
A Rare Neuro-Ophthalmological Condition in a Patient with Lung Adenocarcinoma: The Eight-and-a-Half Syndrome, Case Report and Review of the Literature

 , and
, and 
Abstract
1. Introduction
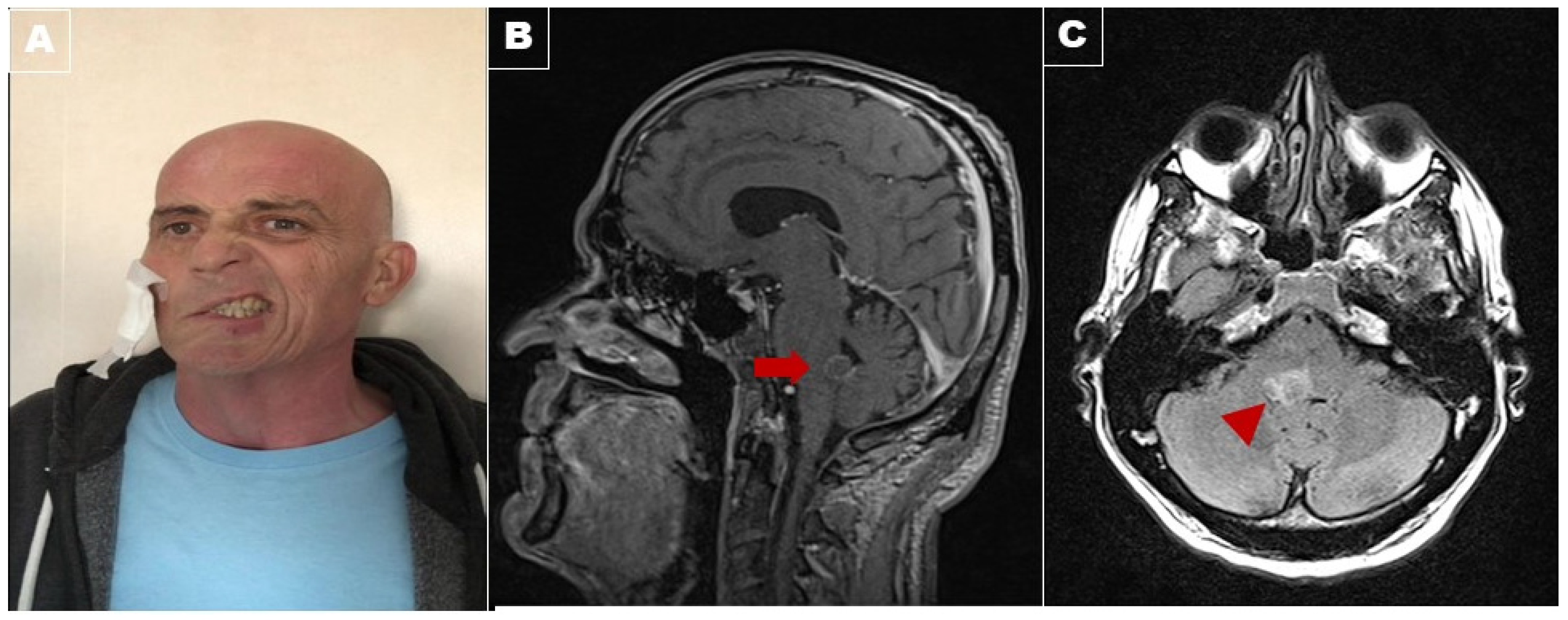
2. Case Report
3. Discussion

{kind=link}
| Etiopathology | Reference | |
|---|---|---|
| Cerebrovascular disease (73%) | Ischemic (60%) | Ahmed [24] |
| Almutlaq [38] | ||
| Bocos-Portillo [9] | ||
| Cole [37] | ||
| Duffy [10] | ||
| Eggenberger [3] | ||
| Green [4] | ||
| Menéndez [39] | ||
| Nandhagopal [5] | ||
| Rosini [33] | ||
| Kumar [34] | ||
| Sarwal [40] | ||
| Shin [41] | ||
| Uysal [42] | ||
| Xie [43] | ||
| Wondergem [44] | ||
| Cavernoma (7%) | Maier [25] | |
| Perković [26] | ||
| Intracranial capillary telangiectasia (3%) | Li [27] | |
| Hemorrhage (3%) | Xia [28] | |
| Multiple sclerosis (17%) | Cárdenas-Rodríguez [2] Guler [6] | |
| Mortzos [29] | ||
| Skaat [45] | ||
| Wanono [46] | ||
| Tuberculosis (7%) | Shao [7] | |
| van Toorn [30] | ||
| Metastases (3%) | Ortiz-Pérez [8] | |
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sciacca, S.; Lynch, J.; Davagnanam, I.; Barker, R. Midbrain, Pons, and Medulla: Anatomy and Syndromes. Radiographics 2019, 39, 1110–1125. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas-Rodríguez, M.A.; Castillo-Torres, S.A.; Chávez-Luévanos, B.; De León-Flores, L. Eight-and-a-half syndrome: Video evidence and updated literature review. BMJ Case Rep. 2020, 13, e234075. [Google Scholar] [CrossRef] [PubMed]
- Eggenberger, E. Eight-and-a-half syndrome: One-and-a-half syndrome plus cranial nerve VII palsy. J. Neuro Ophthalmol. 1998, 18, 114–116. [Google Scholar] [CrossRef]
- Green, K.E.; Rastall, D.P.W.; Eggenberger, E.R. Eight Syndrome: Horizontal Gaze Palsy Plus Ipsilateral Seventh Nerve Palsy. J. Neuroophthalmol. 2018, 38, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Nandhagopal, R.; Krishnamoorthy, S.G. Neurological picture. Eight-and-a-half syndrome. J. Neurol. Neurosurg. Psychiatry 2006, 77, 463. [Google Scholar] [CrossRef]
- Keskin Guler, S.; Güneş, N.; Gokce Cokal, B.; Yurtdaş, M.; Yoldas, T. As the first sign of multiple sclerosis, eight-and-a-half syndrome. Neurol. Sci. 2017, 39, 945–947. [Google Scholar] [CrossRef]
- Shao, K.; Dong, F.; Guo, S.; Wang, J.; Sun, Z. Eight-and-a-half syndrome caused by tuberculous meningitis: A case report. Acta Neurol. Belg. 2021, 121, 591–593. [Google Scholar] [CrossRef]
- Ortiz-Pérez, S.; Sánchez-Dalmau, B.; Mesquida, M.; Fernández, E.; Adán, A. Eight-and-a-half syndrome. Med. Clin. 2010, 134, 45. [Google Scholar] [CrossRef]
- Bocos-Portillo, J.; Ojeda, J.R.; Gomez-Beldarrain, M.; Vazquez-Picon, R.; Garcia-Monco, J.C. Eight-and-a-Half Syndrome. JAMA Neurol. 2015, 72, 830. [Google Scholar] [CrossRef]
- Duffy, A.; Shen, P.Y.; Verro, P.; Nidecker, A.E.; Chow, M. Eight-and-a-half syndrome. Neurol. Clin. Pract. 2014, 4, 526–527. [Google Scholar] [CrossRef]
- Adamczyk, C.; Horn, A. Chapter 9—Reticular Formation: Eye Movements, Gaze, and Blinks. In The Human Nervous System; Elsevier Academic Press: Amsterdam, The Netherlands, 2012; pp. 328–366. ISBN 978-0-12-374236-0. [Google Scholar]
- Büttner-Ennever, J.A. The extraocular motor nuclei: Organization and functional neuroanatomy. Prog. Brain Res. 2006, 151, 95–125. [Google Scholar] [CrossRef] [PubMed]
- Strassman, A.; Highstein, S.M.; McCrea, R.A. Anatomy and physiology of saccadic burst neurons in the alert squirrel monkey. II. Inhibitory burst neurons. J. Comp. Neurol. 1986, 249, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Büttner-Ennever, J.A.; Cohen, B.; Pause, M.; Fries, W. Raphe nucleus of the pons containing omnipause neurons of the oculomotor system in the monkey, and its homologue in man. J. Comp. Neurol. 1988, 267, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Barrios, R.R.; Bottinelli, M.D.; Medoc, J. The study of ocular motility in the comatose patient. J. Neurol. Sci. 1966, 3, 183–206. [Google Scholar] [CrossRef]
- Horn, A.K.E.; Helmchen, C.; Wahle, P. GABAergic neurons in the rostral mesencephalon of the macaque monkey that control vertical eye movements. Ann. N. Y. Acad. Sci. 2003, 1004, 19–28. [Google Scholar] [CrossRef]
- Kochar, P.S.; Kumar, Y.; Sharma, P.; Kumar, V.; Gupta, N.; Goyal, P. Isolated medial longitudinal fasciculus syndrome: Review of imaging, anatomy, pathophysiology and differential diagnosis. Neuroradiol. J. 2018, 31, 95. [Google Scholar] [CrossRef]
- Villano, J.L.; Durbin, E.B.; Normandeau, C.; Thakkar, J.P.; Moirangthem, V.; Davis, F.G. Incidence of brain metastasis at initial presentation of lung cancer. Neuro. Oncol. 2015, 17, 122–128. [Google Scholar] [CrossRef]
- Kwon, H.; Kim, J.W.; Park, M.; Kim, J.W.; Kim, M.; Suh, S.H.; Chang, Y.S.; Ahn, S.J.; Lee, J.M. Brain Metastases From Lung Adenocarcinoma May Preferentially Involve the Distal Middle Cerebral Artery Territory and Cerebellum. Front. Oncol. 2020, 10, 1664. [Google Scholar] [CrossRef]
- Vara-Castrodeza, A.; Torrego-García, J.C.; Puertas-Álvarez, J.L.; Mendo-González, M. Pontine metastases as a cause of dysphagia in lung carcinoma. Clin. Transl. Oncol. 2005, 7, 512–514. [Google Scholar] [CrossRef]
- Andrews, D.W.; Scott, C.B.; Sperduto, P.W.; Flanders, A.E.; Gaspar, L.E.; Schell, M.C.; Werner-Wasik, M.; Demas, W.; Ryu, J.; Bahary, J.P.; et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase III results of the RTOG 9508 randomised trial. Lancet 2004, 363, 1665–1672. [Google Scholar] [CrossRef]
- Kumral, E.; Bayülkem, G.; Evyapan, D. Clinical spectrum of pontine infarction. Clinical-MRI correlations. J. Neurol. 2002, 249, 1659–1670. [Google Scholar] [CrossRef] [PubMed]
- Satake, M.; Kira, J.I.; Yamada, T.; Kobayashi, T. Raymond syndrome (alternating abducent hemiplegia) caused by a small haematoma at the medial pontomedullary junction. J. Neurol. Neurosurg. Psychiatry 1995, 58, 261. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ahmed, H.A.; Al Assaf, O.Y.; Alzarooni, H.M.; Sarathchandran, P. Clinical findings of eight-and-a-half syndrome. Oxford Med. Case Rep. 2020, 2020, 357–358. [Google Scholar] [CrossRef]
- Maier, S.; Motataianu, A.; Bajko, Z.; Romaniuc, A.; Balasa, A. Pontine cavernoma haemorrhage at 24 weeks of pregnancy that resulted in eight-and-a-half syndrome. Acta Neurol. Belg. 2019, 119, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Perković, R.; Kovačević, M.; Buljan, K.; Tomić, S.; Mužević, D. Cavernoma of the fourth ventricle presenting as the eight-and-a-half syndrome. Acta Neurol. Belg. 2021, 121, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Hou, D.; Deng, Y.; Tian, Y. Eight-and-a-Half Syndrome: A Combination of Intracranial Capillary Telangiectasia and Hematencephalon. J. Stroke Cerebrovasc. Dis. 2018, 27, e135–e137. [Google Scholar] [CrossRef] [PubMed]
- Xia, N.G.; Chen, Y.; Li, J.; Chen, X.; Ye, Z.S.; Chen, S.Y.; Zhu, Z.G. Eight-and-a-half syndrome caused by a pontine haemorrhage: A case report and review of the literature. Int. J. Neurosci. 2018, 128, 746–750. [Google Scholar] [CrossRef]
- Mortzos, P.; Nordling, M.M.; Sørensen, T.L. Eight-and-a-half syndrome as presenting sign of childhood multiple sclerosis. J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2014, 18, 490–492. [Google Scholar] [CrossRef]
- van Toorn, R.; Schoeman, J.F.; Donald, P.R. Brainstem tuberculoma presenting as eight-and-a-half syndrome. Eur. J. Paediatr. Neurol. 2006, 10, 41–44. [Google Scholar] [CrossRef]
- Marquart, C.; Strauss, C.; Alfieri, A. Eight-and-a-half syndrome combined with an ipsilateral vertical gaze palsy: A pathophysiological explanation. Clin. Neurol. Neurosurg. 2013, 115, 767–769. [Google Scholar] [CrossRef]
- Felicio, A.C.; Bichuetti, D.B.; Marin, L.F.; dos Santos, W.A.C.; Godeiro-Junior, C. Bilateral horizontal gaze palsy with unilateral peripheral facial paralysis caused by pontine tegmentum infarction. J. Stroke Cerebrovasc. Dis. 2009, 18, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Rosini, F.; Pretegiani, E.; Guideri, F.; Cerase, A.; Rufa, A. Eight and a half syndrome with hemiparesis and hemihypesthesia: The nine syndrome? J. Stroke Cerebrovasc. Dis. 2013, 22, e637–e638. [Google Scholar] [CrossRef] [PubMed]
- Sampath Kumar, N.S.; Raju, C.G.; Kiran, P.R.; Kumar, T.A.; Gopal, B.V.; Khaseem, D.B. Eight-and-a-half syndrome: A rare presentation of pontine infarction. J. Stroke Cerebrovasc. Dis. 2014, 23, e389–e391. [Google Scholar] [CrossRef] [PubMed]
- Allbon, D.S.; Hood, B. La Thirteen-and-a-half syndrome. J. Neuro Ophthalmol. 2016, 36, 191–192. [Google Scholar] [CrossRef]
- Bae, J.S.; Song, H.K. One-and-a-half syndrome with facial diplegia: The 15 1/2 syndrome? J. Neuroophthalmol. 2005, 25, 52–53. [Google Scholar] [CrossRef]
- Cole, D.F.; Wiggins, R.; Carrera, J.; Worrall, B. Teaching Video NeuroImages: From 9 to 8-and-a-Half Syndrome After tPA: The Rebirth of Fellini. Neurology 2021, 96, e1699–e1700. [Google Scholar] [CrossRef]
- Almutlaq, A.; Richard, A. Eight-and-a-half syndrome: One-and-a-half syndrome with peripheral facial nerve palsy. CMAJ 2018, 190, E510. [Google Scholar] [CrossRef]
- Fernández Menéndez, S.; Redondo Robles, L.; Lara Lezama, L.B.; Tejada García, J. Eight and a half syndrome caused by a stroke. Med. Clin. 2015, 144, e23. [Google Scholar] [CrossRef]
- Sarwal, A.; Garewal, M.; Sahota, S.; Sivaraman, M. Eight-and-a-half syndrome. J. Neuroimaging 2009, 19, 288–290. [Google Scholar] [CrossRef]
- Shin, C.; Lee, D.; Ahn, T.B.; Lee, K.M. Hemifacial spasm after eight-and-a-half syndrome. Parkinsonism Relat. Disord. 2018, 54, 123–124. [Google Scholar] [CrossRef]
- Uysal, S.; Demirtas-Tatlidede, A.; Selcuk, O.Y.; Yayla, V. Diffusion-weighted imaging in eight-and-a-half syndrome presenting with transient hemiparesis. Clin. Neuroradiol. 2013, 23, 235–236. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.J.; Yu, H.Q.; Wang, Y.H.; Liu, Q.; Meng, H.M. A case report of eight and a half syndrome. Neurol. Sci. 2016, 37, 821–822. [Google Scholar] [CrossRef] [PubMed]
- Wondergem, N.E.; Ziylan, F.; Bot, J.C.J.; Visser, M.C.; Rinkel, R.N.P.M. Eight-and-a-half syndrome: A complex clinical syndrome caused by a single central lesion. Clin. Neurol. Neurosurg. 2020, 194, 105812. [Google Scholar] [CrossRef] [PubMed]
- Skaat, A.; Huna-Baron, R. Eight-and-a-half syndrome: A rare pontine neuro-ophthalmologic syndrome. Arch. Neurol. 2012, 69, 934–935. [Google Scholar] [CrossRef] [PubMed]
- Wanono, R.; Daelman, L.; Maarouf, A.; Caucheteux, N.; Chaunu, M.P.; Tourbah, A. Eight and a half plus syndrome as a first presentation of multiple sclerosis. Rev. Neurol. 2014, 170, 553–554. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruciani, A.; Motolese, F.; Todisco, A.; Di Lazzaro, V.; Assenza, G. A Rare Neuro-Ophthalmological Condition in a Patient with Lung Adenocarcinoma: The Eight-and-a-Half Syndrome, Case Report and Review of the Literature. Brain Sci. 2022, 12, 451. https://doi.org/10.3390/brainsci12040451
Cruciani A, Motolese F, Todisco A, Di Lazzaro V, Assenza G. A Rare Neuro-Ophthalmological Condition in a Patient with Lung Adenocarcinoma: The Eight-and-a-Half Syndrome, Case Report and Review of the Literature. Brain Sciences. 2022; 12(4):451. https://doi.org/10.3390/brainsci12040451
Chicago/Turabian StyleCruciani, Alessandro, Francesco Motolese, Antonio Todisco, Vincenzo Di Lazzaro, and Giovanni Assenza. 2022. "A Rare Neuro-Ophthalmological Condition in a Patient with Lung Adenocarcinoma: The Eight-and-a-Half Syndrome, Case Report and Review of the Literature" Brain Sciences 12, no. 4: 451. https://doi.org/10.3390/brainsci12040451
APA StyleCruciani, A., Motolese, F., Todisco, A., Di Lazzaro, V., & Assenza, G. (2022). A Rare Neuro-Ophthalmological Condition in a Patient with Lung Adenocarcinoma: The Eight-and-a-Half Syndrome, Case Report and Review of the Literature. Brain Sciences, 12(4), 451. https://doi.org/10.3390/brainsci12040451