
Is It Just Face Blindness? Exploring Developmental Comorbidity in Individuals with Self-Reported Developmental Prosopagnosia



Abstract
:1. Introduction
2. Material and Methods
2.1. Which Neurodevelopmental Deficits and Conditions Could Be Relevant to Assess?
2.2. Participants
2.3. Data Collection
2.4. Measures
2.4.1. The Difficulties and Abilities in Developmental Prosopagnosia Questionnaire
2.4.2. The 20-Item Prosopagnosia Index (PI20)
2.4.3. Items from the Wayfinding Questionnaire
2.4.4. Items from the Adult Reading History Questionnaire
2.4.5. Items Concerning Mathematical Ability
2.4.6. Open-Ended Questions Regarding Difficulties and Abilities
3. Data Analysis
3.1. Statistical Analysis
3.1.1. The Effect of Prosopagnosia Severity on the Presence of Developmental Comorbidity
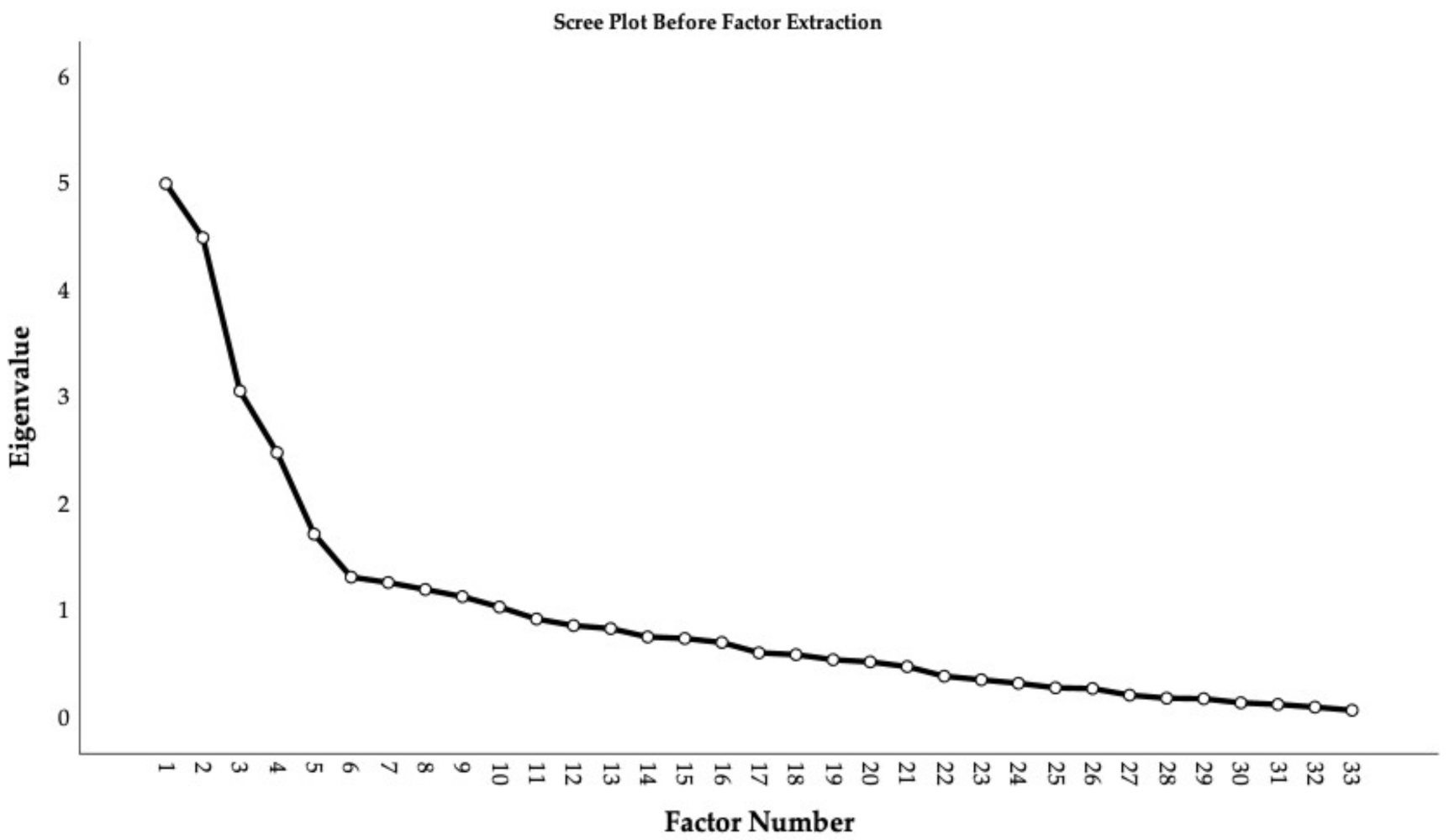
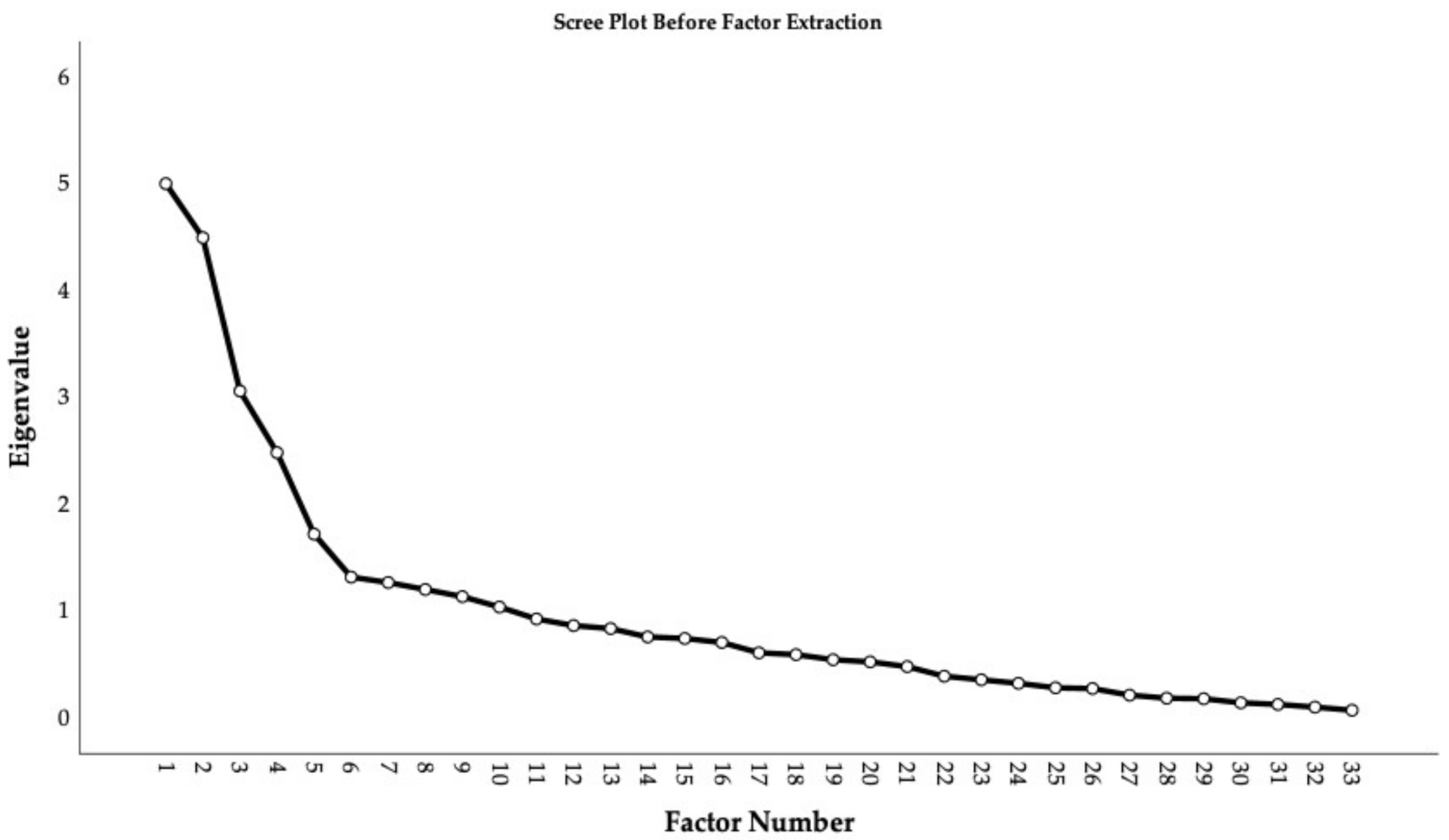
3.1.2. Exploratory Factor Analysis of the Difficulties and Abilities in Developmental Prosopagnosia Questionnaire
3.2. Qualitative Analysis
4. Results
4.1. Amount of Self-Reported Developmental Comorbidity
4.2. Prosopagnosia Severity and Developmental Comorbidity
4.3. Factor Structure of the Difficulties and Abilities in Developmental Prosopagnosia Questionnaire
4.4. Qualitative Categories from the Open-Ended Questions
5. Discussion
5.1. Discussion of Results
5.1.1. Summary of Results
5.1.2. Discussion of Quantitative Results
5.1.3. Comparing the Quantitative and Qualitative Results
‘(…) At work we have to make sure we do not walk within 5 m of an operational machine. I cannot imagine how far that is. I need to memorize the spots where the machines are often positioned, and memorise where I can walk based on where others have walked safely. I will not pass a machine in an unfamiliar spot without instruction from driver or my manager to do so because I can’t tell if I’m at a safe distance.’
‘I am very artistic. I have shown my work and been featured in a variety of mediums throughout my whole life. Most specifically I paint faces and have since I was about 12 years old and was fascinated with faces.’
5.2. General Discussion
5.2.1. High Rates of Self-Reported Developmental Comorbidity in s-DP
5.2.2. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dalrymple, K.A.; Palermo, R. Guidelines for studying developmental prosopagnosia in adults and children. Wiley Interdiscip. Rev. Cogn. Sci. 2016, 7, 73–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yardley, L.; McDermott, L.; Pisarski, S.; Duchaine, B.; Nakayama, K. Psychosocial consequences of developmental prosopagnosia: A problem of recognition. J. Psychosom. Res. 2008, 65, 445–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalrymple, K.A.; Fletcher, K.; Corrow, S.; das Nair, R.; Barton, J.J.S.; Yonas, A.; Duchaine, B. ‘A room full of strangers every day’: The psychosocial impact of developmental prosopagnosia on children and their families. J. Psychosom. Res. 2014, 77, 144–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, D.R. We need a simple test for prosopagnosia. BMJ 2011, 342, 710. [Google Scholar] [CrossRef]
- Barton, J.J.S. Structure and function in acquired prosopagnosia: Lessons from a series of 10 patients with brain damage. J. Neuropsychol. 2008, 2, 197–225. [Google Scholar] [CrossRef]
- Starrfelt, R.; Barton, J.J.S. Prosopagnosia. In Encyclopedia of Behavioral Neuroscience, 2nd ed.; Della Sala, S., Ed.; Elsevier: Oxford, UK, 2022; pp. 597–604. [Google Scholar]
- Kress, T.; Daum, I. Developmental Prosopagnosia: A Review. Behav. Neurol. 2003, 14, 109–121. [Google Scholar] [CrossRef] [Green Version]
- Bate, S.; Tree, J.J. The Definition and Diagnosis of Developmental Prosopagnosia. Q. J. Exp. Psychol. 2017, 70, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Bowles, D.C.; McKone, E.; Dawel, A.; Duchaine, B.; Palermo, R.; Schmalzl, L.; Rivolta, D.; Wilson, C.E.; Yovel, G. Diagnosing prosopagnosia: Effects of ageing, sex, and participant–stimulus ethnic match on the Cambridge Face Memory Test and Cambridge Face Perception Test. Cogn. Neuropsychol. 2009, 26, 423–455. [Google Scholar] [CrossRef]
- Kennerknecht, I.; Grueter, T.; Welling, B.; Wentzek, S.; Horst, J.; Edwards, S.; Grueter, M. First report of prevalence of non-syndromic hereditary prosopagnosia (HPA). Am. J. Med. Genet. Part A 2006, 140A, 1617–1622. [Google Scholar] [CrossRef]
- Barton, J.J.S.; Corrow, S.L. The problem of being bad at faces. Neuropsychologia 2016, 89, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, E.J.; Power, H.; Fawcett, J.M. Women Are at Greater Risk of OCD Than Men: A Meta-Analytic Review of OCD Prevalence Worldwide. J. Clin. Psychiatry 2020, 81, e1–e13. [Google Scholar] [CrossRef]
- Ohnishi, T.; Kobayashi, H.; Yajima, T.; Koyama, T.; Noguchi, K. Psychiatric comorbidities in adult attention-deficit/hyperactivity disorder: Prevalence and patterns in the routine clinical setting. Innov. Clin. Neurosci. 2019, 16, 11–16. [Google Scholar]
- Kessler, R.C.; Adler, L.; Barkley, R.; Biederman, J.; Conners, C.K.; Demler, O.; Faraone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The Prevalence and Correlates of Adult ADHD in the United States: Results From the National Comorbidity Survey Replication. Am. J. Psychiatry 2006, 163, 716–723. [Google Scholar] [CrossRef]
- Bate, S.; Adams, A.; Bennetts, R.; Line, H. Developmental prosopagnosia with concurrent topographical difficulties: A case report and virtual reality training programme. Neuropsychol. Rehabil. 2019, 29, 1290–1312. [Google Scholar] [CrossRef]
- Gray, K.L.H.; Cook, R. Should developmental prosopagnosia, developmental body agnosia, and developmental object agnosia be considered independent neurodevelopmental conditions? Cogn. Neuropsychol. 2018, 35, 59–62. [Google Scholar] [CrossRef]
- Biotti, F.; Gray, K.L.H.; Cook, R. Is developmental prosopagnosia best characterised as an apperceptive or mnemonic condition? Neuropsychologia 2019, 124, 285–298. [Google Scholar] [CrossRef]
- Liu, X.; Li, X.; Song, Y.; Liu, J. Separate and shared neural basis of face memory and face perception in developmental prosopagnosia. Front. Behav. Neurosci. 2021, 15. [Google Scholar] [CrossRef] [PubMed]
- Duchaine, B.; Nakayama, K. Dissociations of Face and Object Recognition in Developmental Prosopagnosia. J. Cogn. Neurosci. 2005, 17, 249–261. [Google Scholar] [CrossRef] [Green Version]
- Duchaine, B.; Germine, L.; Nakayama, K. Family resemblance: Ten family members with prosopagnosia and within-class object agnosia. Cogn. Neuropsychol. 2007, 24, 419–430. [Google Scholar] [CrossRef]
- Rubino, C.; Corrow, S.L.; Corrow, J.C.; Duchaine, B.; Barton, J.J.S. Word and text processing in developmental prosopagnosia. Cogn. Neuropsychol. 2016, 33, 315–328. [Google Scholar] [CrossRef]
- Burns, E.J.; Bennetts, R.J.; Bate, S.; Wright, V.C.; Weidemann, C.T.; Tree, J.J. Intact word processing in developmental prosopagnosia. Sci. Rep. 2017, 7, 1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starrfelt, R.; Klargaard, S.K.; Petersen, A.; Gerlach, C. Reading in Developmental Prosopagnosia: Evidence for a Dissociation Between Word and Face Recognition. Neuropsychology 2018, 32, 138–147. [Google Scholar] [CrossRef] [Green Version]
- Gerlach, C.; Klargaard, S.K.; Starrfelt, R. On the relation between face and object recognition in developmental prosopagnosia: No dissociation but a systematic association. PLoS ONE 2016, 11, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Geskin, J.; Behrmann, M. Congenital prosopagnosia without object agnosia? A literature review. Cogn. Neuropsychol. 2018, 35, 4–54. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B.J.; Dewey, D.M.; Crawford, S.G.; Wilson, B.N. The Term Comorbidity Is of Questionable Value in Reference to Developmental Disorders: Data and Theory. J. Learn. Disabil. 2001, 34, 555–565. [Google Scholar] [CrossRef]
- Dewey, D. What Is Comorbidity and Why Does It Matter in Neurodevelopmental Disorders? Curr. Dev. Disord. Rep. 2018, 5, 235–242. [Google Scholar] [CrossRef]
- Ramus, F. Neurobiology of dyslexia: A reinterpretation of the data. Trends Neurosci. 2004, 27, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Carroll, J.M.; Maughan, B.; Goodman, R.; Meltzer, H. Literacy difficulties and psychiatric disorders: Evidence for comorbidity. J. Child Psychol. Psychiatry 2005, 46, 524–532. [Google Scholar] [CrossRef]
- Willcutt, E.G.; Pennington, B.F.; Olson, R.K.; Chhabildas, N.; Hulslander, J. Neuropsychological Analyses of Comorbidity Between Reading Disability and Attention Deficit Hyperactivity Disorder: In Search of the Common Deficit. Dev. Neuropsychol. 2005, 27, 35–78. [Google Scholar] [CrossRef]
- Klargaard, S.K.; Starrfelt, R.; Petersen, A.; Gerlach, C. Topographic processing in developmental prosopagnosia: Preserved perception but impaired memory of scenes. Cogn. Neuropsychol. 2016, 33, 405–413. [Google Scholar] [CrossRef]
- Sigurdardottir, H.M.; Fridriksdottir, L.E.; Gudjonsdottir, S.; Kristjánsson, Á. Specific problems in visual cognition of dyslexic readers: Face discrimination deficits predict dyslexia over and above discrimination of scrambled faces and novel objects. Cognition 2018, 175, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Carver, L.; Meltzoff, A.N.; Panagiotides, H.; McPartland, J.; Webb, S.J. Neural Correlates of Face and Object Recognition in Young Children with Autism Spectrum Disorder, Developmental Delay, and Typical Development. Child Dev. 2002, 73, 700–717. [Google Scholar] [CrossRef] [Green Version]
- Schultz, R.T. Developmental deficits in social perception in autism: The role of the amygdala and fusiform face area. Int. J. Dev. Neurosci. 2005, 23, 125–141. [Google Scholar] [CrossRef]
- Suri, K.; Lewis, M.; Minar, N.; Willson, E.; Ace, J. Face memory deficits in children and adolescents with autism spectrum disorder. J. Psychopathol. Behav. Assess 2021, 43, 108–118. [Google Scholar] [CrossRef]
- Duchaine, B.; Nakayama, K. The Cambridge Face Memory Test: Results for neurologically intact individuals and an investigation of its validity using inverted face stimuli and prosopagnosic participants. Neuropsychologia 2006, 44, 576–585. [Google Scholar] [CrossRef]
- Corrow, S.L.; Stubbs, J.L.; Schlaug, G.; Buss, S.; Paquette, S.; Duchaine, B.; Barton, J.J.S. Perception of musical pitch in developmental prosopagnosia. Neuropsychologia 2019, 124, 87–97. [Google Scholar] [CrossRef]
- Garrido, L.; Furl, N.; Draganski, B.; Weiskopf, N.; Stevens, J.; Tan, G.C.-Y.; Driver, J.; Dolan, R.J.; Duchaine, B. Voxel-based morphometry reveals reduced grey matter volume in the temporal cortex of developmental prosopagnosics. Brain 2009, 132, 3443–3455. [Google Scholar] [CrossRef]
- Bate, S.; Cook, S.J.; Duchaine, B.; Tree, J.J.; Burns, E.J.; Hodgson, T.L. Intranasal inhalation of oxytocin improves face processing in developmental prosopagnosia. Cortex 2014, 50, 55–63. [Google Scholar] [CrossRef] [Green Version]
- McIntosh, R.D. Exploratory reports: A new article type for Cortex. Cortex 2017, 96, A1–A4. [Google Scholar] [CrossRef] [Green Version]
- Moreau, D.; Wilson, A.J.; McKay, N.S.; Nihill, K.; Waldie, K.E. No evidence for systematic white matter correlates of dyslexia and dyscalculia. Neuroimage Clin. 2018, 18, 356–366. [Google Scholar] [CrossRef]
- Colorafi, K.J.; Evans, B. Qualitative Descriptive Methods in Health Science Research. HERD Health Environ. Res. Des. J. 2016, 9, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Arizpe, J.M.; Saad, E.; Douglas, A.O.; Germine, L.; Wilmer, J.B.; DeGutis, J.M. Self-reported face recognition is highly valid, but alone is not highly discriminative of prosopagnosia-level performance on objective assessments. Behav. Res. Methods 2019, 51, 1102–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duchaine, B.; Yovel, G. 2.21.4.2—Developmental Prosopagnosia. In The Senses: A Comprehensive Reference; Masland, R.H., Albright, T.D., Albright, T.D., Masland, R.H., Dallos, P., Oertel, D., Firestein, S., Beauchamp, G.K., Catherine Bushnell, M., Basbaum, A.I., et al., Eds.; Academic Press: New York, NY, USA, 2008; pp. 345–347. [Google Scholar]
- Grueter, M.; Grueter, T.; Bell, V.; Horst, J.; Laskowski, W.; Sperling, K.; Halligan, P.W.; Elli, H.D.; Kennerknecht, I. Hereditary Prosopagnosia: The First Case Series. Cortex 2007, 43, 734–749. [Google Scholar] [CrossRef]
- Corrow, J.C.; Corrow, S.; Lee, E.; Pancaroglu, R.; Burles, F.; Duchaine, B.; Iaria, G.; Barton, J. Getting lost: Topographic skills in acquired and developmental prosopagnosia. Cortex 2016, 76, 89–103. [Google Scholar] [CrossRef] [Green Version]
- Collins, E.; Dundas, E.; Gabay, Y.; Plaut, D.C.; Behrmann, M. Hemispheric organization in disorders of development. Vis. Cogn. 2017, 25, 416–429. [Google Scholar] [CrossRef]
- Gabay, Y.; Dundas, E.; Plaut, D.; Behrmann, M. Atypical perceptual processing of faces in developmental dyslexia. Brain Lang. 2017, 173, 41–51. [Google Scholar] [CrossRef]
- Sigurdardottir, H.M.; Ívarsson, E.; Kristinsdóttir, K.; Kristjánsson, Á. Impaired Recognition of Faces and Objects in Dyslexia: Evidence for Ventral Stream Dysfunction? Neuropsychology 2015, 29, 739–750. [Google Scholar] [CrossRef] [Green Version]
- Tarkiainen, A.; Helenius, P.; Salmelin, R. Category-specific occipitotemporal activation during face perception in dyslexic individuals: An MEG study. NeuroImage 2003, 19, 1194–1204. [Google Scholar] [CrossRef]
- Kühn, C.D.; Gerlach, C.; Andersen, K.B.; Poulsen, M.; Starrfelt, R. Face recognition in developmental dyslexia: Evidence for dissociation between faces and words. Cogn. Neuropsychol. 2021, 38, 107–115. [Google Scholar] [CrossRef]
- Wilson, A.J.; Andrewes, S.G.; Struthers, H.; Rowe, V.M.; Bogdanovic, R.; Waldie, K.E. Dyscalculia and dyslexia in adults: Cognitive bases of comorbidity. Learn. Individ. Differ. 2015, 37, 118–132. [Google Scholar] [CrossRef]
- Landerl, K.; Moll, K. Comorbidity of learning disorders: Prevalence and familial transmission. J. Child Psychol. Psychiatry 2010, 51, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Moreau, D.; Wiebels, K.; Wilson, A.J.; Waldie, K.E. Volumetric and surface characteristics of gray matter in adult dyslexia and dyscalculia. Neuropsychologia 2019, 127, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Esins, J.; Schultz, J.; Bülthoff, I.; Kennerknecht, I. Galactose uncovers face recognition and mental images in congenital prosopagnosia: The first case report. Nutr. Neurosci. 2014, 17, 239–240. [Google Scholar] [CrossRef] [Green Version]
- Ulimoen, T.K.; Sørensen, T.A. Is Grapheme Colour Synesthesia linked to Prosopagnosia? J. Vis. 2019, 19, 24b. [Google Scholar] [CrossRef]
- Sørensen, T.A. Performance in face perception task is decreased in observers with colour-grapheme synaesthesia. In Proceedings of the Synaesthesia in Perspective: Development, Networks, and Multisensory Processing, Hamburg, Germany, 2014; Universitätsklinikum Hamburg-Eppendorf: Hamburg, Germany, 2014. [Google Scholar]
- Mulvenna, C. Synesthesia and Creativity. In Oxford Handbook of Synesthesia; Simmer, J., Hubbard, S., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 1–27. [Google Scholar]
- Rothen, N.; Meier, B.; Ward, J. Enhanced memory ability: Insights from synaesthesia. Neurosci. Biobehav. Rev. 2012, 36, 1952–1963. [Google Scholar] [CrossRef]
- Bate, S.; Bennetts, R.J.; Gregory, N.; Tree, J.J.; Murray, E.; Adams, A.; Bobak, A.K.; Penton, T.; Yang, T.; Banissy, M.J. Objective Patterns of Face Recognition Deficits in 165 Adults with Self-Reported Developmental Prosopagnosia. Brain Sci. 2019, 9, 133. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, P.I.N.; Wilkinson, D.T.; Ferguson, H.J.; Smith, L.J.; Bindemann, M.; Johnston, R.A.; Schmalzl, L. Perceptual and Memorial Contributions to Developmental Prosopagnosia. Q. J. Exp. Psychol. 2017, 70, 298–315. [Google Scholar] [CrossRef]
- Tree, J.J.; Wilkie, J. Face and object imagery in congenital prosopagnosia: A case series. Cortex 2010, 46, 1189–1198. [Google Scholar] [CrossRef]
- Grüter, T.; Grüter, M.; Bell, V.; Carbon, C.-C. Visual mental imagery in congenital prosopagnosia. Neurosci. Lett. 2009, 453, 135–140. [Google Scholar] [CrossRef]
- Zeman, A.; Dewar, M.; Della Sala, S. Lives without imagery—Congenital aphantasia. Cortex 2015, 73, 378–380. [Google Scholar] [CrossRef] [Green Version]
- Palombo, D.J.; Alain, C.; Söderlund, H.; Khuu, W.; Levine, B. Severely deficient autobiographical memory (SDAM) in healthy adults: A new mnemonic syndrome. Neuropsychologia 2015, 72, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Norton, D.; Ongur, D.; Heckers, S. Inefficient Face Detection in Schizophrenia. Schizophr. Bull. 2007, 34, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belge, J.-B.; Maurage, P.; Mangelinckx, C.; Leleux, D.; Delatte, B.; Constant, E. Facial decoding in schizophrenia is underpinned by basic visual processing impairments. Psychiatry Res. 2017, 255, 167–172. [Google Scholar] [CrossRef]
- SurveyXact By Ramboll. Available online: https://www.surveyxact.dk/ (accessed on 14 December 2021).
- World Medical Association (WMA). World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guterbock, T.M.; Marcopulos, B.A. Survey methods for neuropsychologists: A review of typical methodological pitfalls and suggested solutions. Clin. Neuropsychol. 2020, 34, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Gaule, A.; Sowden, S.; Bird, G.; Cook, R. The 20-item prosopagnosia index (PI20): A self-report instrument for identifying developmental prosopagnosia. R. Soc. Open Sci. 2015, 2, 140343. [Google Scholar] [CrossRef] [Green Version]
- Claessen, M.H.G.; Visser-Meily, J.M.A.; de Rooij, N.K.; Postma, A.; van der Ham, I.J.M. The Wayfinding Questionnaire as a Self-report Screening Instrument for Navigation-related Complaints After Stroke: Internal Validity in Healthy Respondents and Chronic Mild Stroke Patients. Arch. Clin. Neuropsychol. 2016, 31, 839–854. [Google Scholar] [CrossRef] [Green Version]
- de Rooij, N.K.; Claessen, M.H.G.; van der Ham, I.J.M.; Post, M.W.M.; Visser-Meily, J.M.A. The Wayfinding Questionnaire: A clinically useful self-report instrument to identify navigation complaints in stroke patients. Neuropsychol. Rehabil. 2019, 29, 1042–1061. [Google Scholar] [CrossRef]
- Gregory, R.J. Chapter 4 VALIDITY AND TEST CONSTRUCTION. In Psychological Testing: History, Principles, and Applications; Gregory, R.J., Ed.; Pearson Education: Essex, UK, 2014; pp. 118–153. [Google Scholar]
- Rice, G.E.; Kerry, S.J.; Robotham, R.J.; Leff, A.; Ralph, M.L.; Starrfelt, R. Category-selective deficits are the exception and not the rule: Evidence from a case-series of 64 patients with ventral occipito-temporal cortex damage. Cortex 2020, 138, 266–281. [Google Scholar] [CrossRef]
- Lefly, D.L.; Pennington, B.F. Reliability and validity of the Adult Reading History Questionnaire. J. Learn. Disabil. 2000, 33, 286–296. [Google Scholar] [CrossRef]
- Susilo, T.; Duchaine, B. Advances in developmental prosopagnosia research. Curr. Opin. Neurobiol. 2013, 23, 423–429. [Google Scholar] [CrossRef]
- Gerlach, C.; Klargaard, S.K.; Alnæs, D.; Kolskår, K.K.; Karstoft, J.; Westlye, L.T.; Starrfelt, R. Left hemisphere abnormalities in developmental prosopagnosia when looking at faces but not words. Brain Commun. 2019, 1, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bjornsdottir, G.; Halldorsson, J.G.; Steinberg, S.; Hansdottir, I.; Kristjansson, K.; Stefansson, H.; Stefansson, K. The Adult Reading History Questionnaire (ARHQ) in Icelandic: Psychometric Properties and Factor Structure. J. Learn. Disabil. 2014, 47, 532–542. [Google Scholar] [CrossRef]
- Schelke, M.W.; Shapiro, S.D.; Hackett, K.; Chen, J.; Simchon-Steinhof, S.; Ganzer, C.A.; Isaacson, R.S.; Tamboer, P.; Van Vliet, E.; Assuras, S.; et al. Diagnosis of developmental learning and attention disorders in adults: A review of clinical modalities. Neurol. Psychiatry Brain Res. 2017, 23, 27–35. [Google Scholar] [CrossRef]
- Butterworth, B. Personal communication. 26 March. 2020.
- Willcutt, E.G.; Boada, R.; Riddle, M.W.; Chhabildas, N.; DeFries, J.C.; Pennington, B.F. Colorado Learning Difficulties Questionnaire: Validation of a parent-report screening measure. Psychol. Assess. 2011, 23, 778–791. [Google Scholar] [CrossRef] [Green Version]
- Barbaresi, W.J.; Katusic, S.K.; Colligan, R.C.; Weaver, A.L.; Jacobsen, S.J. Math Learning Disorder: Incidence in a Population-Based Birth Cohort, 1976–1982, Rochester, Minn. Ambul. Pediatrics 2005, 5, 281–289. [Google Scholar] [CrossRef]
- Butterworth, B.; Varma, S.; Laurillard, D. Dyscalculia: From Brain to Education. Science 2011, 332, 1049–1053. [Google Scholar] [CrossRef] [Green Version]
- De Visscher, A.; Noël, M.-P.; Pesenti, M.; Dormal, V. Developmental dyscalculia in adults: Beyond numerical magnitude impairment. J. Learn. Disabil. 2018, 51, 600–611. [Google Scholar] [CrossRef]
- Popping, R. Analyzing Open-ended Questions by Means of Text Analysis Procedures. Bull. Méthodol. Sociol. 2015, 128, 23–39. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Macintosh, 27; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- McHugh, M.L. The chi-square test of independence. Biochem. Med. 2013, 23, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-Y. Statistical notes for clinical researchers: Chi-squared test and Fisher’s exact test. Restor. Dent. Endod. 2017, 42, 152–155. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Wegener, D.T.; Maccallum, R.C.; Strahan, E.J. Evaluating the Use of Exploratory Factor Analysis in Psychological Research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Schmitt, T.A. Current Methodological Considerations in Exploratory and Confirmatory Factor Analysis. J. Psychoeduc. Assess. 2011, 29, 304–321. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. Data Distribution. In A Primer on Partial Least Squares Structural Squation Modeling (PLS-SEM), 2nd ed.; Hair, J.F., Ed.; Sage: Los Angeles, CA, USA, 2017; pp. 60–62. [Google Scholar]
- Costello, A.B.; Osborne, J.W. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Principal Components and Factor Analysis. In Using Multivariate Statistics: Pearson New International Edition, 6th ed.; Pearson Education Limited: Essex, UK, 2013; pp. 660–713. [Google Scholar]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- NVivo Qualitative Data Analysis Software; Version 12.6; QSR International Pty Ltd.: Doncaster, VIC, Australia, 2019.
- Yong, A.G.; Pearce, S. A Beginner’s Guide to Factor Analysis: Focusing on Exploratory Factor Analysis. Quant. Methods Psychol. 2013, 9, 79–94. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development: Theory and Applications, 4th ed.; Sage: Los Angeles, CA, USA, 2017. [Google Scholar]
- Ventura, P.; Livingston, L.A.; Shah, P. Adults have moderate-to-good insight into their face recognition ability: Further validation of the 20-item Prosopagnosia Index in a Portuguese sample. Q. J. Exp. Psychol. 2018, 71, 2677–2679. [Google Scholar] [CrossRef] [Green Version]
- DuPaul, G.J.; Weyandt, L.L.; O’Dell, S.M.; Varejao, M. College Students With ADHD:Current Status and Future Directions. J. Atten. Disord. 2009, 13, 234–250. [Google Scholar] [CrossRef]
- Watkins, N.W. (A)phantasia and severely deficient autobiographical memory: Scientific and personal perspectives. Cortex 2018, 105, 41–52. [Google Scholar] [CrossRef]
- Zeman, A.; Milton, F.; Della Sala, S.; Dewar, M.; Frayling, T.; Gaddum, J.; Hattersley, A.; Heuerman-Williamson, B.; Jones, K.; MacKisack, M.; et al. Phantasia—The psychological significance of lifelong visual imagery vividness extremes. Cortex 2020, 130, 426–440. [Google Scholar] [CrossRef]
- Paquette, S.; Li, H.C.; Corrow, S.L.; Buss, S.S.; Barton, J.J.S.; Schlaug, G. Developmental Perceptual Impairments: Cases When Tone-Deafness and Prosopagnosia Co-occur. Front. Hum. Neurosci. 2018, 12, 1–6. [Google Scholar] [CrossRef]
- Iaria, G.; Barton, J.J.S. Developmental topographical disorientation: A newly discovered cognitive disorder. Exp. Brain Res. 2010, 206, 189–196. [Google Scholar] [CrossRef]
- Susilo, T. The face specificity of lifelong prosopagnosia. Cogn. Neuropsychol. 2018, 35, 1–3. [Google Scholar] [CrossRef] [Green Version]
- De Haan, E.H.; Campbell, R. A fifteen year follow-up of a case of developmental prosopagnosia. Cortex 1991, 27, 489–509. [Google Scholar] [CrossRef]
- Johnen, A.; Schmukle, S.C.; Hüttenbrink, J.; Kischka, C.; Kennerknecht, I.; Dobel, C. A family at risk: Congenital prosopagnosia, poor face recognition and visuoperceptual deficits within one family. Neuropsychologia 2014, 58, 52–63. [Google Scholar] [CrossRef]
- Gauthier, I.; Behrmann, M.; Tarr, M.J. Can face recognition really be dissociated from object recognition? J. Cogn. Neurosci. 1999, 11, 349–370. [Google Scholar] [CrossRef]
- Gerlach, C.; Starrfelt, R. Patterns of perceptual performance in developmental prosopagnosia: An in-depth case series. Cogn. Neuropsychol. 2021, 38, 27–49. [Google Scholar] [CrossRef]
- Duchaine, B.C.; Nakayama, K. Developmental prosopagnosia: A window to content-specific face processing. Curr. Opin. Neurobiol. 2006, 16, 166–173. [Google Scholar] [CrossRef]
- Kimchi, R.; Behrmann, M.; Avidan, G.; Amishav, R. Perceptual separability of featural and configural information in congenital prosopagnosia. Cogn. Neuropsychol. 2012, 29, 447–463. [Google Scholar] [CrossRef]
- Stollhoff, R.; Jost, J.; Elze, T.; Kennerknecht, I. Deficits in Long-Term Recognition Memory Reveal Dissociated Subtypes in Congenital Prosopagnosia. PLoS ONE 2011, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Li, J.; Liu, X.; Song, Y.; Wang, R.; Yang, Z.; Liu, J. Altered spontaneous neural activity in the occipital face area reflects behavioral deficits in developmental prosopagnosia. Neuropsychologia 2016, 89, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Jiahui, G.; Yang, H.; Duchaine, B. Developmental prosopagnosics have widespread selectivity reductions across category-selective visual cortex. Proc. Natl. Acad. Sci. USA 2018, 115, E6418–E6427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaywitz, S.E.M.D. Dyslexia. N. Engl. J. Med. 1998, 338, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Shaywitz, S.E.; Shaywitz, B.A.; Fletcher, J.M.; Escobar, M.D. Prevalence of reading disability in boys and girls. Results of the Connecticut Longitudinal Study. JAMA 1990, 264, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Chen, Y.; Hu, X.; Guo, Y.; Zhao, X.; Sun, T.; Wu, Y.; Li, X. An Epidemiological Study of Chinese Children with Developmental Dyslexia. J. Dev. Behav. Pediatr. 2020, 41, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Simner, J.; Mulvenna, C.; Sagiv, N.; Tsakanikos, E.; Witherby, S.A.; Fraser, C.; Scott, K.; Ward, J. Synaesthesia: The Prevalence of Atypical Cross-Modal Experiences. Perception 2006, 35, 1024–1033. [Google Scholar] [CrossRef] [Green Version]
- Watson, M.R.; Akins, K.A.; Spiker, C.; Crawford, L.; Enns, J.T. Synesthesia and learning: A critical review and novel theory. Front. Hum. Neurosci. 2014, 8, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Maurer, D.; Ghloum, J.K.; Gibson, L.C.; Watson, M.R.; Chen, L.M.; Akins, K.; Enns, J.T.; Hensch, T.K.; Werker, J.F. Reduced perceptual narrowing in synesthesia. Proc. Natl. Acad. Sci. USA 2020, 117, 10089–10096. [Google Scholar] [CrossRef]
- Palermo, R.; Rossion, B.; Rhodes, G.; Laguesse, R.; Tez, T.; Hall, B.; Albonico, A.; Malaspina, M.; Daini, R.; Irons, J.; et al. Do People Have Insight into their Face Recognition Abilities? Q. J. Exp. Psychol. 2017, 70, 218–233. [Google Scholar] [CrossRef]
- Zell, E.; Krizan, Z. Do People Have Insight Into Their Abilities? A Metasynthesis. Perspect. Psychol. Sci. 2014, 9, 111–125. [Google Scholar] [CrossRef] [Green Version]
- Murray, E.; Bate, S. Self-ratings of face recognition ability are influenced by gender but not prosopagnosia severity. Psychol. Assess. 2019, 31, 828–832. [Google Scholar] [CrossRef]
- Livingston, L.A.; Shah, P. People with and without prosopagnosia have insight into their face recognition ability. Q. J. Exp. Psychol. 2017, 71, 1260–1262. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.; Sowden, S.; Gaule, A.; Catmur, C.; Bird, G. The 20 item prosopagnosia index (PI20): Relationship with the Glasgow face-matching test. R. Soc. Open Sci. 2015, 2, 150305. [Google Scholar] [CrossRef] [Green Version]
- Gray, K.L.H.; Bird, G.; Cook, R. Robust associations between the 20-item prosopagnosia index and the Cambridge Face Memory Test in the general population. R. Soc. Open Sci. 2017, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Tsantani, M.; Vestner, T.; Cook, R. The Twenty Item Prosopagnosia Index (PI20) provides meaningful evidence of face recognition impairment. R. Soc. Open Sci. 2021, 8, 202062. [Google Scholar] [CrossRef]
- Fields, R.D. White matter in learning, cognition and psychiatric disorders. Trends Neurosci. 2008, 31, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Groves, R.M.; Presser, S.; Dipko, S. The Role of Topic Interest in Survey Participation Decisions. Public Opin. Q. 2004, 68, 2–31. [Google Scholar] [CrossRef] [Green Version]
- Rubenstein, E.; Furnier, S.J.A.i.A. # Bias: The opportunities and challenges of surveys that recruit and collect data of autistic adults online. Autism Adulthood 2021, 3, 120–128. [Google Scholar]
- Maccallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample Size in Factor Analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- de Winter, J.C.F.; Dodou, D.; Wieringa, P.A. Exploratory Factor Analysis With Small Sample Sizes. Multivar. Behav. Res. 2009, 44, 147–181. [Google Scholar] [CrossRef]
- Astle, D.E.; Fletcher-Watson, S. Beyond the Core-Deficit Hypothesis in Developmental Disorders. Curr. Dir. Psychol. Sci. 2020, 29, 431–437. [Google Scholar] [CrossRef]
- Siugzdaite, R.; Bathelt, J.; Holmes, J.; Astle, D.E. Transdiagnostic Brain Mapping in Developmental Disorders. Curr. Biol. 2020, 30, 1245–1257.e1244. [Google Scholar] [CrossRef]

{kind=link}
| Age in Years | n (%) |
|---|---|
| 18–24 | 2 (1.7) |
| 25–34 | 18 (15.7) |
| 35–44 | 38 (33.0) |
| 45–54 | 23 (20.0) |
| 55–64 | 18 (15.7) |
| 65–74 | 14 (12.2) |
| ≥75 | 2 (1.7) |
| Total | 115 (100.0) |
| Demographics | n (%) |
|---|---|
| DP diagnosis * | 34 (29.6) |
| English as first language | 77 (67.0) |
| Handedness (left/right/ambidextrous) | 10/99/6 (8.7/86.1/5.2) |
| Self-Reported Developmental Comorbidity | n (%) |
|---|---|
| Presence of at least one developmental comorbidity a | 65 (56.5) |
| Dyslexia | 4 (3.5) |
| Dyscalculia | 4 (3.5) |
| ADHD | 7 (6.1) |
| Aphantasia | 24 (20.9) |
| Synesthesia | 12 (10.4) |
| Object agnosia | 29 (25.2) |
| Memory problems | 27 (23.5) |
| Presence of not-predefined mental, cognitive or intellectual disorder b | 13 (11.3) |
| Presence of not-predefined conditions related to vision b | 2 (1.7) |
| Presence of not-predefined somatic disorder b | 2 (1.7) |
| Navigation problems * | 29 (25.2) |
| Number of Developmental Comorbidities * | n (%) |
|---|---|
| 0 | 50 (43.5) |
| 1 | 34 (29.6) |
| 2 | 22 (19.1) |
| 3 | 8 (7.0) |
| 5 | 1 (0.9) |
| Total | 115 (100.0) |
| Severity Group Based on PI20 | Number of Cases Reporting Developmental Comorbidity (% of Subsample) |
|---|---|
| Mild DP (n = 15) | 9 (60.0) |
| Moderate DP (n = 42) | 22 (52.4) |
| Severe DP (n = 58) | 34 (58.6) |
| Difficulties and Abilities in Developmental Prosopagnosia Questionnaire Items | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| PI1. My face recognition is worse than most people | 0.456 | −0.173 | −0.165 | |
| PI2. I have always had a bad memory for faces | 0.289 | 0.165 | ||
| PI3. I find it noticeably easier to recognize people who have distinctive facial features | −00.331 | |||
| PI4. I often mistake people I have met before for strangers | 0.430 | |||
| PI5. When I was at school I struggled to recognize my classmates | 0.653 | 0.173 | 0.106 | |
| PI6. When people change their hairstyle, or wear hats, I have problems recognizing them | 0.478 | −0.196 | ||
| PI7. I sometimes have to warn new people I meet that I am ‘bad with faces’ | 0.411 | |||
| PI8. I find it easy to picture individual faces in my mind | 0.154 | −0.160 | ||
| PI9. I am better than most people at putting a ‘name to a face’ | 0.152 | |||
| PI10. Without hearing people’s voices, I struggle to recognize them | 0.548 | 0.115 | ||
| PI11. Anxiety about face recognition has led me to avoid certain social or professional situations | 0.377 | 0.183 | ||
| PI12. I have to try harder than other people to memorize faces | 0.141 | −0.330 | ||
| PI13. I am very confident in my ability to recognize myself in photographs | 0450 | 0.171 | ||
| PI14. I sometimes find movies hard to follow because of difficulties recognizing characters | 0.371 | 0.209 | −0.166 | |
| PI15. My friends and family think I have bad face recognition or bad face memory | 0.472 | −0.141 | ||
| PI16. I feel like I frequently offend by not recognizing who they are | 0.549 | −0.141 | ||
| PI17. It is easy for me to recognize individuals in situations that require people to wear similar clothes (e.g.,suits, uniforms, swimwear) | 0.464 | −0.315 | −0.102 | |
| PI18. At family gatherings, I sometimes confuse individual family members | 0.553 | |||
| PI19. I find it easy to recognize celebrities in ‘before-they-were-famous’ photos, even if they have changed considerably | 0.149 | −0.182 | −0.326 | |
| PI20. It is hard to recognize familiar people when I meet them out of context (e.g.,meeting a work colleague unexpectedly while shopping) | 0.646 | 0.199 | ||
| WQ1. I am good at understanding and following route descriptions | −0.801 | −0.124 | ||
| WQ2. I can always orient myself quickly and correctly when I am in an unknown environment | −0.967 | |||
| WQ3. I can easily find the shortest route to a known destination | −0.911 | |||
| WQ4. I can usually recall a new route after I have walked it once | −0.853 | −0.102 | ||
| WQ5. When I am in a building for the first time, I can easily point to the entrance of this building. | −0.862 | |||
| ARHQ1. How much extra help did you need when learning to read in elementary school? | 0.767 | |||
| ARHQ2. How would you compare your reading skill to that of others in your elementary classes? | −0.140 | 0.744 | ||
| ARHQ3. How much difficulty did you have learning to spell in elementary school? | 0.166 | 0.695 | 0.159 | |
| ARHQ4. How much difficulty did you have learning to read in elementary school? | 0.829 | |||
| ARHQ5. How would you compare your current reading speed to that of others of the same age and education? | 0.171 | 0.558 | −0.120 | |
| MATH1. As a child, did you make careless errors in math, such as adding when the sign indicated subtraction? | 0.156 | 0.108 | 0.779 | |
| MATH2. As a child, did you have trouble learning new math concepts? | 0.128 | 0.816 | ||
| MATH3. Do you have difficulties estimating quantities, e.g., how many coins are lying on a table? | 0.194 | 0.653 |
| Difficulties Codes | Nb | Quote | Strengths Codes | Nb | Quote |
|---|---|---|---|---|---|
| Aphantasia | 24 | ‘I am not very good at visualizing things in my head. I’ve explained that it’s more like when I picture something in my mind, it looks kind of like a Lite Brite toy. With just like colored outlines of things. So imagining The beach, it’s just a yellow line for the sand, some blue blur for the ocean, and an outlined yellow sun. Like a kid drawing.’ | Good Visual Mental Imagery | 7 | ‘I have a very strong visual imagination. I can create whole worlds full of detail in my imagination.’ |
| Difficulties with Math | 27 | ‘I think I have some dyscalculia. I will transpose numbers even though I am trying to be careful and can do this even in a short string of only 3 numbers. However I don’t have trouble with mathematical concepts or at least not up to the usual school leaver level.’ | Mathematical Abilities | 20 | ‘I am better at math than most people. I enjoy math and I’m good at it. Even when I don’t “feel” like I fully understand it, I perform well on math/stats tests.’ |
| Reading and Spelling Difficulties | 8 | ‘Learning a new language is impossible (I live in Indonesia for 23 years). Very slow reader, I easily forget what I have read.’ | Reading and Spelling Abilities | 39 | ‘I’m a very good reader, writer, editor, and proofreader.’ |
| Memory Problems | 21 | ‘I have a terrible memory. I feel like I barely remember anything prior to highschool and I am only 29 years old. Even then things are very foggy. I only remember things if I see them in a photograph.’ | Good Memory | 40 | ‘Far above average skilled in remembering fun facts and historical events. Very good memory in order of recalling details of what’s happened in my own life.’ |
| Object Agnosia | 7 | ‘I’m ‘car-blind’, and had to memorize my parents’ license plates as a child.’ | |||
| Synesthesia | 2 | ‘See colours when listening to music’ | |||
| Lack of Musicality | 17 | ‘Very tone deaf- measures by up to 2 full notes by a music teacher.’ | Musicality | 26 | ‘I can hear something once and play it on the piano.’ |
| Difficulties with Sports | 17 | ‘I am a disaster when it comes to sports or athletics, especially team sports. Partially this is due to my lack of coordination and skill, and partially because I never knew who to pass the ball to!’ | Sports Skills | 12 | ‘I was a highly competitive gymnast for 14 years. I have very good body awareness.’ |
| Motor Coordination and Body–Space Perception | 10 | ‘I’m clumsy, can’t catch or throw, and miss judge and catch the edges of things when walking.’ | |||
| Problems with Inattentiveness, Impulsivity, or Hyperactivity | 2 | ‘Need more time on tasks, partly because I want to be thorough and am afraid of doing mistakes, partly because of lack of routines. Bad at routines and “what to do next”. Easy to distract. “Colour codes” on buttons etc. doesn’t help me, seems like I don’t notice them (I have normal colour vision).’ | |||
| Social and Interpersonal Skills | 12 | ‘Knowing what other people feel, and why they feel it. “intuitive profiling” so to say’ | |||
| Skills in Visual Arts | 12 | ‘I am very artistic. I have shown my work and been featured in a variety of mediums throughout my whole life. Most specifically I paint faces and have since I was about 12 years old and was fascinated with faces.’ | |||
| Navigation Problems | 41 | ‘I am terrible at navigation. Even in a mid-sized town (100,000 people) I have lived for 20 years, I still get lost. I have no clue which is N, S, E, W.’ | Navigation Abilities | 13 | ‘Maps, geography.’ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Svart, N.; Starrfelt, R. Is It Just Face Blindness? Exploring Developmental Comorbidity in Individuals with Self-Reported Developmental Prosopagnosia. Brain Sci. 2022, 12, 230. https://doi.org/10.3390/brainsci12020230
Svart N, Starrfelt R. Is It Just Face Blindness? Exploring Developmental Comorbidity in Individuals with Self-Reported Developmental Prosopagnosia. Brain Sciences. 2022; 12(2):230. https://doi.org/10.3390/brainsci12020230
Chicago/Turabian StyleSvart, Nanna, and Randi Starrfelt. 2022. "Is It Just Face Blindness? Exploring Developmental Comorbidity in Individuals with Self-Reported Developmental Prosopagnosia" Brain Sciences 12, no. 2: 230. https://doi.org/10.3390/brainsci12020230
APA StyleSvart, N., & Starrfelt, R. (2022). Is It Just Face Blindness? Exploring Developmental Comorbidity in Individuals with Self-Reported Developmental Prosopagnosia. Brain Sciences, 12(2), 230. https://doi.org/10.3390/brainsci12020230