
Spatial Instability during Precision Grip–Lift in Children with Poor Manual Dexterity

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. The M-ABC2 Manual Dexterity Test
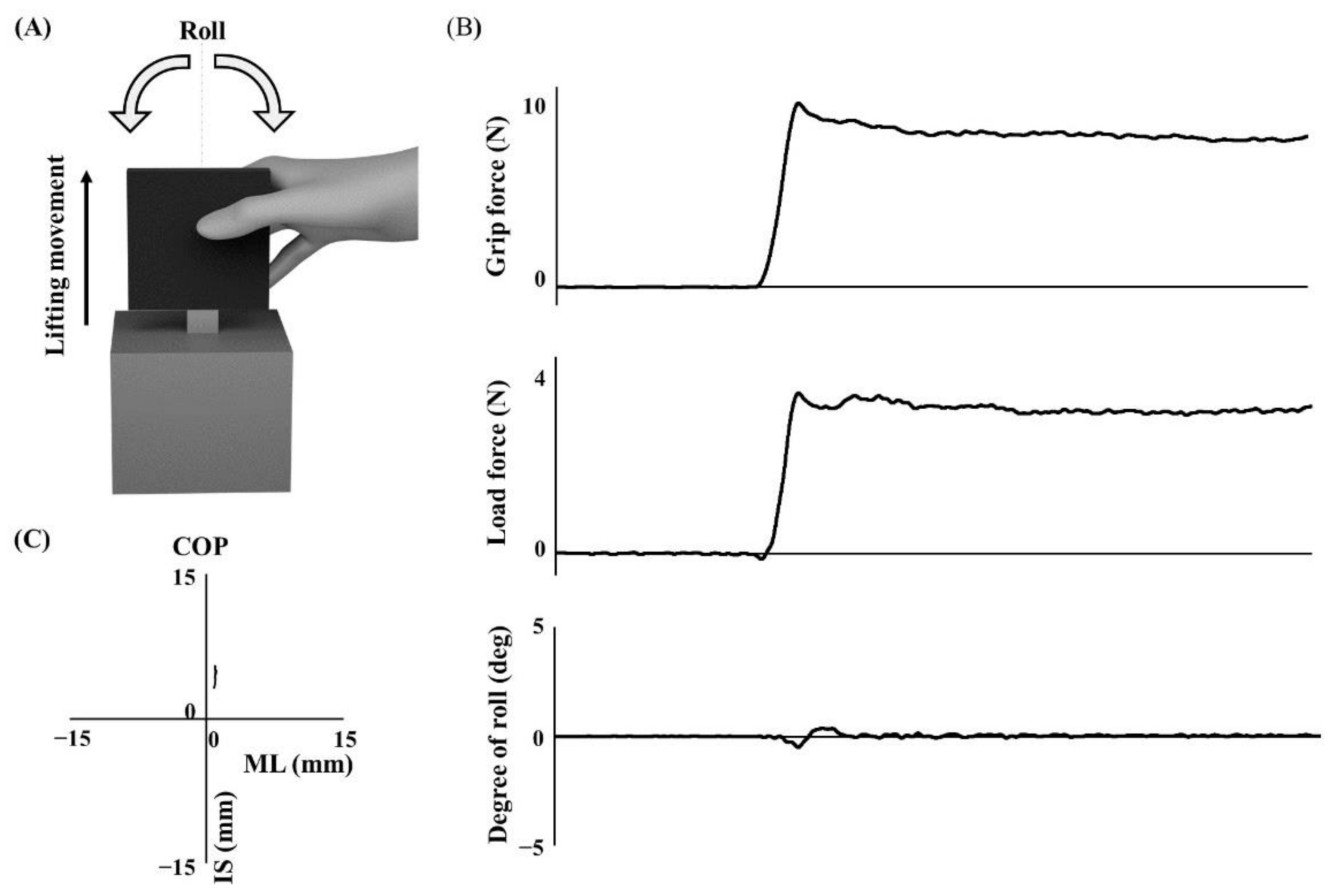
2.4. Apparatus
2.5. Grip–Lift Task
2.6. Data Processing and Statistical Analyses
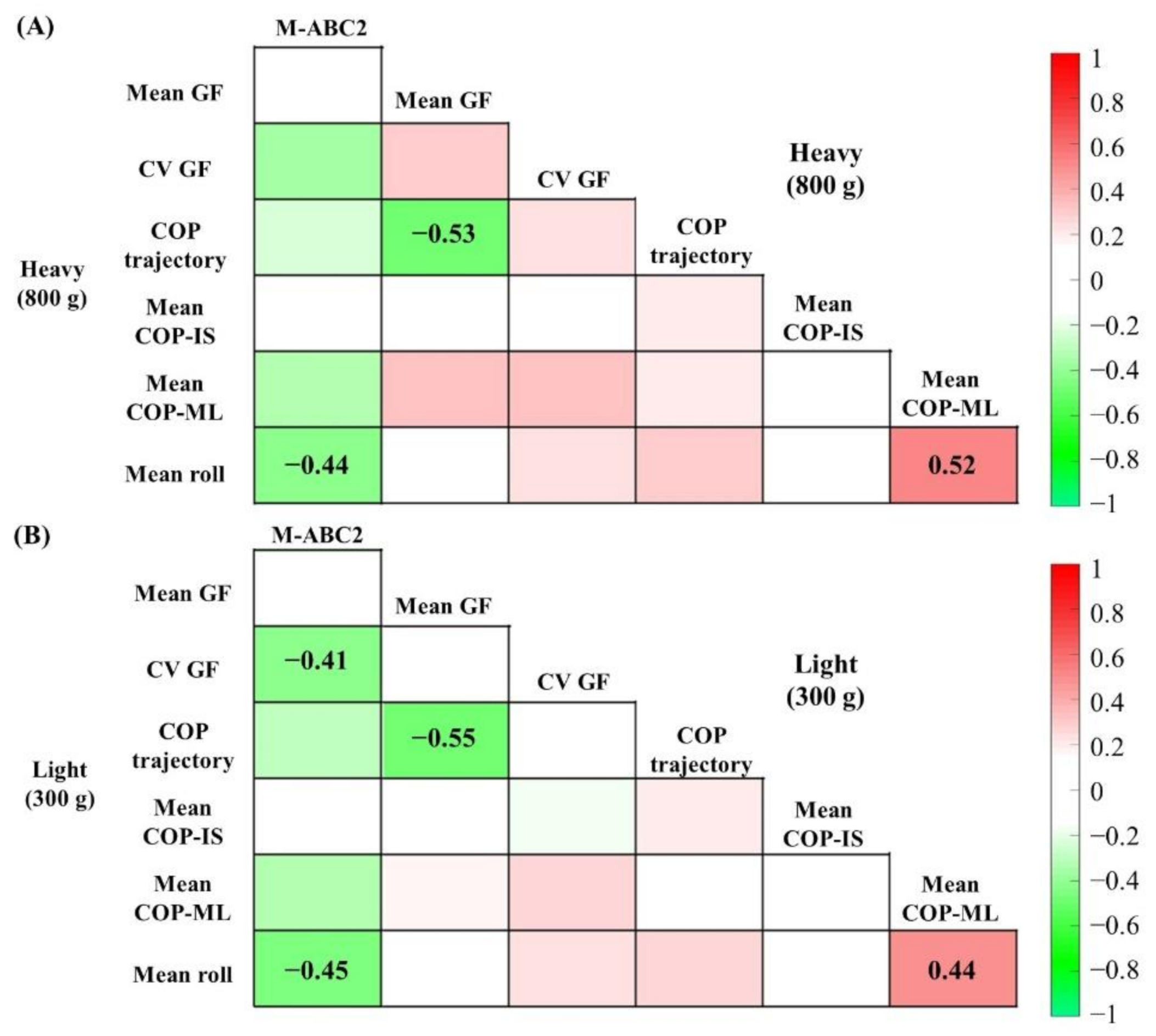
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef] [PubMed]
- Bo, J.; Bastian, A.J.; Kagerer, F.A.; Contreras-Vidal, J.L.; Clark, J.E. Temporal variability in continuous versus discontinuous drawing for children with developmental coordination disorder. Neurosci. Lett. 2008, 431, 215–220. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kagerer, F.A.; Bo, J.; Contreras-Vidal, J.L.; Clark, J.E. Visuomotor adaptation in children with developmental coordination disorder. Mot. Control 2004, 8, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Adams, I.L.J.; Lust, J.M.; Wilson, P.H.; Steenbergen, B. Compromised motor control in children with DCD: A deficit in the internal model?—A systematic review. Neurosci. Biobehav. Rev. 2014, 47, 225–244. [Google Scholar] [CrossRef]
- Wilson, P.H.; Ruddock, S.; Smits-Engelsman, B.; Polatajko, H.; Blank, R. Understanding performance deficits in developmental coordination disorder: A meta-analysis of recent research: Review. Dev. Med. Child. Neurol. 2013, 55, 217–228. [Google Scholar] [CrossRef]
- Kirby, A.; Edwards, L.; Sugden, D. Emerging adulthood in developmental co-ordination disorder: Parent and young adult perspectives. Res. Dev. Disabil. 2011, 32, 1351–1360. [Google Scholar] [CrossRef]
- Missiuna, C.; Campbell, W.N. Psychological aspects of developmental coordination disorder: Can we establish causality? Curr. Dev. Disord. Rep. 2014, 1, 125–131. [Google Scholar] [CrossRef]
- Forssberg, H.; Eliasson, A.C.; Kinoshita, H.; Johansson, R.S.; Westling, G. Development of human precision grip I: Basic coordination of force. Exp. Brain Res. 1991, 85, 451–457. [Google Scholar] [CrossRef]
- Fu, Q.; Zhang, W.; Santello, M. Anticipatory planning and control of grasp positions and forces for dexterous two-digit manipulation. J. Neurosci. 2010, 30, 9117–9126. [Google Scholar] [CrossRef]
- Nowak, D.A.; Glasauer, S.; Hermsdörfer, J. Force control in object manipulation—A model for the study of sensorimotor control strategies. Neurosci. Biobehav. Rev. 2013, 37, 1578–1586. [Google Scholar] [CrossRef]
- Flanagan, J.R.; Bowman, M.C.; Johansson, R.S. Control strategies in object manipulation tasks. Curr. Opin. Neurobiol. 2006, 16, 650–659. [Google Scholar] [CrossRef]
- Pereira, H. Parametric control of fingertip forces during precision grip lifts in children with DCD (developmental coordination disorder) and DAMP (deficits in attention motor control and perception). Neuropsychologia 2001, 39, 478–488. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.C.M.; Westenberg, Y.; Duysens, J. Children with developmental coordination disorder are equally able to generate force but show more variability than typically developing children. Hum. Mov. Sci. 2008, 27, 296–309. [Google Scholar] [CrossRef]
- Golenia, L.; Bongers, R.M.; van Hoorn, J.F.; Otten, E.; Mouton, L.J.; Schoemaker, M.M. Variability in coordination patterns in children with developmental coordination disorder (DCD). Hum. Mov. Sci. 2018, 60, 202–213. [Google Scholar] [CrossRef]
- Hyde, C.; Wilson, P. Online motor control in children with developmental coordination disorder: Chronometric analysis of double-step reaching performance. Child Care Health Dev. 2011, 37, 111–122. [Google Scholar] [CrossRef]
- Fuelscher, I.; Williams, J.; Enticott, P.G.; Hyde, C. Reduced motor imagery efficiency is associated with online control difficulties in children with probable developmental coordination disorder. Res. Dev. Disabil. 2015, 45–46, 239–252. [Google Scholar] [CrossRef]
- Nobusako, S.; Sakai, A.; Tsujimoto, T.; Shuto, T.; Nishi, Y.; Asano, D.; Furukawa, E.; Zama, T.; Osumi, M.; Shimada, S.; et al. Deficits in visuo-motor temporal integration impacts manual dexterity in probable developmental coordination disorder. Front. Neurol. 2018, 9, 114. [Google Scholar] [CrossRef]
- Nobusako, S.; Sakai, A.; Tsujimoto, T.; Shuto, T.; Nishi, Y.; Asano, D.; Furukawa, E.; Zama, T.; Osumi, M.; Shimada, S.; et al. Manual Dexterity is a strong predictor of visuo-motor temporal integration in children. Front. Psychol. 2018, 9, 948. [Google Scholar] [CrossRef]
- Augurelle, A.-S.; Smith, A.M.; Lejeune, T.; Thonnard, J.-L. Importance of cutaneous feedback in maintaining a secure grip during manipulation of hand-held objects. J. Neurophysiol. 2003, 89, 665–671. [Google Scholar] [CrossRef]
- Zhang, W.; Gordon, A.M.; Fu, Q.; Santello, M. Manipulation after object rotation reveals independent sensorimotor memory representations of digit positions and forces. J. Neurophysiol. 2010, 103, 2953–2964. [Google Scholar] [CrossRef]
- Bair, W.-N.; Barela, J.A.; Whitall, J.; Jeka, J.J.; Clark, J.E. Children with developmental coordination disorder benefit from using vision in combination with touch information for quiet standing. Gait Posture 2011, 34, 183–190. [Google Scholar] [CrossRef]
- Bair, W.-N.; Kiemel, T.; Jeka, J.J.; Clark, J.E. Development of multisensory reweighting is impaired for quiet stance control in children with developmental coordination disorder (DCD). PLoS ONE 2012, 7, e40932. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A.; Barnett, A.L. Movement Assessment Battery for Children-2, 2nd ed.; The Psychological Corporation: San Antonio, TX, USA, 2007; ISBN 978-0-7491-3608-6. [Google Scholar]
- Quaney, B.M.; Perera, S.; Maletsky, R.; Luchies, C.W.; Nudo, R.J. Impaired grip force modulation in the ipsilesional hand after unilateral middle cerebral artery stroke. Neurorehabil. Neural. Repair 2005, 19, 338–349. [Google Scholar] [CrossRef]
- Lin, B.-S.; Kuo, S.-F.; Lee, I.-J.; Lu, L.-H.; Chen, P.-Y.; Wang, P.-C.; Lai, C.-H.; Wang, X.-M.; Lin, C.-H. The impact of aging and reaching movements on grip stability control during manual precision tasks. BMC Geriatr. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Akiyama, R.; Noguchi, N.; Kondo, K.; Tanaka, K.; Lee, B. Aging and bimanual effects on finger center of pressure during precision grip: Different strategies for spatial stability. Sensors 2021, 21, 8396. [Google Scholar] [CrossRef]
- Kurihara, J.; Lee, B.; Hara, D.; Noguchi, N.; Yamazaki, T. Increased center of pressure trajectory of the finger during precision grip task in stroke patients. Exp. Brain Res. 2019, 237, 327–333. [Google Scholar] [CrossRef]
- Gutterman, J.; Lee-Miller, T.; Friel, K.M.; Dimitropoulou, K.; Gordon, A.M. Anticipatory motor planning and control of grasp in children with unilateral spastic cerebral palsy. Brain Sci. 2021, 11, 1161. [Google Scholar] [CrossRef]
- Marneweck, M.; Lee-Miller, T.; Santello, M.; Gordon, A.M. Digit position and forces covary during anticipatory control of whole-hand manipulation. Front. Hum. Neurosci. 2016, 10, 461. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. Stat. Theory Appl. 1979, 6, 65–70. [Google Scholar]
- Parikh, P.J.; Cole, K.J. Handling objects in old age: Forces and moments acting on the object. J. Appl. Physiol. 2012, 112, 1095–1104. [Google Scholar] [CrossRef]
- Deconinck, F.J.A.; De Clercq, D.; Van Coster, R.; Ooostra, A.; Dewitte, G.; Savelsbergh, G.J.P.; Cambier, D.; Lenoir, M. Sensory contributions to balance in boys with developmental coordination disorder. Adapt. Phys. Act. Q. 2008, 25, 17–35. [Google Scholar] [CrossRef]
- Licari, M.K.; Reynolds, J.E. Understanding performance variability in developmental coordination disorder: What does it all mean? Curr. Dev. Disord. Rep. 2017, 4, 53–59. [Google Scholar] [CrossRef]
- Lukos, J.R.; Ansuini, C.; Santello, M. Anticipatory control of grasping: Independence of sensorimotor memories for kinematics and kinetics. J. Neurosci. 2008, 28, 12765–12774. [Google Scholar] [CrossRef]
- Zoia, S.; Castiello, U.; Blason, L.; Scabar, A. Reaching in children with and without developmental coordination disorder under normal and perturbed vision. Dev. Neuropsychol. 2005, 27, 257–273. [Google Scholar] [CrossRef]
- Davidson, P.R.; Wolpert, D.M. Widespread access to predictive models in the motor system: A short review. J. Neural. Eng. 2005, 2, S313–S319. [Google Scholar] [CrossRef]
- Wolpert, D.M. Computational approaches to motor control. Trends Cogn. Sci. 1997, 1, 209–216. [Google Scholar] [CrossRef]
- Williams, J.; Thomas, P.R.; Maruff, P.; Butson, M.; Wilson, P.H. Motor, visual and egocentric transformations in children with developmental coordination disorder. Child Care Health Dev. 2006, 32, 633–647. [Google Scholar] [CrossRef]
- Bo, J.; Lee, C.-M. Motor skill learning in children with developmental coordination disorder. Res. Dev. Disabil. 2013, 34, 2047–2055. [Google Scholar] [CrossRef]
- Itzcovich, E.; Riani, M.; Sannita, W.G. Stochastic resonance improves vision in the severely impaired. Sci. Rep. 2017, 7, 12840. [Google Scholar] [CrossRef]
- Lakshminarayanan, K.; Lauer, A.W.; Ramakrishnan, V.; Webster, J.G.; Seo, N.J. Application of vibration to wrist and hand skin affects fingertip tactile sensation. Physiol. Rep. 2015, 3, e12465. [Google Scholar] [CrossRef]
- Nobusako, S.; Osumi, M.; Matsuo, A.; Furukawa, E.; Maeda, T.; Shimada, S.; Nakai, A.; Morioka, S. Subthreshold vibrotactile noise stimulation immediately improves manual dexterity in a child with developmental coordination disorder: A single-case study. Front. Neurol. 2019, 10, 717. [Google Scholar] [CrossRef]
- Nobusako, S.; Osumi, M.; Matsuo, A.; Furukawa, E.; Maeda, T.; Shimada, S.; Nakai, A.; Morioka, S. Influence of Stochastic Resonance on Manual Dexterity in Children with Developmental Coordination Disorder: A Double-Blind Interventional Study. Front. Neurol. 2021, 12, 626608. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Low Manual Dexterity | High Manual Dexterity | |
|---|---|---|
| Sample | 11 | 55 |
| Age, y | 9.00 (±2.30) | 9.16 (±1.93) |
| Sex: | ||
| Male | 4 | 28 |
| Female | 7 | 27 |
| Preferred hand: | ||
| Right | 10 | 53 |
| Left | 1 | 2 |
| M-ABC-2 percentile score | 12.45 (±5.02) | 70.38 (±21.90) |
| Mean ± SD | Two-Way ANOVA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low Manual Dexterity | High Manual Dexterity | Weight | Group | Interaction | |||||||||
| Heavy | Light | Heavy | Light | F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |
| Mean GF, N | 10.94 ± 1.97 | 4.36 ± 1.26 | 10.49 ± 1.93 | 4.29 ± 1.24 | 273.78 | <0.01 | 0.68 | 0.49 | 0.49 | <0.01 | 0.25 | 0.62 | <0.01 |
| CV, GF | 0.45 ± 0.14 | 0.38 ± 0.06 | 0.34 ± 0.04 | 0.32 ± 0.05 | 9.83 | <0.01 | 0.07 | 33.66 | <0.01 | 0.21 | 3.54 | 0.06 | 0.03 |
| COP trajectory, mm | 34.13 ± 9.18 | 57.78 ± 16.28 | 27.21 ± 8.94 | 38.04 ± 13.65 | 37.73 | <0.01 | 0.23 | 22.56 | <0.01 | 0.16 | 5.22 | <0.05 | 0.04 |
| Mean COP-IS, mm | 15.83 ± 5.78 | 16.6 ± 8.04 | 17.24 ± 5.71 | 15.6 ± 5.58 | 0.10 | 0.75 | <0.01 | 0.02 | 0.88 | <0.01 | 0.75 | 0.39 | <0.01 |
| Mean COP-ML, mm | 8.70 ± 4.44 | 8.85 ± 5.01 | 3.99 ± 1.79 | 3.69 ± 1.62 | 0.01 | 0.91 | <0.01 | 70.27 | <0.01 | 0.35 | 0.15 | 0.70 | <0.01 |
| Mean roll deg | 3.22 ± 1.52 | 3.15 ± 1.33 | 1.04 ± 0.45 | 1.14 ± 0.44 | 1.47 | 0.23 | <0.01 | 163.96 | <0.01 | 0.56 | 0.28 | 0.60 | <0.01 |
| Post-Hoc Analysis | |||||||||||||
| Between Weight | Between Group | ||||||||||||
| Low Manual Dexterity | High Manual Dexterity | Heavy | Light | ||||||||||
| p | d | p | d | p | d | p | d | ||||||
| COP trajectory, mm | <0.01 | 1.95 | <0.01 | 0.89 | 0.08 | 0.57 | <0.01 | 1.62 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishi, Y.; Nobusako, S.; Tsujimoto, T.; Sakai, A.; Nakai, A.; Morioka, S. Spatial Instability during Precision Grip–Lift in Children with Poor Manual Dexterity. Brain Sci. 2022, 12, 598. https://doi.org/10.3390/brainsci12050598
Nishi Y, Nobusako S, Tsujimoto T, Sakai A, Nakai A, Morioka S. Spatial Instability during Precision Grip–Lift in Children with Poor Manual Dexterity. Brain Sciences. 2022; 12(5):598. https://doi.org/10.3390/brainsci12050598
Chicago/Turabian StyleNishi, Yuki, Satoshi Nobusako, Taeko Tsujimoto, Ayami Sakai, Akio Nakai, and Shu Morioka. 2022. "Spatial Instability during Precision Grip–Lift in Children with Poor Manual Dexterity" Brain Sciences 12, no. 5: 598. https://doi.org/10.3390/brainsci12050598
APA StyleNishi, Y., Nobusako, S., Tsujimoto, T., Sakai, A., Nakai, A., & Morioka, S. (2022). Spatial Instability during Precision Grip–Lift in Children with Poor Manual Dexterity. Brain Sciences, 12(5), 598. https://doi.org/10.3390/brainsci12050598