

Obsessive–Compulsive Symptoms in Children Are Related to Sensory Sensitivity and to Seeking Proxies for Internal States


Abstract
1. Introduction
2. Method
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analyses
3. Results
3.1. Demographic Characteristics
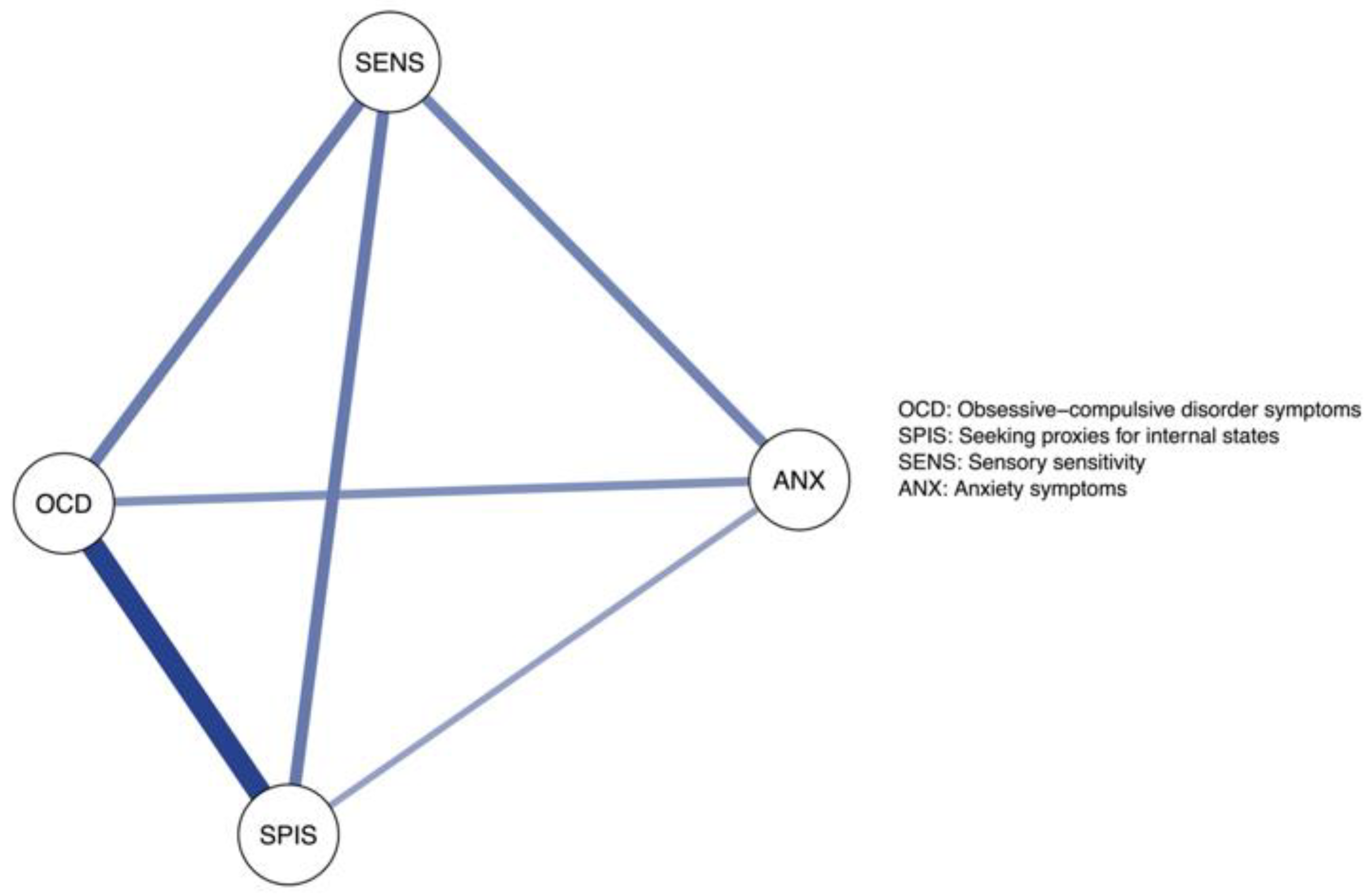
3.2. Linear Regression, Dominance Analysis, and Network Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Cervin, M. Obsessive-compulsive disorder: Diagnosis, clinical features, nosology, and epidemiology. Psychiatr. Clin. 2023, 46, 1–16. [Google Scholar] [CrossRef]
- Cervin, M.; Miguel, E.C.; Güler, A.S.; Ferrão, Y.A.; Erdoğdu, A.B.; Lazaro, L.; Gökçe, S.; Geller, D.A.; Yulaf, Y.; Başgül, Ş.S.; et al. Towards a definitive symptom structure of obsessive−compulsive disorder: A factor and network analysis of 87 distinct symptoms in 1366 individuals. Psychol. Med. 2022, 52, 3267–3279. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.E.; Rosario, M.C.; Brown, T.A.; Carter, A.S.; Leckman, J.F.; Sukhodolsky, D.; Katsovitch, L.; King, R.; Geller, D.; Pauls, D.L. Principal components analysis of obsessive–compulsive disorder symptoms in children and adolescents. Biol. Psychiatry 2007, 61, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Lewin, A.B.; Wu, M.S.; Murphy, T.K.; Storch, E.A. Sensory over-responsivity in pediatric obsessive-compulsive disorder. J. Psychopathol. Behav. Assess. 2015, 37, 134–143. [Google Scholar] [CrossRef]
- Gomes de Alvarenga, P.; de Mathis, M.A.; Dominguez Alves, A.C.; do Rosario, M.C.; Fossaluza, V.; Hounie, A.G.; Miguel, E.C.; Torres, A.R. Clinical features of tic-related obsessive-compulsive disorder: Results from a large multicenter study. CNS Spectr. 2012, 17, 87–93. [Google Scholar] [CrossRef]
- Miguel, E.C.; Baer, L.; Coffey, B.J.; Rauch, S.L.; Savage, C.R.; O’Sullivan, R.L.; Phillips, K.; Moretti, C.; Leckman, J.F.; Jenike, M.A. Phenomenological differences appearing with repetitive behaviours in obsessive-compulsive disorder and Gilles de la Tourette’s syndrome. Br. J. Psychiatry 1997, 170, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Bloch, M.H.; Landeros-Weisenberger, A.; Rosario, M.C.; Pittenger, C.; Leckman, J.F. Meta-analysis of the symptom structure of obsessive-compulsive disorder. Am. J. Psychiatry 2008, 165, 1532–1542. [Google Scholar] [CrossRef]
- Öst, L.G.; Riise, E.N.; Wergeland, G.J.; Hansen, B.; Kvale, G. Cognitive behavioral and pharmacological treatments of OCD in children: A systematic review and meta-analysis. J. Anxiety Disord. 2016, 43, 58–69. [Google Scholar] [CrossRef]
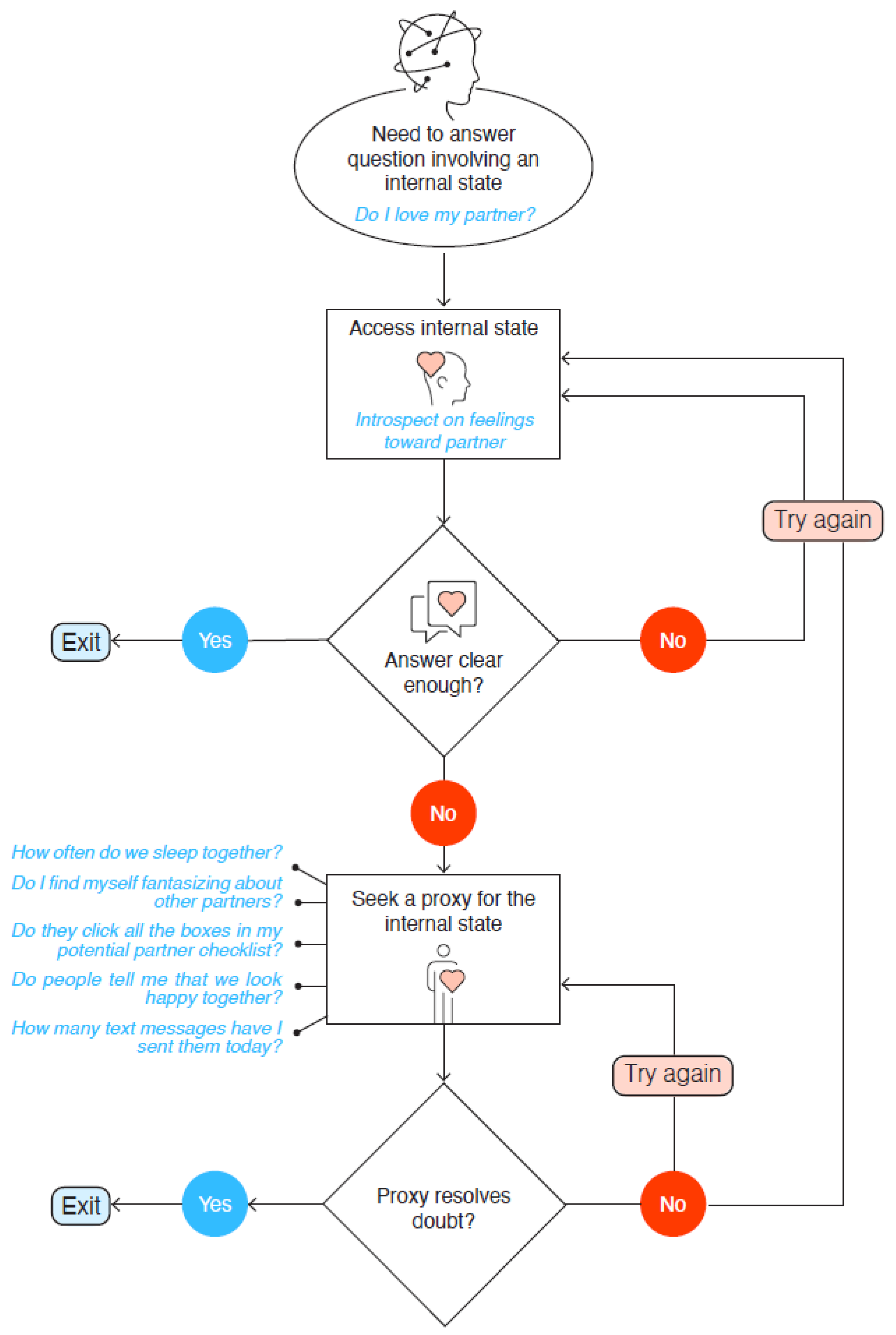
- Dar, R.; Lazarov, A.; Liberman, N. Seeking proxies for internal states (SPIS): Towards a novel model of obsessive-compulsive disorder. Behav. Res. Ther. 2021, 147, 103987. [Google Scholar] [CrossRef]
- Liberman, N.; Lazarov, A.; Dar, R. Obsessive-compulsive disorder: The underlying role of diminished access to internal states. Curr. Dir. Psychol. Sci. 2023, 32, 118–124. [Google Scholar] [CrossRef]
- Bart, O.; Bar-Shalita, T.; Mansour, H.; Dar, R. Relationships among sensory responsiveness, anxiety, and ritual behaviors in children with and without atypical sensory responsiveness. Phys. Occup. Ther. Pediatr. 2017, 37, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Ben-Sasson, A.; Podoly, T.Y. Sensory over responsivity and obsessive compulsive symptoms: A cluster analysis. Compr. Psychiatry 2017, 73, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Cervin, M. Sensory processing difficulties in children and adolescents with obsessive-compulsive and anxiety disorders. Res. Child Adolesc. Psychopathol. 2023, 51, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Conelea, C.A.; Carter, A.C.; Freeman, J.B. Sensory over-responsivity in a sample of children seeking treatment for anxiety. J. Dev. Behav. Pediatr. 2014, 35, 510–521. [Google Scholar] [CrossRef]
- Dar, R.; Kahn, D.T.; Carmeli, R. The relationship between sensory processing, childhood rituals, and obsessive-compulsive symptoms. J. Behav. Ther. Exp. Psychiatry 2012, 43, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Houghton, D.C.; Stein, D.J.; Cortese, B.M. Exteroceptive sensory abnormalities in childhood and adolescent anxiety and obsessive-compulsive disorder: A critical review. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Amador, B.; Cervin, M.; Martínez-González, A.; Piqueras, J. OCD-Spectrum Spain Research Group Sensory Overresponsivity and Symptoms Across the Obsessive-Compulsive Spectrum: Web-Based Longitudinal Observational Study. J. Med. Internet Res. 2023, 25, e37847. [Google Scholar] [CrossRef]
- Van Hulle, C.A.; Esbensen, K.; Goldsmith, H.H. Co-occurrence of sensory over-responsivity with obsessive-compulsive symptoms in childhood and early adolescence. J. Dev. Behav. Pediatr. JDBP 2019, 40, 377. [Google Scholar] [CrossRef]
- Rossi, S.; Bartalini, S.; Ulivelli, M.; Mantovani, A.; Di Muro, A.; Goracci, A.; Castrogiovanni, P.; Battistini, N.; Passero, S. Hypofunctioning of sensory gating mechanisms in patients with obsessive-compulsive disorder. Biol. Psychiatry 2005, 57, 16–20. [Google Scholar] [CrossRef]
- Russo, M.; Naro, A.; Mastroeni, C.; Morgante, F.; Terranova, C.; Muscatello, M.R.; Zoccali, R.; Calabrò, R.S.; Quartarone, A. Obsessive-compulsive disorder: A “sensory-motor” problem? Int. J. Psychophysiol. 2014, 92, 74–78. [Google Scholar] [CrossRef]
- Miller, L.J.; Lane, S.J. Toward a consensus in terminology in sensory integration theory and practice: Part 1: Taxonomy of neurophysiological processes. Sens. Integr. Spec. Interest Sect. Q. 2000, 23, 1–4. [Google Scholar]
- Brown, C.E.; Dunn, W. Adolescent/Adult Sensory Profile: User’s Manual; Psychological Corporation: Washington, DC, USA, 2002. [Google Scholar] [CrossRef]
- Carter, A.S.; Ben-Sasson, A.; Briggs-Gowan, M.J. Sensory over-responsivity, psychopathology, and family impairment in school-aged children. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.J.; Anzalone, M.E.; Lane, S.J.; Cermak, S.A.; Osten, E.T. Concept evolution in sensory integration: A proposed nosology for diagnosis. Am. J. Occup. Ther. 2007, 61, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W. The impact of sensory processing abilities on the daily lives of young children and their families: A conceptual model. Infants Young Child. 1997, 9, 23–35. [Google Scholar] [CrossRef]
- Dunn, W. The sensations of everyday life: Empirical, theoretical, and pragmatic considerations. Am. J. Occup. Ther. 2001, 55, 608–620. [Google Scholar] [CrossRef]
- Rieke, E.F.; Anderson, D. Adolescent/adult sensory profile and obsessive-compulsive disorder. Am. J. Occup. Ther. 2009, 63, 138–145. [Google Scholar] [CrossRef]
- Hazen, E.P.; Reichert, E.L.; Piacentini, J.C.; Miguel, E.C.; Do Rosario, M.C.; Pauls, D.; Geller, D.A. Case series: Sensory intolerance as a primary symptom of pediatric OCD. Ann. Clin. Psychiatry 2008, 20, 199–203. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fonagy, P. Affect Regulation, Mentalization, and the Development of the Self; Other Press: New York, NY, USA, 2002. [Google Scholar]
- Fonagy, P.; Steele, M.; Steele, H.; Moran, G.S.; Higgitt, A.C. The Capacity for Understanding Mental States—The Reflective Self in Parent and Child and Its Significance for Security of Attachment. Infant Ment. Health J. 1991, 12, 201–218. [Google Scholar] [CrossRef]
- Slade, A. Parental reflective functioning: An introduction. Attach. Hum. Dev. 2005, 7, 269–281. [Google Scholar] [CrossRef]
- Rohrer, J.M.; Hünermund, P.; Arslan, R.C.; Elson, M. That’sa lot to PROCESS! Pitfalls of popular path models. Adv. Methods Pract. Psychol. Sci. 2022, 5, 25152459221095827. [Google Scholar]
- Foa, E.B.; Coles, M.; Huppert, J.D.; Pasupuleti, R.V.; Franklin, M.E.; March, J. Development and validation of a child version of the obsessive-compulsive inventory. Behav. Ther. 2010, 41, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Jiménez, T.; Piqueras, J.A.; Lázaro, L.; Moreno, E.; Ortiz, A.G.; Godoy, A. Metric invariance, reliability, and validity of the Child Version of the Obsessive-Compulsive Inventory (OCI-CV) in community and clinical samples. J. Obs.-Compuls. Relat. Disord. 2016, 9, 1–8. [Google Scholar] [CrossRef]
- Cervin, M.; Garcia-Delgar, B.; Calvo, R.; Ortiz, A.E.; Lazaro, L. Symptom dimension breakpoints for the obsessive-compulsive inventory-child version (OCI-CV). Child Psychiatry Hum. Dev. 2023, 54, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Liberman, N.; Dar, R. Obsessive-compulsive tendencies are related to seeking proxies for internal states in everyday life. J. Behav. Ther. Exp. Psychiatry 2018, 61, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W. Sensory Profile: User’s Manual; Psychological Corporation: Washington, DC, USA, 1999. [Google Scholar] [CrossRef]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale construction and psychometric characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Brent, D.A.; Chiappetta, L.; Bridge, J.; Monga, S.; Baugher, M. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Azen, R.; Budescu, D.V. The dominance analysis approach for comparing predictors in multiple regression. Psychol. Methods 2003, 8, 129. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Fried, E.I. A tutorial on regularized partial correlation networks. Psychol. Methods 2018, 23, 617. [Google Scholar] [CrossRef]
- Lazarov, A.; Dar, R.; Oded, Y.; Liberman, N. Are obsessive-compulsive tendencies related to reliance on external proxies for internal states? Evidence from biofeedback-aided relaxation studies. Behav. Res. Ther. 2010, 48, 516–523. [Google Scholar] [CrossRef]
- Lazarov, A.; Liberman, N.; Hermesh, H.; Dar, R. Seeking proxies for internal states in obsessive–compulsive disorder. J. Abnorm. Psychol. 2014, 123, 695. [Google Scholar] [CrossRef]
- Sullivan, H.S. The Collected Works of Harry Stack Sullivan (Vol. 1): The Interpersonal Theory of Psychiatry; Perry, H.S., Gawel, M.L., Eds.; W.W. Norton: Singapore, 1953. [Google Scholar]
- Higgins, E.T. Shared-Reality Development in Childhood. Perspect. Psychol. Sci. 2016, 11, 466–495. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, M. A Natural History of Human Thinking; Harvard University Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Leckman, J.F.; Bloch, M.H. A developmental and evolutionary perspective on obsessive-compulsive disorder: Whence and whither compulsive hoarding? Am. J. Psychiatry 2008, 165, 1229–1233. [Google Scholar] [CrossRef] [PubMed]
- Lazarov, A.; Dar, R.; Liberman, N.; Oded, Y. Obsessive-compulsive tendencies and undermined confidence are related to reliance on proxies for internal states in a false feedback paradigm. J. Behav. Ther. Exp. Psychiatry 2012, 43, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Lazarov, A.; Cohen, T.; Liberman, N.; Dar, R. Can doubt attenuate access to internal states? Implications for obsessive-compulsive disorder. J. Behav. Ther. Exp. Psychiatry 2015, 49, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Steinman, S.A.; Ahmari, S.E.; Choo, T.; Kimeldorf, M.B.; Feit, R.; Loh, S.; Risbrough, V.; Geyer, M.A.; Steinglass, J.E.; Wall, M.; et al. Prepulse inhibition deficits only in females with obsessive compulsive disorder. Depress. Anxiety 2016, 33, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Geller, D.A.; Biederman, J.; Faraone, S.; Agranat, A.; Cradock, K.; Hagermoser, L.; Kim, G.; Frazier, J.; Coffey, B.J. Developmental aspects of obsessive-compulsive disorder: Findings in children, adolescents, and adults. J. Nerv. Ment. Dis. 2001, 189, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.E.; Geller, D.A.; Jenike, M.; Pauls, D.; Shaw, D.; Mullin, B.; Faraone, S.V. Long-term outcome of pediatric obsessive–compulsive disorder: A meta-analysis and qualitative review of the literature. Acta Psychiatr. Scand. 2004, 110, 4–13. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| M (SD) | Min–Max | Skewness | Kurtosis | |
|---|---|---|---|---|
| SPISI-CV Total Score | 41.60 (14.07) | 21–95 | 0.56 | −0.13 |
| OTHS Total Score | 21.38 (7.49) | 12–49 | 1.02 | 0.24 |
| OCI-CV Total score | 31.44 (10.61) | 21–75 | 1.40 | 1.93 |
| OCI-CV Doubting/checking | 6.80 (2.51) | 5–20 | 1.99 | 4.72 |
| OCI-CV Obsessing | 6.40 (2.81) | 4–17 | 1.39 | 1.67 |
| OCI-CV Ordering | 4.91 (2.55) | 3–15 | 1.50 | 1.68 |
| OCI-CV Washing | 4.33 (2.00) | 3–12 | 1.67 | 2.28 |
| SCARED Total Score | 7.40 (1.99) | 5–14 | 0.99 | 0.35 |
| Full Sample | OCI-CV | SPISI-CV | OTHS | SCARED |
|---|---|---|---|---|
| OCI-CV | - | 0.71 * | 0.59 * | 0.49 * |
| SPISI-CV | - | 0.59 * | 0.47 * | |
| OTHS | - | 0.48 * | ||
| SCARED | - | |||
| Girls (above diagonal) Boys (below diagonal) | OCI-CV | SPISI-CV | OTHS | SCARED |
| OCI-CV | - | 0.72 * | 0.55 * | 0.50 * |
| SPISI-CV | 0.68 * | - | 0.60 * | 0.44 * |
| OTHS | 0.65 * | 0.57 * | - | 0.49 * |
| SCARED | 0.47 * | 0.51 * | 0.47 * | - |
| Mothers (above diagonal) Father (below diagonal) | OCI-CV | SPISI-CV | OTHS | SCARED |
| OCI-CV | - | 0.72 * | 0.60 * | 0.44 * |
| SPISI-CV | 0.68 * | - | 0.59 * | 0.44 * |
| OTHS | 0.57 * | 0.57 * | - | 0.41 * |
| SCARED | 0.54 * | 0.50 * | 0.56 * | - |
| Independent Variable | β | 95% Confidence Interval for β | p |
|---|---|---|---|
| Seeking proxies for internal states | 0.51 | 0.43–0.59 | <0.001 |
| Sensory sensitivity | 0.22 | 0.14–0.31 | <0.001 |
| Anxiety symptoms | 0.15 | 0.07–0.22 | <0.001 |
| Age | 0.03 | −0.04–0.09 | 0.43 |
| Gender | −0.02 | −0.08–0.05 | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tal, I.; Cervin, M.; Liberman, N.; Dar, R. Obsessive–Compulsive Symptoms in Children Are Related to Sensory Sensitivity and to Seeking Proxies for Internal States. Brain Sci. 2023, 13, 1463. https://doi.org/10.3390/brainsci13101463
Tal I, Cervin M, Liberman N, Dar R. Obsessive–Compulsive Symptoms in Children Are Related to Sensory Sensitivity and to Seeking Proxies for Internal States. Brain Sciences. 2023; 13(10):1463. https://doi.org/10.3390/brainsci13101463
Chicago/Turabian StyleTal, Ilil, Matti Cervin, Nira Liberman, and Reuven Dar. 2023. "Obsessive–Compulsive Symptoms in Children Are Related to Sensory Sensitivity and to Seeking Proxies for Internal States" Brain Sciences 13, no. 10: 1463. https://doi.org/10.3390/brainsci13101463
APA StyleTal, I., Cervin, M., Liberman, N., & Dar, R. (2023). Obsessive–Compulsive Symptoms in Children Are Related to Sensory Sensitivity and to Seeking Proxies for Internal States. Brain Sciences, 13(10), 1463. https://doi.org/10.3390/brainsci13101463