
Frailty as a Predictor of Outcomes in Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Eligibility
2.2. Data Extraction
2.3. Meta-Analysis: Synthesis of Results
2.4. Quality Evaluation
3. Results
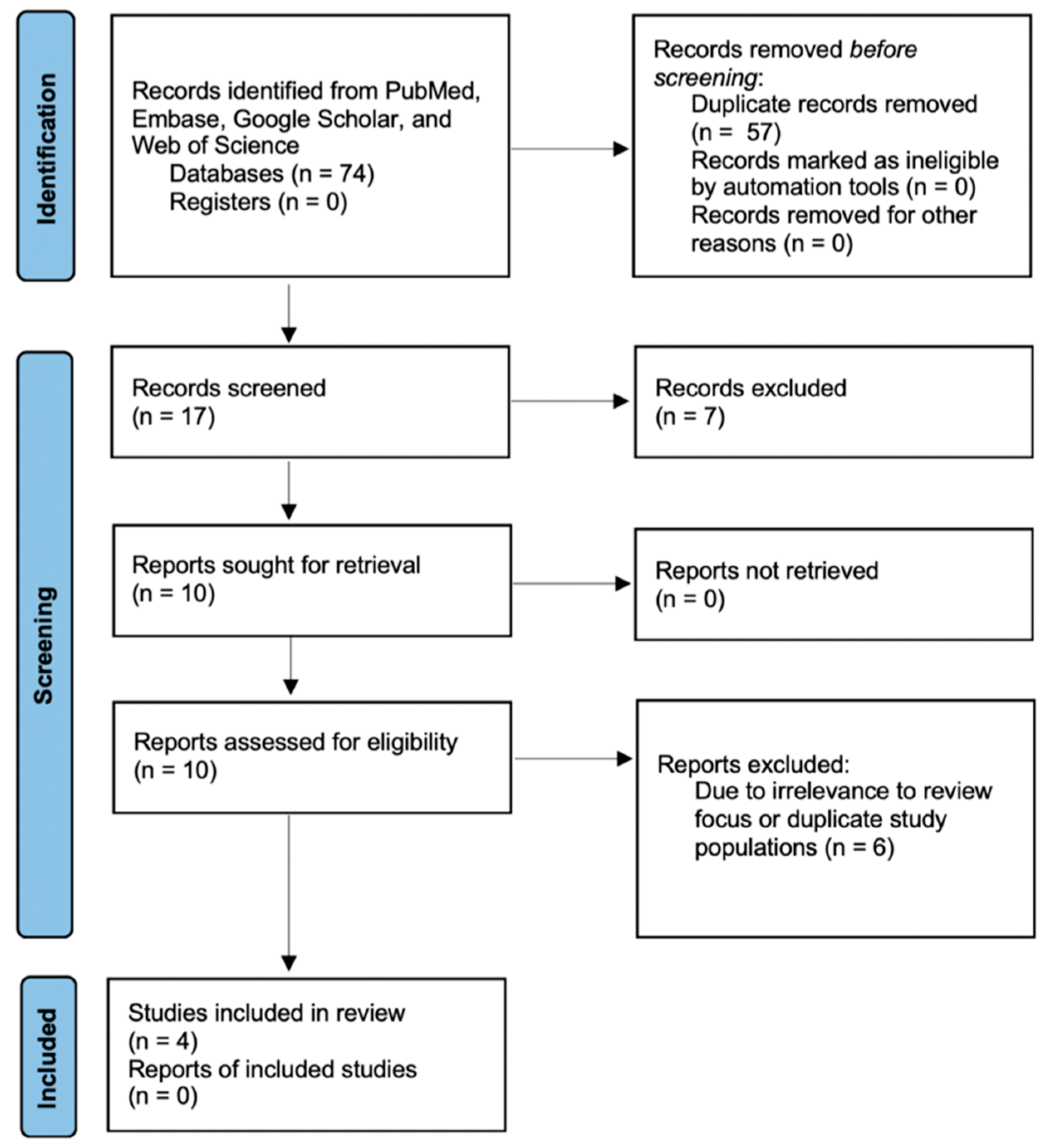
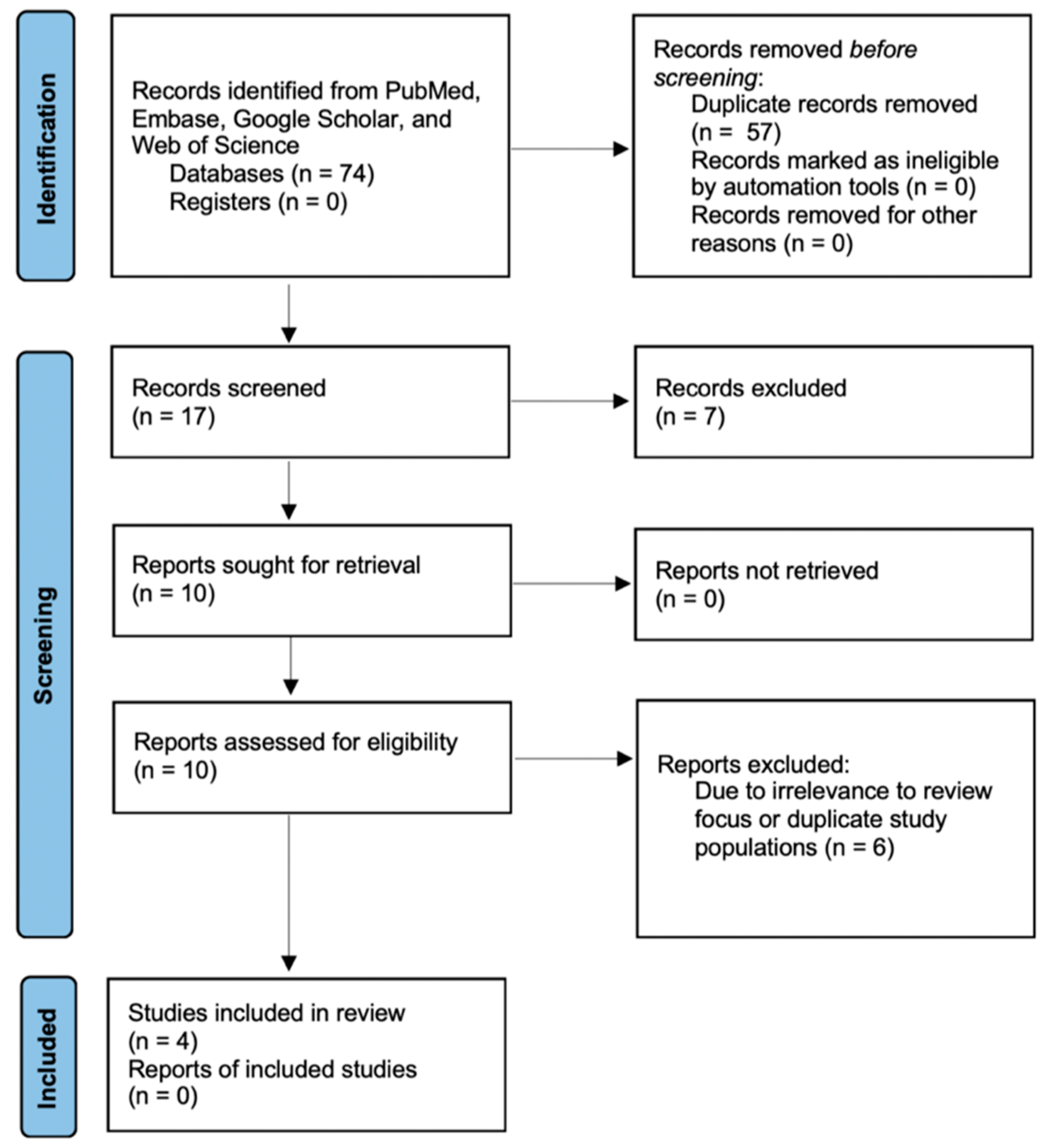
3.1. Search Results
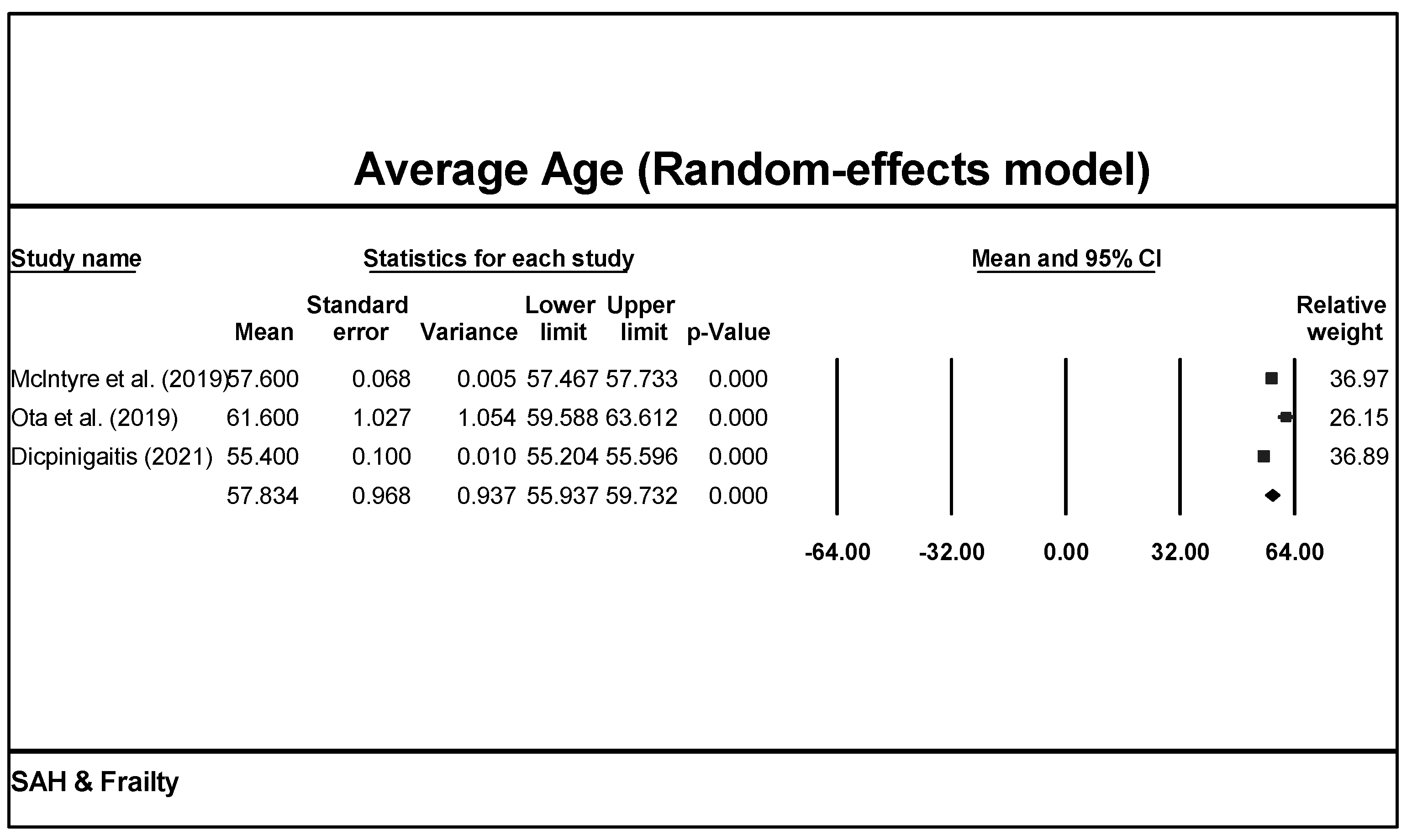
3.2. Demographics
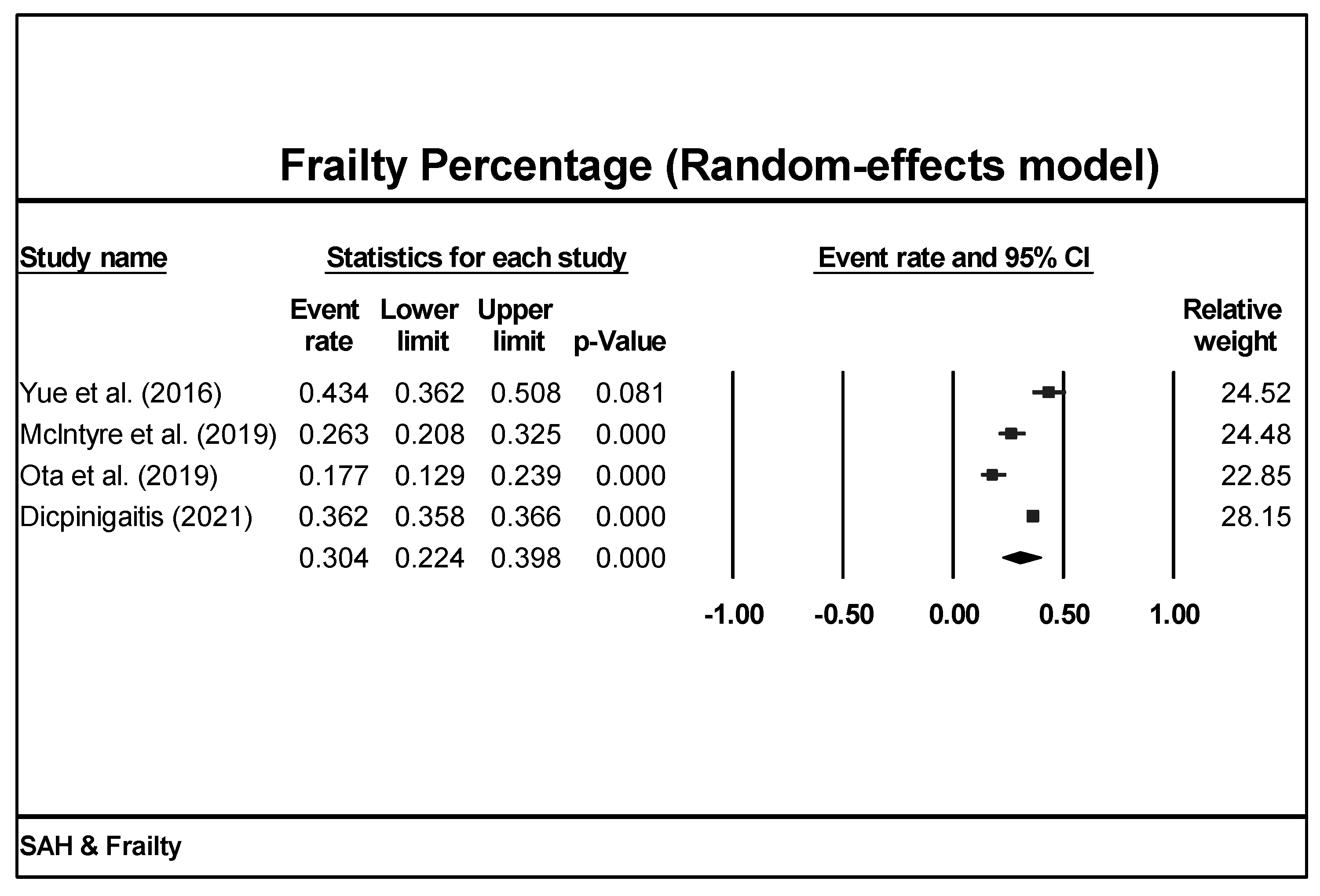
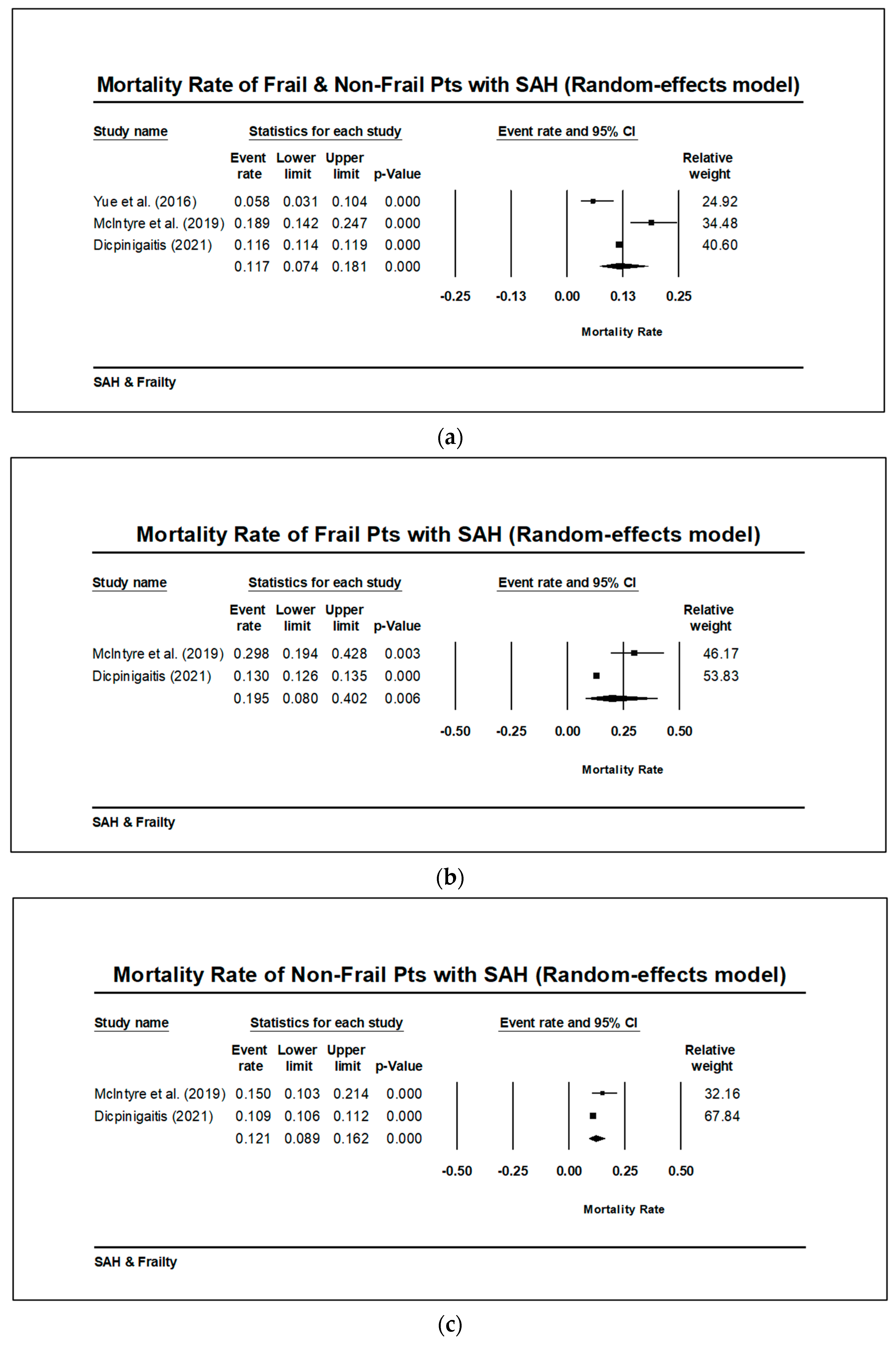
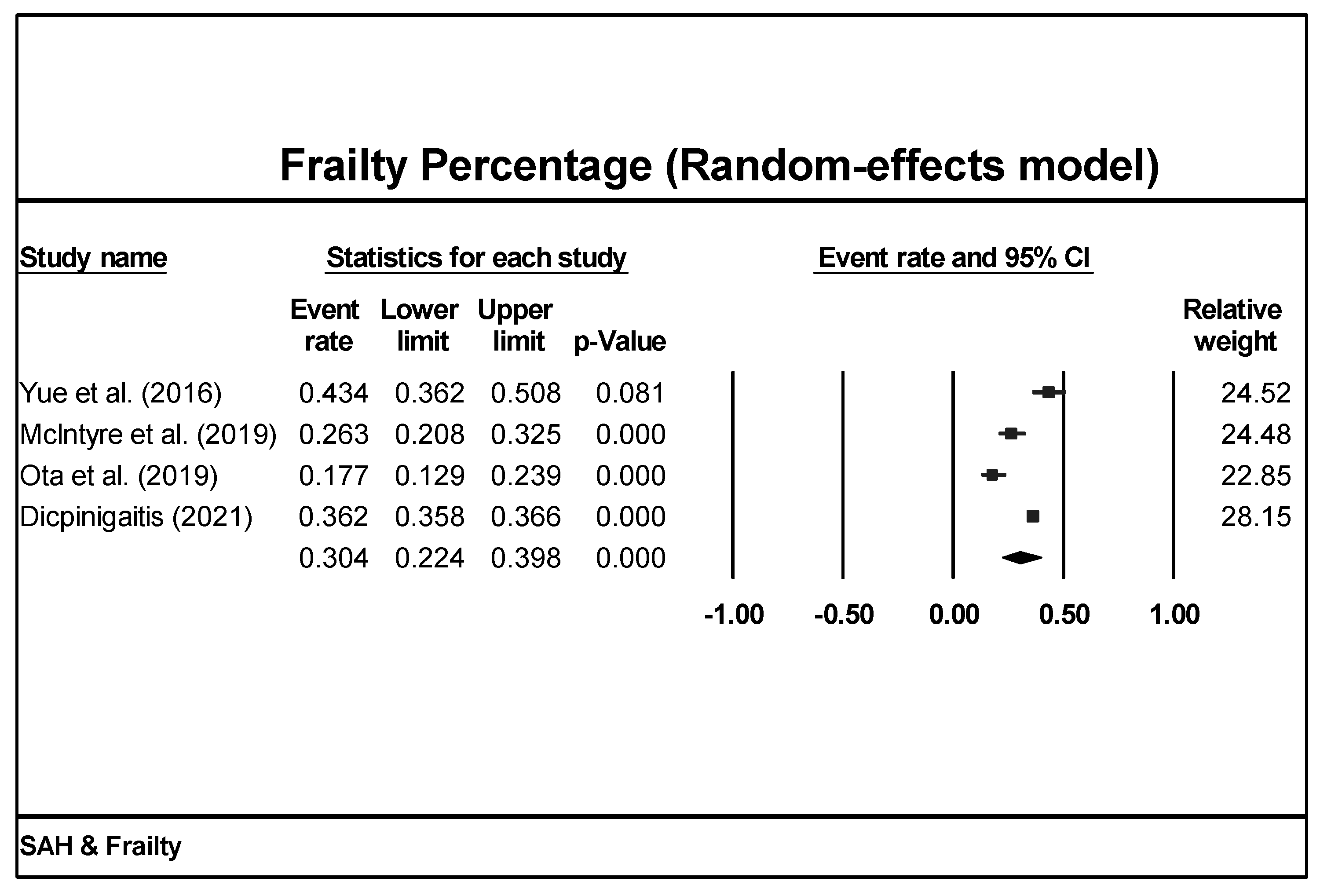
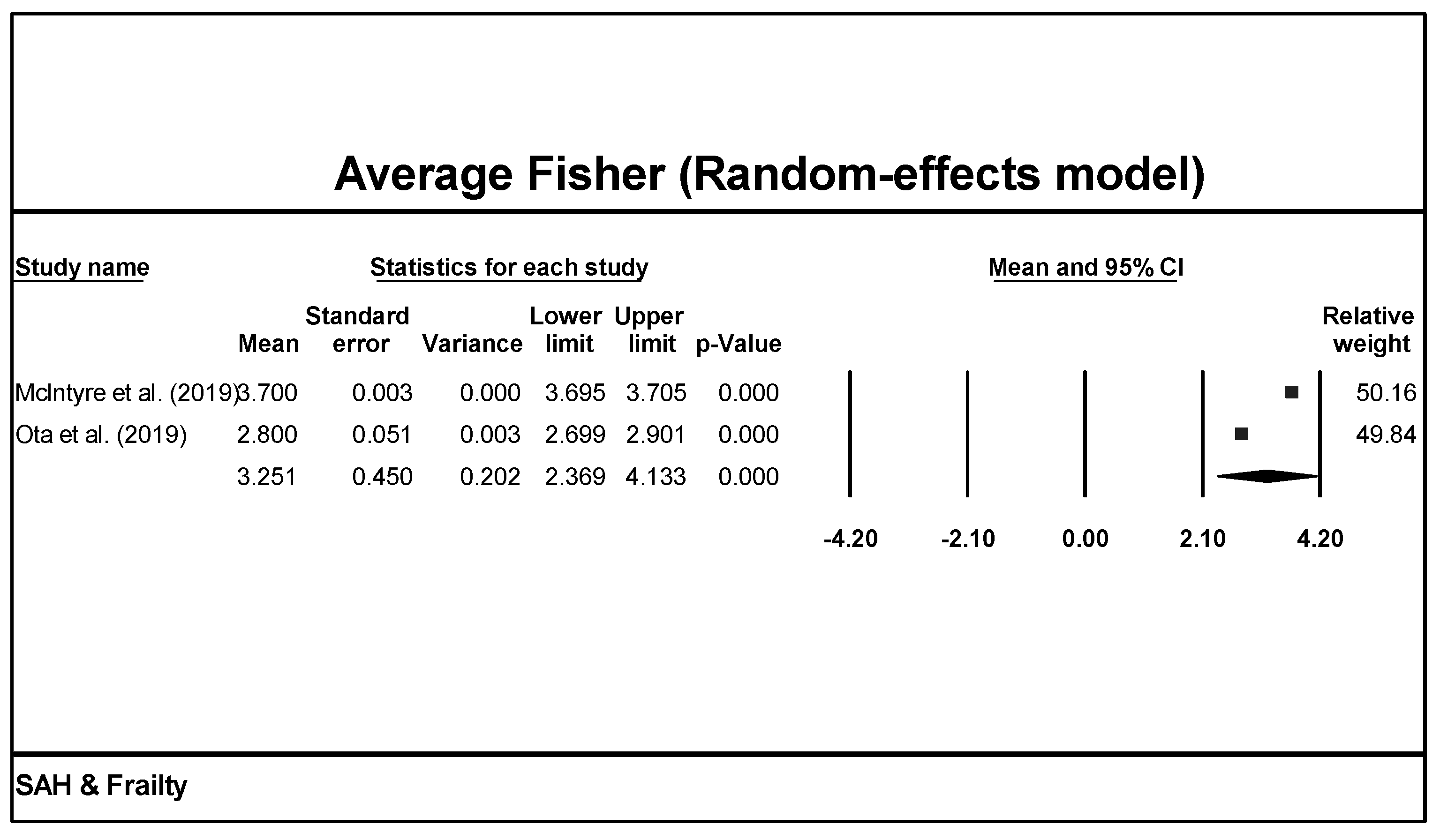
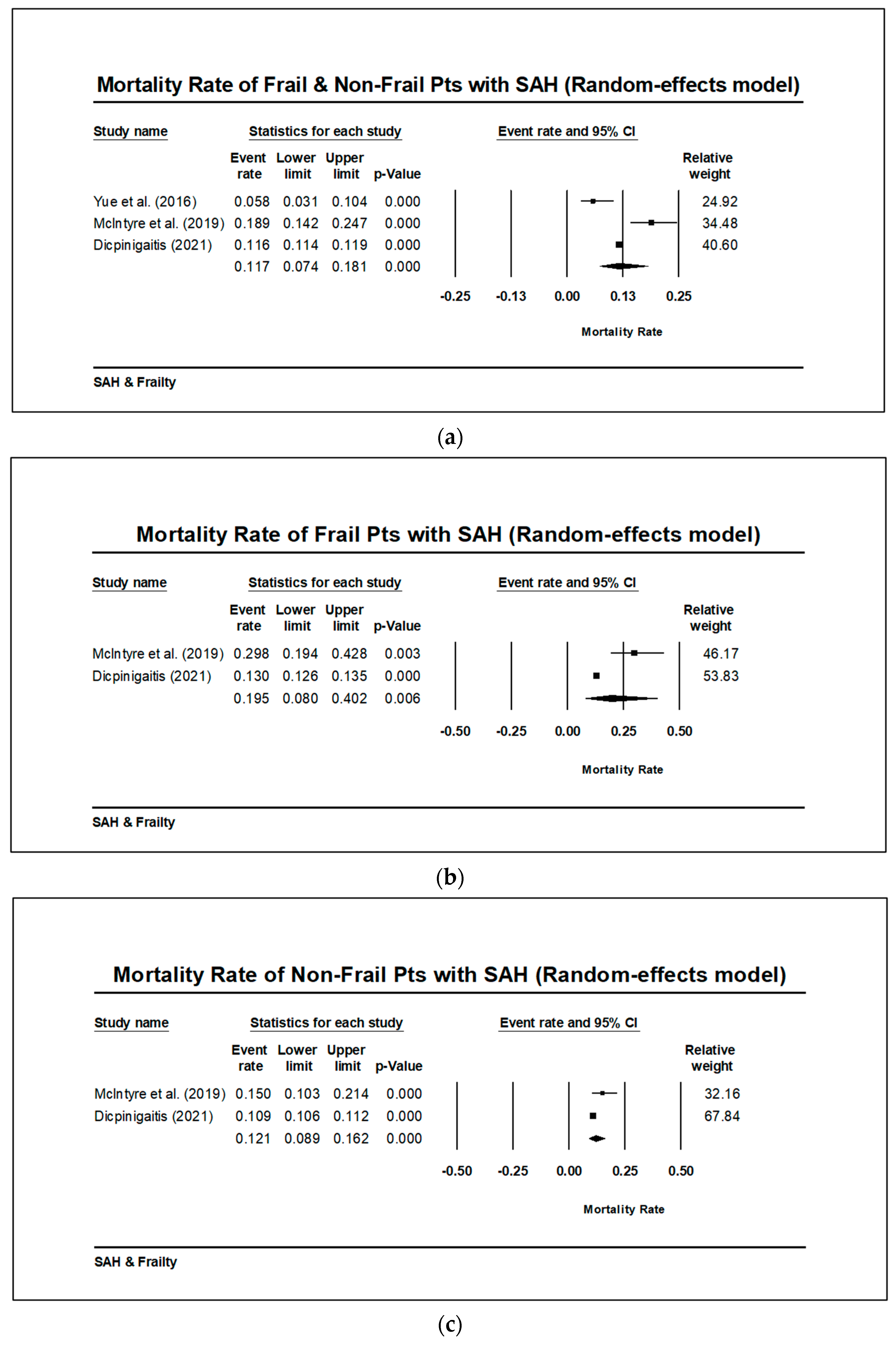
3.3. Frailty Measurements and Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buta, B.J.; Walston, J.D.; Godino, J.G.; Park, M.; Kalyani, R.R.; Xue, Q.-L.; Bandeen-Roche, K.; Varadhan, R. Frailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res. Rev. 2015, 26, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Walston, J.D.; Ferrucci, L. Frailty. In Hazzard’s Geriatric Medicine and Gerontology; Halter, J.B., Ouslander, J.G., Tinetti, M.E., et al., Eds.; McGraw-Hill Medical: New York, NY, USA, 2009; p. 631e645. [Google Scholar]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.P.; Morley, J.E.; Ong, P.; et al. Frailty: An Emerging Public Health Priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; O’Shea, D. Fitness and frailty: Opposite ends of a challenging continuum! Will the end of age discrimination make frailty assessments an imperative? Age Ageing 2013, 42, 279–280. [Google Scholar] [CrossRef]
- Cesari, M.; Pérez-Zepeda, M.U.; Marzetti, E. Frailty and Multimorbidity: Different Ways of Thinking About Geriatrics. J. Am. Med. Dir. Assoc. 2017, 18, 361–364. [Google Scholar] [CrossRef]
- Stenholm, S.; Ferrucci, L.; Vahtera, J.; O Hoogendijk, E.; Huisman, M.; Pentti, J.; Lindbohm, J.V.; Bandinelli, S.; Guralnik, J.M.; Kivimäki, M. Natural Course of Frailty Components in People Who Develop Frailty Syndrome: Evidence from Two Cohort Studies. J. Gerontol. Ser. A 2018, 74, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Voshaar, R.C.O. Prevalence of Frailty in Community-Dwelling Older Persons: A Systematic Review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of Frailty in Middle-Aged and Older Community-Dwelling Europeans Living in 10 Countries. J. Gerontol. Ser. A 2009, 64A, 675–681. [Google Scholar] [CrossRef]
- Espinoza, S.E.; Hazuda, H.P. Frailty in older Mexican-American and European American adults: Is there an ethnic disparity? J. Am. Geriatr. Soc. 2008, 56, 1744e1749. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; Mitnitski, A. Changes in relative fitness and frailty across the adult lifespan: Evidence from the Canadian National Population Health Survey. Can. Med. Assoc. J. 2011, 183, E487–E494. [Google Scholar] [CrossRef]
- Feng, Z.; Lugtenberg, M.; Franse, C.; Fang, X.; Hu, S.; Jin, C.; Raat, H. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies. PLoS ONE 2017, 12, e0178383. [Google Scholar] [CrossRef]
- Gill, T.M.; Baker, D.I.; Gottschalk, M.; Peduzzi, P.N.; Allore, H.; Byers, A. A Program to Prevent Functional Decline in Physically Frail, Elderly Persons Who Live at Home. N. Engl. J. Med. 2002, 347, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Velanovich, V.; Antoine, H.; Swartz, A.; Peters, D.; Rubinfeld, I. Accumulating deficits model of frailty and postoperative mortality and morbidity: Its application to a national database. J. Surg. Res. 2013, 183, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of Deficits as a Proxy Measure of Aging. ScientificWorldJournal 2001, 1, 323–336. [Google Scholar] [CrossRef] [PubMed]
- Leven, D.M.; Lee, N.J.; Kim, J.S.; Kothari, P.; Steinberger, J.; Guzman, J.; Skovrlj, B.; Shin, J.I.; Phan, K.; Caridi, J.M.; et al. Frailty Is Predictive of Adverse Postoperative Events in Patients Undergoing Lumbar Fusion. Glob. Spine J. 2017, 7, 529–535. [Google Scholar] [CrossRef]
- Makary, M.A.; Segev, D.L.; Pronovost, P.J.; Syin, D.; Bandeen-Roche, K.; Patel, P.; Takenaga, R.; Devgan, L.; Holzmueller, C.G.; Tian, J.; et al. Frailty as a Predictor of Surgical Outcomes in Older Patients. J. Am. Coll. Surg. 2010, 210, 901–908. [Google Scholar] [CrossRef]
- Seib, C.D.; Rochefort, H.; Chomsky-Higgins, K.; Gosnell, J.E.; Suh, I.; Shen, W.T.; Duh, Q.-Y.; Finlayson, E. Association of Patient Frailty With Increased Morbidity After Common Ambulatory General Surgery Operations. JAMA Surg. 2018, 153, 160–168. [Google Scholar] [CrossRef]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef]
- Wallace, L.M.K.; Wallace, L.M.K.; Theou, O.; Theou, O.; Godin, J.; Godin, J.; Andrew, M.K.; Andrew, M.K.; A Bennett, D.; A Bennett, D.; et al. Investigation of frailty as a moderator of the relationship between neuropathology and dementia in Alzheimer’s disease: A cross-sectional analysis of data from the Rush Memory and Aging Project. Lancet Neurol. 2019, 18, 177–184. [Google Scholar] [CrossRef]
- Perry, J.J.; Stiell, I.G.; Sivilotti, M.L.A.; Bullard, M.J.; Hohl, C.M.; Sutherland, J.; Émond, M.; Worster, A.; Lee, J.S.; Mackey, D.; et al. Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache. JAMA 2013, 310, 1248–1255. [Google Scholar] [CrossRef]
- Claassen, J.; Park, S. Spontaneous subarachnoid haemorrhage. Lancet 2022, 400, 846–862. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Hoffman, H.; Anikpezie, N.; Philip, K.; Wee, C.; Choudhry, R.; Albright, K.C.; Masoud, H.; Beutler, T.; Schmidt, E.; et al. Trends in the Incidence of Spontaneous Subarachnoid Hemorrhages in the United States, 2007–2017. Neurology 2023, 100, e123–e132. [Google Scholar] [CrossRef]
- Al-Mufti, F.; Mayer, A.S.; Kaur, G.; Bassily, D.; Li, B.; Holstein, M.L.; Ani, J.; Matluck, E.N.; Kamal, H.; Nuoman, R.; et al. Neurocritical care management of poor-grade subarachnoid hemorrhage: Unjustified nihilism to reasonable optimism. Neuroradiol. J. 2021, 34, 542–551. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, M.; Gandhi, C.; Dragonette, J.; Schmidt, M.; Cole, C.; Santarelli, J.; Lehrer, R.; Al-Mufti, F.; Bowers, C.A. Increasing Frailty Predicts Worse Outcomes and Increased Complications After Angiogram-Negative Subarachnoid Hemorrhages. World Neurosurg. 2019, 134, e181–e188. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, M.K.; Gandhi, C.; Long, A.; Van Hoof, A.; Li, B.; Patel, V.; Afridi, A.; Halabi, M.; Schmidt, M.; Cole, C.; et al. Age predicts outcomes better than frailty following aneurysmal subarachnoid hemorrhage: A retrospective cohort analysis. Clin. Neurol. Neurosurg. 2019, 187, 105558. [Google Scholar] [CrossRef]
- Yue, Q.; Liu, Y.; Leng, B.; Xu, B.; Gu, Y.; Chen, L.; Zhu, W.; Mao, Y. A Prognostic Model for Early Post-Treatment Outcome of Elderly Patients with Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2016, 95, 253–261. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ota, N.; Noda, K.; Hatano, Y.; Hashimoto, A.; Miyazaki, T.; Kondo, T.; Kinoshita, Y.; Kamiyama, H.; Tokuda, S.; Kamada, K.; et al. Preoperative Predictors and Prognosticators After Microsurgical Clipping of Poor-Grade Subarachnoid Hemorrhage: A Retrospective Study. World Neurosurg. 2019, 125, e582–e592. [Google Scholar] [CrossRef]
- Von Hippel, P.T. The heterogeneity statistic I2 can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef]
- OCEBM Levels of Evidence Working Group. The Oxford Levels of Evidence 2; Oxford Centre for Evidence-Based Medicine: Oxford, UK; Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 17 October 2023).
- Dicpinigaitis, A.J.; McIntyre, M.K.; Al-Mufti, F.; Kazim, S.F.; Li, B.; Schmidt, M.H.; Gandhi, C.D.; Cole, C.D.; Bowers, C.A. Association of baseline frailty status with clinical outcome following aneurysmal subarachnoid hemorrhage. J. Stroke Cerebrovasc. Dis. 2022, 31, 106394. [Google Scholar] [CrossRef]
- Zacharia, B.E.; Hickman, Z.L.; Grobelny, B.T.; DeRosa, P.; Kotchetkov, I.; Ducruet, A.F.; Connolly, E.S. Epidemiology of Aneurysmal Subarachnoid Hemorrhage. Neurosurg. Clin. N. Am. 2010, 21, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Shea, A.M.; Reed, S.D.; Curtis, L.H.; Alexander, M.J.; Villani, J.J.; Schulman, K.A. CHARACTERISTICS OF NONTRAUMATIC SUBARACHNOID HEMORRHAGE IN THE UNITED STATES IN 2003. Neurosurgery 2007, 61, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- van Donkelaar, C.E.; Bakker, N.A.; Birks, J.; Veeger, N.J.; Metzemaekers, J.D.; Molyneux, A.J.; Groen, R.J.; van Dijk, J.M.C. Prediction of Outcome After Aneurysmal Subarachnoid Hemorrhage. Stroke 2019, 50, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Ingall, T.; Asplund, K.; Mähönen, M.; Bonita, R. A Multinational Comparison of Subarachnoid Hemorrhage Epidemiology in the WHO MONICA Stroke Study. Stroke 2000, 31, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Rohrmann, S. Epidemiology of Frailty in Older People. Adv. Exp. Med. Biol. 2020, 1216, 21–27. [Google Scholar] [CrossRef]
- Theou, O.; Brothers, T.D.; Rockwood, M.R.; Haardt, D.; Mitnitski, A.; Rockwood, K. Exploring the relationship between national economic indicators and relative fitness and frailty in middle-aged and older Europeans. Age Ageing 2013, 42, 614–619. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Xue, Q.-L. The Frailty Syndrome: Definition and Natural History. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef]
- Lanzino, G.; Kassell, N.F.; Germanson, T.P.; Kongable, G.L.; Truskowski, L.L.; Torner, J.C.; Jane, J.A. Age and outcome after aneurysmal subarachnoid hemorrhage: Why do older patients fare worse? J. Neurosurg. 1996, 85, 410–418. [Google Scholar] [CrossRef]
- Goldberg, J.; Schoeni, D.; Mordasini, P.; Z’graggen, W.; Gralla, J.; Raabe, A.; Beck, J.; Fung, C. Survival and Outcome After Poor-Grade Aneurysmal Subarachnoid Hemorrhage in Elderly Patients. Stroke 2018, 49, 2883–2889. [Google Scholar] [CrossRef]
- Chaer, R.A.; Shen, J.; Rao, A.; Cho, J.S.; Abu Hamad, G.; Makaroun, M.S. Cerebral reserve is decreased in elderly patients with carotid stenosis. J. Vasc. Surg. 2010, 52, 569–575. [Google Scholar] [CrossRef]
- Virta, J.J.; Satopää, J.; Luostarinen, T.; Raj, R. One-Year Outcome After Aneurysmal Subarachnoid Hemorrhage in Elderly Patients. World Neurosurg. 2020, 143, e334–e343. [Google Scholar] [CrossRef]
- van Donkelaar, C.E.; Bakker, N.A.; Veeger, N.J.G.M.; Uyttenboogaart, M.; Metzemaekers, J.D.M.; Eshghi, O.; Mazuri, A.; Foumani, M.; Luijckx, G.-J.; Groen, R.J.M.; et al. Prediction of outcome after subarachnoid hemorrhage: Timing of clinical assessment. J. Neurosurg. 2017, 126, 52–59. [Google Scholar] [CrossRef]
- Mahta, A.; Murray, K.; Reznik, M.E.; Thompson, B.B.; Wendell, L.C.; Furie, K.L. Early Neurological Changes and Interpretation of Clinical Grades in Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2021, 30, 105939. [Google Scholar] [CrossRef] [PubMed]
- Koo, A.B.; Elsamadicy, A.A.; Renedo, D.; Sarkozy, M.; Sherman, J.; Reeves, B.C.; Havlik, J.; Antonios, J.; Sujijantarat, N.; Hebert, R.; et al. Higher Hospital Frailty Risk Score is associated with increased complications and healthcare resource utilization after endovascular treatment of ruptured intracranial aneurysms. J. NeuroInterventional Surg. 2022, 15, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, E.; Macdonald, P.S.; Newton, P.J.; Chang, S.; Wilhelm, K.; Jha, S.R.; Malouf, M. Reversibility of Frailty after Lung Transplantation. J. Transplant. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Li, C.-M.; Chen, C.-Y.; Li, C.-Y.; Wang, W.-D.; Wu, S.-C. The effectiveness of a comprehensive geriatric assessment intervention program for frailty in community-dwelling older people: A randomized, controlled trial. Arch. Gerontol. Geriatr. 2010, 50, S39–S42. [Google Scholar] [CrossRef]
- Stuck, A.; Siu, A.; Wieland, G.; Rubenstein, L.; Adams, J. Comprehensive geriatric assessment: A meta-analysis of controlled trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef]
- Van Craen, K.; Braes, T.; Wellens, N.; Denhaerynck, K.; Flamaing, J.; Moons, P.; Boonen, S.; Gosset, C.; Petermans, J.; Milisen, K. The Effectiveness of Inpatient Geriatric Evaluation and Management Units: A Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2009, 58, 83–92. [Google Scholar] [CrossRef]
- De Almeida Mello, J.; Hermans, K.; Van Audenhove, C.; Macq, J.; Declercq, A. Evaluations of home care interventions for frail older persons using the interRAI Home Care instrument: A systematic review of the literature. J. Am. Med. Dir. Assoc. 2015, 16, 173.e1-10. [Google Scholar] [CrossRef] [PubMed]
- Ellis, G.; Whitehead, M.A.; Robinson, D.; O’neill, D.; Langhorne, P. Comprehensive geriatric assessment for older adults admitted to hospital: Meta-analysis of randomised controlled trials. BMJ 2011, 343, d6553. [Google Scholar] [CrossRef]
- Walston, J.; Buta, B.; Xue, Q.-L. Frailty Screening and Interventions: Considerations for clinical practice. Clin. Geriatr. Med. 2018, 34, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Vetrano, D.L.; Palmer, K.M.; Galluzzo, L.; Giampaoli, S.; Marengoni, A.; Bernabei, R.; Onder, G. Hypertension and frailty: A systematic review and meta-analysis. BMJ Open 2018, 8, e024406. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.-T.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Denfeld, Q.E.; Winters-Stone, K.; Mudd, J.O.; Gelow, J.M.; Kurdi, S.; Lee, C.S. The prevalence of frailty in heart failure: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 236, 283–289. [Google Scholar] [CrossRef]
- Gutiérrez-Valencia, M.; Izquierdo, M.; Cesari, M.; Casas-Herrero, Á.; Inzitari, M.; Martínez-Velilla, N. The relationship between frailty and polypharmacy in older people: A systematic review. Br. J. Clin. Pharmacol. 2018, 84, 1432–1444. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Samaniego, L.L.; Bernabei, R.; Onder, G.; Rodríguez-Mañas, L.; et al. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A 2018, 74, 659–666. [Google Scholar] [CrossRef]
- Aguayo, G.A.; Donneau, A.-F.; Vaillant, M.T.; Schritz, A.; Franco, O.H.; Stranges, S.; Malisoux, L.; Guillaume, M.; Witte, D.R. Agreement Between 35 Published Frailty Scores in the General Population. Am. J. Epidemiol. 2017, 186, 420–434. [Google Scholar] [CrossRef]
- Al Saedi, A.; Feehan, J.; Phu, S.; Duque, G. Current and emerging biomarkers of frailty in the elderly. Clin. Interv. Aging 2019, ume 14, 389–398. [Google Scholar] [CrossRef]
- Rodríguez-Mañas, L.; Féart, C.; Mann, G.; Viña, J.; Chatterji, S.; Chodzko-Zajko, W.; Harmand, M.G.-C.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an Operational Definition of Frailty: A Delphi Method Based Consensus Statement. The Frailty Operative Definition-Consensus Conference Project. J. Gerontol. Ser. A 2012, 68, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Calvani, R.; Marini, F.; Cesari, M.; Tosato, M.; Anker, S.D.; Von Haehling, S.; Miller, R.R.; Bernabei, R.; Landi, F.; Marzetti, E.; et al. Biomarkers for physical frailty and sarcopenia: State of the science and future developments. J. Cachexia Sarcopenia Muscle 2015, 6, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Coelho-Junior, H.J.; Calvani, R.; Marzetti, E.; Vetrano, D.L. Biomarkers shared by frailty and sarcopenia in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 73, 101530. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Author (Year) | Assessments | Scoring System |
|---|---|---|---|
| Physical Frailty Phenotype (PFP) | Fried et al. (2001) [13] | Weight loss (0 or 1), decreased grip strength (0 or 1), exhaustion (0 or 1), low activity (0 or 1), 10 m walking speed (0 or 1) | 0: non-frail 1–2: pre-frail *3–5: frail |
| Frailty Index (FI) | Mitnitski et al. (2001) [15] | 92 total variables that reflect severity of illness or presence of comorbidities | 0 or 1 for each selected variable |
| Modified Frailty Index (mFI) | Velanovich et al. (2013) [14] | 11 total variables that focus on accumulated deficits, including history of diabetes mellitus, chronic obstructive pulmonary disease, congestive heart failure, myocardial infarction, history of coronary intervention, hypertension medication, peripheral vascular disease, impaired sensorium, transient ischemic attack or cerebrovascular accident, and cerebrovascular accident with deficit | 0 or 1 for each variable |
| Gill Frailty Measure | Gill et al. (2002) [12] | 10 physician-diagnosed chronic conditions and 8 activities of daily living | 0 or 1 for each variable |
| Author (Year) | Country | Setting | Study Type (Number of Patients) | Years of Study | Eligible Age (Year) | Patient Age in Years (n) | Number of Cases | Level of Evidence |
|---|---|---|---|---|---|---|---|---|
| Yue et al. (2016) [27] | China | Single center | Retrospective (109) and Prospective (64) | 12/2010 to 12/2013 | ≥60 | categories, 60–69 (134), 70–79 (32), >80 (7) | 173 | 2b |
| Mclntyre et al. (2019) [26] | USA | Single center | Retrospective | 06/2014 to 07/2018 | no restriction | mean, 57.6 ± 1.0 range, 14–98 | 217 | 2b |
| Ota et al. (2019) [29] | Japan | Single center | Retrospective | 04/2012 to 03/2017 | no restriction | mean, 61.6 ± 14 | 186 | 2b |
| Dicpinigaitis et al. (2022) [32] | USA | Multi- center | Retrospective | 2010 to 2018 | ≥18 | mean, 55.4 ± 0.1 | 64,102 | 2b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fortunato, M.; Lin, F.; Uddin, A.; Subah, G.; Patel, R.; Feldstein, E.; Lui, A.; Dominguez, J.; Merckling, M.; Xu, P.; et al. Frailty as a Predictor of Outcomes in Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Brain Sci. 2023, 13, 1498. https://doi.org/10.3390/brainsci13101498
Fortunato M, Lin F, Uddin A, Subah G, Patel R, Feldstein E, Lui A, Dominguez J, Merckling M, Xu P, et al. Frailty as a Predictor of Outcomes in Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Brain Sciences. 2023; 13(10):1498. https://doi.org/10.3390/brainsci13101498
Chicago/Turabian StyleFortunato, Michael, Fangyi Lin, Anaz Uddin, Galadu Subah, Rohan Patel, Eric Feldstein, Aiden Lui, Jose Dominguez, Matthew Merckling, Patricia Xu, and et al. 2023. "Frailty as a Predictor of Outcomes in Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis" Brain Sciences 13, no. 10: 1498. https://doi.org/10.3390/brainsci13101498
APA StyleFortunato, M., Lin, F., Uddin, A., Subah, G., Patel, R., Feldstein, E., Lui, A., Dominguez, J., Merckling, M., Xu, P., McIntyre, M., Gandhi, C., & Al-Mufti, F. (2023). Frailty as a Predictor of Outcomes in Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Brain Sciences, 13(10), 1498. https://doi.org/10.3390/brainsci13101498