H.G. The ascending reticular activating system from pontine reticular formation to the hypothalamus in the human brain. Neurosci. Lett. 2015, 590, 58–61. [Google Scholar] [CrossRef]
- Yeo, S.S.; Chang, P.H.; Jang, S.H. The ascending reticular activating system from pontine reticular formation to the thalamus in the human brain. Front. Hum. Neurosci. 2013, 7, 416. [Google Scholar] [CrossRef]
- Kim, H.; Jeong, E.J.; Park, D.H.; Czosnyka, Z.; Yoon, B.C.; Kim, K.; Czosnyka, M.; Kim, D.-J. Finite element analysis of periventricular lucency in hydrocephalus: Extravasation or transependymal CSF absorption? J. Neurosurg. 2016, 124, 334–341. [Google Scholar] [CrossRef]
- Corbett, A.; Bennett, H.; Kos, S. Cognitive dysfunction following subcortical infarction. Arch. Neurol. 1994, 51, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Sinnecker, T.; Ruberte, E.; Schädelin, S.; Canova, V.; Amann, M.; Naegelin, Y.; Penner, I.-K.; Müller, J.; Kuhle, J.; Décard, B.; et al. New and enlarging white matter lesions adjacent to the ventricle system and thalamic atrophy are independently associated with lateral ventricular enlargement in multiple sclerosis. J. Neurol. 2020, 267, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.J.; Delbaere, K.; Close, J.C.; Sachdev, P.S.; Lord, S.R. Impact of white matter lesions on physical functioning and fall risk in older people: A systematic review. Stroke 2011, 42, 2086–2090. [Google Scholar] [CrossRef] [PubMed]
- Ikegami, S.; Takahashi, J.; Uehara, M.; Tokida, R.; Nishimura, H.; Sakai, A.; Kato, H. Physical performance reflects cognitive function, fall risk, and quality of life in community-dwelling older people. Sci. Rep. 2019, 9, 12242. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.A.; Ricci, N.A.; Nogueira, E.C.; Perracini, M.R. The Berg Balance Scale as a clinical screening tool to predict fall risk in older adults: A systematic review. Physiotherapy 2018, 104, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Breisinger, T.P.; Skidmore, E.R.; Niyonkuru, C.; Terhorst, L.; Campbell, G.B. The Stroke Assessment of Fall Risk (SAFR): Predictive validity in inpatient stroke rehabilitation. Clin. Rehabil. 2014, 28, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Choi, E.S.; Park, D. In-hospital fall prediction using machine learning algorithms and the Morse fall scale in patients with acute stroke: A nested case-control study. BMC Med. Inform. Decis. Mak. 2023, 23, 246. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Jia, B.; Kong, J.; Zhang, X.; Lei, L.; Tao, Z.; Ma, L.; Xiang, Q.; Zhou, Y.; Cui, Y. Drug-induced fall risk in older patients: A pharmacovigilance study of FDA adverse event reporting system database. Front. Pharmacol. 2022, 13, 1044744. [Google Scholar] [CrossRef]

{kind=link}
| Fall Group (n = 43) | Non-Fall Group (n = 95) | p Value | |
|---|---|---|---|
| Age | 73.6 ± 10.0 | 73.9 ± 9.55 | 0.84 |
| 52–90 (range) | 47–88 (range) | ||
| Duration from onset to CT | 36.1 ± 22.9 | 38.2 ± 24.4 | 0.63 |
| 0–108 (range) | 0–110 (range) | ||
| MMSE | 14.5 ± 9.1 | 14.6 ± 11.2 | 0.92 |
| 0–28 (range) | 0–30 (range) | ||
| FIM | 34.9 ± 12.9 | 43.4 ± 24.4 | 0.008 ** |
| 21–119 (range) | 18–123 (range) | ||
| Total number of CT findings | 2.67 ± 1.42 | 1.89 ± 1.47 | 0.004 ** |
| 0–4 (range) | 0–6 (range) | ||
| FAC | 2.0 ± 1.66 | 2.27 ± 2.0 | 0.40 |
| 1–5 (range) | 0–5 (range) |
| OR | 95% CI | p Value | VIF | |
|---|---|---|---|---|
| PVL | 6.3 | 2.16–18.3 | 0.0007 *** | 1.04 |
| Thalamus | 16.2 | 5.43–47.8 | 0.00000005 *** | 1.04 |
| Divided into the basal forebrain | 0.000001 | 0–0 | 0.993 | 1 |
| Lateral ventricle enlargement | 1.21 | 0.44–3.27 | 0.704 | 1 |
| Distant from the lateral ventricle | 1.96 | 0.44–8.6 | 0.37 | 1.01 |
| Adjacent to the lateral ventricle | 0.61 | 0.21–1.71 | 0.3 | 1.01 |
| Posterior parietal lobe | 1.12 | 0.19–6.82 | 0.336 | 1.06 |
| Anterior parietal lobe | 1.1 | 0.299–6.59 | 0.9 | 1.24 |
| Middle parietal lobe | 2.79 | 0.53–14.7 | 0.22 | 1.28 |
| Posterior limb of the internal capsule | 2.37 | 0.79–7.08 | 0.121 | 1.07 |
| Anterior limb of the internal capsule | 2.04 | 0.52–7.97 | 0.3 | 1.03 |
| putamen | 0.41 | 0.14–1.22 | 0.11 | 1.04 |
| OR | 95% CI | p Value | VIF | |
|---|---|---|---|---|
| Age | 0.945 | 0.89–0.99 | 0.03 * | 1.26 |
| PVL | 6.45 | 2.25–18.5 | 0.0005 *** | 1.2 |
| Thalamus | 15.6 | 5.78–42.0 | 0.00000005 *** | 1.09 |
| Divided into the basal forebrain | 0.000006 | 0–0 | 0.993 | 1 |
| Lateral ventricle enlargement | 2.31 | 1.09–4.9 | 0.029 * | 1.04 |
| Distant from the lateral ventricle | 0.782 | 0.255–2.4 | 0.668 | 1.01 |
| Adjacent to the lateral ventricle | 1.29 | 0.612–2.71 | 0.506 | 1.01 |
| Posterior parietal lobe | 1.88 | 0.519–6.82 | 0.336 | 1.06 |
| Anterior parietal lobe | 1.1 | 0.299–4.06 | 0.884 | 1.24 |
| Middle parietal lobe | 1.07 | 0.36–3.15 | 0.909 | 1.29 |
| Posterior limb of the internal capsule | 1.76 | 0.798–3.9 | 0.161 | 1.08 |
| Anterior limb of the internal capsule | 1.3 | 0.476–3.56 | 0.607 | 1.03 |
| Putamen | 0.596 | 0.276–1.29 | 0.188 | 1.06 |
| OR | 95% CI | p Value | VIF | |
|---|---|---|---|---|
| Age | 0.812 | 0.67–0.97 | 0.02 * | 1.24 |
| PVL | 30.9 | 1.57–607 | 0.02 * | 1.42 |
| Thalamus | 241 | 7–8280 | 0.002 ** | 1.97 |
| Divided into the basal forebrain | ||||
| Lateral ventricle enlargement | 3.24 | 0.68–15.3 | 0.138 | 1.2 |
| Distant from the lateral ventricle | 0.15 | 0.009–2.44 | 0.183 | 1.09 |
| Adjacent to the lateral ventricle | 6.38 | 1.32–30.8 | 0.02 * | 1.2 |
| Posterior parietal lobe | 1.71 | 0.185–15.9 | 0.635 | 1.03 |
| Anterior parietal lobe | 6.25 | 0.389–100 | 0.196 | 1.13 |
| Middle parietal lobe | 0.158 | 0.0122–2.04 | 0.158 | 1.15 |
| Posterior limb of the internal capsule | 9.79 | 1.65–58.1 | 0.012 * | 1.63 |
| Anterior limb of the internal capsule | 3.6 | 0.19–68.5 | 0.394 | 1.04 |
| Putamen | 0.281 | 0.0496–1.59 | 0.152 | 1.6 |
| OR | 95% CI | p Value | VIF | |
|---|---|---|---|---|
| Age | 0.98 | 0.919–1.06 | 0.74 | 1.15 |
| PVL | 6.13 | 1.66–22.6 | 0.006 ** | 1.03 |
| Thalamus | 10.1 | 2.91–34.8 | 0.0002 *** | 1.14 |
| Divided into the basal forebrain | 0.000005 | 0–0 | 0.99 | 1 |
| Lateral ventricle enlargement | 1.47 | 0.552–3.91 | 0.44 | 1.03 |
| Distant from the lateral ventricle | 1.27 | 0.348–4.63 | 0.71 | 1.01 |
| Adjacent to the lateral ventricle | 0.72 | 0.262–1.99 | 0.53 | 1.04 |
| Posterior parietal lobe | 2.66 | 0.451–15.7 | 0.28 | 1.18 |
| Anterior parietal lobe | 0.21 | 0.025–1.73 | 0.14 | 1.54 |
| Middle parietal lobe | 3.49 | 0.881–13.8 | 0.07 | 1.4 |
| Posterior limb of the internal capsule | 0.36 | 0.098–1.37 | 0.13 | 1.26 |
| Anterior limb of the internal capsule | 4.43 | 1.11–17.8 | 0.03 * | 1.28 |
| Putamen | 0.32 | 0.105–1.03 | 0.056 | 1.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomita, T.; Yuminaga, H.; Takashima, H.; Masuda, T.; Mano, T. Image Findings as Predictors of Fall Risk in Patients with Cerebrovascular Disease. Brain Sci. 2023, 13, 1690. https://doi.org/10.3390/brainsci13121690
Tomita T, Yuminaga H, Takashima H, Masuda T, Mano T. Image Findings as Predictors of Fall Risk in Patients with Cerebrovascular Disease. Brain Sciences. 2023; 13(12):1690. https://doi.org/10.3390/brainsci13121690
Chicago/Turabian StyleTomita, Tatsuya, Hisanori Yuminaga, Hideki Takashima, Takashi Masuda, and Tomoo Mano. 2023. "Image Findings as Predictors of Fall Risk in Patients with Cerebrovascular Disease" Brain Sciences 13, no. 12: 1690. https://doi.org/10.3390/brainsci13121690
APA StyleTomita, T., Yuminaga, H., Takashima, H., Masuda, T., & Mano, T. (2023). Image Findings as Predictors of Fall Risk in Patients with Cerebrovascular Disease. Brain Sciences, 13(12), 1690. https://doi.org/10.3390/brainsci13121690