
After 55 Years of Neurorehabilitation, What Is the Plan?



{kind=link}
Abstract
:1. Introduction
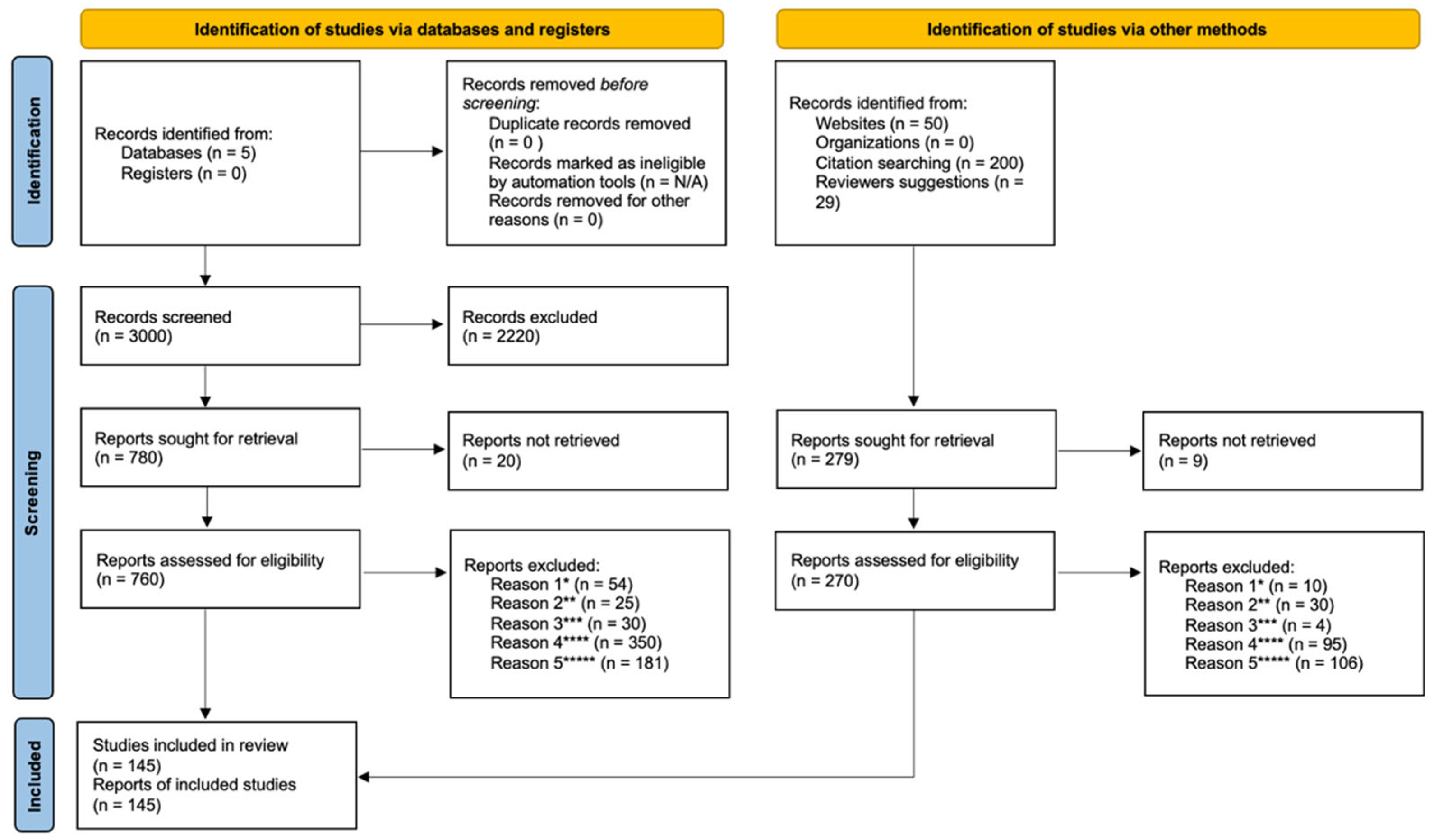
2. Searching Strategy and Selection Criteria
3. Intensity and Effectiveness: A Simple Correlation?
3.1. The Biological Clocks
3.2. The Learning Brain
3.3. The Impact of Fatigue
3.4. The Impact of Psychological Factors
3.5. Reconfiguration Costs and Whole-Brain Homeostasis
4. The Challenge of a New Paradigm
5. The Promised Revolution of New Technologies: A Real Opportunity or a Headlong Rush?
6. Discussion
7. Conclusions
8. Study Limitations and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Neurological Disorders: Public Health Challenges; World Health Organization: Geneva, Switzerland, 2006; p. 218. [Google Scholar]
- Khan, F.; Amatya, B.; Galea, M.P.; Gonzenbach, R.; Kesselring, J. Neurorehabilitation: Applied neuroplasticity. J. Neurol. 2016, 264, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Vos, T.; Nichols, E.; Owolabi, M.O.; Carroll, W.M.; Dichgans, M.; Deuschl, G.; Parmar, P.; Brainin, M.; Murray, C. The global burden of neurological disorders: Translating evidence into policy. Lancet Neurol. 2019, 19, 255–265. [Google Scholar] [CrossRef]
- Harris, S.R.; Winstein, C. The Past, Present, and Future of Neurorehabilitation: From NUSTEP Through IV STEP and Beyond. J. Neurol. Phys. Ther. 2017, 41, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Frasca, D.; Tomaszczyk, J.; McFadyen, B.J.; Green, R.E. Traumatic brain injury and post-acute decline: What role does environmental enrichment play? A scoping review. Front. Hum. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, D.; Janzen, S.; McIntyre, A.; Vermeer, J.; Britt, E.; Teasell, R. Comprehensive Outpatient Rehabilitation Program: Hospital-Based Stroke Outpatient Rehabilitation. J. Stroke Cerebrovasc. Dis. 2016, 25, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Wissel, J.; Olver, J.; Sunnerhagen, K.S. Navigating the Poststroke Continuum of Care. J. Stroke Cerebrovasc. Dis. 2013, 22, 1–8. [Google Scholar] [CrossRef]
- Kreutzer, J.S.; Agyemang, A.A.; Weedon, D.; Zasler, N.; Oliver, M.; Sorensen, A.A.; van Wijngaarden, S.; Leahy, E. The top 100 cited neurorehabilitation papers. NeuroRehabilitation 2017, 40, 163–174. [Google Scholar] [CrossRef] [Green Version]
- Slade, A.; Tennant, A.; Chamberlain, M.A. A randomised controlled trial to determine the effect of intensity of therapy upon length of stay in a neurological rehabilitation setting. J. Rehabil. Med. 2002, 34, 260–266. [Google Scholar] [CrossRef] [Green Version]
- Pollock, A.; Baer, G.; Campbell, P.; Choo, P.L.; Forster, A.; Morris, J.; Pomeroy, V.M.; Langhorne, P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst. Rev. 2014, 2014, CD001920. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.; Amatya, B.; Ng, L.; Demetrios, M.; Zhang, N.Y.; Turner-Stokes, L. Multidisciplinary rehabilitation for follow-up of women treated for breast cancer. Cochrane Database Syst. Rev. 2012, 2021, CD009553. [Google Scholar] [CrossRef]
- Iosa, M.; Morone, G.; Cherubini, A.; Paolucci, S. The Three Laws of Neurorobotics: A Review on What Neurorehabilitation Robots Should Do for Patients and Clinicians. J. Med. Biol. Eng. 2016, 36, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viruega, H.; Gaillard, I.; Briatte, L.; Gaviria, M. Inter-Day Reliability and Changes of Surface Electromyography on Two Postural Muscles Throughout 12 Weeks of Hippotherapy on Patients with Cerebral Palsy: A Pilot Study. Brain Sci. 2020, 10, 281. [Google Scholar] [CrossRef]
- Königs, M.; Beurskens, E.A.; Snoep, L.; Scherder, E.J.; Oosterlaan, J. Effects of Timing and Intensity of Neurorehabilitation on Functional Outcome After Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 1149–1159.e1. [Google Scholar] [CrossRef] [PubMed]
- Cheeran, B.; Talelli, P.; Mori, F.; Koch, G.; Suppa, A.; Edwards, M.; Houlden, H.; Bhatia, K.; Greenwood, R.; Rothwell, J.C. A common polymorphism in the brain-derived neurotrophic factor gene (BDNF) modulates human cortical plasticity and the response to rTMS. J. Physiol. 2008, 586, 5717–5725. [Google Scholar] [CrossRef] [PubMed]
- Müller-Dahlhaus, J.F.M.; Orekhov, Y.; Liu, Y.; Ziemann, U. Interindividual variability and age-dependency of motor cortical plasticity induced by paired associative stimulation. Exp. Brain Res. 2008, 187, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Iyer, M.B.; Schleper, N.; Wassermann, E.M. Priming Stimulation Enhances the Depressant Effect of Low-Frequency Repetitive Transcranial Magnetic Stimulation. J. Neurosci. 2003, 23, 10867–10872. [Google Scholar] [CrossRef]
- Stefan, K.; Wycislo, M.; Classen, J. Modulation of Associative Human Motor Cortical Plasticity by Attention. J. Neurophysiol. 2004, 92, 66–72. [Google Scholar] [CrossRef]
- Sale, M.; Ridding, M.; Nordstrom, M. Circadian Modulation off Neuroplasticity in Humans and Potential Therapeutic Implications. Rev. Neurosci. 2010, 21, 55–66. [Google Scholar] [CrossRef] [Green Version]
- Sale, M.; Ridding, M.C.; Nordstrom, M.A. Cortisol Inhibits Neuroplasticity Induction in Human Motor Cortex. J. Neurosci. 2008, 28, 8285–8293. [Google Scholar] [CrossRef] [Green Version]
- Reddy, S.; Reddy, V.; Sharma, S. Physiology, Circadian Rhythm. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ivanov, P.C.; Hu, K.; Hilton, M.F.; Shea, S.A.; Stanley, H.E. Endogenous circadian rhythm in human motor activity uncoupled from circadian influences on cardiac dynamics. Proc. Natl. Acad. Sci. USA 2007, 104, 20702–20707. [Google Scholar] [CrossRef] [Green Version]
- Halpern, A.I.; Jansen, J.A.; Giladi, N.; Mirelman, A.; Hausdorff, J.M. Does Time of Day influence postural control and gait? A review of the literature. Gait Posture 2021, 92, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.C.; Ii, W.H.W.; Bumgarner, J.R.; Meléndez-Fernández, O.H.; Liu, J.A.; Hughes, H.L.; Kaper, A.L.; Nelson, R.J. Circadian Variation in Efficacy of Medications. Clin. Pharmacol. Ther. 2020, 109, 1457–1488. [Google Scholar] [CrossRef]
- Albrecht, U. Timing to Perfection: The Biology of Central and Peripheral Circadian Clocks. Neuron 2012, 74, 246–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Veen, D.R.; Riede, S.J.; Heideman, P.D.; Hau, M.; Van Der Vinne, V.; Hut, R.A. Flexible clock systems: Adjusting the temporal programme. Philos. Trans. R. Soc. B Biol. Sci. 2017, 372, 20160254. [Google Scholar] [CrossRef] [PubMed]
- Porcu, A.; Riddle, M.; Dulcis, D.; Welsh, D.K. Photoperiod-Induced Neuroplasticity in the Circadian System. Neural Plast. 2018, 2018, 5147585. [Google Scholar] [CrossRef] [Green Version]
- Dibner, C.; Schibler, U.; Albrecht, U. The Mammalian Circadian Timing System: Organization and Coordination of Central and Peripheral Clocks. Annu. Rev. Physiol. 2010, 72, 517–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krakauer, J.W. Motor learning: Its relevance to stroke recovery and neurorehabilitation. Curr. Opin. Neurol. 2006, 19, 84–90. [Google Scholar] [CrossRef]
- Dayan, E.; Cohen, L.G. Neuroplasticity Subserving Motor Skill Learning. Neuron 2011, 72, 443–454. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.P.; Cohen, L.G.; Westlake, K.P. The Intersection of Offline Learning and Rehabilitation. Front. Hum. Neurosci. 2021, 15. [Google Scholar] [CrossRef]
- Krakauer, J.W.; Mazzoni, P. Human sensorimotor learning: Adaptation, skill, and beyond. Curr. Opin. Neurobiol. 2011, 21, 636–644. [Google Scholar] [CrossRef]
- Taylor, J.A.; Ivry, R.B. Cerebellar and Prefrontal Cortex Contributions to Adaptation, Strategies, and Reinforcement Learning. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2014; Volume 210, pp. 217–253. [Google Scholar] [CrossRef] [Green Version]
- Roemmich, R.T.; Bastian, A.J. Closing the Loop: From Motor Neuroscience to Neurorehabilitation. Annu. Rev. Neurosci. 2018, 41, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.J.; Grimwood, P.D.; Morris, R.G.M. Synaptic Plasticity and Memory: An Evaluation of the Hypothesis. Annu. Rev. Neurosci. 2000, 23, 649–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudai, Y.; Karni, A.; Born, J. The Consolidation and Transformation of Memory. Neuron 2015, 88, 20–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, M.B.; Soares, A.B. Reconsolidation of human motor memory: From boundary conditions to behavioral interventions—How far are we from clinical applications? Behav. Brain Res. 2018, 353, 83–90. [Google Scholar] [CrossRef]
- Lang, C.E.; Lohse, K.R.; Birkenmeier, R.L. Dose and timing in neurorehabilitation. Curr. Opin. Neurol. 2015, 28, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Pt, C.E.L.; Strube, M.J.; Bland, M.D.; Waddell, K.; Cherry-Allen, K.M.; Nudo, R.J.; Dromerick, A.W.; Birkenmeier, R.L. Dose response of task-specific upper limb training in people at least 6 months poststroke: A phase II, single-blind, randomized, controlled trial. Ann. Neurol. 2016, 80, 342–354. [Google Scholar] [CrossRef] [Green Version]
- Chaudhuri, A.; Behan, P.O. Fatigue in neurological disorders. Lancet 2004, 363, 978–988. [Google Scholar] [CrossRef]
- Gandevia, S.C. Spinal and Supraspinal Factors in Human Muscle Fatigue. Physiol. Rev. 2001, 81, 1725–1789. [Google Scholar] [CrossRef]
- Löscher, W.N.; Nordlund, M.M. Central fatigue and motor cortical excitability during repeated shortening and lengthening actions. Muscle Nerve 2002, 25, 864–872. [Google Scholar] [CrossRef]
- Tanaka, M.; Watanabe, Y. Supraspinal regulation of physical fatigue. Neurosci. Biobehav. Rev. 2012, 36, 727–734. [Google Scholar] [CrossRef]
- Acciarresi, M.; Bogousslavsky, J.; Paciaroni, M. Post-Stroke Fatigue: Epidemiology, Clinical Characteristics and Treatment. Eur. Neurol. 2014, 72, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Juárez-Belaúnde, A.; Orcajo, E.; Lejarreta, S.; Davila-Pérez, P.; León, N.; Oliviero, A. La fatiga en el daño cerebral sobrevenido. Neurología, 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Rottoli, M.; La Gioia, S.; Frigeni, B.; Barcella, V. Pathophysiology, assessment and management of multiple sclerosis fatigue: An update. Expert Rev. Neurother. 2016, 17, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, S.; Iosa, M.; Coiro, P.; Venturiero, V.; Savo, A.; De Angelis, D.; Morone, G. Post-Stroke Depression Increases Disability More Than 15% in Ischemic Stroke Survivors: A Case-Control Study. Front. Neurol. 2019, 10, 926. [Google Scholar] [CrossRef] [Green Version]
- Ghorbanpour, Z.; Taghizadeh, G.; Hosseini, S.A.; Pishyareh, E.; Ghomsheh, F.T.; Bakhshi, E.; Mehdizadeh, H. Overload of anxiety on postural control impairments in chronic stroke survivors: The role of external focus and cognitive task on the automaticity of postural control. PLoS ONE 2021, 16, e0252131. [Google Scholar] [CrossRef]
- Prediger, R.D.; Matheus, F.C.; Schwarzbold, M.L.; Lima, M.M.S.; Vital, M.A. Anxiety in Parkinson’s disease: A critical review of experimental and clinical studies. Neuropharmacology 2012, 62, 115–124. [Google Scholar] [CrossRef]
- Martens, K.E.; Ellard, C.G.; Almeida, Q.J. Does Anxiety Cause Freezing of Gait in Parkinson’s Disease? PLoS ONE 2014, 9, e106561. [Google Scholar] [CrossRef] [Green Version]
- Martens, K.A.E.; Ellard, C.G.; Almeida, Q.J. Anxiety-provoked gait changes are selectively dopa-responsive in Parkinson’s disease. Eur. J. Neurosci. 2015, 42, 2028–2035. [Google Scholar] [CrossRef]
- Haagsma, J.A.; Scholten, A.C.; Andriessen, T.M.; Vos, P.E.; Van Beeck, E.F.; Polinder, S. Impact of Depression and Post-Traumatic Stress Disorder on Functional Outcome and Health-Related Quality of Life of Patients with Mild Traumatic Brain Injury. J. Neurotrauma 2015, 32, 853–862. [Google Scholar] [CrossRef]
- Martens, K.; Hall, J.; Gilat, M.; Georgiades, M.; Walton, C.; Lewis, S. Anxiety is associated with freezing of gait and attentional set-shifting in Parkinson’s disease: A new perspective for early intervention. Gait Posture 2016, 49, 431–436. [Google Scholar] [CrossRef]
- Văcăraș, V.; Văcăraș, V.; Nistor, C.; Văcăraș, D.; Opre, A.N.; Blaga, P.; Mureșanu, D.F. The Influence of Depression and Anxiety on Neurological Disability in Multiple Sclerosis Patients. Behav. Neurol. 2020, 2020, e6738645. [Google Scholar] [CrossRef]
- Hackett, M.L.; Pickles, K. Part I: Frequency of Depression after Stroke: An Updated Systematic Review and Meta-Analysis of Observational Studies. Int. J. Stroke 2014, 9, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Bullmore, E.; Sporns, O. The economy of brain network organization. Nat. Rev. Neurosci. 2012, 13, 336–349. [Google Scholar] [CrossRef] [PubMed]
- Achard, S.; Bullmore, E. Efficiency and Cost of Economical Brain Functional Networks. PLoS Comput. Biol. 2007, 3, e17. [Google Scholar] [CrossRef]
- Attwell, D.; Laughlin, S.B. An Energy Budget for Signaling in the Grey Matter of the Brain. J. Cereb. Blood Flow Metab. 2001, 21, 1133–1145. [Google Scholar] [CrossRef]
- Laughlin, S.B.; Sejnowski, T.J. Communication in Neuronal Networks. Science 2003, 301, 1870–1874. [Google Scholar] [CrossRef] [Green Version]
- Karbowski, J. Global and regional brain metabolic scaling and its functional consequences. BMC Biol. 2007, 5, 18. [Google Scholar] [CrossRef] [Green Version]
- Kitzbichler, M.G.; Henson, R.N.A.; Smith, M.; Nathan, P.J.; Bullmore, E. Cognitive Effort Drives Workspace Configuration of Human Brain Functional Networks. J. Neurosci. 2011, 31, 8259–8270. [Google Scholar] [CrossRef] [Green Version]
- Viscomi, M.T.; Molinari, M. Remote Neurodegeneration: Multiple Actors for One Play. Mol. Neurobiol. 2014, 50, 368–389. [Google Scholar] [CrossRef]
- Sylvain, N.J.; Salman, M.M.; Pushie, M.J.; Hou, H.; Meher, V.; Herlo, R.; Peeling, L.; Kelly, M.E. The effects of trifluoperazine on brain edema, aquaporin-4 expression and metabolic markers during the acute phase of stroke using photothrombotic mouse model. Biochim. Biophys. Acta (BBA) Biomembr. 2021, 1863, 183573. [Google Scholar] [CrossRef]
- Tovar-Y-Romo, L.B.; Penagos-Puig, A.; Ramírez-Jarquín, J.O. Endogenous recovery after brain damage: Molecular mechanisms that balance neuronal life/death fate. J. Neurochem. 2015, 136, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Ramón y Cajal, S. Histology of the Nervous System of Man and Vertebrates; History of Neuroscience; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Holliday, M.A. Metabolic rate and organ size during growth from infancy to maturity and during late gastation and early infancy. Pediatrics 1971, 47 (Suppl. 2), 169+. [Google Scholar]
- Flachenecker, P.; Kobelt, G.; Berg, J.; Capsa, D.; Gannedahl, M.; Platform, T.E.M.S. New insights into the burden and costs of multiple sclerosis in Europe: Results for Germany. Mult. Scler. J. 2017, 23, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Rajsic, S.; Gothe, H.; Borba, H.H.; Sroczynski, G.; Vujicic, J.; Toell, T.; Siebert, U. Economic burden of stroke: A systematic review on post-stroke care. Eur. J. Health Econ. 2019, 20, 107–134. [Google Scholar] [CrossRef] [PubMed]
- Nudo, R.J.; Wise, B.M.; SiFuentes, F.; Milliken, G.W. Neural Substrates for the Effects of Rehabilitative Training on Motor Recovery After Ischemic Infarct. Science 1996, 272, 1791–1794. [Google Scholar] [CrossRef] [Green Version]
- Veerbeek, J.; van Wegen, E.; Van Peppen, R.; Van Der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What Is the Evidence for Physical Therapy Poststroke? A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e87987. [Google Scholar] [CrossRef] [Green Version]
- Shklovsky, V.M.; Zotova, L.I.; Malyukova, N.G.; Mamicheva, E.D.; Petrushevsky, A.G.; Mayorova, L.; Syrnikova, B.A. A fight for life and dignity: A case of massive traumatic brain injury and the paths for treatment and neurorehabilitation. PsyCh J. 2016, 5, 48–56. [Google Scholar] [CrossRef]
- Sarajuuri, J.; Vink, M.; Tokola, K. Relationship between late objective and subjective outcomes of holistic neurorehabilitation in patients with traumatic brain injury. Brain Inj. 2018, 32, 1749–1757. [Google Scholar] [CrossRef]
- Viruega, H.; Gaviria, M. Functional Weight of Somatic and Cognitive Networks and Asymmetry of Compensatory Mechanisms: Collaboration or Divergency among Hemispheres after Cerebrovascular Accident? Life 2021, 11, 495. [Google Scholar] [CrossRef]
- Engel, G.L. The Need for a New Medical Model: A Challenge for Biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; World Bank. World Report on Disability 2011; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Bowen, A.; Knapp, P.; Gillespie, D.; Nicolson, D.J.; Vail, A. Non-pharmacological interventions for perceptual disorders following stroke and other adult-acquired, non-progressive brain injury. Cochrane Database Syst. Rev. 2011, 2011, CD007039. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.S.Y.; Pollock, A.; Campbell, T.; Durward, B.R.; Hagen, S. Cognitive rehabilitation for executive dysfunction in adults with stroke or other adult non-progressive acquired brain damage. Cochrane Database Syst. Rev. 2013, 2013, CD008391. [Google Scholar] [CrossRef] [PubMed]
- Levack, W.M.; Weatherall, M.; Hay-Smith, E.J.C.; Dean, S.G.; McPherson, K.; Siegert, R.J. Goal setting and strategies to enhance goal pursuit for adults with acquired disability participating in rehabilitation. Cochrane Database Syst. Rev. 2015, 2015, CD009727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perucca, P.; Gilliam, F.G. Adverse effects of antiepileptic drugs. Lancet Neurol. 2012, 11, 792–802. [Google Scholar] [CrossRef]
- Farach, F.J.; Pruitt, L.D.; Jun, J.J.; Jerud, A.B.; Zoellner, L.A.; Roy-Byrne, P.P. Pharmacological treatment of anxiety disorders: Current treatments and future directions. J. Anxiety Disord. 2012, 26, 833–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, E.Y.; Ghosh, N.; Yanni, D.; Lee, S.; Alexandru, D.; Mozaffar, T. A Review of Spasticity Treatments: Pharmacological and Interventional Approaches. Crit. Rev. Phys. Rehabil. Med. 2013, 25, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Abad, V.C.; Guilleminault, C. Pharmacological Treatment of Sleep Disorders and Its Relationship with Neuroplasticity. In Sleep, Neuronal Plasticity and Brain Function; Meerlo, P., Benca, R.M., Abel, T., Eds.; Current Topics in Behavioral Neurosciences; Springer: Berlin/Heidelberg, Germany, 2015; Volume 25, pp. 503–553. [Google Scholar] [CrossRef]
- Binder, A.; Baron, R. The Pharmacological Therapy of Chronic Neuropathic Pain. Dtsch. Ärztebl. Int. 2016, 113, 616–625. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, C.; Kouzouna, A.; Simcox, C.; Pandyan, A.D. Pharmacological interventions other than botulinum toxin for spasticity after stroke. Cochrane Database Syst. Rev. 2016, 10, CD010362. [Google Scholar] [CrossRef]
- Sabella, D. Antidepressant Medications. AJN Am. J. Nurs. 2018, 118, 52–59. [Google Scholar] [CrossRef]
- Quentin, R.; Awosika, O.; Cohen, L.G. Plasticity and Recovery of Function. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; Volume 163, pp. 473–483. [Google Scholar] [CrossRef]
- Ezendam, D.; Bongers, R.M.; Jannink, M.J.A. Systematic review of the effectiveness of mirror therapy in upper extremity function. Disabil. Rehabil. 2009, 31, 2135–2149. [Google Scholar] [CrossRef]
- Thieme, H.; Morkisch, N.; Mehrholz, J.; Pohl, M.; Behrens, J.; Borgetto, B.; Dohle, C. Mirror therapy for improving motor function after stroke. Cochrane Database Syst. Rev. 2018, 2018, CD008449. [Google Scholar] [CrossRef] [PubMed]
- Fritz, S.L.; Butts, R.J.; Wolf, S.L. Constraint-induced movement therapy: From history to plasticity. Expert Rev. Neurother. 2012, 12, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, D.; Sirtori, V.; Castellini, G.; Moja, L.; Gatti, R. Constraint-induced movement therapy for upper extremities in people with stroke. Cochrane Database Syst. Rev. 2015, 2017, CD004433. [Google Scholar] [CrossRef] [Green Version]
- Knutson, J.S.; Fu, M.J.; Sheffler, L.R.; Chae, J. Neuromuscular Electrical Stimulation for Motor Restoration in Hemiplegia. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 729–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, S.-C.; Khan, A.; Song, R.; Tong, R.K.-Y. Rewiring the Lesioned Brain: Electrical Stimulation for Post-Stroke Motor Restoration. J. Stroke 2020, 22, 47–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquez-Chin, C.; Popovic, M.R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: A review. Biomed. Eng. Online 2020, 19, 34. [Google Scholar] [CrossRef]
- Ibitoye, M.O.; Hamzaid, N.A.; Hasnan, N.; Abdul Wahab, A.K.; Davis, G.M. Strategies for Rapid Muscle Fatigue Reduction during FES Exercise in Individuals with Spinal Cord Injury: A Systematic Review. PLoS ONE 2016, 11, e0149024. [Google Scholar] [CrossRef] [Green Version]
- Ye, G.; Theventhiran, P.; Masani, K. Effect of Spatially Distributed Sequential Stimulation on Fatigue in Functional Electrical Stimulation Rowing. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 999–1008. [Google Scholar] [CrossRef]
- Koutsou, A.D.; Moreno, J.C.; del Ama, A.J.; Rocon, E.; Pons, J.L. Advances in selective activation of muscles for non-invasive motor neuroprostheses. J. Neuroeng. Rehabil. 2016, 13, 56. [Google Scholar] [CrossRef] [Green Version]
- Liew, S.-L.; Santarnecchi, E.; Buch, E.R.; Cohen, L.G. Non-invasive brain stimulation in neurorehabilitation: Local and distant effects for motor recovery. Front. Hum. Neurosci. 2014, 8, 378. [Google Scholar] [CrossRef] [Green Version]
- Siebner, H.R.; Hartwigsen, G.; Kassuba, T.; Rothwell, J.C. How does transcranial magnetic stimulation modify neuronal activity in the brain? Implications for studies of cognition. Cortex 2009, 45, 1035–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandrini, M.; Cohen, L.G. Noninvasive Brain Stimulation in Neurorehabilitation. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2013; Volume 116, pp. 499–524. [Google Scholar] [CrossRef] [Green Version]
- Julkunen, P.; Kimiskidis, V.K.; Belardinelli, P. Bridging the gap: TMS-EEG from lab to clinic. J. Neurosci. Methods 2022, 369, 109482. [Google Scholar] [CrossRef] [PubMed]
- Adeyemo, B.O.; Simis, M.; Macea, D.D.; Fregni, F. Systematic Review of Parameters of Stimulation, Clinical Trial Design Characteristics, and Motor Outcomes in Non-Invasive Brain Stimulation in Stroke. Front. Psychiatry 2012, 3, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, W.-Y.; Cheng, C.-H.; Liao, K.-K.; Lee, I.-H.; Lin, Y.-Y. Effects of Repetitive Transcranial Magnetic Stimulation on Motor Functions in Patients With Stroke. Stroke 2012, 43, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Hao, Z.; Wang, D.; Zeng, Y.; Liu, M. Repetitive transcranial magnetic stimulation for improving function after stroke. Cochrane Database Syst. Rev. 2013, 2013, CD008862. [Google Scholar] [CrossRef] [Green Version]
- Di Pino, G.; Pellegrino, G.; Assenza, G.; Capone, F.; Ferreri, F.; Formica, D.; Ranieri, F.; Tombini, M.; Ziemann, U.; Rothwell, J.; et al. Modulation of brain plasticity in stroke: A novel model for neurorehabilitation. Nat. Rev. Neurol. 2014, 10, 597–608. [Google Scholar] [CrossRef]
- Elsner, B.; Kugler, J.; Pohl, M.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for improving activities of daily living, and physical and cognitive functioning, in people after stroke. Cochrane Database Syst. Rev. 2020, 2020, CD009645. [Google Scholar] [CrossRef]
- Morone, G.; Ghooshchy, S.G.; Palomba, A.; Baricich, A.; Santamato, A.; Ciritella, C.; Ciancarelli, I.; Molteni, F.; Gimigliano, F.; Iolascon, G.; et al. Differentiation among bio- and augmented- feedback in technologically assisted rehabilitation. Expert Rev. Med. Devices 2021, 18, 513–522. [Google Scholar] [CrossRef]
- Woodford, H.J.; Price, C.I. EMG biofeedback for the recovery of motor function after stroke. Cochrane Database Syst. Rev. 2007, 2010, CD004585. [Google Scholar] [CrossRef]
- Bowman, T.; Gervasoni, E.; Arienti, C.; Lazzarini, S.; Negrini, S.; Crea, S.; Cattaneo, D.; Carrozza, M. Wearable Devices for Biofeedback Rehabilitation: A Systematic Review and Meta-Analysis to Design Application Rules and Estimate the Effectiveness on Balance and Gait Outcomes in Neurological Diseases. Sensors 2021, 21, 3444. [Google Scholar] [CrossRef]
- Spencer, J.; Wolf, S.L.; Kesar, T.M. Biofeedback for Post-stroke Gait Retraining: A Review of Current Evidence and Future Research Directions in the Context of Emerging Technologies. Front. Neurol. 2021, 12, 637199. [Google Scholar] [CrossRef] [PubMed]
- Renton, T.; Tibbles, A.; Topolovec-Vranic, J. Neurofeedback as a form of cognitive rehabilitation therapy following stroke: A systematic review. PLoS ONE 2017, 12, e0177290. [Google Scholar] [CrossRef] [PubMed]
- Lebedev, M.; Nicolelis, M.A.L. Brain-Machine Interfaces: From Basic Science to Neuroprostheses and Neurorehabilitation. Physiol. Rev. 2017, 97, 767–837. [Google Scholar] [CrossRef] [PubMed]
- Payedimarri, A.B.; Ratti, M.; Rescinito, R.; Vanhaecht, K.; Panella, M. Effectiveness of Platform-Based Robot-Assisted Rehabilitation for Musculoskeletal or Neurologic Injuries: A Systematic Review. Bioengineering 2022, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Morasso, P.; Casadio, M.; Giannoni, P.; Masia, L.; Sanguineti, V.; Squeri, V.; Vergaro, E. Desirable features of a “humanoid” robot-therapist. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 2418–2421. [Google Scholar] [CrossRef]
- Zhang, X.; Yue, Z.; Wang, J. Robotics in Lower-Limb Rehabilitation after Stroke. Behav. Neurol. 2017, 2017, 3731802. [Google Scholar] [CrossRef] [Green Version]
- Gasperina, S.D.; Roveda, L.; Pedrocchi, A.; Braghin, F.; Gandolla, M. Review on Patient-Cooperative Control Strategies for Upper-Limb Rehabilitation Exoskeletons. Front. Robot. AI 2021, 8, 745018. [Google Scholar] [CrossRef]
- Garro, F.; Chiappalone, M.; Buccelli, S.; De Michieli, L.; Semprini, M. Neuromechanical Biomarkers for Robotic Neurorehabilitation. Front. Neurorobot. 2021, 15, 742163. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; van Wegen, E.; Meskers, C.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb After Stroke. Neurorehabilit. Neural Repair 2016, 31, 107–121. [Google Scholar] [CrossRef]
- O’Neil, O.; Fernandez, M.M.; Herzog, J.; Beorchia, M.; Gower, V.; Gramatica, F.; Starrost, K.; Kiwull, L. Virtual Reality for Neurorehabilitation: Insights From 3 European Clinics. PMR 2018, 10, S198–S206. [Google Scholar] [CrossRef]
- Riva, G.; Mancuso, V.; Cavedoni, S.; Stramba-Badiale, C. Virtual reality in neurorehabilitation: A review of its effects on multiple cognitive domains. Expert Rev. Med. Devices 2020, 17, 1035–1061. [Google Scholar] [CrossRef]
- Iosa, M.; Aydin, M.; Candelise, C.; Coda, N.; Morone, G.; Antonucci, G.; Marinozzi, F.; Bini, F.; Paolucci, S.; Tieri, G. The Michelangelo Effect: Art Improves the Performance in a Virtual Reality Task Developed for Upper Limb Neurorehabilitation. Front. Psychol. 2021, 11, 611956. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.; Gamito, P.; Lopes, B.; Silva, A.R.; Galhordas, J.; Pereira, E.; Ramos, E.; Silva, A.P.; Jorge, Á.; Fantasia, A. Computerized cognitive training using virtual reality on everyday life activities for patients recovering from stroke. Disabil. Rehabil. Assist. Technol. 2022, 17, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Osumi, M.; Ichinose, A.; Sumitani, M.; Wake, N.; Sano, Y.; Yozu, A.; Kumagaya, S.; Kuniyoshi, Y.; Morioka, S. Restoring movement representation and alleviating phantom limb pain through short-term neurorehabilitation with a virtual reality system. Eur. J. Pain 2016, 21, 140–147. [Google Scholar] [CrossRef]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 2018, CD008349. [Google Scholar] [CrossRef] [Green Version]
- Dockx, K.; Bekkers, E.M.; Van den Bergh, V.; Ginis, P.; Rochester, L.; Hausdorff, J.M.; Mirelman, A.; Nieuwboer, A. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2016, 12, CD010760. [Google Scholar] [CrossRef]
- Massetti, T.; Trevizan, I.L.; Arab, C.; Favero, F.M.; Ribeiro-Papa, D.C.; Monteiro, C. Virtual reality in multiple sclerosis—A systematic review. Mult. Scler. Relat. Disord. 2016, 8, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Rosly, M.M.; Rosly, H.M.; Oam, G.M.D.; Husain, R.; Hasnan, N. Exergaming for individuals with neurological disability: A systematic review. Disabil. Rehabil. 2016, 39, 727–735. [Google Scholar] [CrossRef]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Singh, M.; Pandey, P.K.; Bhasin, A.; Padma, M.V.; Mohanty, S. Application of Stem Cells in Stroke: A Multifactorial Approach. Front. Neurosci. 2020, 14, 473. [Google Scholar] [CrossRef]
- Wei, L.; Wei, Z.Z.; Jiang, M.Q.; Mohamad, O.; Yu, S.P. Stem cell transplantation therapy for multifaceted therapeutic benefits after stroke. Prog. Neurobiol. 2017, 157, 49–78. [Google Scholar] [CrossRef]
- Yasuhara, T.; Kameda, M.; Sasaki, T.; Tajiri, N.; Date, I. Cell Therapy for Parkinson’s Disease. Cell Transplant. 2017, 26, 1551–1559. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lv, Z.-Y.; Li, Y. Progress in clinical trials of stem cell therapy for cerebral palsy. Neural Regen. Res. 2021, 16, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Gaviria, M.; Celeghin, A.; Michael-Titus, A.T.; Pallier, P.N. Editorial: Brain Plasticity and Contribution of the Emotional Brain to Neural Remodelling After Injury. Front. Neurol. 2020, 11, 606271. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.B.; Willerslev-Olsen, M.; Christiansen, L.; Lundbye-Jensen, J.; Lorentzen, J. Science-Based Neurorehabilitation: Recommendations for Neurorehabilitation From Basic Science. J. Mot. Behav. 2015, 47, 7–17. [Google Scholar] [CrossRef]
- Winstein, C.J.; Kay, D.B. Translating the science into practice. Prog. Brain Res. 2015, 218, 331–360. [Google Scholar] [CrossRef]
- Viruega, H.; Gaillard, I.; Carr, J.; Greenwood, B.; Gaviria, M. Short- and Mid-Term Improvement of Postural Balance after a Neurorehabilitation Program via Hippotherapy in Patients with Sensorimotor Impairment after Cerebral Palsy: A Preliminary Kinetic Approach. Brain Sci. 2019, 9, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viruega, H.; Imbernon, C.; Chausson, N.; Altarcha, T.; Aghasaryan, M.; Soumah, D.; Lescieux, E.; Flamand-Roze, C.; Simon, O.; Bedin, A.; et al. Neurorehabilitation through Hippotherapy on Neurofunctional Sequels of Stroke: Effect on Patients’ Functional Independence, Sensorimotor/Cognitive Capacities and Quality of Life, and the Quality of Life of Their Caregivers—A Study Protocol. Brain Sci. 2022, 12, 619. [Google Scholar] [CrossRef]
- Ramachandran, V.S.; Rogers-Ramachandran, D. Synaesthesia in phantom limbs induced with mirrors. Proc. R. Soc. B Biol. Sci. 1996, 263, 377–386. [Google Scholar] [CrossRef]
- Wolpert, D.M.; Ghahramani, Z.; Jordan, M.I. An Internal Model for Sensorimotor Integration. Science 1995, 269, 1880–1882. [Google Scholar] [CrossRef]
- Hogeveen, J.; Salvi, C.; Grafman, J. ‘Emotional Intelligence’: Lessons from Lesions. Trends Neurosci. 2016, 39, 694–705. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.; Ferriero, D.M.; Frisoni, G.B.; Bettegowda, C.; Gokaslan, Z.L.; Kessler, J.A.; Vezzani, A.; Waxman, S.G.; Jarius, S.; Wildemann, B.; et al. Neurology—The next 10 years. Nat. Rev. Neurol. 2015, 11, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Yasuhara, T.; Kawauchi, S.; Kin, K.; Morimoto, J.; Kameda, M.; Sasaki, T.; Bonsack, B.; Kingsbury, C.; Tajiri, N.; Borlongan, C.V.; et al. Cell therapy for central nervous system disorders: Current obstacles to progress. CNS Neurosci. Ther. 2019, 26, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacks, O. The Man Who Mistook His Wife for a Hat and Other Clinical Tales, 1st ed.; Simon & Schuster: New York, NY, USA, 1998. [Google Scholar]
- Kapur, N. Paradoxes in rehabilitation. Disabil. Rehabil. 2019, 42, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- Mane, R.; Chouhan, T.; Guan, C. BCI for stroke rehabilitation: Motor and beyond. J. Neural Eng. 2020, 17, 041001. [Google Scholar] [CrossRef]
- Bradnam, L.V.; Meiring, R.M.; Boyce, M.; McCambridge, A. Neurorehabilitation in dystonia: A holistic perspective. J. Neural Transm. 2020, 128, 549–558. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viruega, H.; Gaviria, M. After 55 Years of Neurorehabilitation, What Is the Plan? Brain Sci. 2022, 12, 982. https://doi.org/10.3390/brainsci12080982
Viruega H, Gaviria M. After 55 Years of Neurorehabilitation, What Is the Plan? Brain Sciences. 2022; 12(8):982. https://doi.org/10.3390/brainsci12080982
Chicago/Turabian StyleViruega, Hélène, and Manuel Gaviria. 2022. "After 55 Years of Neurorehabilitation, What Is the Plan?" Brain Sciences 12, no. 8: 982. https://doi.org/10.3390/brainsci12080982
APA StyleViruega, H., & Gaviria, M. (2022). After 55 Years of Neurorehabilitation, What Is the Plan? Brain Sciences, 12(8), 982. https://doi.org/10.3390/brainsci12080982