
Aβ42 as a Biomarker of Alzheimer’s Disease: Is Saliva a Viable Alternative to Cerebrospinal Fluid?
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Saliva Collection
2.3. CSF Collection
2.4. Statistical Analyses
3. Results
3.1. Overall Population
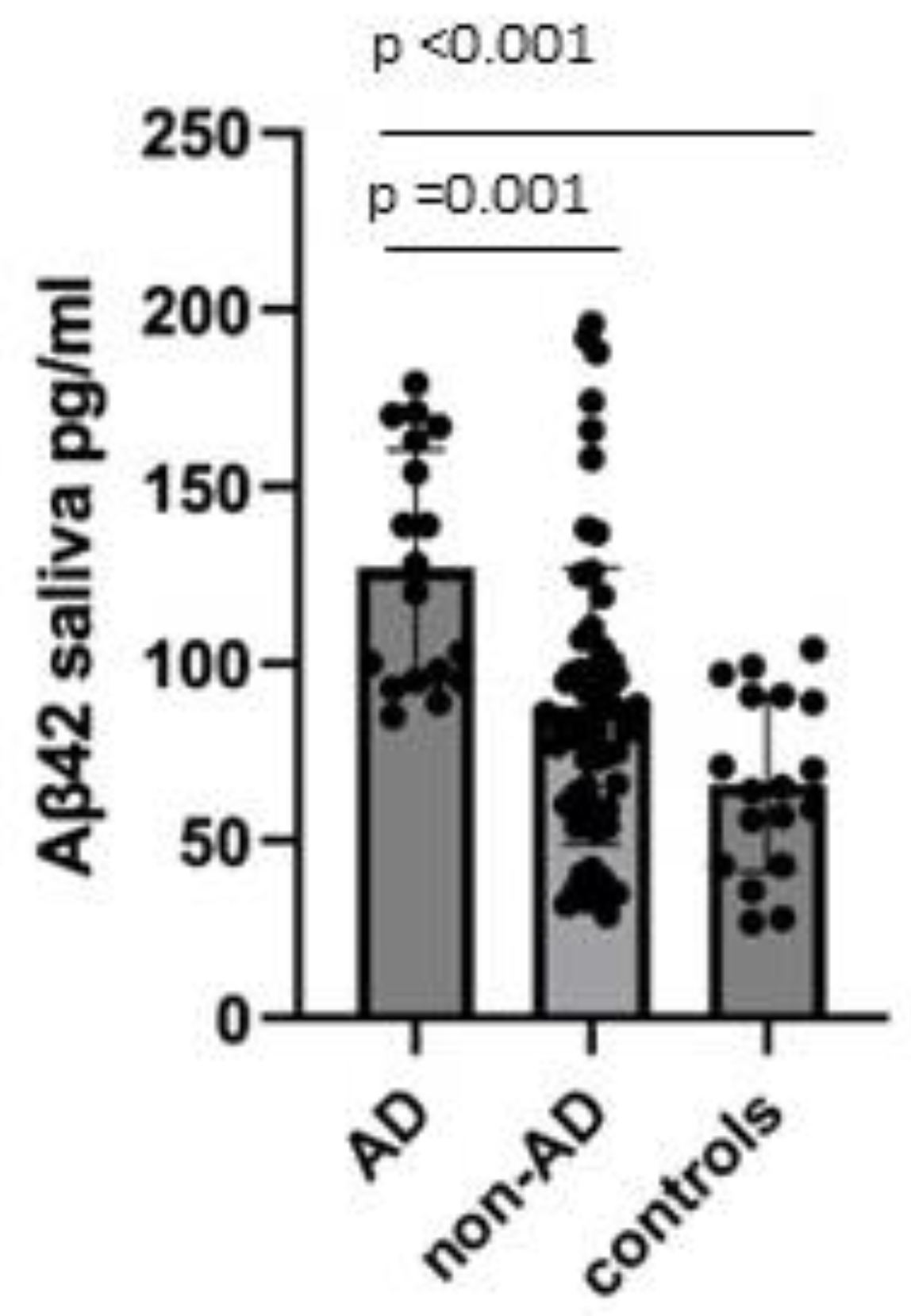
3.2. Analysis of Salivary Aβ42 Concentrations
3.3. Validation of Diagnostic Performance by the ROC Curve
3.4. Correlation between Salivary and Cerebrospinal Fluid Concentrations of Aβ42
3.5. Salivary Aβ42 and Clinical Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murphy, M.P.; LeVine, H. Alzheimer’s Disease and the β-Amyloid Peptide. J. Alzheimers Dis. 2010, 19, 311. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Pozo, A.; Frosch, M.P.; Masliah, E.; Hyman, B.T. Neuropathological Alterations in Alzheimer Disease. Cold Spring Harb. Perspect. Med. 2011, 1, a006189. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Ashton, N.J.; Ide, M.; Zetterberg, H.; Blennow, K. Salivary Biomarkers for Alzheimer’s Disease and Related Disorders. Neurol. Ther. 2019, 8 (Suppl. S2), 83–94. [Google Scholar] [CrossRef] [PubMed]
- Wolgin, M.; Zobernig, M.; Dvornyk, V.; Braun, R.J.; Kielbassa, A.M. Systematic Review on Saliva Biomarkers in Patients Diagnosed with Morbus Alzheimer and Morbus Parkinson. Biomedicines 2022, 10, 1702. [Google Scholar] [CrossRef]
- Bermejo-Pareja, F.; Antequera, D.; Vargas, T.; Molina, J.A.; Carro, E. Saliva levels of Abeta1-42 as potential biomarker of Alzheimer’s disease: A pilot study. BMC Neurol. 2010, 10, 108. [Google Scholar] [CrossRef]
- Cui, Y.; Zhang, H.; Zhu, J.; Liao, Z.; Wang, S.; Liu, W. Investigation of Whole and Glandular Saliva as a Biomarker for Alzheimer’s Disease Diagnosis. Brain Sci. 2022, 12, 595. [Google Scholar] [CrossRef]
- Kim, C.-B.; Choi, Y.Y.; Song, W.K.; Song, K.-B. Antibody-based magnetic nanoparticle immunoassay for quantification of Alzheimer’s disease pathogenic factor. J. Biomed. Opt. 2014, 19, 051205. [Google Scholar] [CrossRef]
- Tvarijonaviciute, A.; Zamora, C.; Ceron, J.J.; Bravo-Cantero, A.F.; Pardo-Marin, L.; Valverde, S.; Lopez-Jornet, P. Salivary Biomarkers in Alzheimer’s Disease. Clin. Oral. Investig. 2020, 24, 3437–3444. [Google Scholar] [CrossRef]
- Shi, M.; Sui, Y.-T.; Peskind, E.R.; Li, G.; Hwang, H.; Devic, I.; Ginghina, C.; Edgar, J.S.; Pan, C.; Goodlett, D.R.; et al. Salivary Tau Species are Potential Biomarkers of Alzheimer’s Disease. J. Alzheimers Dis. 2011, 27, 299–305. [Google Scholar] [CrossRef]
- Marksteiner, J.; Defrancesco, M.; Humpel, C. Saliva tau and phospho-tau-181 measured by Lumipulse in patients with Alzheimer’s disease. Front. Aging Neurosci. 2022, 14, 1014305. [Google Scholar] [CrossRef] [PubMed]
- Schöll, M.; Maass, A.; Mattsson, N.; Ashton, N.J.; Blennow, K.; Zetterberg, H.; Jagust, W. Biomarkers for Tau Pathology. Mol. Cell. Neurosci. 2019, 97, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Bălașa, A.F.; Chircov, C.; Grumezescu, A.M. Body Fluid Biomarkers for Alzheimer’s Disease—An Up-To-Date Overview. Biomedicines 2020, 8, 421. [Google Scholar] [CrossRef]
- Farah, R.; Haraty, H.; Salame, Z.; Fares, Y.; Ojcius, D.M.; Sadier, N.S. Salivary biomarkers for the diagnosis and monitoring of neurological diseases. Biomed. J. 2018, 41, 63–87. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Guo, J.-P.; Kennedy, K.; McGeer, E.G.; McGeer, P.L. A Method for Diagnosing Alzheimer’s Disease Based on Salivary Amyloid-β Protein 42 Levels. J. Alzheimers Dis. 2017, 55, 1175–1182. [Google Scholar] [CrossRef]
- Sabbagh, M.N.; Shi, J.; Lee, M.; Arnold, L.; Al-Hasan, Y.; Heim, J.; McGeer, P. Salivary beta amyloid protein levels are detectable and differentiate patients with Alzheimer’s disease dementia from normal controls: Preliminary findings. BMC Neurol. 2018, 18, 155. [Google Scholar] [CrossRef]
- François, M.; Fenech, M.F.; Thomas, P.; Hor, M.; Rembach, A.; Martins, R.N.; Rainey-Smith, S.R.; Masters, C.L.; Ames, D.; Rowe, C.C.; et al. The Australian Imaging Biomarkers and Lifestyle Study Research Group, null. High Content, Multi-Parameter Analyses in Buccal Cells to Identify Alzheimer’s Disease. Curr. Alzheimer Res. 2016, 13, 787–799. [Google Scholar] [CrossRef]
- Humpel, C. Identifying and validating biomarkers for Alzheimer’s disease. Trends Biotechnol. 2011, 29, 26–32. [Google Scholar] [CrossRef]
- Reuster, T.; Rilke, O.; Oehler, J. High correlation between salivary MHPG and CSF MHPG. Psychopharmacology 2002, 162, 415–418. [Google Scholar] [CrossRef]
- Ship, J.A.; Decarli, C.; Friedland, R.P.; Baum, B.J. Diminished Submandibular Salivary Flow in Dementia of the Alzheimer Type. J. Gerontol. 1990, 45, M61–M66. [Google Scholar] [CrossRef]
- Mattsson, N.; Lönneborg, A.; Boccardi, M.; Blennow, K.; Hansson, O.; Geneva Task Force for the Roadmap of Alzheimer’s Biomarkers. Clinical Validity of Cerebrospinal Fluid Aβ42, Tau, and Phospho-Tau as Biomarkers for Alzheimer’s Disease in the Context of a Structured 5-Phase Development Framework. Neurobiol. Aging 2017, 52, 196–213. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Characteristics | AD | non-AD | Controls | p-Value | p-Value after the Bonferroni Correction |
|---|---|---|---|---|---|
| Gender M/F (%) | 8/10 (44/56) | 30/34 (44/56) | 7/11 (39/61) | 0.843 | - |
| Age (years ±SD) | 72.13 ± 5.45 | 69.34 ± 7.48 | 65.67 ± 12.02 | 0.08 | - |
| Disease duration (years ±SD) | 2.83 ± 2.28 | 2.65 ± 2.88 | - | 0.79 | - |
| MMSE (±SD) | 22.47 ± 3.78 | 23.66 ± 3.95 | - | 0.34 | - |
| CSF and saliva biomarkers | AD | non-AD | Controls | p-Value | p-Value after the Bonferroni correction |
| t-tau [pg/mL] (±SD) | 299.50 ± 317.12 | 157.48 ± 144.94 | 86.83 ± 65.75 | 0.002 ** | AD vs. non-AD 0.011 * AD vs. Controls 0.002 ** |
| p-tau [pg/mL] (±SD) | 60.11 ± 43.53 | 40.8 ± 40.86 | 26.28 ± 12.80 | 0.025 * | AD vs. non-AD 0.18 AD vs. Controls 0.027 * |
| Aβ42 CSF [pg/mL] (±SD) | 454.39 ± 51.86 | 903.28 ± 311.60 | 1127.61 ± 358.85 | 0.000 *** | AD vs. non-AD <0.001 *** AD vs. Controls <0.001 *** |
| Aβ42 saliva [pg/mL] (±SD) | 127.11 ± 33.44 | 88.03 ± 39.04 | 66.11 ± 24.82 | 0.000 *** | AD vs. non-AD <0.001 *** AD vs. Controls <0.001 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boschi, S.; Roveta, F.; Grassini, A.; Marcinnò, A.; Cermelli, A.; Ferrandes, F.; Rainero, I.; Rubino, E. Aβ42 as a Biomarker of Alzheimer’s Disease: Is Saliva a Viable Alternative to Cerebrospinal Fluid? Brain Sci. 2022, 12, 1729. https://doi.org/10.3390/brainsci12121729
Boschi S, Roveta F, Grassini A, Marcinnò A, Cermelli A, Ferrandes F, Rainero I, Rubino E. Aβ42 as a Biomarker of Alzheimer’s Disease: Is Saliva a Viable Alternative to Cerebrospinal Fluid? Brain Sciences. 2022; 12(12):1729. https://doi.org/10.3390/brainsci12121729
Chicago/Turabian StyleBoschi, Silvia, Fausto Roveta, Alberto Grassini, Andrea Marcinnò, Aurora Cermelli, Fabio Ferrandes, Innocenzo Rainero, and Elisa Rubino. 2022. "Aβ42 as a Biomarker of Alzheimer’s Disease: Is Saliva a Viable Alternative to Cerebrospinal Fluid?" Brain Sciences 12, no. 12: 1729. https://doi.org/10.3390/brainsci12121729
APA StyleBoschi, S., Roveta, F., Grassini, A., Marcinnò, A., Cermelli, A., Ferrandes, F., Rainero, I., & Rubino, E. (2022). Aβ42 as a Biomarker of Alzheimer’s Disease: Is Saliva a Viable Alternative to Cerebrospinal Fluid? Brain Sciences, 12(12), 1729. https://doi.org/10.3390/brainsci12121729