
The Clinical Profile of Cat-Scratch Disease’s Neuro-Ophthalmological Effects

 ,
, 
 ,
,
Abstract
1. Introduction
2. Transmission Agent
3. Presentation in Clinical Practice
4. Immunopathology
5. Neurotropism
6. Neurologic Manifestations
6.1. Encephalopathy
6.2. Encephalitis
6.3. Other Neurological Manifestations
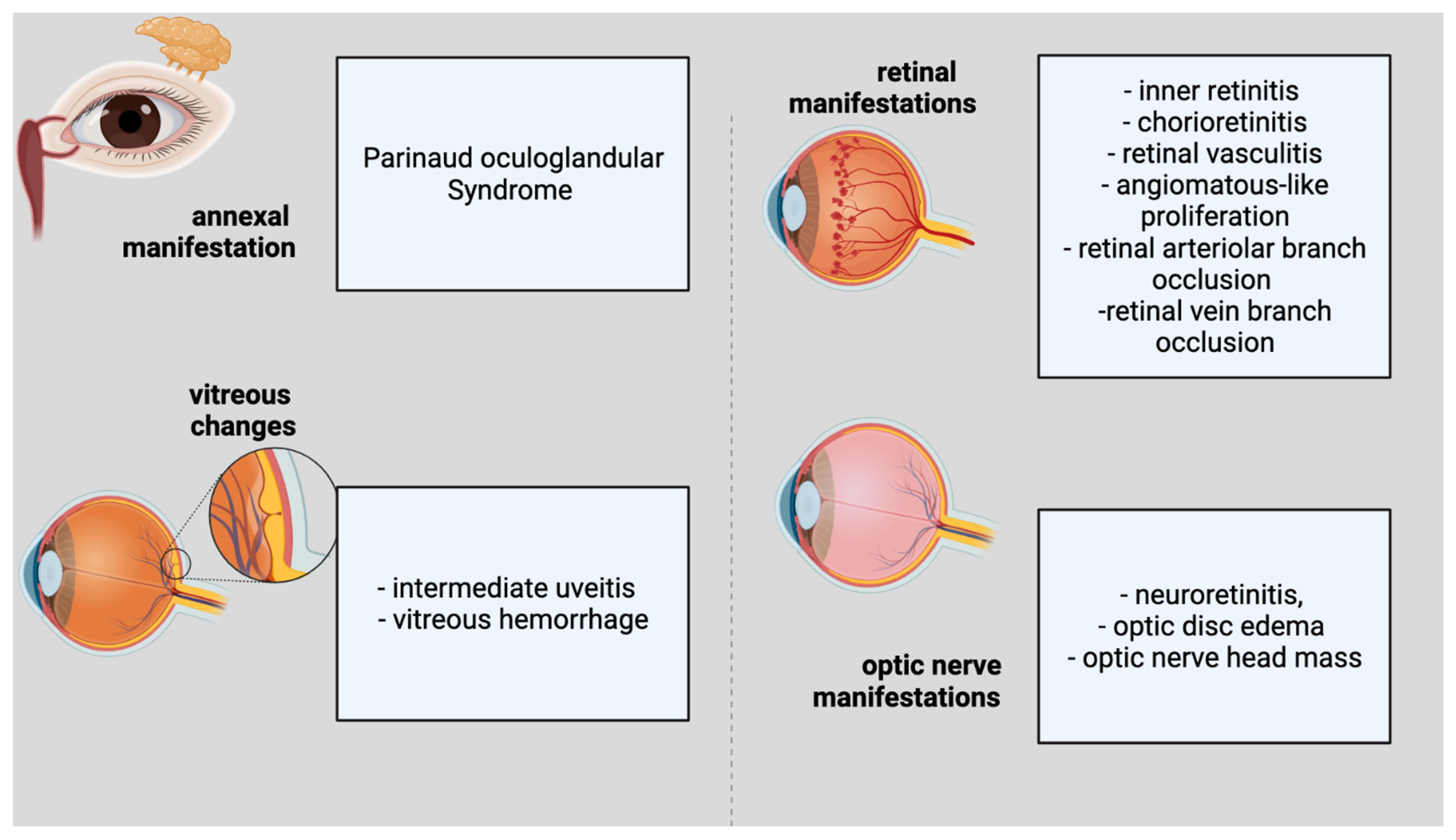
7. Ocular Manifestations
Neuroretinitis
8. Therapy

{kind=link}
| Author | Site of Lesion | Treatment | Dosage | Time | |
|---|---|---|---|---|---|
| Antibiotics | Corticoids | ||||
| Lee et al. [167] | Nodule of the upper lid | Topical gentamicin and systemic erythromycin | - | N/A | N/A |
| Kodoma et al. [170] | Neuroretinitis | 14 patients: Antibiotics: ciprofloxacin, doxycycline, sulfamethoxazole, erythromycin or cephems | 14 patients: prednisolone, betamethasone, methylprednisolone | N/A | N/A |
| Garcia Garcia et al. [13] | Parotid gland abscess and aseptic meningitis | Doxycycline and rifampicin | - | N/A | Two weeks |
| Canneti et al. [171] | Thirty-nine CSD patients | 31 patients (8 patients with neurologic manifestations of CSD) | 2 patients with neurologic manifestations of CSD | N/A | N/A |
| Bejarano et al. [172] | encephalopathy | Clarithromycin (5 days), cefotaxime (3 days), Meropenem (2 days), Vancomycin (2 days), Piperacillin-tazobactam (5 days), Azithromycin (134 days), rifampin (134 days) | - | Clarithromycin 15 mg/kg/day, cefotaxime 90 mg/kg/4 h, meropenem 40 mg/kg/8 h, vancomycin 10 mg/kg/6 h, piperacillin-tazobactam 80 mg–10 mg/kg/6 h, azithromycin 10 mg/kg/day | NA |
| Armengol et al. [97] | encephalopathy | Erythromycin | - | NA | 5 days |
| Fouch et al. [109] | encephalitis | Cephalexin | - | NA | 7 days |
| Balakrishnan et al. [101] | Vasculitis, cerebral infarction | Azithromycin Ceftriaxone | Azithromycin 500 mg Ceftriaxone 2 g | Azithromycin 8 weeks Ceftriaxone 8 weeks | |
| Cerpa et al. [124] | Encephalitis with convulsive status | Ciprofloxacin Cotrimoxazole Rifampicin Azithromycin | Ciprofloxacin 300 mg × 3/day Cotrimoxazole 110 mg × 3/day Rifampicin 450 mg Azithromycin 350 mg | Ciprofloxacin two weeks Cotrimoxazole two weeks Rifampicin 4 weeks Azithromycin 4 weeks | |
| Schuster et al. [102] | Neurologic CSD with hyperactivity | Doxycycline Rifampin | NA | 2 weeks | |
| Rosas et al. [176] | encephalitis associated with left arm flaccid paralysis | Doxycycline | 100 mg × 2/zi | 2 weeks | |
| Bilawsky et al. [179] | Neuroretinitis in pregnant woman | None | |||
| Celiker et al. [147] | Neuroretinitis in three patients | Doxycycline | NA | NA | |
| Raihan et al. [177] | Neuroretinitis in four patients | Azithromycin (3 cases) Doxycycline (1 case) | Azithromycin 250 mg Doxycycline 200 mg | Azithromycin 4–6 weeks Doxycycline 4 weeks | |
| Mutucumarana et al. [120] | VII-th nerve palsy | Azithromycin and rifampin | NA | 2 weeks | |
| Zakhour et al. [178] | Transverse myelitis and Guillain-Barré syndrome | Ceftriaxone, vancomycin, doxycycline | Ceftriaxone and vancomycin a few days; Doxycycline 2 weeks | ||
| Fouch et al. [109] | Disseminated Bartonella henselae | Cephalexin | NA | ||
| Farooque et al. [107] | Persistent focal seizures and encephalopathy | NA | 4 weeks | ||
| Pinto et al. [180] | aseptic meningitis and neuroretinitis | Azythromicin, Doxycicline, Rifampin | Azythromicin 500 mg; Doxycicline 100 mg; Rifampin 300 mg | Azythromicin a few days; Doxycicline and Rifampin a month | |
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Theel, E.S.; Ross, T. Seasonality of Bartonella henselae IgM and IgG antibody positivity rates. J. Clin. Microbiol. 2019, 57, e01263-19. [Google Scholar] [CrossRef] [PubMed]
- Klotz, S.A.; Ianas, V.; Elliott, S.P. Cat-scratch disease. Am. Fam. Physician 2011, 83, 152–155. [Google Scholar] [PubMed]
- Biancardi, A.L.; Curi, A.L.L. Cat-scratch disease. Ocul. Immunol. Inflamm. 2014, 22, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Florin, T.A.; Zaoutis, T.E.; Zaoutis, L.B. Beyond cat scratch disease: Widening spectrum of Bartonella henselae infection. Pediatrics 2008, 121, e1413–e1425. [Google Scholar] [CrossRef]
- Kordick, D.L.; Hilyard, E.J.; Hadfield, T.L.; Wilson, K.H.; Steigerwalt, A.G.; Brenner, D.J.; Breitschwerdt, E.B. Bartonella clarridgeiae, a newly recognized zoonotic pathogen causing inoculation papules, fever, and lymphadenopathy (cat scratch disease). J. Clin. Microbiol. 1997, 35, 1813–1818. [Google Scholar] [CrossRef]
- Zangwill, K.M. Cat scratch disease and other Bartonella infections. Adv. Exp. Med. Biol. 2013, 764, 159–166. [Google Scholar] [CrossRef]
- Foil, L.; Andress, E.; Freeland, R.L.; Roy, A.F.; Rutledge, R.; Triche, P.C.; O’Reilly, K.L. Experimental infection of domestic cats with Bartonella henselae by inoculation of Ctenocephalides felis (Siphonaptera: Pulicidae) feces. J. Med. Entomol. 1998, 35, 625–628. [Google Scholar] [CrossRef]
- Lamps, L.W.; Scott, M.A. Cat-scratch disease: Historic, clinical, and pathologic perspectives. Am. J. Clin. Pathol. 2004, 121, S71–S80. [Google Scholar] [CrossRef]
- Zangwill, K.M.; Hamilton, D.H.; Perkins, B.A.; Regnery, R.L.; Plikaytis, B.D.; Hadler, J.L.; Cartter, M.L.; Wenger, J.D. Cat scratch disease in Connecticut. Epidemiology, risk factors, and evaluation of a new diagnostic test. N. Engl. J. Med. 1993, 329, 8–13. [Google Scholar] [CrossRef]
- Jackson, L.A.; Perkins, B.A.; Wenger, J.D. Cat scratch disease in the United States: An analysis of three national databases. Am. J. Public Health 1993, 83, 1707–1711. [Google Scholar] [CrossRef]
- Nelson, C.A.; Saha, S.; Mead, P.S. Cat-scratch disease in the United States, 2005–2013. Emerg. Infect. Dis. 2016, 22, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- Pons, I.; Sanfeliu, I.; Cardeñosa, N.; Nogueras, M.M.; Font, B.; Segura, F. Serological evidence of Bartonella henselae infection in healthy people in Catalonia, Spain. Epidemiol. Infect. 2008, 136, 1712–1716. [Google Scholar] [CrossRef] [PubMed]
- García, J.C.; Núñez, M.J.; Castro, B.; Fernández, J.M.; Portillo, A.; Oteo, J.A. Hepatosplenic cat scratch disease in immunocompetent adults: Report of 3 cases and review of the literature. Medicine 2014, 93, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Gai, M.; d’Onofrio, G.; di Vico, M.C.; Ranghino, A.; Nappo, A.; Diena, D.; Novero, D.; Limerutti, G.; Messina, M.; Biancone, L. Cat-scratch disease: Case report and review of the literature. Transplant. Proc. 2015, 47, 2245–2247. [Google Scholar] [CrossRef]
- Regnery, R.L.; Childs, J.E.; Koehler, J.E. Infections associated with Bartonella species in persons infected with human immunodeficiency virus. Clin. Infect. Dis. 1995, 21 (Suppl. 1), S94–S98. [Google Scholar] [CrossRef]
- Kurbasic, M.; Jones, V.F.; Maxfield, C.M. Radiological case of the month. Atypical cat-scratch disease. Arch. Pediatr. Adolesc. Med. 1999, 153, 761–762. [Google Scholar] [CrossRef][Green Version]
- Anderson, B.; Lu, E.; Jones, D.; Regnery, R. Characterization of a 17-kilodalton antigen of Bartonella henselae reactive with sera from patients with cat scratch disease. J. Clin. Microbiol. 1995, 33, 2358–2365. [Google Scholar] [CrossRef]
- Kohler, J.E. Rochalzmaea henselae infection: A new zoonosis of the domestic cat as a reservoir. Pediatr. Infect. Dis. J. 1994, 13, 673. [Google Scholar] [CrossRef]
- Chomel, B.B.; Kasten, R.W.; Floyd-Hawkins, K.; Chi, B.; Yamamoto, K.; Roberts-Wilson, J.; Gurfield, A.N.; Abbott, R.C.; Pedersen, N.C.; Koehler, J.E. Experimental transmission of Bartonella henselae by the cat flea. J. Clin. Microbiol. 1996, 34, 1952–1956. [Google Scholar] [CrossRef]
- Nawrocki, C.C.; Max, R.J.; Marzec, N.S.; Nelson, C.A. Atypical manifestations of cat-scratch disease, United States, 2005–2014. Emerg. Infect. Dis. 2020, 26, 1438–1446. [Google Scholar] [CrossRef]
- Spach, D.H.; Koehler, J.E. Bartonella-associated infections. Infect. Dis. Clin. N. Am. 1998, 12, 137–155. [Google Scholar] [CrossRef]
- Angelakis, E.; Raoult, D. Pathogenicity and treatment of Bartonella infections. Int. J. Antimicrob. Agents 2014, 44, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A. Ocular complications of cat scratch disease. Br. J. Ophthalmol. 2020, 104, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Ormerod, L.D.; Dailey, J.P. Ocular manifestations of cat-scratch disease. Curr. Opin. Ophthalmol. 1999, 10, 209–216. [Google Scholar] [CrossRef]
- Windsor, J.J. Cat-scratch disease: Epidemiology, aetiology and treatment. Br. J. Biomed. Sci. 2001, 58, 101–110. [Google Scholar]
- Metzkor-Cotter, E.; Kletter, Y.; Avidor, B.; Varon, M.; Golan, Y.; Ephros, M.; Giladi, M. Long-term serological analysis and clinical follow-up of patients with cat scratch disease. Clin. Infect. Dis. 2003, 37, 1149–1154. [Google Scholar] [CrossRef]
- Jacomo, V.; Kelly, P.J.; Raoult, D. Natural History of Bartonella Infections (an Exception to Koch’s Postulate). Clin. Vaccine Immunol. 2002, 9, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Massei, F.; Gori, L.; Macchia, P.; Maggiore, G. The expanded spectrum of bartonellosis in children. Infect. Dis. Clin. N. Am. 2005, 19, 691–711. [Google Scholar] [CrossRef]
- Hajjaji, N.; Hocqueloux, L.; Kerdraon, R.; Bret, L. Bone infection in cat-scratch disease: A review of the literature. J. Infect. 2007, 54, 417–421. [Google Scholar] [CrossRef]
- Spinella, A.; Lumetti, F.; Sandri, G.; Cestelli, V.; Mascia, M.T. Beyond cat scratch disease: A case report of bartonella infection mimicking vasculitic disorder. Case Rep. Infect. Dis. 2012, 2012, 354625. [Google Scholar] [CrossRef]
- Herremans, M.; Vermeulen, M.J.; Van de Kassteele, J.; Bakker, J.; Schellekens, J.F.P.; Koopmans, M.P.G. The use of Bartonella henselae-specific age dependent IgG and IgM in diagnostic models to discriminate diseased from non-diseased in Cat Scratch Disease serology. J. Microbiol. Methods 2007, 71, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Mazur-Melewska, K.; Mania, A.; Kemnitz, P.; Figlerowicz, M.; Służewski, W. Cat-scratch disease: A wide spectrum of clinical pictures. Postepy Dermatol. Alergol. 2015, 32, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Carithers, H.A. Cat-scratch disease: An overview based on a study of 1200 patients. Am. J. Dis. Child. 1985, 139, 1124. [Google Scholar] [CrossRef] [PubMed]
- Margileth, A.M. Cat scratch disease. Adv. Pediatr. Infect. Dis. 1993, 8, 1–21. [Google Scholar]
- Schaible, U.E.; Collins, H.L.; Kaufmann, S.H. Confrontation between intracellular bacteria and the immune system. Adv. Immunol. 1999, 71, 267–377. [Google Scholar] [PubMed]
- Knodler, L.A.; Celli, J.; Finlay, B.B. Pathogenic trickery: Deception of host cell processes. Nat. Rev. Mol. Cell Biol. 2001, 2, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Karem, K.L. Immune aspects of Bartonella. Crit. Rev. Microbiol. 2000, 26, 133–145. [Google Scholar] [CrossRef]
- Kobayashi, K.; Kaneda, K.; Kasama, T. Immunopathogenesis of delayed-type hypersensitivity. Microsc. Res. Tech. 2001, 53, 241–245. [Google Scholar] [CrossRef]
- Karem, K.L.; Dubois, K.A.; McGill, S.L.; Regnery, R.L. Characterization of Bartonella henselae-specific immunity in BALB/c mice. Immunology 1999, 97, 352–358. [Google Scholar] [CrossRef]
- Hong, J.; Li, Y.; Hua, X.; Bai, Y.; Wang, C.; Zhu, C.; Du, Y.; Yang, Z.; Yuan, C. Lymphatic Circulation Disseminates Bartonella Infection into Bloodstream. J. Infect. Dis. 2017, 215, 303–311. [Google Scholar] [CrossRef]
- O’Rourke, F.; Schmidgen, T.; Kaiser, P.O.; Linke, D.; Kempf, V.A.J. Adhesins of Bartonella spp. Adv. Exp. Med. Biol. 2011, 715, 51–70. [Google Scholar] [CrossRef] [PubMed]
- Riess, T.; Andersson, S.G.E.; Lupas, A.; Schaller, M.; Schäfer, A.; Kyme, P.; Martin, J.; Wälzlein, J.-H.; Ehehalt, U.; Lindroos, H.; et al. Bartonella adhesin a mediates a proangiogenic host cell response. J. Exp. Med. 2004, 200, 1267–1278. [Google Scholar] [CrossRef]
- McCord, A.M.; Burgess, A.W.O.; Whaley, M.J.; Anderson, B.E. Interaction of Bartonella henselae with endothelial cells promotes monocyte/macrophage chemoattractant protein 1 gene expression and protein production and triggers monocyte migration. Infect. Immun. 2005, 73, 5735–5742. [Google Scholar] [CrossRef] [PubMed]
- Varney, M.L.; Olsen, K.J.; Mosley, R.L.; Bucana, C.D.; Talmadge, J.E.; Singh, R.K. Monocyte/macrophage recruitment, activation and differentiation modulate interleukin-8 production: A paracrine role of tumor-associated macrophages in tumor angiogenesis. In Vivo 2002, 16, 471–477. [Google Scholar] [PubMed]
- Mosepele, M.; Mazo, D.; Cohn, J. Bartonella infection in immunocompromised hosts: Immunology of vascular infection and vasoproliferation. Clin. Dev. Immunol. 2012, 2012, 612809. [Google Scholar] [CrossRef]
- Fuhrmann, O.; Arvand, M.; Göhler, A.; Schmid, M.; Krüll, M.; Hippenstiel, S.; Seybold, J.; Dehio, C.; Suttorp, N. Bartonella henselae induces NF-kappaB-dependent upregulation of adhesion molecules in cultured human endothelial cells: Possible role of outer membrane proteins as pathogenic factors. Infect. Immun. 2001, 69, 5088–5097. [Google Scholar] [CrossRef]
- Cerimele, F.; Brown, L.F.; Bravo, F.; Ihler, G.M.; Kouadio, P.; Arbiser, J.L. Infectious angiogenesis: Bartonella bacilliformis infection results in endothelial production of angiopoetin-2 and epidermal production of vascular endothelial growth factor. Am. J. Pathol. 2003, 163, 1321–1327. [Google Scholar] [CrossRef]
- Reed, J.B.; Scales, D.K.; Wong, M.T.; Lattuada, C.P., Jr.; Dolan, M.J.; Schwab, I.R. Bartonella henselae neuroretinitis in cat scratch disease. Diagnosis, management, and sequelae. Ophthalmology 1998, 105, 459–466. [Google Scholar] [CrossRef]
- Brouqui, P.; Raoult, D. Bartonella quintana invades and multiplies within endothelial cells in vitro and in vivo and forms intracellular blebs. Res. Microbiol. 1996, 147, 719–731. [Google Scholar] [CrossRef]
- Dehio, C. Bartonella-host-cell interactions and vascular tumour formation. Nat. Rev. Microbiol. 2005, 3, 621–631. [Google Scholar] [CrossRef]
- Resto-Ruiz, S.I.; Schmiederer, M.; Sweger, D.; Newton, C.; Klein, T.W.; Friedman, H.; Anderson, B.E. Induction of a potential paracrine angiogenic loop between human THP-1 macrophages and human microvascular endothelial cells during Bartonella henselae infection. Infect. Immun. 2002, 70, 4564–4570. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vayssier-Taussat, M.; Le Rhun, D.; Deng, H.K.; Biville, F.; Cescau, S.; Danchin, A.; Marignac, G.; Lenaour, E.; Boulouis, H.J.; Mavris, M.; et al. The Trw type IV secretion system of Bartonella mediates host-specific adhesion to erythrocytes. PLoS Pathog. 2010, 6, e1000946. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, L.; Joo, D.; Sun, S.-C. NF-κB signaling in inflammation. Signal Transduct. Target. Ther. 2017, 2. [Google Scholar] [CrossRef]
- Pulliainen, A.T.; Dehio, C. Bartonella henselae: Subversion of vascular endothelial cell functions by translocated bacterial effector proteins. Int. J. Biochem. Cell Biol. 2009, 41, 507–510. [Google Scholar] [CrossRef]
- Adal, K.A.; Cockerell, C.J.; Petri, W.A., Jr. Cat scratch disease, bacillary angiomatosis, and other infections due to Rochalimaea. N. Engl. J. Med. 1994, 330, 1509–1515. [Google Scholar] [CrossRef]
- Selby, G.; Walker, G.L. Cerebral arteritis in cat-scratch disease. Neurology 1979, 29, 1413–1418. [Google Scholar] [CrossRef]
- O’Hara, P.J.; Sheppard, P.O.; Thøgersen, H.; Venezia, D.; Haldeman, B.A.; McGrane, V.; Houamed, K.M.; Thomsen, C.; Gilbert, T.L.; Mulvihill, E.R. The ligand-binding domain in metabotropic glutamate receptors is related to bacterial periplasmic binding proteins. Neuron 1993, 11, 41–52. [Google Scholar] [CrossRef]
- Nitsch, C.; Hubauer, H. Distant blood-brain barrier opening in subfields of the rat hippocampus after intrastriatal injections of kainic acid but not ibotenic acid. Neurosci. Lett. 1986, 64, 53–58. [Google Scholar] [CrossRef]
- Bangash, I.H.; Kandt, R.S.; D’Souza, B.J.; Heinz, R. Hyperdensity on CT after seizure: A pitfall. J. Child Neurol. 1987, 2, 276–278. [Google Scholar] [CrossRef]
- Andrews, P.I.; McNamara, J.O. Rasmussen’s encephalitis: An autoimmune disorder? Curr. Opin. Neurol. 1996, 9, 141–145. [Google Scholar] [CrossRef]
- Harms, A.; Dehio, C. Intruders below the radar: Molecular pathogenesis of Bartonella spp. Clin. Microbiol. Rev. 2012, 25, 42–78. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.L.; Kogelnik, A.M.; Mozayeni, R.B.; Cherry, N.A.; Breitschwerdt, E.B. Neurological and immunological dysfunction in two patients with Bartonella henselae bacteremia. Clin. Case Rep. 2017, 5, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Muñana, K.R.; Vitek, S.M.; Hegarty, B.C.; Kordick, D.L.; Breitschwerdt, E.B. Infection of fetal feline brain cells in culture with Bartonella henselae. Infect. Immun. 2001, 69, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Dehio, C.; Meyer, M.; Berger, J.; Schwarz, H.; Lanz, C. Interaction of Bartonella henselae with endothelial cells results in bacterial aggregation on the cell surface and the subsequent engulfment and internalisation of the bacterial aggregate by a unique structure, the invasome. J. Cell Sci. 1997, 110 Pt 18, 2141–2154. [Google Scholar] [CrossRef]
- Rhomberg, T.A.; Truttmann, M.C.; Guye, P.; Ellner, Y.; Dehio, C. A translocated protein of Bartonella henselae interferes with endocytic uptake of individual bacteria and triggers uptake of large bacterial aggregates via the invasome. Cell. Microbiol. 2009, 11, 927–945. [Google Scholar] [CrossRef]
- Kyme, P.A.; Haas, A.; Schaller, M.; Peschel, A.; Iredell, J.; Kempf, V.A.J. Unusual trafficking pattern of Bartonella henselae -containing vacuoles in macrophages and endothelial cells: Trafficking of B. henselae-containing vacuoles. Cell. Microbiol. 2005, 7, 1019–1034. [Google Scholar] [CrossRef]
- Maeno, N.; Oda, H.; Yoshiie, K.; Wahid, M.R.; Fujimura, T.; Matayoshi, S. Live Bartonella henselae enhances endothelial cell proliferation without direct contact. Microb. Pathog. 1999, 27, 419–427. [Google Scholar] [CrossRef]
- Álvarez-Fernández, A.; Breitschwerdt, E.B.; Solano-Gallego, L. Bartonella infections in cats and dogs including zoonotic aspects. Parasit. Vectors 2018, 11, 624. [Google Scholar] [CrossRef]
- Díaz-Flores, L.; Gutiérrez, R.; Madrid, J.F.; Varela, H.; Valladares, F.; Acosta, E.; Martín-Vasallo, P.; Díaz-Flores, L., Jr. Pericytes. Morphofunction, interactions and pathology in a quiescent and activated mesenchymal cell niche. Histol. Histopathol. 2009, 24, 909–969. [Google Scholar] [CrossRef]
- Benjamin, L.E.; Hemo, I.; Keshet, E. A plasticity window for blood vessel remodelling is defined by pericyte coverage of the preformed endothelial network and is regulated by PDGF-B and VEGF. Development 1998, 125, 1591–1598. [Google Scholar] [CrossRef]
- Greenberg, J.I.; Shields, D.J.; Barillas, S.G.; Acevedo, L.M.; Murphy, E.; Huang, J.; Scheppke, L.; Stockmann, C.; Johnson, R.S.; Angle, N.; et al. A role for VEGF as a negative regulator of pericyte function and vessel maturation. Nature 2008, 456, 809–813. [Google Scholar] [CrossRef]
- Aiello, L.P.; Northrup, J.M.; Keyt, B.A.; Takagi, H.; Iwamoto, M.A. Hypoxic regulation of vascular endothelial growth factor in retinal cells. Arch. Ophthalmol. 1995, 113, 1538–1544. [Google Scholar] [CrossRef]
- Yamagishi, S.; Yonekura, H.; Yamamoto, Y.; Fujimori, H.; Sakurai, S.; Tanaka, N.; Yamamoto, H. Vascular endothelial growth factor acts as a pericyte mitogen under hypoxic conditions. Lab. Investig. 1999, 79, 501–509. [Google Scholar]
- Kempf, V.A.; Volkmann, B.; Schaller, M.; Sander, C.A.; Alitalo, K.; Riess, T.; Autenrieth, I.B. Evidence of a leading role for VEGF in Bartonella henselae-induced endothelial cell proliferations. Cell. Microbiol. 2001, 3, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Dubey, S.; Varney, M.L.; Dave, B.J.; Singh, R.K. IL-8 directly enhanced endothelial cell survival, proliferation, and matrix metalloproteinases production and regulated angiogenesis. J. Immunol. 2003, 170, 3369–3376. [Google Scholar] [CrossRef] [PubMed]
- Varanat, M.; Maggi, R.G.; Linder, K.E.; Breitschwerdt, E.B. Infection of human brain vascular pericytes (HBVPs) by Bartonella henselae. Med. Microbiol. Immunol. 2013, 202, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.K.; Guthmiller, J.M.; Joly, S.; Organ, C.C.; Dawson, D.V. Interleukin-1 and interleukin-8 in nicotine- and lipopolysaccharide-exposed gingival keratinocyte cultures. J. Periodontal Res. 2010, 45, 583–588. [Google Scholar] [CrossRef]
- Matera, G.; Liberto, M.C.; Quirino, A.; Barreca, G.S.; Lamberti, A.G.; Iannone, M.; Mancuso, E.; Palma, E.; Cufari, F.A.; Rotiroti, D.; et al. Bartonella quintana lipopolysaccharide effects on leukocytes, CXC chemokines and apoptosis: A study on the human whole blood and a rat model. Int. Immunopharmacol. 2003, 3, 853–864. [Google Scholar] [CrossRef]
- McCord, A.M.; Resto-Ruiz, S.I.; Anderson, B.E. Autocrine role for interleukin-8 in Bartonella henselae-induced angiogenesis. Infect. Immun. 2006, 74, 5185–5190. [Google Scholar] [CrossRef][Green Version]
- Trinchieri, G.; Scott, P. Interleukin-12: A proinflammatory cytokine with immunoregulatory functions. Res. Immunol. 1995, 146, 423–431. [Google Scholar] [CrossRef]
- Musso, D.; Drancourt, M.; Raoult, D. Lack of bactericidal effect of antibiotics except aminoglycosides on Bartonella (Rochalimaea) henselae. J. Antimicrob. Chemother. 1995, 36, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Wear, D.J.; Margileth, A.M.; Hadfield, T.L.; Fischer, G.W.; Schlagel, C.J.; King, F.M. Cat scratch disease: A bacterial infection. Science 1983, 221, 1403–1405. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, S.W.; Wolf, S.M.; Steinberg, E.A. Cat-scratch encephalopathy. Neurology 1997, 49, 876–878. [Google Scholar] [CrossRef] [PubMed]
- Dickson, D.W.; Mattiace, L.A.; Kure, K.; Hutchins, K.; Lyman, W.D.; Brosnan, C.F. Microglia in human disease, with an emphasis on acquired immune deficiency syndrome. Lab. Investig. 1991, 64, 135–156. [Google Scholar]
- Tyor, W.R.; Glass, J.D.; Griffin, J.W.; Becker, P.S.; McArthur, J.C.; Bezman, L.; Griffin, D.E. Cytokine expression in the brain during the acquired immunodeficiency syndrome. Ann. Neurol. 1992, 31, 349–360. [Google Scholar] [CrossRef]
- Selmaj, K.W.; Raine, C.S. Tumor necrosis factor mediates myelin and oligodendrocyte damage in vitro. Ann. Neurol. 1988, 23, 339–346. [Google Scholar] [CrossRef]
- Opavsky, M.A. Cat scratch disease: The story continues. Can. J. Infect. Dis. 1997, 8, 43–49. [Google Scholar] [CrossRef]
- Seals, J.E.; Oken, H.A. Cat Scratch Encephalopathy. Md Med. J. 1999, 48, 176–178. [Google Scholar]
- Breitschwerdt, E.B.; Mascarelli, P.E.; Schweickert, L.A.; Maggi, R.G.; Hegarty, B.C.; Bradley, J.M.; Woods, C.W. Hallucinations, sensory neuropathy, and peripheral visual deficits in a young woman infected with Bartonella koehlerae. J. Clin. Microbiol. 2011, 49, 3415–3417. [Google Scholar] [CrossRef]
- Klein, J.D. Cat scratch disease. Pediatr. Rev. 1994, 15, 348–353. [Google Scholar] [CrossRef]
- Lyon, L.W. Neurologic manifestations of cat-scratch disease. Report of a case and review of the literature. Arch. Neurol. 1971, 25, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Shinall, E.A. Cat-scratch disease: A review of the literature. Pediatr. Dermatol. 1990, 7, 11–18. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Holman, R.C.; Curns, A.T.; O’Reilly, M.; McQuiston, J.H.; Steiner, C.A. Epidemiology of cat-scratch disease hospitalizations among children in the United States. Pediatr. Infect. Dis. J. 2005, 24, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Seah, A.B.H.; Azran, M.S.; Rucker, J.C.; Biousse, V.; Martin, D.F.; Newman, N.J. Magnetic resonance imaging abnormalities in cat-scratch disease encephalopathy. J. Neuroophthalmol. 2003, 23, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Gerber, J.E.; Johnson, J.E.; Scott, M.A.; Madhusudhan, K.T. Fatal meningitis and encephalitis due to Bartonella henselae bacteria. J. Forensic Sci. 2002, 47, 640–644. [Google Scholar] [CrossRef]
- Swedo, S.E.; Seidlitz, J.; Kovacevic, M.; Latimer, M.E.; Hommer, R.; Lougee, L.; Grant, P. Clinical presentation of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections in research and community settings. J. Child Adolesc. Psychopharmacol. 2015, 25, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Armengol, C.E.; Hendley, J.O. Cat-scratch disease encephalopathy: A cause of status epilepticus in school-aged children. J. Pediatr. 1999, 134, 635–638. [Google Scholar] [CrossRef]
- Stevens, H. Cat-scratch fever encephalitis. AMA Am. J. Dis. Child. 1952, 84, 218–222. [Google Scholar] [CrossRef]
- Genizi, J.; Kasis, I.; Schif, A.; Shahar, E. Effect of high-dose methyl-prednisolone on brainstem encephalopathy and basal ganglia impairment complicating cat scratch disease. Brain Dev. 2007, 29, 377–379. [Google Scholar] [CrossRef]
- Anbu, A.T.; Foulerton, M.; McMaster, P.; Bakalinova, D. Basal ganglia involvement in a child with cat-scratch disease. Pediatr. Infect. Dis. J. 2003, 22, 931–932. [Google Scholar] [CrossRef]
- Balakrishnan, N.; Ericson, M.; Maggi, R.; Breitschwerdt, E.B. Vasculitis, cerebral infarction and persistent Bartonella henselae infection in a child. Parasit. Vectors 2016, 9, 254. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.L.; Honeycutt, T.C.B.; Hamrick, H.J. Status epilepticus due to cat scratch disease: Recognition, diagnosis, and thoughts on pathogenesis. Pediatr. Emerg. Care 2016, 32, 789–791. [Google Scholar] [CrossRef] [PubMed]
- Marienfeld, C.B.; Dicapua, D.B.; Sze, G.K.; Goldstein, J.M. Expressive aphasia as a presentation of encephalitis with Bartonella henselae infection in an immunocompetent adult. Yale J. Biol. Med. 2010, 83, 67–71. [Google Scholar] [PubMed]
- Kolski, H.; Ford-Jones, E.L.; Richardson, S.; Petric, M.; Nelson, S.; Jamieson, F.; Blaser, S.; Gold, R.; Otsubo, H.; Heurter, H.; et al. Etiology of acute childhood encephalitis at The Hospital for Sick Children, Toronto, 1994–1995. Clin. Infect. Dis. 1998, 26, 398–409. [Google Scholar] [CrossRef] [PubMed]
- Marra, M. Neurologic complications of Bartonella henselae infection Christina. Curr. Opin. Neurol. 1995, 8, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Baylor, P.; Garoufi, A.; Karpathios, T.; Lutz, J.; Mogelof, J.; Moseley, D. Transverse myelitis in 2 patients with Bartonella henselae infection (cat scratch disease). Clin. Infect. Dis. 2007, 45, e42–e45. [Google Scholar] [CrossRef] [PubMed]
- Farooque, P.; Khurana, D.S.; Melvin, J.J. Persistent focal seizures after cat scratch encephalopathy. Pediatr. Neurol. 2010, 42, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Cherinet, Y.; Tomlinson, R. Cat scratch disease presenting as acute encephalopathy. Emerg. Med. J. 2008, 25, 703–704. [Google Scholar] [CrossRef] [PubMed]
- Fouch, B.; Coventry, S. A case of fatal disseminated Bartonella henselae infection (cat-scratch disease) with encephalitis. Arch. Pathol. Lab. Med. 2007, 131, 1591–1594. [Google Scholar] [CrossRef]
- Walter, R.S.; Eppes, S.C. Cat scratch disease presenting with peripheral facial nerve paralysis. Pediatrics 1998, 101, E13. [Google Scholar] [CrossRef]
- Ganesan, K.; Mizen, K. Cat scratch disease: An unusual cause of facial palsy and partial ptosis: Case report. J. Oral Maxillofac. Surg. 2005, 63, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, G.S.; Katz, A. Epilepsia partialis continua as an atypical presentation of cat scratch disease in a young adult. Neurology 2002, 59, 1815–1816. [Google Scholar] [CrossRef]
- Puligheddu, M.; Giagheddu, A.; Genugu, F.; Giagheddu, M.; Marrosu, F. Epilepsia partialis continua in cat scratch disease. Seizure 2004, 13, 191–195. [Google Scholar] [CrossRef][Green Version]
- Rocha, J.L.; Pellegrino, L.N.; Riella, L.V.; Martins, L.T. Acute hemiplegia associated with cat-scratch disease. Braz. J. Infect. Dis. 2004, 8, 263–266. [Google Scholar] [CrossRef][Green Version]
- Easley, R.B.; Cooperstock, M.S.; Tobias, J.D. Cat-scratch disease causing status epilepticus in children. South. Med. J. 1999, 92, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Brinar, V.V.; Habek, M. Rare infections mimicking MS. Clin. Neurol. Neurosurg. 2010, 112, 625–628. [Google Scholar] [CrossRef]
- Salgado, C.D.; Weisse, M.E. Transverse myelitis associated with probable cat-scratch disease in a previously healthy pediatric patient. Clin. Infect. Dis. 2000, 31, 609–611. [Google Scholar] [CrossRef]
- Schaller, J.L.; Burkland, G.A.; Langhoff, P.J. Do bartonella infections cause agitation, panic disorder, and treatment-resistant depression? MedGenMed 2007, 9, 54. [Google Scholar]
- Nakamura, C.; Inaba, Y.; Tsukahara, K.; Mochizuki, M.; Sawanobori, E.; Nakazawa, Y.; Aoyama, K. A pediatric case with peripheral facial nerve palsy caused by a granulomatous lesion associated with cat scratch disease. Brain Dev. 2018, 40, 159–162. [Google Scholar] [CrossRef]
- Mutucumarana, C.P.; Kumar, R.D.; Foradori, D.M.; Ramgopal, V.; Demmler, G.J. Facial nerve palsy in a child with fever of unknown origin. Clin. Pediatr. 2020, 59, 516–518. [Google Scholar] [CrossRef]
- Premachandra, D.J.; Milton, C.M. Cat scratch disease in the parotid gland presenting with facial paralysis. Br. J. Oral Maxillofac. Surg. 1990, 28, 413–415. [Google Scholar] [CrossRef]
- Chiu, A.G.; Hecht, D.A.; Prendiville, S.A.; Mesick, C.; Mikula, S.; Deeb, Z.E. Atypical presentations of cat scratch disease in the head and neck. Otolaryngol. Head Neck Surg. 2001, 125, 414–416. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.K.; Vaphiades, M.S.; Saccente, M. Cat-scratch disease presenting as neuroretinitis and peripheral facial palsy. J. Neuroophthalmol. 1999, 19, 240–241. [Google Scholar] [CrossRef] [PubMed]
- Cerpa Polar, R.; Orellana, G.; Silva Caso, W.; Sánchez Carbonel, J.; Santisteban, J.; Del Valle Mendoza, J.; Santisteban, J. Encephalitis with convulsive status in an immunocompetent pediatric patient caused by Bartonella henselae. Asian Pac. J. Trop. Med. 2016, 9, 610–613. [Google Scholar] [CrossRef]
- Lewis, D.W.; Tucker, S.H. Central nervous system involvement in cat scratch disease. Pediatrics 1986, 77, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, M.J.; Rutten, G.J.; Verhagen, I.; Peeters, M.F.; van Dijken, P.J. Transient paresis associated with cat-scratch disease: Case report and literature review of vertebral osteomyelitis caused by Bartonella henselae: Case report and literature review of vertebral osteomyelitis caused by Bartonella henselae. Pediatr. Infect. Dis. J. 2006, 25, 1177–1181. [Google Scholar] [CrossRef] [PubMed]
- Yap, S.M.; Saeed, M.; Logan, P.; Healy, D.G. Bartonella neuroretinitis (cat-scratch disease). Pract. Neurol. 2020, 20, 505–506. [Google Scholar] [CrossRef] [PubMed]
- Grando, D.; Sullivan, L.J.; Flexman, J.P.; Watson, M.W.; Andrew, J.H. Bartonella henselae associated with Parinaud’s oculoglandular syndrome. Clin. Infect. Dis. 1999, 28, 1156–1158. [Google Scholar] [CrossRef]
- Cunningham, E.T.; Koehler, J.E. Ocular bartonellosis. Am. J. Ophthalmol. 2000, 130, 340–349. [Google Scholar] [CrossRef]
- Solley, W.A.; Martin, D.F.; Newman, N.J.; King, R.; Callanan, D.G.; Zacchei, T.; Wallace, R.T.; Parks, D.J.; Bridges, W.; Sternberg, P., Jr. Cat scratch disease: Posterior segment manifestations. Ophthalmology 1999, 106, 1546–1553. [Google Scholar] [CrossRef]
- Oray, M.; Önal, S.; Koç Akbay, A.; Tuğal Tutkun, İ. Diverse clinical signs of ocular involvement in cat scratch disease. Turk. J. Ophthalmol. 2017, 47, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Amer, R.; Tugal-Tutkun, I. Ophthalmic manifestations of bartonella infection. Curr. Opin. Ophthalmol. 2017, 28, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Eiger-Moscovich, M.; Amer, R.; Oray, M.; Tabbara, K.F.; Tugal-Tutkun, I.; Kramer, M. Retinal artery occlusion due to Bartonella henselae infection: A case series. Acta Ophthalmol. 2016, 94, e367–e370. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.M.; Davis, J.L.; Gass, D.M. Branch retinal arterial occlusions in multifocal retinitis with optic nerve edema. Arch. Ophthalmol. 1995, 113, 1271–1276. [Google Scholar] [CrossRef]
- Batsos, G.; Kabanarou, S.A.; Fotiou, P.; Rouvas, A.; Xirou, T. Retinal arterial occlusive disease in a young patient with cat scratch disease. Case Rep. Ophthalmol. 2013, 4, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.V.; Michels, K.S.; Lauer, A.K.; Samples, J.R. Bartonella henselae infection associated with neuroretinitis, central retinal artery and vein occlusion, neovascular glaucoma, and severe vision loss. Am. J. Ophthalmol. 2004, 137, 187–189. [Google Scholar] [CrossRef]
- Schadlu, R.; Apte, R.S. Spontaneous resolution of an inflammation-associated epiretinal membrane with previously documented posterior vitreous detachment. Br. J. Ophthalmol. 2007, 91, 1252–1253. [Google Scholar] [CrossRef] [PubMed]
- Andreev, A.N.; Bushuev, A.V.; Svetozarskiy, S.N. A case of secondary epiretinal membrane spontaneous release. Case Rep. Ophthalmol. Med. 2016, 2016, 4925763. [Google Scholar] [CrossRef]
- Ozgonul, C.; Besirli, C.G. Macular hole closure following spontaneous release of vitreomacular traction. BMJ Case Rep. 2017, 2017, bcr2016218547. [Google Scholar] [CrossRef]
- Warren, K.; Goldstein, E.; Hung, V.S.; Koehler, J.E.; Richardson, W. Use of retinal biopsy to diagnose Bartonella (formerly Rochalimaea) henselae retinitis in an HIV-infected patient. Arch. Ophthalmol. 1998, 116, 937–940. [Google Scholar] [CrossRef]
- Best, J.A.; Price, B. Central scotoma without prodromal illness caused by Bartonella henselae neuroretinitis. Am. J. Emerg. Med. 2013, 31, 887.e1–887.e2. [Google Scholar] [CrossRef] [PubMed]
- Suhler, E.B.; Lauer, A.K.; Rosenbaum, J.T. Prevalence of serologic evidence of cat scratch disease in patients with neuroretinitis11The authors have no proprietary interest in the products mentioned herein. Ophthalmology 2000, 107, 871–876. [Google Scholar] [CrossRef]
- Tey, M.S.-Y.; Govindasamy, G.; Vendargon, F.M. The clinical spectrum of ocular bartonellosis: A retrospective study at a tertiary centre in Malaysia. J. Ophthalmic Inflamm. Infect. 2020, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Annoura, K.; Sano, I.; Makino, S.; Kawashima, H. Multiple ocular manifestations in a case of cat scratch disease without systemic signs. GMS Ophthalmol. Cases 2020, 10, Doc45. [Google Scholar] [CrossRef]
- Rodríguez-Castelblanco, Á.; Cordero-Coma, M. Leber’s idiopathic stellate neuroretinitis: Diagnostic and therapeutic conflicts. Arch. Soc. Esp. Oftalmol. (Engl. Ed.) 2019, 94, 413–416. [Google Scholar] [CrossRef]
- Gass, J.D. Diseases of the optic nerve that may simulate macular disease. Trans. Sect. Ophthalmol. Am. Acad. Ophthalmol. Otolaryngol. 1977, 83, 763–770. [Google Scholar]
- Celiker, H.; Kazokoglu, H.; Eraslan, M.; Cerman, E.; Karabas, L. Bartonella henselae Neuroretinitis in Patients without Cat Scratch. Jpn. J. Infect. Dis. 2018, 71, 397–401. [Google Scholar] [CrossRef]
- Rabina, G.; Goldstein, M. Cat scratch disease, ocular manifestations. In Encyclopedia of Ophthalmology; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–3. ISBN 9783642359514. [Google Scholar]
- Williams, D.M.; Schachter, J. Role of cell-mediated immunity in chlamydial infection: Implications for ocular immunity. Rev. Infect. Dis. 1985, 7, 754–759. [Google Scholar] [CrossRef]
- Pîrvu, A.S.; Andrei, A.M.; Stănciulescu, E.C.; Baniță, I.M.; Pisoschi, C.G.; Jurja, S.; Ciuluvica, R. NAD+ metabolism and retinal degeneration (Review). Exp. Ther. Med. 2021, 22, 670. [Google Scholar] [CrossRef]
- Ray, S.; Gragoudas, E. Neuroretinitis. Int. Ophthalmol. Clin. 2001, 41, 83–102. [Google Scholar] [CrossRef]
- Jurja, S.; Hîncu, M.; Dobrescu, M.A.; Golu, A.E.; Bălăşoiu, A.T.; Coman, M. Ocular cells and light: Harmony or conflict? Rom. J. Morphol. Embryol. 2014, 55, 257–261. [Google Scholar]
- Jurja, S.; Coman, M.; Hîncu, M.C. The ultraviolet influence upon soft eye tissues. Rom. J. Morphol. Embryol. 2017, 58, 45–52. [Google Scholar]
- Maitland, C.G.; Miller, N.R. Neuroretinitis. Arch. Ophthalmol. 1984, 102, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Purvin, V.; Sundaram, S.; Kawasaki, A. Neuroretinitis: Review of the literature and new observations. J. Neuroophthalmol. 2011, 31, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Kahloun, R.; Khairallah-Ksiaa, I.; Abroug, N.; Mahmoud, A.; Ben Yahia, S.; Zaouali, S.; Jelliti, B.; Khairallah, M. Final diagnosis in patients referred with a diagnosis of neuroretinitis. Neuroophthalmology 2015, 39, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.C.; Brucker, A.J.; Tamhankar, M.A. An atypical presentation of Bartonella neuroretinitis. Retina 2016, 36, e18–e19. [Google Scholar] [CrossRef] [PubMed]
- Chi, S.L.; Stinnett, S.; Eggenberger, E.; Foroozan, R.; Golnik, K.; Lee, M.S.; Bhatti, M.T. Clinical characteristics in 53 patients with cat scratch optic neuropathy. Ophthalmology 2012, 119, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Aziz, H.A.; Plesec, T.P.; Sabella, C.; Udayasankar, U.K.; Singh, A.D. Cat scratch disease: Expanded spectrum. Ocul. Oncol. Pathol. 2016, 2, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Freitas-Neto, C.A.; Oréfice, F.; Costa, R.A.; Oréfice, J.L.; Dhanireddy, S.; Maghsoudlou, A.; Foster, C.S. Multimodal imaging assisting the early diagnosis of cat-scratch neuroretinitis. Semin. Ophthalmol. 2016, 31, 495–498. [Google Scholar] [CrossRef]
- McClintic, J.; Srivastava, S.K. Imaging in the diagnosis and management of ocular cat scratch disease. Int. Ophthalmol. Clin. 2012, 52, 155–161. [Google Scholar] [CrossRef]
- Fish, R.H.; Hogan, R.N.; Nightingale, S.D.; Anand, R. Peripapillary angiomatosis associated with cat-scratch neuroretinitis. Arch. Ophthalmol. 1992, 110, 323. [Google Scholar] [CrossRef] [PubMed]
- Habot-Wilner, Z.; Tiosano, L.; Sanchez, J.M.; Shulman, S.; Barequet, D.; Rahat, O.; Amarilyo, G.; Amer, R. Demographic and clinical features of pediatric uveitis in Israel. Ocul. Immunol. Inflamm. 2020, 28, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Habot-Wilner, Z.; Zur, D.; Goldstein, M.; Goldenberg, D.; Shulman, S.; Kesler, A.; Giladi, M.; Neudorfer, M. Macular findings on optical coherence tomography in cat-scratch disease neuroretinitis. Eye 2011, 25, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Conrad, D.A. Treatment of cat-scratch disease. Curr. Opin. Pediatr. 2001, 13, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, M.T.; Lee, M.S. Should patients with bartonella neuroretinitis receive treatment? J. Neuroophthalmol. 2014, 34, 412–416. [Google Scholar] [CrossRef]
- Lee, W.R.; Chawla, J.C.; Reid, R. Bacillary angiomatosis of the conjunctiva. Am. J. Ophthalmol. 1994, 118, 152–157. [Google Scholar] [CrossRef]
- Prutsky, G.; Domecq, J.P.; Mori, L.; Bebko, S.; Matzumura, M.; Sabouni, A.; Shahrour, A.; Erwin, P.J.; Boyce, T.G.; Montori, V.M.; et al. Treatment outcomes of human bartonellosis: A systematic review and meta-analysis. Int. J. Infect. Dis. 2013, 17, e811–e819. [Google Scholar] [CrossRef]
- Rostad, C.A.; McElroy, A.K.; Hilinski, J.A.; Thompson, M.P.; Drew, C.P.; Denison, A.M.; Zaki, S.R.; Mahle, W.T.; Rogers, J.; Abramowsky, C.R.; et al. Bartonella henselae-mediated disease in solid organ transplant recipients: Two pediatric cases and a literature review. Transpl. Infect. Dis. 2012, 14, E71–E81. [Google Scholar] [CrossRef]
- Kodama, T.; Masuda, H.; Ohira, A. Neuroretinitis associated with cat-scratch disease in Japanese patients: Acta Ophthalmologica Scandinavica 2003. Acta Ophthalmol. Scand. 2003, 81, 653–657. [Google Scholar] [CrossRef]
- Canneti, B.; Cabo-López, I.; Puy-Núñez, A.; García García, J.C.; Cores, F.J.; Trigo, M.; Suárez-Gil, A.P.; Rodriguez-Regal, A. Neurological presentations of Bartonella henselae infection. Neurol. Sci. 2019, 40, 261–268. [Google Scholar] [CrossRef]
- Peláez Bejarano, A.; Sánchez Del Moral, R.; Guisado-Gil, A.B. Bartonella henselae encephalopathy in a paediatric patient: A case report and treatment review. J. Clin. Pharm. Ther. 2020, 45, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Atıcı, S.; Kadayıfcı, E.K.; Karaaslan, A.; Toper, M.H.; Celikel, C.A.; Soysal, A.; Bakır, M. Atypical presentation of cat-scratch disease in an immunocompetent child with serological and pathological evidence. Case Rep. Pediatr. 2014, 2014, 397437. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bogue, C.W. Antibiotic therapy for cat-scratch disease? Pediatr. Infect. Dis. J. 1990, 9, 69. [Google Scholar] [CrossRef]
- Collipp, P.J. Cat-scratch disease therapy. Arch. Pediatr. Adolesc. Med. 1989, 143, 1261. [Google Scholar] [CrossRef] [PubMed]
- Rosas, L.; Rao, K.; McGough, C.; Becker, A. A rare case of Bartonella encephalitis with hemiplegia. Child Neurol. Open 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Raihan, A.-R.; Zunaina, E.; Wan-Hazabbah, W.-H.; Adil, H.; Lakana-Kumar, T. Neuroretinitis in ocular bartonellosis: A case series. Clin. Ophthalmol. 2014, 8, 1459–1466. [Google Scholar] [CrossRef] [PubMed]
- Zakhour, R.; Mancias, P.; Heresi, G.; Pérez, N. Transverse myelitis and Guillain-Barré syndrome associated with cat-scratch disease, Texas, USA, 2011. Emerg. Infect. Dis. 2018, 24, 1754–1755. [Google Scholar] [CrossRef] [PubMed]
- Bilavsky, E.; Amit, S.; Avidor, B.; Ephros, M.; Giladi, M. Cat scratch disease during pregnancy. Obstet. Gynecol. 2012, 119, 640–644. [Google Scholar] [CrossRef]
- Pinto, V.L., Jr.; Curi, A.L.; Pinto, A.D.S.; Nunes, E.P.; Teixeira, M.D.L.B.; Rozental, T.; Favacho, A.R.; de Lemos, E.R.S.; Bóia, M.N. Cat scratch disease complicated with aseptic meningitis and neuroretinitis. Braz. J. Infect. Dis. 2008, 12, 158–160. [Google Scholar] [CrossRef]

| Disease | Possible Mechanism | Source |
|---|---|---|
| Cat-scratch disease | B henslae rapidly infects human erythrocytes and can be found in lymph nodes or affect any cell or organ in the body. | Bartonella henselae transmitted by cats or dogs |
| Carrion’s disease | The bacterium adheres to erythrocyte surfaces. Through bacterial invasion and reproduction, many erythrocytes in the bloodstream are destroyed prematurely, leading to hemolytic anemia. | Bartonella bacilliformis transmitted by the night-biting sand fly known as Lutzomyia (formerly Phlebotomus). |
| Trench fever | Fever is the predominant symptom, with isolated febrile episodes or four-to-five-day feverish episodes or two-to-six-week persistent febrile episodes. | Bartonella quintana is transmitted by contamination of a skin abrasion or louse-bite wound with the feces of an infected body louse (Pediculus humanus corporis). |
| Symptoms | Signs |
|---|---|
| Regional pain or body aches | Primary skin lesion that starts as a vesicle |
| Lymph nodes near the original scratch or bite can become swollen, tender, or painful | Regional unilateral lymphadenopathy |
| Prolonged fever | Rash |
| Fatigue | Lack of energy and tiredness |
| Loss of appetite | Weight loss |
| Sore throat | Regional signs of inflammation |
| Abdominal pain | Hepatomegaly and splenomegaly |
| Headaches | Encephalopathy |
| Joint pain | Unusual gait |
| Inflammatory | Vascular | Neurogenic |
|---|---|---|
| Endothelial cells and CD-34 hematopoietic progenitors Bartonella adhesin A facilitates attachment to extracellular matrix and mammalian host cells The type IV secretion system VirB/VirD4 is a critical virulence factor Trw-system, extra adhesins, and maybe filamentous hemagglutinins of alpha-, beta-, and gamma-proteobacteria are virulence factors | Arterial infections and vasoproliferative lesions B. henselae is quickly absorbed by endothelial cells in vitro, a mechanism mediated by actin B. henselae is quickly absorbed by endothelial cells in vitro, a mechanism mediated by actin B. henselae stimulates endothelial cell growth through VEGF release Bacterial proliferation results in the release of proinflammatory chemicals and growth regulators, and the cessation of apoptosis, which manifests as new lumps inside the vascular system | Circulating antibodies may induce an immune response by specifically damaging the blood–brain barrier Circulating pathogenic antibodies could enter the nervous system through the blood–brain barrier B. henselae may invade human brain vascular pericytes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurja, S.; Stroe, A.Z.; Pundiche, M.B.; Docu Axelerad, S.; Mateescu, G.; Micu, A.O.; Popescu, R.; Oltean, A.; Docu Axelerad, A. The Clinical Profile of Cat-Scratch Disease’s Neuro-Ophthalmological Effects. Brain Sci. 2022, 12, 217. https://doi.org/10.3390/brainsci12020217
Jurja S, Stroe AZ, Pundiche MB, Docu Axelerad S, Mateescu G, Micu AO, Popescu R, Oltean A, Docu Axelerad A. The Clinical Profile of Cat-Scratch Disease’s Neuro-Ophthalmological Effects. Brain Sciences. 2022; 12(2):217. https://doi.org/10.3390/brainsci12020217
Chicago/Turabian StyleJurja, Sanda, Alina Zorina Stroe, Mihaela Butcaru Pundiche, Silviu Docu Axelerad, Garofita Mateescu, Alexandru Octavian Micu, Raducu Popescu, Antoanela Oltean, and Any Docu Axelerad. 2022. "The Clinical Profile of Cat-Scratch Disease’s Neuro-Ophthalmological Effects" Brain Sciences 12, no. 2: 217. https://doi.org/10.3390/brainsci12020217
APA StyleJurja, S., Stroe, A. Z., Pundiche, M. B., Docu Axelerad, S., Mateescu, G., Micu, A. O., Popescu, R., Oltean, A., & Docu Axelerad, A. (2022). The Clinical Profile of Cat-Scratch Disease’s Neuro-Ophthalmological Effects. Brain Sciences, 12(2), 217. https://doi.org/10.3390/brainsci12020217