

Retrospective Study Shows That Serum Levels of Chemokine CXCL10 and Cytokine GDF15 Support a Diagnosis of Sporadic Inclusion Body Myositis and Immune-Mediated Necrotizing Myopathy


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects and Materials
2.2. Quantification of Serum CXCL10 and GDF15 Levels
2.3. Immunofluorescence, Immunohistochemistry and Histochemistry
3. Results
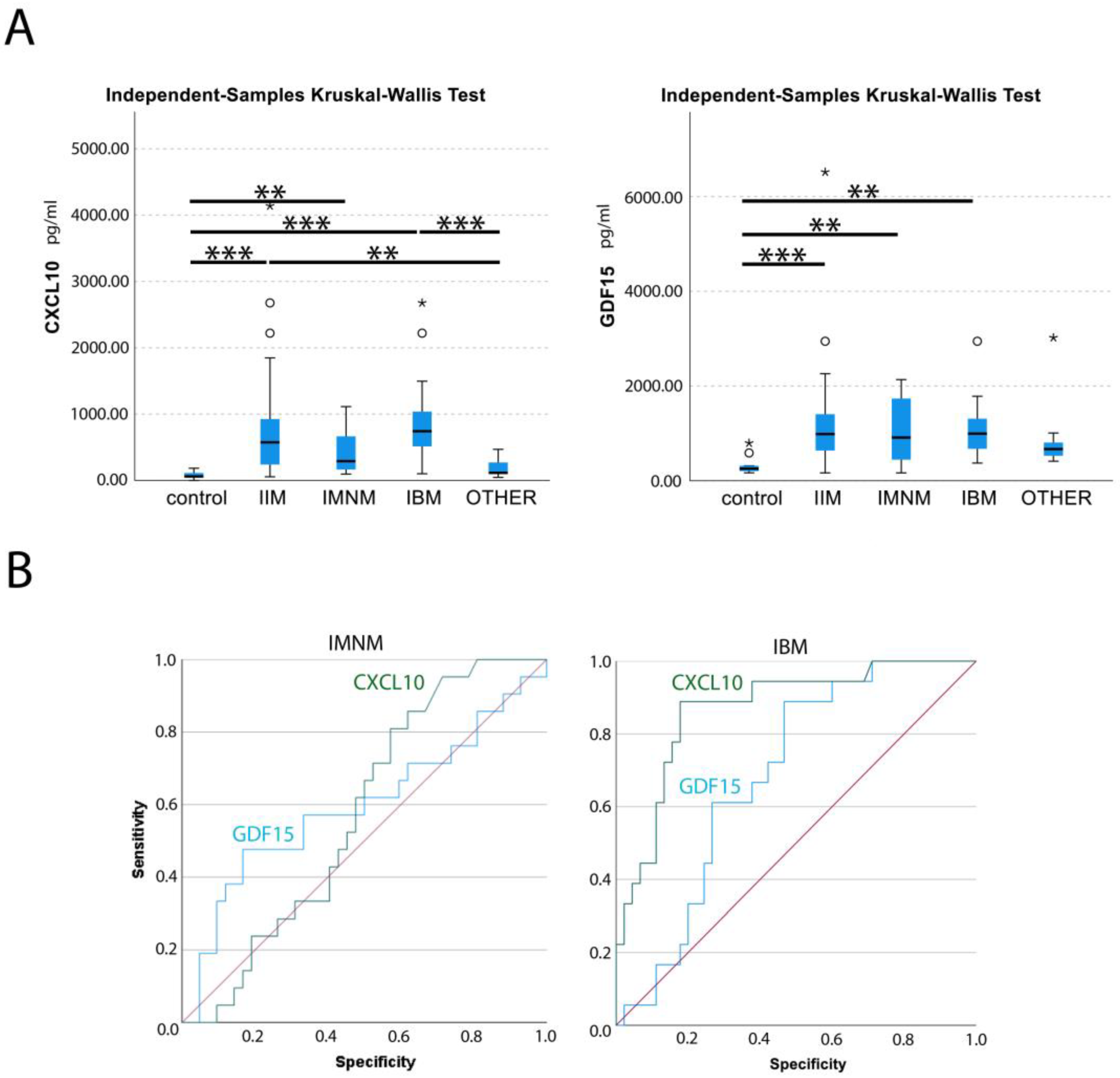
3.1. Increased CXCL10 and GDF15 Levels in IIM Sera
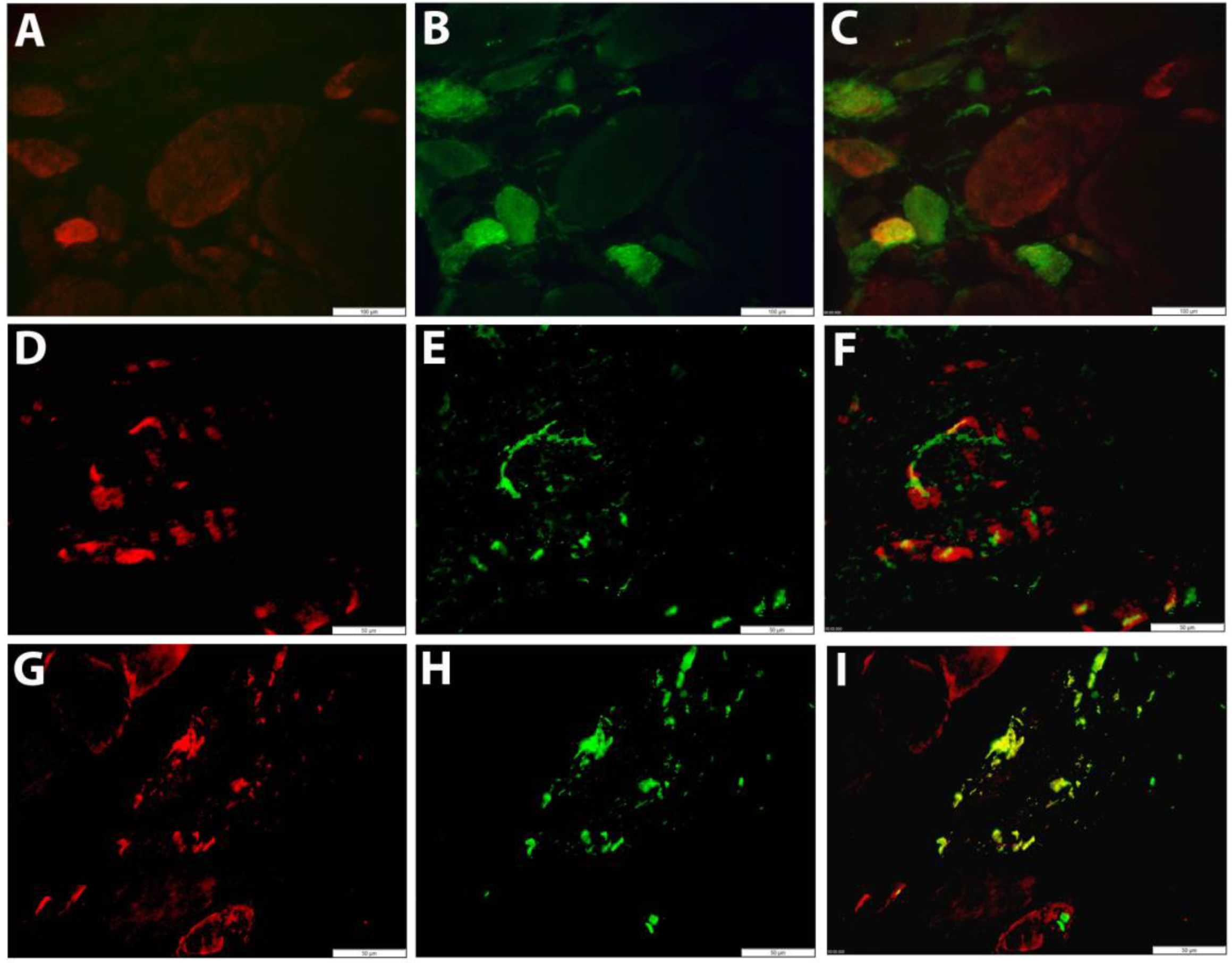
3.2. Localization of CXCL10 to Muscle Fibers and Actively Invading Inflammatory Cells
3.3. Co-Localization of GDF15 with Markers of Autophagy and Regeneration in Muscle Fibers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (second of two parts). N. Engl. J. Med. 1975, 292, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Targoff, I.N.; Miller, F.W.; Medsger, T.A., Jr.; Oddis, C.V. Classification criteria for the idiopathic inflammatory myopathies. Curr. Opin. Rheumatol. 1997, 9, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Griggs, R.C.; Askanas, V.; DiMauro, S.; Engel, A.; Karpati, G.; Mendell, J.R.; Rowland, L.P. Inclusion body myositis and myopathies. Ann. Neurol. 1995, 38, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Amlani, A.; Choi, M.Y.; Tarnopolsky, M.; Brady, L.; Clarke, A.E.; Garcia-De La Torre, I.; Mahler, M.; Schmeling, H.; Barber, C.E.; Jung, M.; et al. Anti-NT5c1A Autoantibodies as Biomarkers in Inclusion Body Myositis. Front. Immunol. 2019, 10, e745. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, J.E.; Amato, A.A.; Lecky, B.R.; Choy, E.H.; Lundberg, I.E.; Rose, M.R.; Vencovsky, J.; de Visser, M.; Hughes, R.A. 119th ENMC international workshop: Trial design in adult idiopathic inflammatory myopathies, with the exception of inclusion body myositis, 10–12 October 2003, Naarden, The Netherlands. Neuromuscul. Disord. 2004, 14, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Lin, Y.; Qiao, L.; Chen, J.; Shi, Q. Characteristics of cardiac involvement in immune-mediated necrotizing myopathy. Front. Immunol. 2023, 14, e1094611. [Google Scholar] [CrossRef] [PubMed]
- Wells, M.; Alawi, S.; Thin, K.Y.M.; Gunawardena, H.; Brown, A.R.; Edey, A.; Pauling, J.D.; Barratt, S.L.; Adamali, H.I. A multidisciplinary approach to the diagnosis of antisynthetase syndrome. Front. Med. 2022, 9, 959653. [Google Scholar] [CrossRef]
- De Bleecker, J.L.; De Paepe, B.; Aronica, E.; de Visser, M.; Amato, A.; Aronica, E.; Benveniste, O.; De Bleecker, J.; de Boer, O.; De Paepe, B.; et al. 205th ENMC International Workshop: Pathology diagnosis of idiopathic inflammatory myopathies Part II 28–30 March 2014, Naarden, The Netherlands. Neuromuscul. Disord. 2015, 25, 268–272. [Google Scholar] [CrossRef]
- Mageriu, V.; Manole, E.; Bastian, A.E.; Staniceanu, F. Role of myokines in myositis pathogenesis and their potential to be new therapeutic targets in idiopathic inflammatory myopathies. J. Immunol. Res. 2020, 2020, 9079083. [Google Scholar] [CrossRef]
- Deyhle, M.R.; Hafen, P.S.; Parmley, J.; Preece, C.N.; Robison, M.; Sorensen, J.R.; Jackson, B.; Eggett, D.L.; Hancock, C.R.; Hyldahl, R.D. CXCL10 increases in human skeletal muscle following damage but is not necessary for muscle regeneration. Physiol. Rep. 2018, 6, e13689. [Google Scholar] [CrossRef] [PubMed]
- Raju, R.; Vasconcelos, O.; Granger, R.; Dalakas, M.C. Expression of IFN-γ-inducible chemokines in inclusion body myositis. J. Neuroimmunol. 2003, 141, 125–131. [Google Scholar] [CrossRef] [PubMed]
- De Paepe, B.; De Keyzer, K.; Martin, J.J.; De Bleecker, J.L. Alpha-chemokine receptors CXCR1–3 and their ligands in idiopathic inflammatory myopathies. Acta Neuropathol. 2005, 109, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Limongi, F. The CXCR3 chemokines in inflammatory myopathies. Clin. Ter. 2015, 166, e56–e61. [Google Scholar] [CrossRef] [PubMed]
- Szodoray, P.; Philip Alex, P.; Nicholas Knowlton, N.; Centola, M.; Dozmorov, I.; Csipo, I.; Nagy, A.T.; Constantin, T.; Ponyi, A.; Nakken, B.; et al. Idiopathic inflammatory myopathies, signified by distinctive peripheral cytokines, chemokines and the TNF family members B-cell activating factor and a proliferation inducing ligand. Rheumatology 2010, 49, 1867–1877. [Google Scholar] [CrossRef] [PubMed]
- Uruha, A.; Noguchi, S.; Sato, W.; Nishimura, H.; Mitsuhashi, S.; Yamamura, T.; Nishino, I. Plasma IP-10 level distinguishes inflammatory myopathy. Neurology 2015, 85, 293–294. [Google Scholar] [CrossRef] [PubMed]
- Wienke, J.; Bellutti Enders, F.; Lim, J.; Mertens, J.S.; van den Hoogen, L.L.; Wijngaarde, C.A.; Yeo, J.G.; Meyer, A.; Otten, H.G.; Fritsch-Stork, R.D.E.; et al. Galectin-9 and CXCL10 as Biomarkers for Disease Activity in Juvenile Dermatomyositis: A Longitudinal Cohort Study and Multicohort Validation. Arthritis Rheumatol. 2019, 71, 1377–1390. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhao, L.; Xiao, Y.; Xie, S.; Long, Y.; Wei, Y.; Meng, Q.; Li, X.; Luo, H.; Zhu, H. The Expression of Cytokine Profiles and Related Receptors in Idiopathic Inflammatory Myopathies. Front. Pharmacol. 2022, 13, e852055. [Google Scholar] [CrossRef]
- Fuchs, T.; Trollor, J.N.; Crawford, J.; Baune, B.T.; Samaras, K.; Campbell, L.; Breit, S.N.; Brodaty, H.; Sachdev, P.; Smith, E.; et al. Macrophage inhibitory cytokine-1 is associated with cognitive impairment and predicts cognitive decline—The Sydney Memory and Aging Study. Neurol. Psychiatr. Brain Res. 2014, 20, 9. [Google Scholar] [CrossRef]
- De Paepe, B.; Verhamme, F.; De Bleecker, J.L. The myokine GDF-15 is a potential biomarker for myositis and associates with the protein aggregates of sporadic inclusion body myositis. Cytokine 2020, 127, e154966. [Google Scholar] [CrossRef]
- Oikawa, Y.; Izumi, R.; Koide, M.; Hagiwara, Y.; Kanzaki, M.; Suzuki, N.; Kikuchi, K.; Matsuhashi, T.; Akiyama, Y.; Ichijo, M.; et al. Mitochondrial dysfunction underlying sporadic inclusion body myositis is ameliorated by the mitochondrial homing drug MA-5. PLoS ONE 2020, 15, e0231064. [Google Scholar] [CrossRef] [PubMed]
- Qiu, M.; Sun, X.; Qi, X.; Liu, X.; Zhang, Y.; Zhang, N.; Lu, F.; Liu, W.; Changjing, F.; Wang, Q.; et al. The diagnostic value of GDF-15 for myocardial involvement in idiopathic inflammatory myopathy. Rheumatology 2021, 60, 2826–2833. [Google Scholar] [CrossRef] [PubMed]
- Weeding, E.; Tiniakou, E. Therapeutic Management of Immune-Mediated Necrotizing Myositis. Curr. Treat. Options Rheumatol. 2021, 7, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Junior, H.J.; Picca, A.; Calvani, R.; Uchida, M.C.; Marzetti, E. If my muscle could talk: Myokines as a biomarker of frailty. Exp. Gerontol. 2019, 127, e110715. [Google Scholar] [CrossRef] [PubMed]
- Corinaldesi, C.; Ross, R.L.; Abignano, G.; Antinozzi, C.; Marampon, F.; di Luigi, L.; Buch, M.H.; Riccieri, V.; Lenzi, A.; Crescioli, C.; et al. Muscle Damage in Systemic Sclerosis and CXCL10: The Potential Therapeutic Role of PDE5 Inhibition. Int. J. Mol. Sci. 2021, 22, 2894. [Google Scholar] [CrossRef] [PubMed]
- Ogundele, M.; Zhang, J.S.; Goswami, M.V.; Barbieri, M.L.; Dang, U.J.; Novak, J.S.; Hoffman, E.P.; Nagaraju, K.; CINRG-DNHS Investigators; Hathout, Y. Validation of Chemokine Biomarkers in Duchenne Muscular Dystrophy. Life 2021, 11, 827. [Google Scholar] [CrossRef]
- De Paepe, B. The Cytokine Growth Differentiation Factor-15 and Skeletal Muscle Health: Portrait of an Emerging Widely Applicable Disease Biomarker. Int. J. Mol. Sci. 2022, 23, 13180. [Google Scholar] [CrossRef] [PubMed]
- May, B.M.; Pimentel, M.; Zimerman, L.I.; Rohde, L.E. GDF-15 as a Biomarker in Cardiovascular Disease. Arq. Bras. Cardiol. 2021, 116, 494–500. [Google Scholar]
- Wang, Y.; Jiang, T.; Jiang, M.; Gu, S. Appraising growth differentiation factor 15 as a promising biomarker in digestive system tumors: A meta-analysis. BMC Cancer 2019, 19, e177. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Qiu, Y.; Zhou, M.; Chen, M.; Hu, Y.; Hong, S.; Jiang, L.; Guo, Y. Circulating FGF21 and GDF15 as Biomarkers for Screening, Diagnosis, and Severity Assessment of Primary Mitochondrial Disorders in Children. Front. Pediatr. 2022, 10, e851534. [Google Scholar] [CrossRef]
- Pedersen, B.; Febbraio, M. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Gil, C.I.; Ost, M.; Kasch, J.; Schumann, S.; Heider, S.; Klaus, S. Role of GDF15 in active lifestyle induced metabolic adaptations and acute exercise response in mice. Sci. Rep. 2019, 9, e20120. [Google Scholar] [CrossRef] [PubMed]
- Morrow, R.M.; Picard, M.; Derbeneva, O.; Leipzig, J.; McManus, M.J.; Gouspillou, G.; Barbat-Artigas, S.; Dos Santos, C.; Hepple, R.T.; Murdock, D.G.; et al. Mitochondrial energy deficiency leads to hyperproliferation of skeletal muscle mitochondria and enhanced insulin sensitivity. Proc. Natl. Acad. Sci. USA 2017, 114, 2705–2727. [Google Scholar] [CrossRef] [PubMed]
- Ishiuchi, Y.; Sato, H.; Tsujimura, K.; Kawaguchi, H.; Matsuwaki, T.; Yamanouchi, K.; Nishihara, M.; Nedachi, T. Skeletal muscle cell contraction reduces a novel myokine, chemokine (C-X-C motif) ligand 10 (CXCL10): Potential roles in exercise-regulated angiogenesis. Biosci. Biotechnol. Biochem. 2018, 82, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.G.; Brown, D.A.; Fairlie, W.D.; Bauskin, A.R.; Brown, P.K.; Munier, M.L.C.; Russell, P.K.; Salamonsen, L.A.; Wallace, E.M.; Breit, S.N. The Transforming Growth Factor-β Superfamily Cytokine Macrophage Inhibitory Cytokine-1 Is Present in High Concentrations in the Serum of Pregnant Women. J. Clin. Endocrinol. Metab. 2000, 85, 4781–4788. [Google Scholar] [CrossRef] [PubMed]
- Oba, K.; Ishikawa, J.; Tamura, Y.; Fujita, Y.; Ito, M.; Iizuka, A.; Fujiwara, Y.; Kodera, R.; Toba, A.; Toyoshima, K.; et al. Serum growth differentiation factor 15 level is associated with muscle strength and lower extremity function in older patients with cardiometabolic disease. Geriatr. Gerontol. Int. 2020, 20, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Herpich, C.; Franz, K.; Ost, M.; Otten, L.; Coleman, V.; Klaus, S.; Müller-Werdan, U.; Norman, K. Associations Between Serum GDF15 Concentrations, Muscle Mass, and Strength Show Sex-Specific Differences in Older Hospital Patients. Rejuvenation Res. 2021, 24, 14–19. [Google Scholar] [CrossRef]
- Welsh, P.; Kimenai, D.M.; Marioni, R.E.; Hayward, C.; Campbell, A.; Porteous, D.; Mills, N.L.; O’Rahilly, S.; Sattar, N. Reference ranges for GDF-15, and risk factors associated with GDF-15, in a large general population cohort. Clin. Chem. Lab. Med. 2022, 60, 1820–1829. [Google Scholar] [CrossRef]
- Vila, G.; Riedl, M.; Anderwald, C.; Resl, M.; Handisurya, A.; Clodi, M.; Prager, G.; Ludvik, B.; Krebs, M.; Luger, A. The relationship between insulin resistance and the cardiovascular biomarker growth differentiation factor-15 in obese patients. Clin. Chem. 2011, 57, 309–316. [Google Scholar] [CrossRef]
- Carballo-Casla, A.; García-Esquinas, E.; Buño-Soto, A.; Struijk, E.A.; López-García, E.; Rodríguez-Artalejo, F.; Ortolá, R. Metabolic syndrome and Growth Differentiation Factor 15 in older adults. GeroScience 2022, 44, 867–880. [Google Scholar] [CrossRef]
- Badowski, M.; Darbouze, L.; Harris, D.T. Evaluation of biobanked blood spot cards to detect cytokines in blood. Cytotherapy 2020, 22, S139–S140. [Google Scholar] [CrossRef]
- Morales, M.; Alayi, T.D.; Tawalbeh, S.M.; Sydenstricker, A.V.; Spathis, R.; Kim, H.; Nagaraju, K.; Hathout, Y.; Rider, L.G. Urine proteomics by mass spectrometry identifies proteins involved in key pathogenic pathways in patients with juvenile dermatomyositis. Rheumatology 2023, 62, 3161–3168. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gomez, M.V.; Pizarro-Sanchez, S.; Gracia-Iguacel, C.; Cano, S.; Cannata-Ortiz, P.; Sanchez-Rodriguez, J.; Sanz, A.B.; Sanchez-Niño, M.D.; Ortiz, A. Urinary Growth Differentiation Factor-15 (GDF15) levels as a biomarker of adverse outcomes and biopsy findings in chronic kidney disease. J. Nephrol. 2021, 34, 1819–1832. [Google Scholar] [CrossRef]
- Manole, E.; Ceafalan, L.C.; Popescu, B.O.; Dumitru, C.; Bastian, A.E. Myokines as Possible Therapeutic Targets in Cancer Cachexia. J. Immunol. Res. 2018, 22, e8260742. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | ID | Gender | Age | BMI | CK | Autoantibodies | Medication | Associated Disease/Comorbidities |
|---|---|---|---|---|---|---|---|---|
| IMNM | 01 | F | 67 | 33 | 1417 | HMGCR+ | GC IVIG | Myocardial infarction, Hashimoto’s thyroiditis, diabetes |
| 02 | F | 77 | 25 | 2614 | HMGCR+ | |||
| 03 | F | 60 | 24 | 6923 | HMGCR+ | Cancer | ||
| 04 | M | 61 | 27 | 851 | HMGCR+ | STAT | Cerebellar ataxia, diabetes, obstructive sleep apnea | |
| 05 | F | 76 | 30 | 7000 | HMGCR+ | STAT GC | Sjogren’s syndrome, diabetes | |
| 06 | F | 74 | 22 | 10,899 | HMGCR+ | STAT | Diabetes | |
| 07 | M | 73 | 31 | 7855 | HMGCR+ | STAT | ||
| 08 | F | 70 | 25 | 9356 | HMGCR+ | STAT | Pneumocystis pneumonia, ischemic heart disease, diabetes | |
| 09 | F | 72 | 20 | 5572 | HMGCR+ | STAT | ||
| 10 | M | 68 | 26 | 1889 | HMGCR+ | STAT | Coronary heart disease | |
| 11 | M | 73 | >25 | 4876 | HMGCR+ | STAT | Coronary heart disease, diabetes | |
| 12 | F | 60 | 22 | 5749 | HMGCR+ | GC | ||
| 13 | F | 56 | 23 | 6144 | SRP+ | GC IVIG TNF | ||
| 14 | F | 65 | 20 | 6168 | SRP+ | STAT | ||
| 15 | M | 67 | 23 | 609 | SAE1+ | STAT GC | Diabetes | |
| 16 | F | 68 | 31 | 100 | Ro52+ | GC | Sudeck dystrophy, diabetes, diverticulitis | |
| 17 | F | 53 | 22 | 233 | PM/Scl75+ | |||
| 18 | F | 74 | 21 | 3000 | ND | GC | Hypothyroidism, heart failure | |
| 19 | M | 46 | 26 | 10,264 | ND | GC | RA | |
| 20 | M | 57 | 29 | 400 | ND | GC | RA, atherosclerosis | |
| 21 | F | 53 | 31 | 150 | ND | GC | ||
| IBM | 01 | M | 73 | 21 | 170 | cN1A+ | GC | |
| 02 | F | 68 | 19 | 262 | cN1A+ | |||
| 03 | M | 72 | 22 | 128 | cN1A+ | GC | ||
| 04 | M | 76 | 25 | 186 | cN1A+ | |||
| 05 | M | 62 | 25 | 513 | cN1A+ | |||
| 06 | F | 61 | 20 | 717 | cN1A- | |||
| 07 | F | 75 | 21 | 290 | cN1A- | RA | ||
| 08 | F | 82 | 24 | 160 | cN1A- | |||
| 09 | F | 70 | 25 | 658 | cN1A- | Cancer | ||
| 10 | M | 76 | >25 | 399 | cN1A- | GC β-BL | Pericarditis | |
| 11 | M | 72 | 25 | 68 | cN1A- | STAT GC | Hypercholestrolemia | |
| 12 | M | 66 | 24 | 579 | cN1A- | IVIG | Psoriasis, diabetes, atherosclerosis | |
| 13 | F | 64 | 31 | 134 | cN1A- | STAT | Hashimoto’s thyroiditis | |
| 14 | M | 70 | 22 | 118 | ND | GC | RA, COPD | |
| 15 | M | 73 | <25 | 303 | ND | |||
| 16 | M | 66 | <25 | 626 | ND | Diabetes, hypercholesterolemia | ||
| 17 | M | 61 | 26 | 356 | ND | |||
| 18 | M | 84 | >25 | 180 | ND | Myocardial infarction, Hashimoto’s thyroiditis | ||
| OM | 01 | F | 42 | 23 | 542 | GC | Sjogren’s syndrome | |
| 02 | M | 56 | 24 | 462 | cN1A- | Spondyloarthritis, coronary heart disease | ||
| 03 | M | 70 | 27 | 308 | SSA+ Ro52+ | RA, cancer, diabetes | ||
| DM | 01 | F | 57 | <25 | 2139 | Mi2+ | GC | |
| 02 | M | 44 | ND | 1616 | ND | |||
| ASS | 01 | F | 61 | 23 | 3046 | Ro52+ Jo1+ | ILD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Paepe, B.; Bracke, K.R.; De Bleecker, J.L. Retrospective Study Shows That Serum Levels of Chemokine CXCL10 and Cytokine GDF15 Support a Diagnosis of Sporadic Inclusion Body Myositis and Immune-Mediated Necrotizing Myopathy. Brain Sci. 2023, 13, 1369. https://doi.org/10.3390/brainsci13101369
De Paepe B, Bracke KR, De Bleecker JL. Retrospective Study Shows That Serum Levels of Chemokine CXCL10 and Cytokine GDF15 Support a Diagnosis of Sporadic Inclusion Body Myositis and Immune-Mediated Necrotizing Myopathy. Brain Sciences. 2023; 13(10):1369. https://doi.org/10.3390/brainsci13101369
Chicago/Turabian StyleDe Paepe, Boel, Ken R. Bracke, and Jan L. De Bleecker. 2023. "Retrospective Study Shows That Serum Levels of Chemokine CXCL10 and Cytokine GDF15 Support a Diagnosis of Sporadic Inclusion Body Myositis and Immune-Mediated Necrotizing Myopathy" Brain Sciences 13, no. 10: 1369. https://doi.org/10.3390/brainsci13101369
APA StyleDe Paepe, B., Bracke, K. R., & De Bleecker, J. L. (2023). Retrospective Study Shows That Serum Levels of Chemokine CXCL10 and Cytokine GDF15 Support a Diagnosis of Sporadic Inclusion Body Myositis and Immune-Mediated Necrotizing Myopathy. Brain Sciences, 13(10), 1369. https://doi.org/10.3390/brainsci13101369