
Neurological Pupil Index for the Early Prediction of Outcome in Severe Acute Brain Injury Patients

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Automated Quantitative Pupillometry
2.3. Patient Management
2.4. Radiological and Outcome Assessment
2.5. Data Collection and Analysis
3. Results
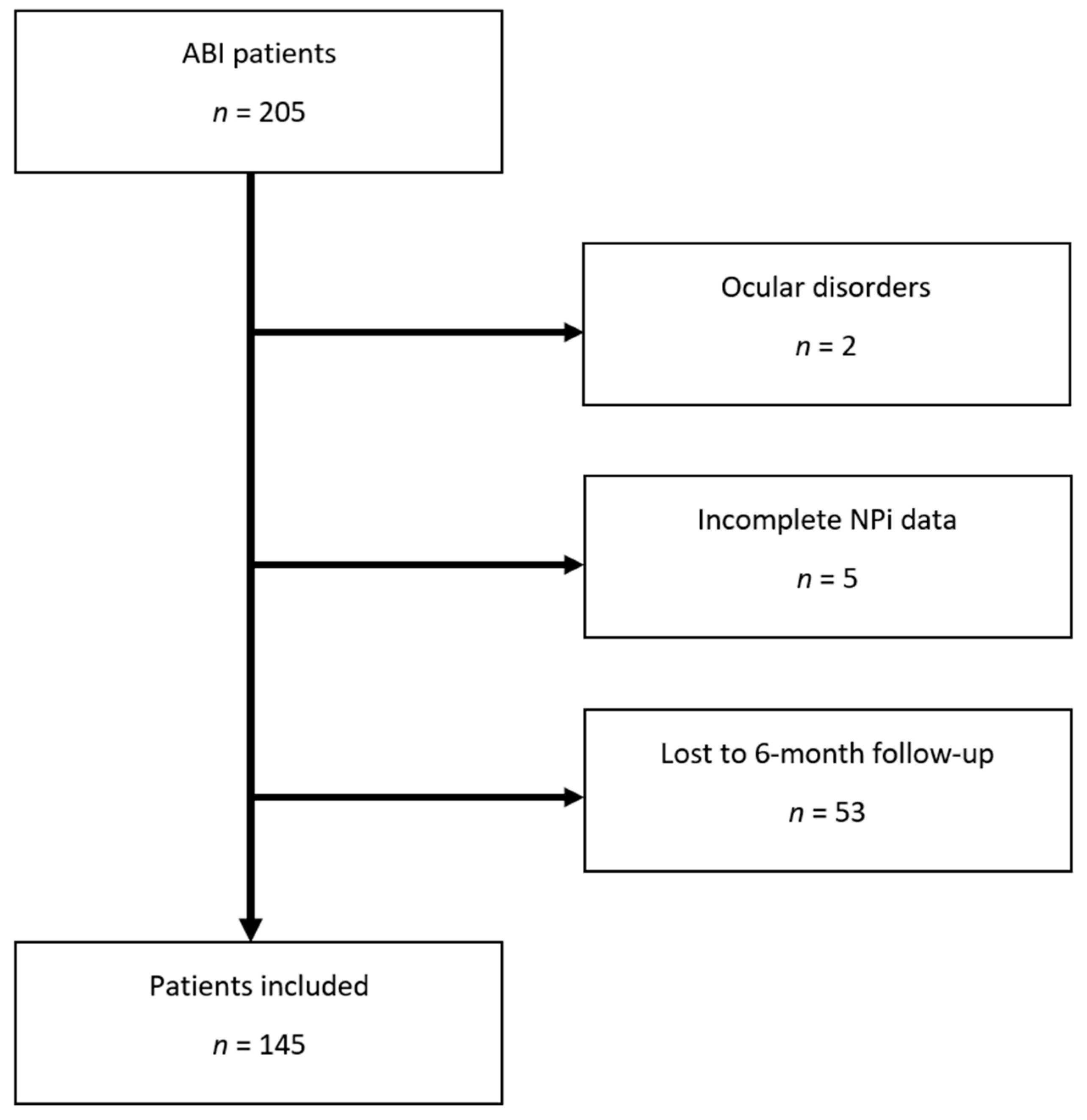
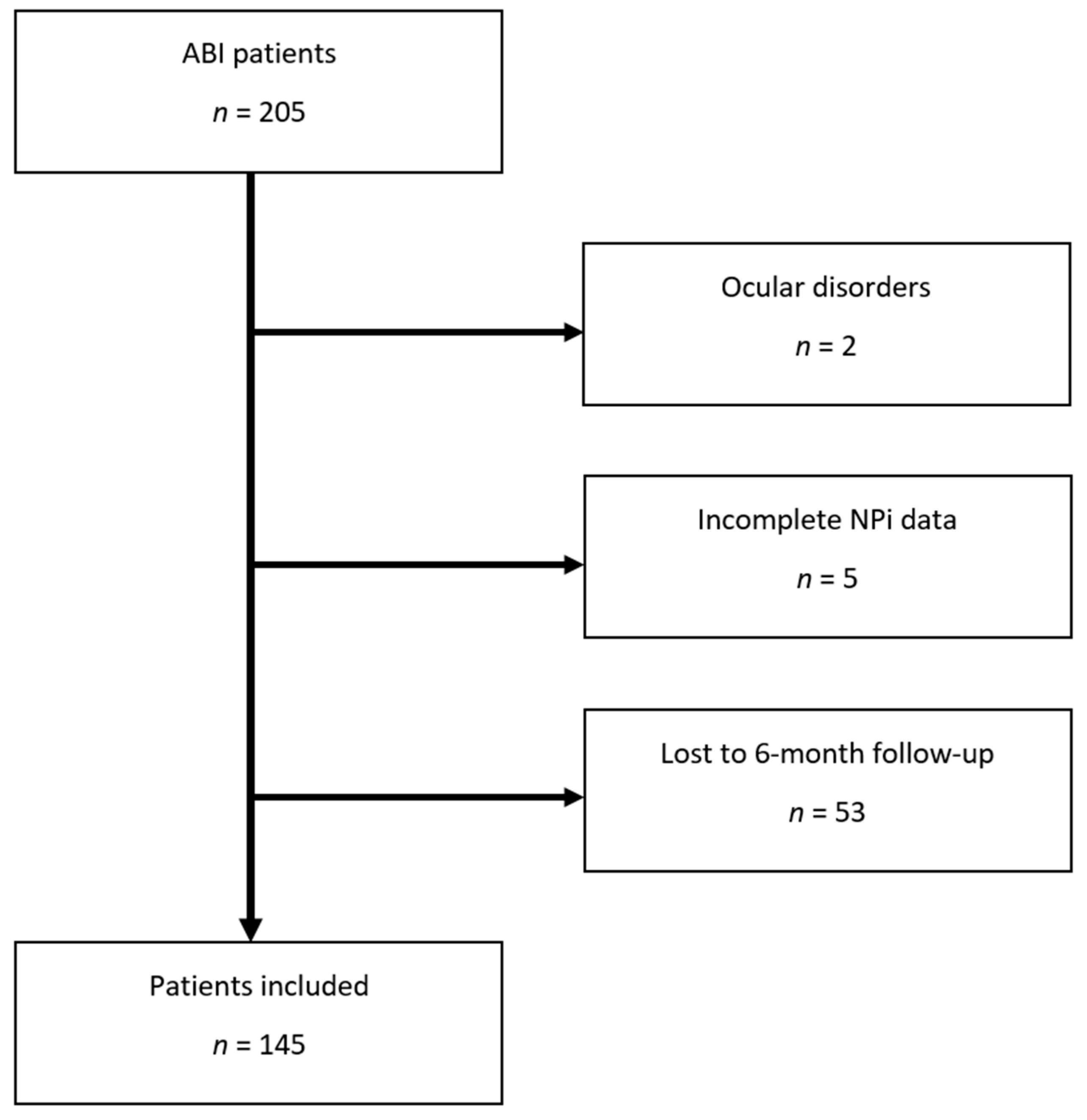
3.1. Patient Characteristics
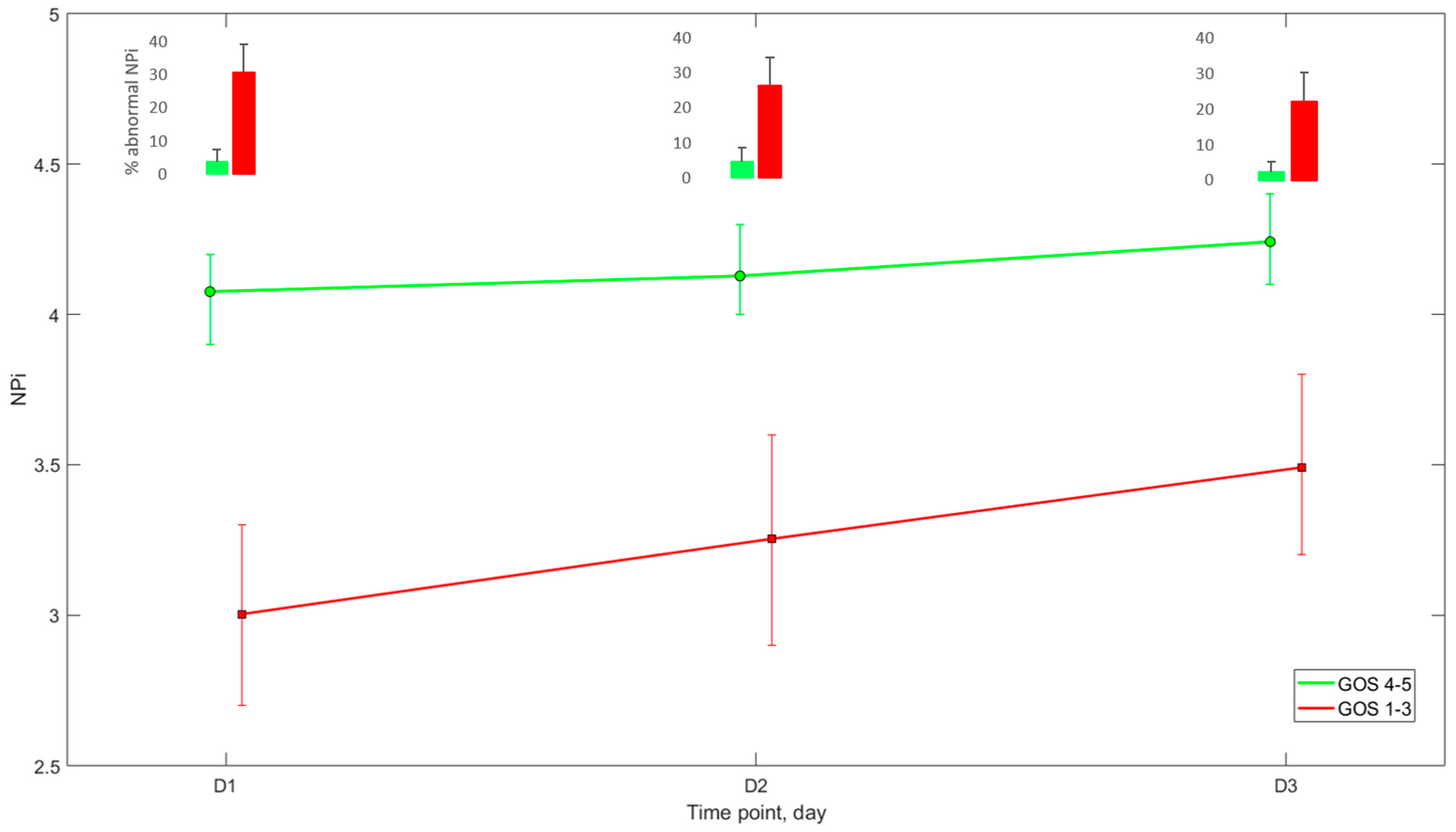
3.2. Outcome Associations
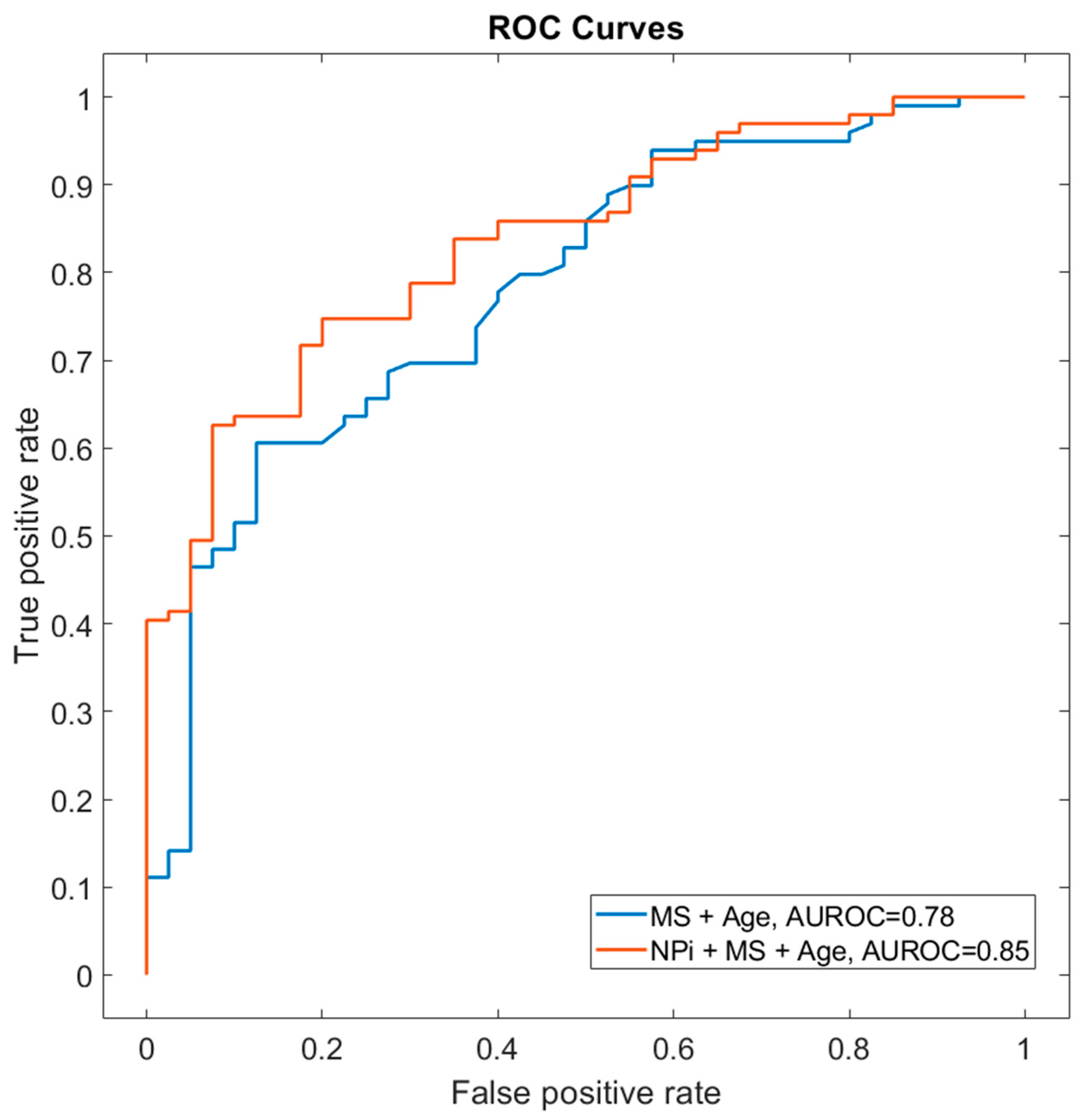
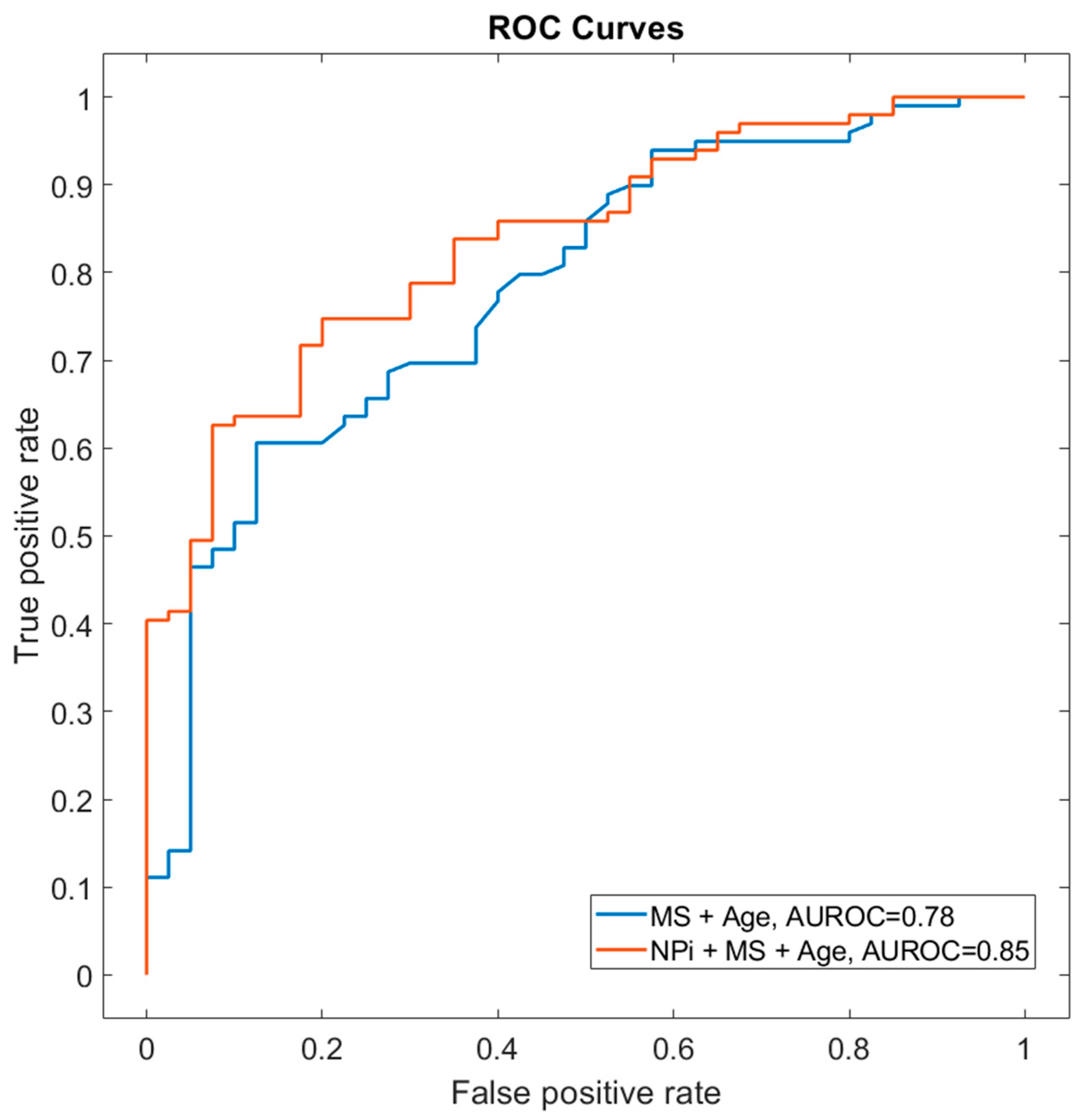
3.3. Prognostic Performance of NPi
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marmarou, A.; Lu, J.; Butcher, I.; McHugh, G.S.; Murray, G.D.; Steyerberg, E.W.; Mushkudiani, N.A.; Choi, S.; Maas, A.I.R. Prognostic Value of The Glasgow Coma Scale And Pupil Reactivity in Traumatic Brain Injury Assessed Pre-Hospital And on Enrollment: An IMPACT Analysis. J. Neurotrauma 2007, 24, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Majdan, M.; Steyerberg, E.W.; Nieboer, D.; Mauritz, W.; Rusnak, M.; Lingsma, H.F. Glasgow Coma Scale Motor Score and Pupillary Reaction To Predict Six-Month Mortality in Patients with Traumatic Brain Injury: Comparison of Field and Admission Assessment. J. Neurotrauma 2015, 32, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, R.D.; Sutter, R. Prognosis in Severe Brain Injury. Crit. Care Med. 2013, 41, 1104–1123. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; King, N.K.K.; Neilson, S.J.; Gandhi, M.P.; Ng, I. External Validation of the CRASH and IMPACT Prognostic Models in Severe Traumatic Brain Injury. J. Neurotrauma 2014, 31, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Cariou, A. Post-Resuscitation Care: ERC–ESICM Guidelines 2015. Intensive Care Med. 2015, 41, 2204–2206. [Google Scholar] [CrossRef] [Green Version]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef]
- Chesnut, R.M.; Gautille, T.; Blunt, B.A.; Klauber, M.R.; Marshall, L.E. The Localizing Value of Asymmetry in Pupillary Size in Severe Head Injury: Relation to Lesion Type and Location. Neurosurgery 1994, 34, 840–845; discussion 845–846. [Google Scholar] [CrossRef]
- Chesnut, R.; Aguilera, S.; Buki, A.; Bulger, E.; Citerio, G.; Cooper, D.J.; Arrastia, R.D.; Diringer, M.; Figaji, A.; Gao, G.; et al. A Management Algorithm for Adult Patients with Both Brain Oxygen and Intracranial Pressure Monitoring: The Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2020, 46, 919–929. [Google Scholar] [CrossRef] [Green Version]
- Ritter, A.M.; Muizelaar, J.P.; Barnes, T.; Choi, S.; Fatouros, P.; Ward, J.; Bullock, M.R. Brain Stem Blood Flow, Pupillary Response, and Outcome in Patients with Severe Head Injuries. Neurosurgery 1999, 44, 941–948. [Google Scholar] [CrossRef]
- Couret, D.; Boumaza, D.; Grisotto, C.; Triglia, T.; Pellegrini, L.; Ocquidant, P.; Bruder, N.J.; Velly, L.J. Reliability of Standard Pupillometry Practice in Neurocritical Care: An Observational, Double-Blinded Study. Crit. Care 2016, 20, 99. [Google Scholar] [CrossRef] [Green Version]
- Olson, D.M.; Stutzman, S.; Saju, C.; Wilson, M.; Zhao, W.; Aiyagari, V. Interrater Reliability of Pupillary Assessments. Neurocritical Care 2016, 24, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Morelli, P.; Oddo, M.; Ben-Hamouda, N. Role of Automated Pupillometry in Critically Ill Patients. Minerva Anestesiol. 2019, 85, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Jahns, F.-P.; Miroz, J.P.; Messerer, M.; Daniel, R.T.; Taccone, F.S.; Eckert, P.; Oddo, M. Quantitative Pupillometry for the Monitoring of Intracranial Hypertension in Patients with Severe Traumatic Brain Injury. Crit. Care 2019, 23, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoun, S.G.; Stutzman, S.E.; Vo, P.-U.N.; Ahmadieh, T.Y.E.; Osman, M.; Neeley, O.; Plitt, A.; Caruso, J.P.; Aiyagari, V.; Atem, F.; et al. Detection of Delayed Cerebral Ischemia Using Objective Pupillometry in Patients with Aneurysmal Subarachnoid Hemorrhage. J. Neurosurg. 2019, 132, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Oddo, M.; Sandroni, C.; Citerio, G.; Miroz, J.-P.; Horn, J.; Rundgren, M.; Cariou, A.; Payen, J.-F.; Storm, C.; Stammet, P.; et al. Quantitative versus Standard Pupillary Light Reflex for Early Prognostication in Comatose Cardiac Arrest Patients: An International Prospective Multicenter Double-Blinded Study. Intensive Care Med. 2018, 44, 2102–2111. [Google Scholar] [CrossRef] [Green Version]
- Riker, R.R.; Sawyer, M.E.; Fischman, V.G.; May, T.; Lord, C.; Eldridge, A.; Seder, D.B. Neurological Pupil Index and Pupillary Light Reflex by Pupillometry Predict Outcome Early After Cardiac Arrest. Neurocritical Care 2019, 32, 152–161. [Google Scholar] [CrossRef]
- Tamura, T.; Namiki, J.; Sugawara, Y.; Sekine, K.; Yo, K.; Kanaya, T.; Yokobori, S.; Roberts, R.; Abe, T.; Yokota, H.; et al. Quantitative Assessment of Pupillary Light Reflex for Early Prediction of Outcomes after Out-of-Hospital Cardiac Arrest: A Multicentre Prospective Observational Study. Resuscitation 2018, 131, 108–113. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-Resuscitation Care. Resuscitation 2021, 161, 220–269. [Google Scholar] [CrossRef]
- Korevaar, D.A.; Cohen, J.F.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Moher, D.; de Vet, H.C.W.; Altman, D.G.; et al. Updating Standards for Reporting Diagnostic Accuracy: The Development of STARD 2015. Res. Integr. Peer Rev. 2016, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Gombart, Z.; Rogers, S.; Gardiner, S.; Cecil, S.; Bullock, R. Pupillary Reactivity as an Early Indicator of Increased Intracranial Pressure: The Introduction of the Neurological Pupil Index. Surg. Neurol. Int. 2011, 2, 82. [Google Scholar] [CrossRef] [Green Version]
- Hemphill, J.C.; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bederson, J.B.; Connolly, E.S., Jr.; Batjer, H.H.; Dacey, R.G.; Dion, J.E.; Diringer, M.N.; Duldner, J.E., Jr.; Harbaugh, R.E.; Patel, A.B.; Rosenwasser, R.H. Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage: A statement for healthcare professionals from a special writing group of the Stroke Council. Stroke 2009, 40, 994–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, E.S., Jr.; Rabinstein, A.A.; Carhuapoma, J.R.; Derdeyn, C.P.; Dion, J.; Higashida, R.T.; Hoh, B.L.; Kirkness, C.J.; Naidech, A.M.; Ogilvy, C.S.; et al. Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012, 43, 1711–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puffer, R.C.; Yue, J.K.; Mesley, M.; Billigen, J.B.; Sharpless, J.; Fetzick, A.L.; Puccio, A.; Diaz-Arrastia, R.; Okonkwo, D.O. Long-Term Outcome in Traumatic Brain Injury Patients with Midline Shift: A Secondary Analysis of the Phase 3 COBRIT Clinical Trial. J. Neurosurg. 2018, 131, 596–603. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Gao, G.; Wu, X.; Feng, J.; Hui, J.; Mao, Q.; Lecky, F.; Lingsma, H.; Maas, A.I.R.; Jiang, J.; China CENTER-TBI Registry Participants. Clinical Characteristics and Outcomes in Patients with Traumatic Brain Injury in China: A Prospective, Multicentre, Longitudinal, Observational Study. Lancet Neurol. 2020, 19, 670–677. [Google Scholar] [CrossRef]
- Oddo, M.; Taccone, F.; Galimberti, S.; Rebora, P.; Citerio, G. Outcome Prognostication of Acute Brain Injury Using the Neurological Pupil Index (ORANGE) Study: Protocol for a Prospective, Observational, Multicentre, International Cohort Study. BMJ Open 2021, 11, e046948. [Google Scholar] [CrossRef]
- Mohammadifard, M.; Ghaemi, K.; Hanif, H.; Sharifzadeh, G.; Haghparast, M. Marshall and Rotterdam Computed Tomography Scores in Predicting Early Deaths after Brain Trauma. Eur. J. Transl. Myol. 2018, 28, 7542. [Google Scholar] [CrossRef]
- Lindvall, P.; Runnerstam, M.; Birgander, R.; Koskinen, L.-O.D. The Fisher Grading Correlated to Outcome in Patients with Subarachnoid Haemorrhage. Br. J. Neurosurg. 2009, 23, 188–192. [Google Scholar] [CrossRef]
- Larson, M.D.; Behrends, M. Portable Infrared Pupillometry: A Review. Anesth. Analg. 2015, 120, 1242–1253. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Favourable Outcome (GOS 4–5) N = 42 | Unfavourable Outcome (GOS 1–3) N = 103 * | p Value |
|---|---|---|---|
| Age, years | 46 ± 18 | 60 ± 16 | <0.0001 |
| Female gender, n (%) | 16 (38) | 47 (46) | 0.46 |
| ICU length of stay, days | 10 [8–12] | 11 [10–12] | 0.516 |
| GCS on site | 7 ± 3 | 7 ± 4 | 0.93 |
| TBI vs. non-TBI, n (%) | 26 (62) | 39 (38) | 0.01 |
| Midline shift on head CT ≥ 5 mm, n (%) | 7 (17) | 48 (47) | 0.0008 |
| Midline shift on head CT, mm | 2.0 [1.1–3] | 4.9 [3.9–5.9] | 0.003 |
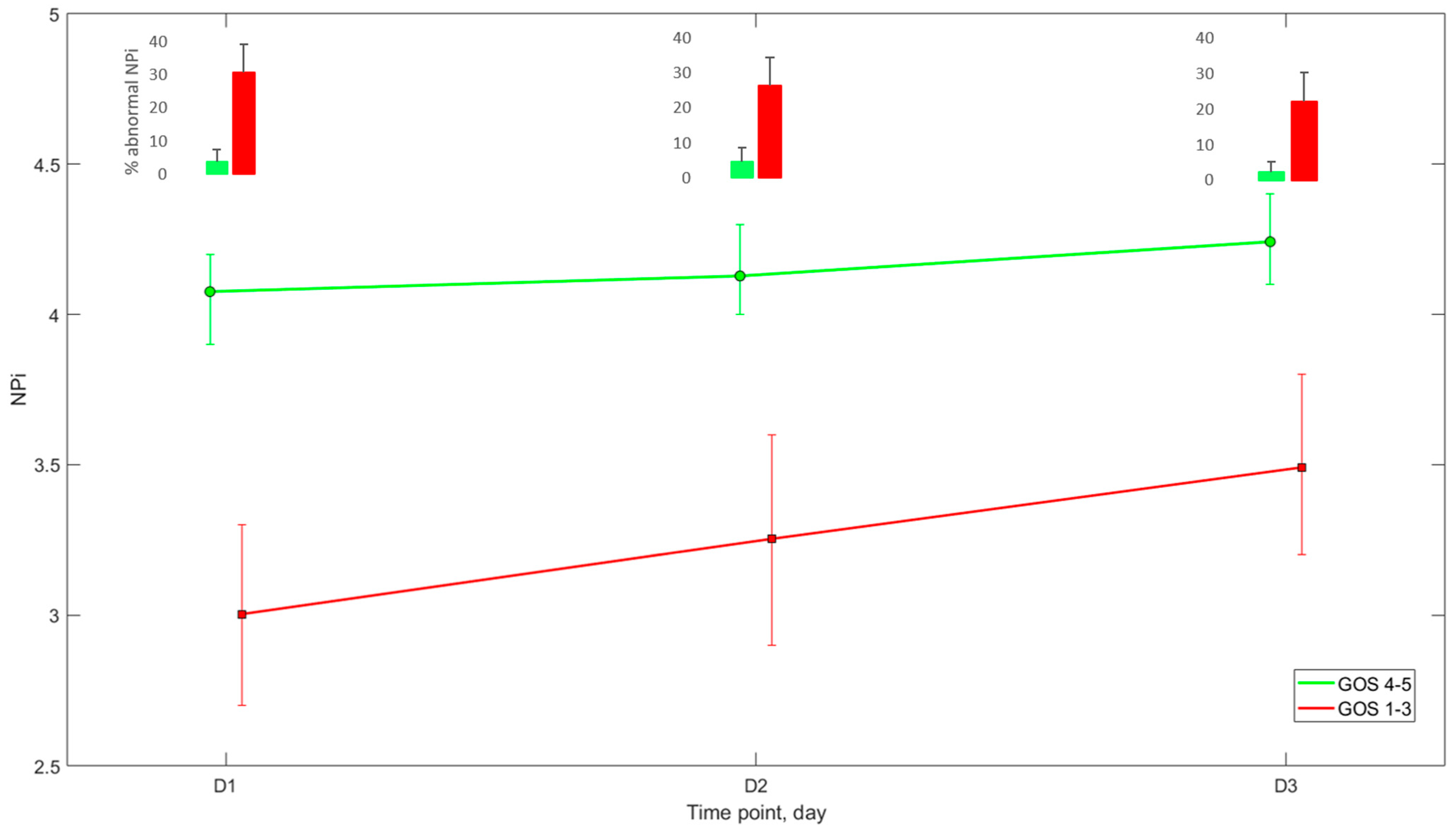
| NPi *, day 1 | 4.1 [3.9–4.2] | 3.0 [2.7–3.3] | 0.009 |
| NPi *, day 2 | 4.1 [4–4.3] | 3.3 [2.9–3.6] | 0.051 |
| NPi *, day 3 | 4.2 [4.1–4.4] | 3.5 [3.2–3.8] | 0.06 |
| Abnormal NPi < 3 (%), day 1 | 4 [0–8] | 31 [22.5–39] | 0.0001 |
| Abnormal NPi < 3 (%), day 2 | 4.5 [0.5–9] | 26.5 [18.5–34.5] | 0.003 |
| Abnormal NPi < 3 (%), day 3 | 2 [0–5] | 22 [14–30] | 0.0039 |
| Variable | Patient Number | Unfavourable Outcome (GOS 1–3) at 6 Months, n (%) | Specificity % (95% CI) | Sensitivity % (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|
| Neurological Pupil index (NPi) < 3 | ||||||
| Day 1–3 post-admission | 145 | 103 (71) | 98 (87–100) | 34 (25–44) | 97 (83–100) | 38 (34–41) |
| Day 1 | 139 | 99 (71) | 97 (85–100) | 33 (24–44) | 97 (82–100) | 33 (30–37) |
| Day 2 | 132 | 94 (71) | 97 (86–100) | 31 (22–41) | 97 (80–100) | 36 (33–40) |
| Day 3 | 119 | 83 (70) | 100 (90–100) | 24 (15–35) | 100 | 36 (34–39) |
| Head CT scan showing ≥ 5 mm midline shift | ||||||
| Day1 | 145 | 103 (71) | 83 (69–93) | 47 (37–57) | 87 (77–93) | 39 (34–44) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romagnosi, F.; Bernini, A.; Bongiovanni, F.; Iaquaniello, C.; Miroz, J.-P.; Citerio, G.; Taccone, F.S.; Oddo, M. Neurological Pupil Index for the Early Prediction of Outcome in Severe Acute Brain Injury Patients. Brain Sci. 2022, 12, 609. https://doi.org/10.3390/brainsci12050609
Romagnosi F, Bernini A, Bongiovanni F, Iaquaniello C, Miroz J-P, Citerio G, Taccone FS, Oddo M. Neurological Pupil Index for the Early Prediction of Outcome in Severe Acute Brain Injury Patients. Brain Sciences. 2022; 12(5):609. https://doi.org/10.3390/brainsci12050609
Chicago/Turabian StyleRomagnosi, Federico, Adriano Bernini, Filippo Bongiovanni, Carolina Iaquaniello, John-Paul Miroz, Giuseppe Citerio, Fabio Silvio Taccone, and Mauro Oddo. 2022. "Neurological Pupil Index for the Early Prediction of Outcome in Severe Acute Brain Injury Patients" Brain Sciences 12, no. 5: 609. https://doi.org/10.3390/brainsci12050609
APA StyleRomagnosi, F., Bernini, A., Bongiovanni, F., Iaquaniello, C., Miroz, J.-P., Citerio, G., Taccone, F. S., & Oddo, M. (2022). Neurological Pupil Index for the Early Prediction of Outcome in Severe Acute Brain Injury Patients. Brain Sciences, 12(5), 609. https://doi.org/10.3390/brainsci12050609