




Clopidogrel with Aspirin versus Aspirin Alone following Intravenous Thrombolysis in Minor Stroke: A 1-Year Follow-Up Study
 and
and 
Abstract
1. Introduction
2. Methods
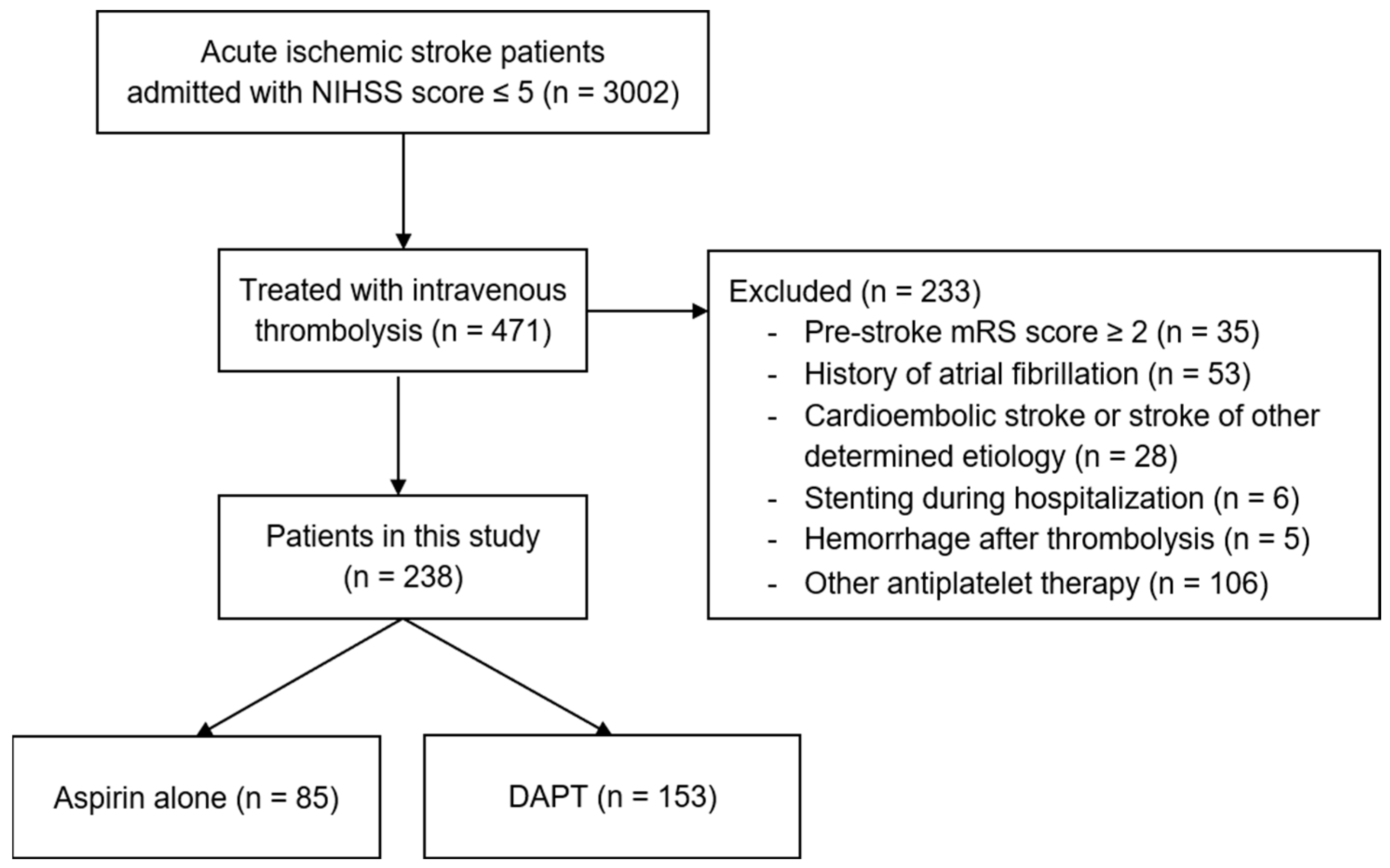
2.1. Study Participants
2.2. Baseline Characteristics
2.3. Outcome Assessments
2.4. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Baseline Characteristics
3.3. Primary Outcome
3.4. Secondary Outcomes
3.5. Subgroup Analyses
3.6. Outcomes with NIHSS Score ≤ 3 versus NIHSS Scores 4 to 5
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tu, W.-J.; Hua, Y.; Yan, F.; Bian, H.; Yang, Y.; Lou, M.; Kang, D.; He, L.; Chu, L.; Zeng, J.; et al. Prevalence of stroke in China, 2013–2019: A population-based study. Lancet Reg. Health West. Pac. 2022, 28, 100550. [Google Scholar] [CrossRef]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Saber, H.; Saver, J.L. Distributional Validity and Prognostic Power of the National Institutes of Health Stroke Scale in US Administrative Claims Data. JAMA Neurol. 2020, 77, 606. [Google Scholar] [CrossRef]
- Hobeanu, C.; Lavallée, P.C.; Charles, H.; Labreuche, J.; Albers, G.W.; Caplan, L.R.; Donnan, G.A.; Ferro, J.M.; Hennerici, M.G.; Molina, C.A.; et al. Risk of subsequent disabling or fatal stroke in patients with transient ischaemic attack or minor ischaemic stroke: An international, prospective cohort study. Lancet Neurol. 2022, 21, 889–898. [Google Scholar] [CrossRef]
- Heldner, M.R.; Seners, P.; Li, L. Editorial: Challenges in Acute Minor Ischemic Stroke. Front. Neurol. 2022, 13, 698. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418, Correction in Stroke 2019, 50, e440–e441. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Zhao, X.; Liu, L.; Wang, D.; Wang, C.; Wang, C.; Li, H.; Meng, X.; Cui, L.; et al. Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack. N. Engl. J. Med. 2013, 369, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.C.; Easton, J.D.; Farrant, M.; Barsan, W.; Conwit, R.A.; Elm, J.J.; Kim, A.S.; Lindblad, A.S.; Palesch, Y.Y.; Neurological Emergencies Treatment Trials Network; et al. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. N. Engl. J. Med. 2018, 379, 215–225. [Google Scholar] [CrossRef]
- Wang, Y.; Pan, Y.; Zhao, X.; Li, H.; Wang, D.; Johnston, S.C.; Liu, L.; Meng, X.; Wang, A.; Wang, C.; et al. Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack (CHANCE) Trial. Circulation 2015, 132, 40–46. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, X.; Johnston, S.C.; Xian, Y.; Hu, B.; Wang, C.; Wang, D.; Liu, L.; Li, H.; Fang, J.; et al. Effect of clopidogrel with aspirin on functional outcome in TIA or minor stroke. Neurology 2015, 85, 573–579. [Google Scholar] [CrossRef]
- Cucchiara, B.; Elm, J.; Easton, J.D.; Coutts, S.B.; Willey, J.Z.; Biros, M.H.; Ross, M.A.; Johnston, S.C. Disability After Minor Stroke and Transient Ischemic Attack in the POINT Trial. Stroke 2020, 51, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Lin, F.; Wang, Z.; Shao, X.; Gong, Y.; Zhang, S.; Cui, Y.; Yang, D.; Lei, H.; Cheng, Z.; et al. Dual Antiplatelet Therapy after Intravenous Thrombolysis for Acute Minor Ischemic Stroke. Eur. Neurol. 2019, 82, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Chen, N.; Sun, H.; Jiang, T.; Deng, Q.; Zhou, J.; Zhang, Y. Dual Antiplatelet Therapy in Patients with Minor Stroke Receiving Intravenous Thrombolysis. Front. Neurol. 2022, 13, 819896. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Gu, H.; Zhao, X.-Q.; Yang, X.; Wang, C.; Wang, Y.-L.; Liu, L.-P.; Zhou, Q.; Fisher, M.; Li, Z.; et al. Clinical Characteristics and In-Hospital Outcomes of Varying Definitions of Minor Stroke. Stroke 2021, 52, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Chao, B.-H.; Cao, L.; Tu, W.-J.; Wang, L.-D. Stroke Center Care and Outcome: Results from the CSPPC Stroke Program. Transl. Stroke Res. 2019, 11, 377–386. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., III. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Banks, J.L.; Marotta, C.A. Outcomes Validity and Reliability of the Modified Rankin Scale: Implications for Stroke Clinical Trials. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef]
- Ganesh, A.; Luengo-Fernandez, R.; Wharton, R.M.; Rothwell, P.M. Ordinal vs dichotomous analyses of modified Rankin Scale, 5-year outcome, and cost of stroke. Neurology 2018, 91, e1951–e1960. [Google Scholar] [CrossRef]
- Ballester, B.R.; Maier, M.; Duff, A.; Cameirão, M.; Bermúdez, S.; Duarte, E.; Cuxart, A.; Rodriguez, S.; Mozo, R.M.S.S.; Verschure, P.F.M.J. A critical time window for recovery extends beyond one-year post-stroke. J. Neurophysiol. 2019, 122, 350–357. [Google Scholar] [CrossRef]
- Wang, X.-G.; Zhang, L.-Q.; Liao, X.-L.; Pan, Y.; Shi, Y.-Z.; Wang, C.-J.; Wang, Y.-L.; Liu, L.-P.; Zhao, X.-Q.; Wang, Y.-J.; et al. Unfavorable Outcome of Thrombolysis in Chinese Patients with Cardioembolic Stroke: A Prospective Cohort Study. CNS Neurosci. Ther. 2015, 21, 657–661. [Google Scholar] [CrossRef]
- Lange, M.C.; Ribas, G.; Scavasine, V.; Ducci, R.D.-P.; Mendes, D.C.; Zétola, V.D.H.F.; Cabral, N.; Rundek, T. Stroke recurrence in the different subtypes of ischemic stroke. The importance of the intracranial disease. Arq. Neuro-Psiquiatr. 2018, 76, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Cabral, N.L.; Nagel, V.; Conforto, A.B.; Magalhaes, P.S.; Venancio, V.G.; Safanelli, J.; Ibiapina, F.; Mazin, S.; França, P.; Liberato, R.M.; et al. High five-year mortality rates of ischemic stroke subtypes: A prospective cohort study in Brazil. Int. J. Stroke 2018, 14, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.-S.; Lee, S.-H.; Kim, E.G.; Cho, K.-H.; Chang, D.I.; Rha, J.-H.; Bae, H.-J.; Lee, K.B.; Kim, D.E.; Park, J.-M.; et al. Recurrent Ischemic Lesions After Acute Atherothrombotic Stroke. Stroke 2016, 47, 2323–2330. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yi, X.; Zhang, B.; Liao, D.; Lin, J.; Chi, L. Clopidogrel Plus Aspirin Prevents Early Neurologic Deterioration and Improves 6-Month Outcome in Patients with Acute Large Artery Atherosclerosis Stroke. Clin. Appl. Thromb. 2014, 21, 453–461. [Google Scholar] [CrossRef]
- Kwok, C.S.; Shoamanesh, A.; Copley, H.C.; Myint, P.K.; Loke, Y.K.; Benavente, O.R. Efficacy of Antiplatelet Therapy in Secondary Prevention Following Lacunar Stroke. Stroke 2015, 46, 1014–1023. [Google Scholar] [CrossRef]
- Berberich, A.; Schneider, C.; Herweh, C.; Hielscher, T.; Reiff, T.; Bendszus, M.; Gumbinger, C.; Ringleb, P. Risk factors associated with progressive lacunar strokes and benefit from dual antiplatelet therapy. Eur. J. Neurol. 2020, 27, 817–824. [Google Scholar] [CrossRef]
- Dettori, J.R. Loss to follow-up. Evid.-Based Spine-Care J. 2011, 2, 7–10. [Google Scholar] [CrossRef]
- Sullivan, L.M.; Weinberg, J.; Keaney, J.F., Jr. Common Statistical Pitfalls in Basic Science Research. J. Am. Heart Assoc. 2016, 5, e004142. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Aspirin | DAPT | p Value |
|---|---|---|---|
| (n = 85) | (n = 153) | ||
| Age, yr, median (IQR) | 64 (55–73) | 66 (60–74) | 0.139 |
| Male sex, n (%) | 70 (82.4) | 117 (76.5) | 0.289 |
| Medical history, n (%) | |||
| Previous stroke or TIA | 18 (21.2) | 35 (22.9) | 0.763 |
| Previous coronary artery disease | 1 (1.2) | 14 (9.2) | 0.016 |
| Hypertension | 56 (65.9) | 103 (67.3) | 0.821 |
| Diabetes mellitus | 22 (25.9) | 34 (22.2) | 0.524 |
| Hypercholesterolemia | 2 (2.4) | 3 (2.0) | 0.587 |
| Current smoking, n (%) | 37 (43.5) | 67 (43.8) | 0.969 |
| Stroke etiology, n (%) | 0.002 | ||
| LAA | 21 (24.7) | 73 (47.7) | |
| SAO | 59 (69.4) | 76 (49.7) | |
| SUE | 5 (5.9) | 4 (2.6) | |
| OCSP classification, n (%) | 0.721 | ||
| TACI | 0 | 1 (0.7%) | |
| PACI | 58 (68.2) | 110 (71.9) | |
| POCI | 16 (18.8) | 22 (14.4) | |
| LACI | 11 (12.9) | 20 (13.1) | |
| Baseline NIHSS score, median (IQR) | 3 (2–4) | 3 (2–4) | 0.588 |
| DNT, minutes, median (IQR) | 30 (20–40) | 30 (21–40) | 0.917 |
| Medications | |||
| Statins, n (%) | 78 (91.8) | 147 (96.1) | 0.161 |
| Anti-hypertensive agents, n (%) | 57 (67.1) | 106 (69.3) | 0.724 |
| Anti-diabetic drugs, n(%) | 29 (34.1) | 50 (32.7) | 0.821 |
| Outcomes at 1 Year | Aspirin | DAPT | Unadjusted OR (95% CI) | p Value | Adjusted OR (95% CI) * | p Value |
|---|---|---|---|---|---|---|
| Total population | n = 74 | n = 131 | ||||
| mRS score, median (IQR) | 0 (0–1) | 0 (0–1) | 1.49 (0.83–2.69) | 0.185 | 2.19 (1.12–4.28) | 0.022 |
| mRS score of 0, n (%) | 45 (60.8) | 95 (72.5) | 1.71 (0.93–1.70) | 0.085 | 2.44 (1.21–4.95) | 0.013 |
| mRS score of 0–1, n (%) | 62 (83.8) | 110 (84.0) | 1.01 (0.47–2.20) | 0.972 | 1.50 (0.63–3.58) | 0.358 |
| mRS score of 0–2, n (%) | 69 (93.2) | 118 (90.1) | 0.66 (0.23–1.92) | 0.444 | 0.90 (0.28–2.92) | 0.866 |
| Stroke due to LAA | n = 17 | n = 65 | ||||
| mRS score, median (IQR) | 0 (0–2) | 0 (0–1.5) | 1.27 (0.46–3.54) | 0.648 | 1.55 (0.53–4.47) | 0.421 |
| mRS score of 0, n (%) | 9 (52.9) | 40 (61.5) | 1.42 (0.49–4.17) | 0.521 | 1.70 (0.55–5.27) | 0.362 |
| mRS score of 0–1, n (%) | 12 (70.6) | 49 (75.4) | 1.28 (0.39–4.18) | 0.687 | 1.41 (0.41–4.4) | 0.581 |
| mRS score of 0–2, n (%) | 15 (88.2) | 55 (84.6) | 0.73 (0.15–3.71) | 0.708 | 0.93 (0.16–5.24) | 0.931 |
| Stroke due to SAO | n = 53 | n = 63 | ||||
| mRS score, median (IQR) | 0 (0–1) | 0 (0–0) | 2.87 (1.24–6.64) | 0.014 | 4.02 (1.52–10.62) | 0.005 |
| mRS score of 0, n (%) | 32 (60.4) | 52 (82.5) | 3.10 (1.32–7.27) | 0.009 | 4.09 (1.58–10.59) | 0.004 |
| mRS score of 0–1, n (%) | 46 (86.8) | 58 (92.1) | 1.77 (0.53–5.93) | 0.358 | 2.46 (0.62–9.70) | 0.199 |
| mRS score of 0–2, n (%) | 50 (94.3) | 60 (95.2) | 1.20 (0.23–6.21) | 0.828 | 1.43 (0.24–8.48) | 0.693 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, H.-M.; Lian, H.-W.; E, Y.; Duan, R.; Zhou, J.-S.; Chen, X.-L.; Jiang, T. Clopidogrel with Aspirin versus Aspirin Alone following Intravenous Thrombolysis in Minor Stroke: A 1-Year Follow-Up Study. Brain Sci. 2023, 13, 20. https://doi.org/10.3390/brainsci13010020
Cao H-M, Lian H-W, E Y, Duan R, Zhou J-S, Chen X-L, Jiang T. Clopidogrel with Aspirin versus Aspirin Alone following Intravenous Thrombolysis in Minor Stroke: A 1-Year Follow-Up Study. Brain Sciences. 2023; 13(1):20. https://doi.org/10.3390/brainsci13010020
Chicago/Turabian StyleCao, Hai-Ming, Hui-Wen Lian, Yan E, Rui Duan, Jun-Shan Zhou, Xiang-Liang Chen, and Teng Jiang. 2023. "Clopidogrel with Aspirin versus Aspirin Alone following Intravenous Thrombolysis in Minor Stroke: A 1-Year Follow-Up Study" Brain Sciences 13, no. 1: 20. https://doi.org/10.3390/brainsci13010020
APA StyleCao, H.-M., Lian, H.-W., E, Y., Duan, R., Zhou, J.-S., Chen, X.-L., & Jiang, T. (2023). Clopidogrel with Aspirin versus Aspirin Alone following Intravenous Thrombolysis in Minor Stroke: A 1-Year Follow-Up Study. Brain Sciences, 13(1), 20. https://doi.org/10.3390/brainsci13010020