

Effects of Aerobic Exercise on Markers of Brain Injury in Methamphetamine-Dependent Individuals: A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Experimental Design
2.3. Study Subjects
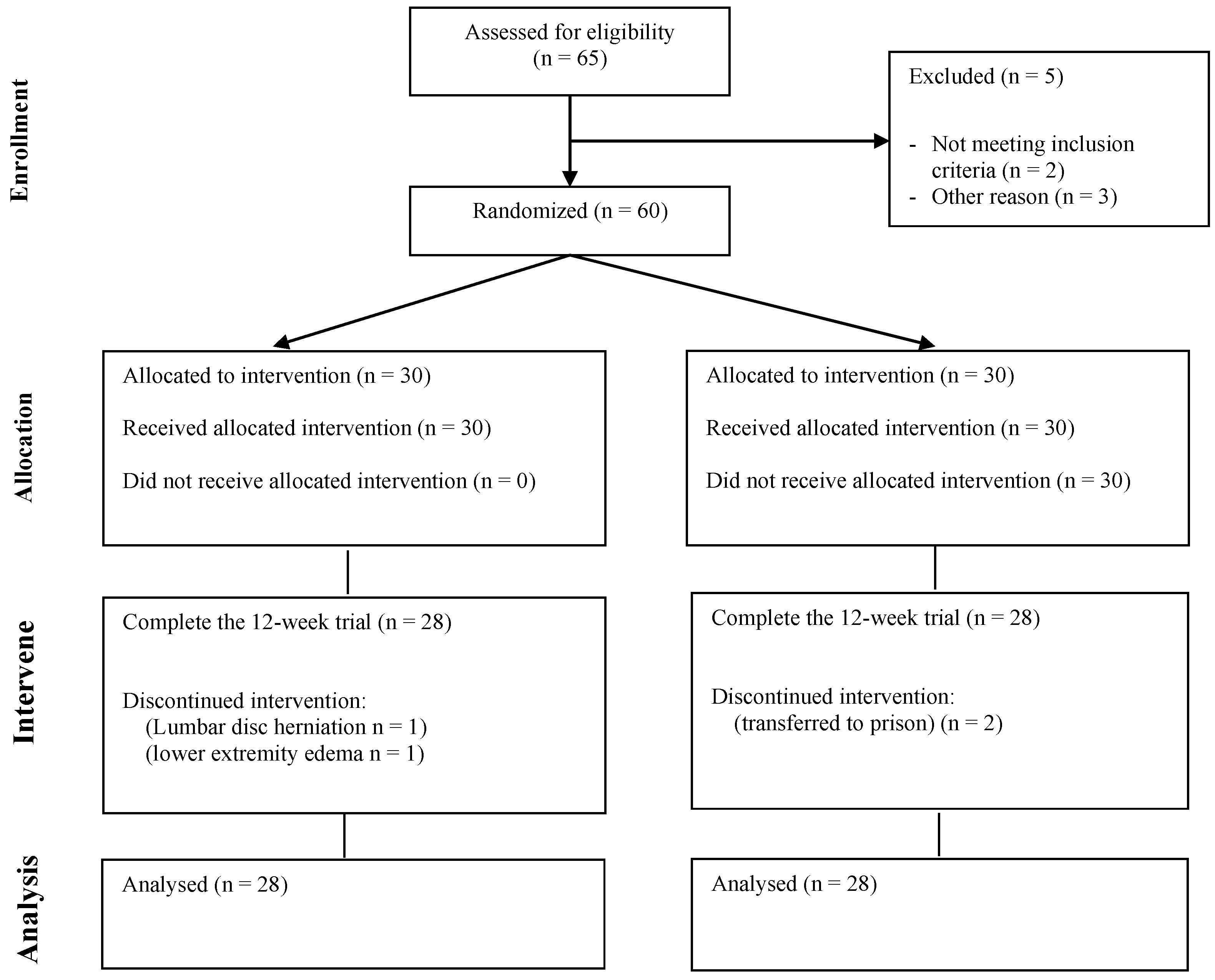
2.3.1. Recruitment and Grouping of Study Subjects
2.3.2. Inclusion and Exclusion Criteria
2.4. Exercise Intervention Program
2.5. Exercise Intervention Program
2.6. Statistical Analysis
3. Results
3.1. Baseline Conditions of Subjects
3.2. Changes in Serum NSE and S100b among Subjects before and after Aerobic Exercise Intervention
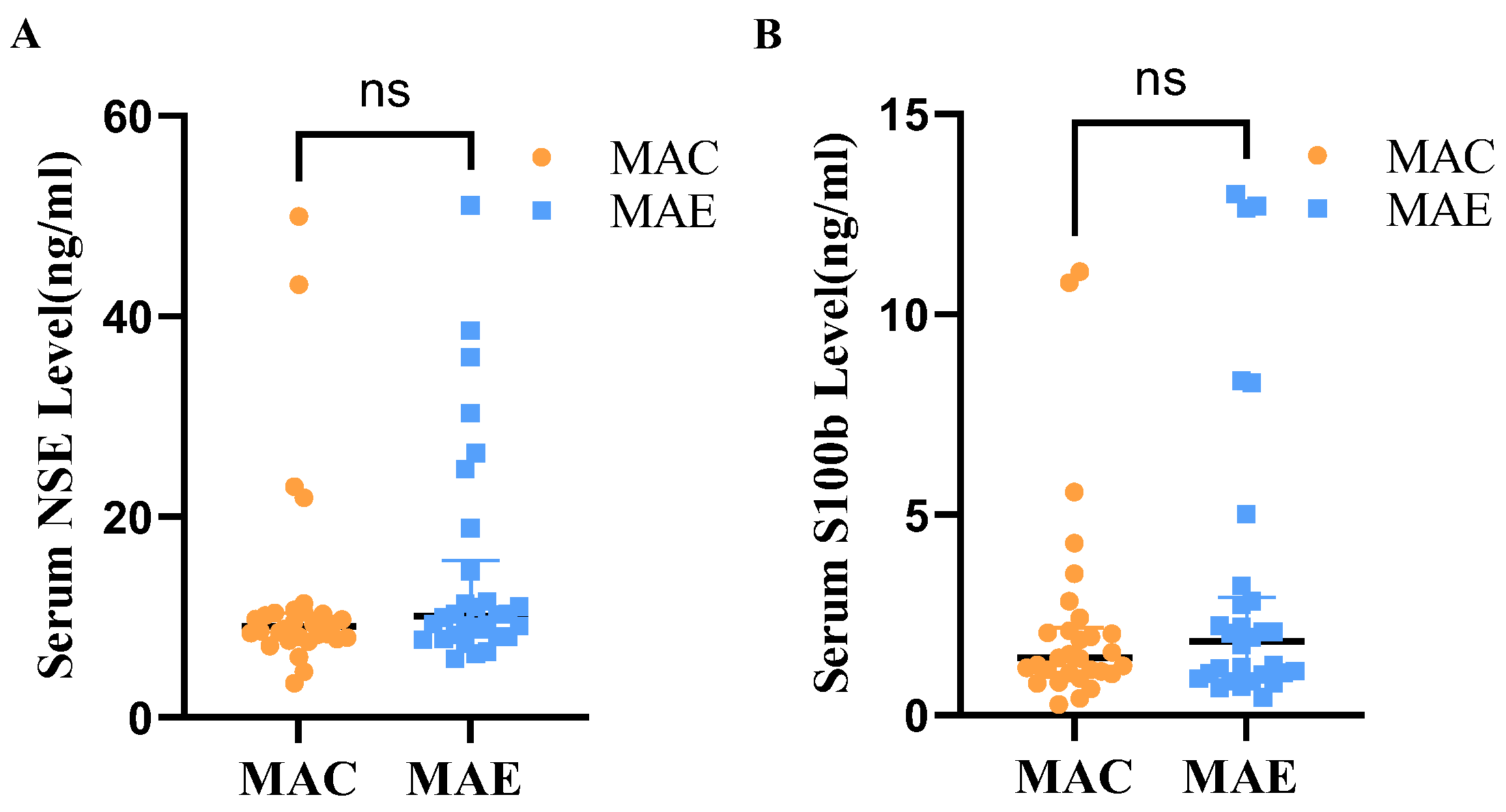
3.2.1. Serum NSE and S100b Levels among Subjects before Aerobic Exercise Intervention
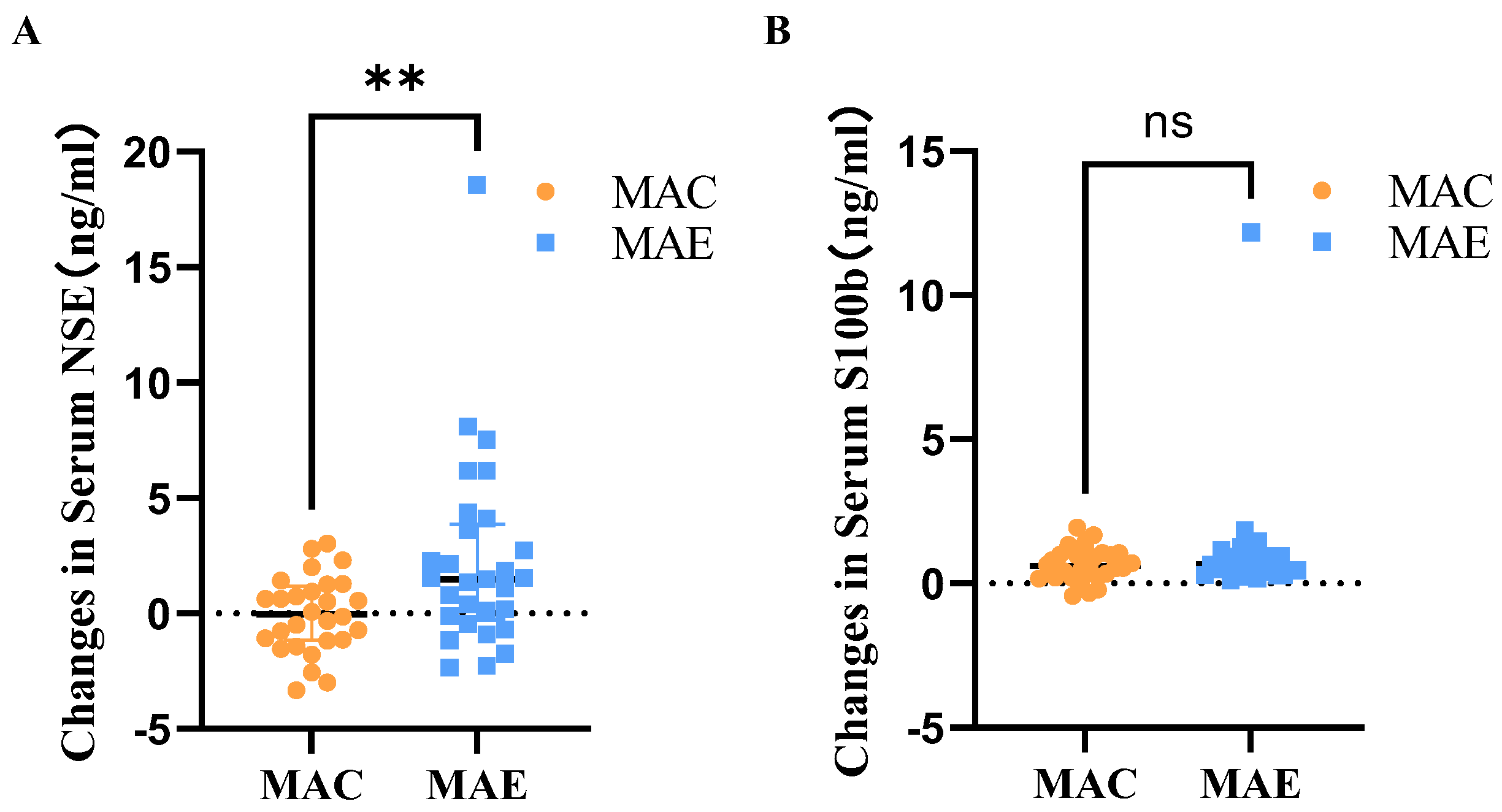
3.2.2. Serum NSE and S100b Levels among Subjects before and after Aerobic Exercise Intervention
3.3. Plasma NfL Changes in Subjects before and after Aerobic Exercise Intervention
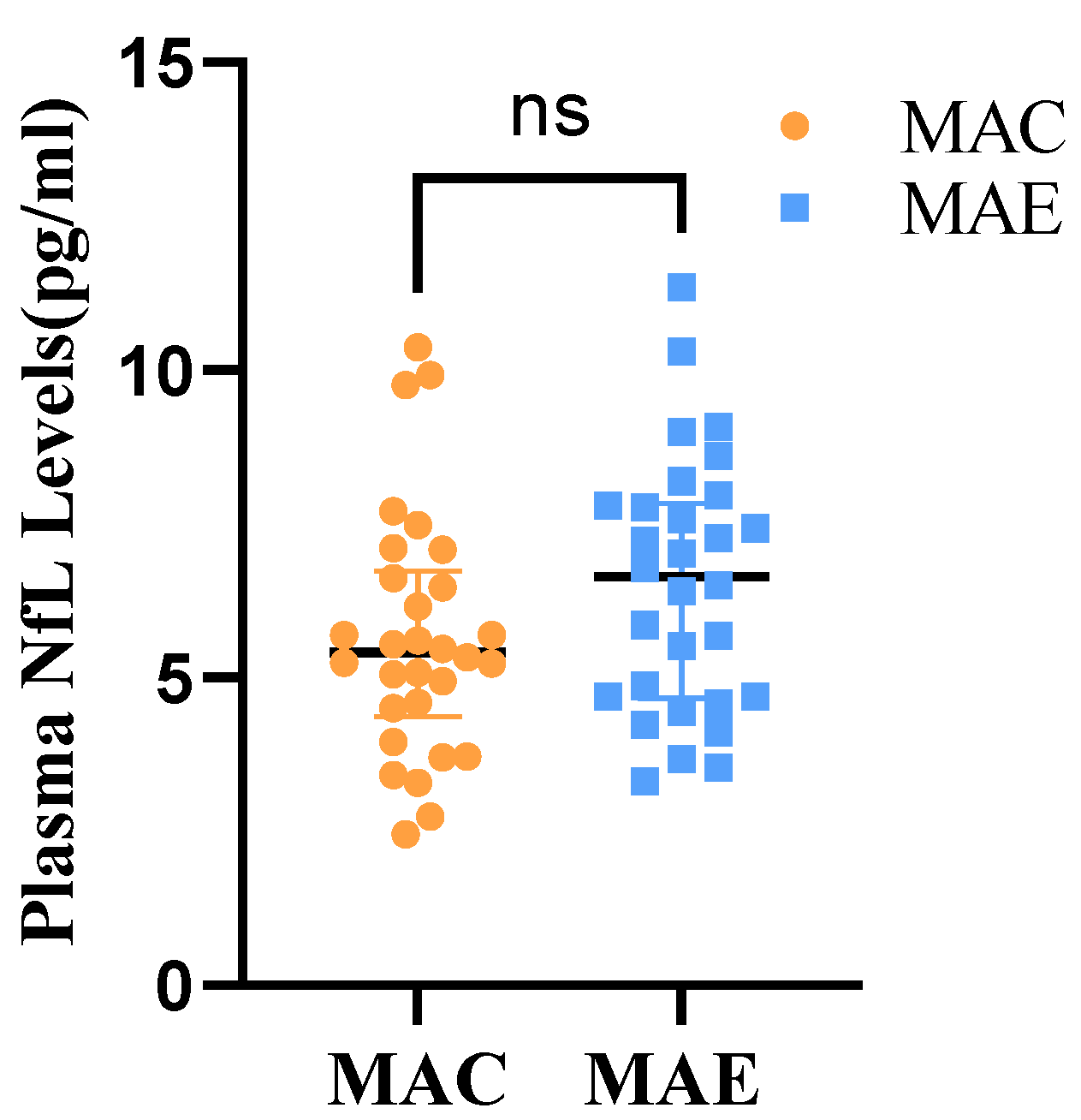
3.3.1. Plasma NfL Levels in Subjects before Aerobic Exercise Intervention
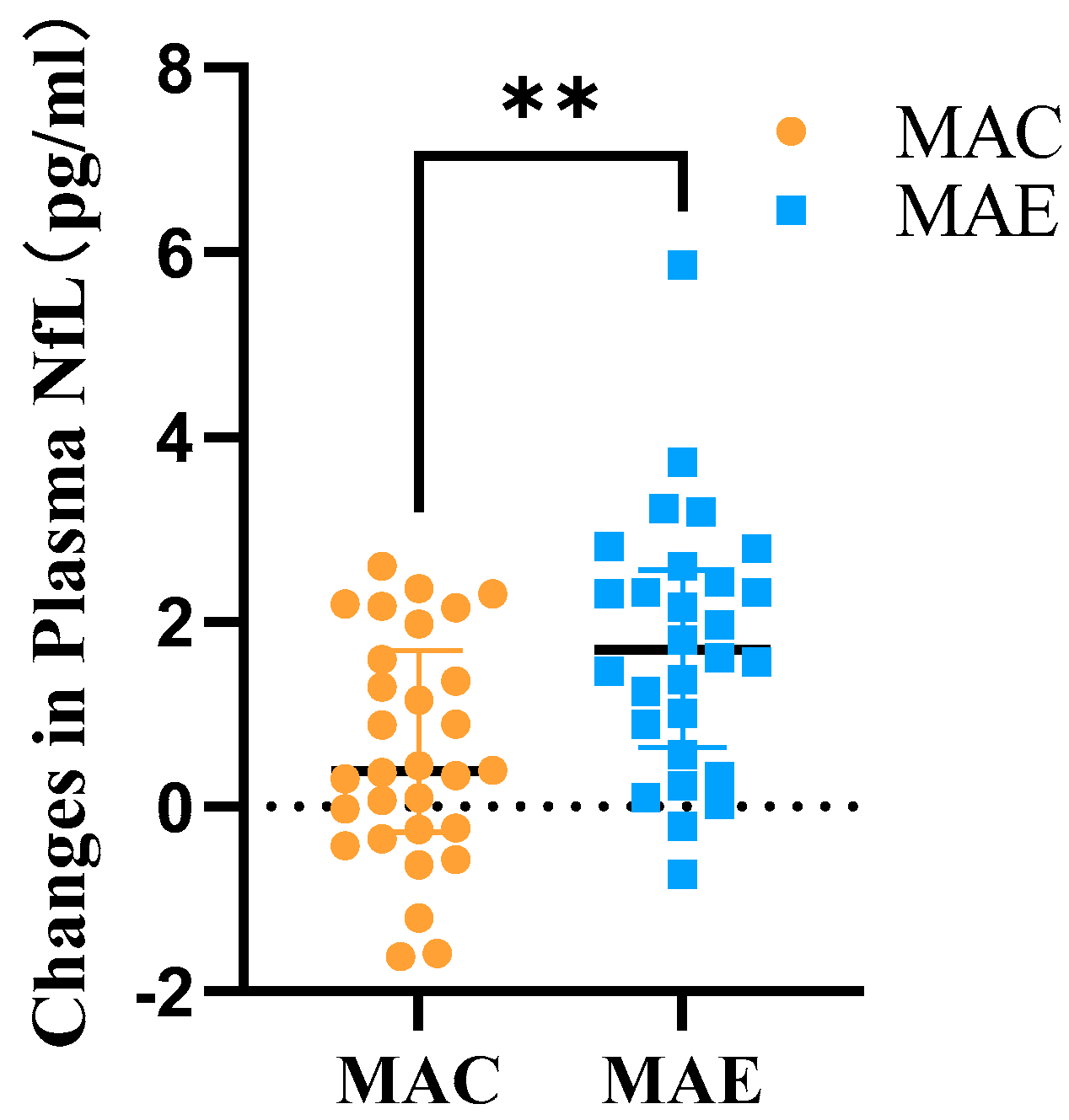
3.3.2. Plasma NfL Differences in Subjects before and after Exercise Intervention
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNODC. World Drug Report. 2021. Available online: https://www.unodc.org/unodc/en/data-and-alysis/wdr-2021_booklet-2.html (accessed on 1 July 2022).
- Qie, X.; Wen, D.; Guo, H.; Xu, G.; Liu, S.; Shen, Q.; Liu, Y.; Zhang, W.; Cong, B.; Ma, C. Endoplasmic Reticulum Stress Mediates Methamphetamine-Induced Blood–Brain Barrier Damage. Front. Pharmacol. 2017, 8, 639. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, S.; Daiwile, A.P.; Cadet, J.L. Neurotoxicity of methamphetamine: Main effects and mechanisms. Exp. Neurol. 2021, 344, 113795. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Kim, H.J.; Lim, B.; Wylegala, A.; Toborek, M. Methamphetamine-Induced Occludin Endocytosis Is Mediated by the Arp2/3 Complex-Regulated Actin Rearrangement. J. Biol. Chem. 2013, 288, 33324–33334. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; He, J.T.; Zhang, K.K.; Chen, L.J.; Wang, Q.; Xie, X.L. Methamphetamine Reduces Expressions of Tight Junction Proteins, Rearranges F-Actin Cytoskeleton and Increases the Blood Brain Barrier Permeability Via the Rhoa/Rock-Dependent Pathway. Biochem. Biophys. Res. Commun. 2019, 509, 395–401. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The Blood-Brain Barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef]
- Toborek, M.; Seelbach, M.J.; Choi, Y.J.; András, I.E.; Chen, L.; Hennig, B.; Esser, K.A. Voluntary exercise protects against methamphetamine-induced oxidative stress in brain microvasculature and disruption of the blood-brain barrier. FASEB J. 2009, 23, 1020.7. [Google Scholar] [CrossRef]
- Koob, G.F.; Le Moal, M. Drug Addiction, Dysregulation of Reward, and Allostasis. Neuropsychopharmacology 2001, 24, 97–129. [Google Scholar] [CrossRef]
- Northrop, N.A.; Yamamoto, B.K. Methamphetamine Effects on Blood-Brain Barrier Structure and Function. Front. Neurosci. 2015, 9, 69. [Google Scholar] [CrossRef]
- Morais, A.P.D.; Pita, I.R.; Ribeiro, C.F.; Pereira, F.C. The neurobiological mechanisms of physical exercise in methamphetamine addiction. CNS Neurosci. Ther. 2017, 24, 85–97. [Google Scholar] [CrossRef]
- Park, M.; Levine, H.; Toborek, M. Exercise protects against methamphetamine-induced aberrant neurogenesis. Sci. Rep. 2016, 6, srep34111. [Google Scholar] [CrossRef]
- Huang, J.; Zheng, Y.; Gao, D.; Hu, M.; Yuan, T. Effects of Exercise on Depression, Anxiety, Cognitive Control, Craving, Physical Fitness and Quality of Life in Methamphetamine-Dependent Patients. Front. Psychiatry 2020, 10, 999. [Google Scholar] [CrossRef]
- Wang, D.; Zhou, C.; Zhao, M.; Wu, X.; Chang, Y.-K. Dose–response relationships between exercise intensity, cravings, and inhibitory control in methamphetamine dependence: An ERPs study. Drug Alcohol Depend. 2016, 161, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Rawson, R.A.; Chudzynski, J.; Gonzales, R.; Mooney, L.; Dickerson, D.; Ang, A.; Dolezal, B.; Cooper, C.B. The Impact of Exercise On Depression and Anxiety Symptoms Among Abstinent Methamphetamine-Dependent Individuals in A Residential Treatment Setting. J. Subst. Abus. Treat. 2015, 57, 36–40. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Chudzynski, J.; Storer, T.W.; Abrazado, M.; Penate, J.; Mooney, L.; Dickerson, D.; Rawson, R.A.; Cooper, C.B. Eight Weeks of Exercise Training Improves Fitness Measures in Methamphetamine-Dependent Individuals in Residential Treatment. J. Addict. Med. 2013, 7, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Dolezal, B.A.; Chudzynski, J.; Dickerson, D.; Mooney, L.; Rawson, R.A.; Garfinkel, A.; Cooper, C.B. Exercise Training Improves Heart Rate Variability after Methamphetamine Dependency. Med. Sci. Sports Exerc. 2014, 46, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.A. Neurofilaments in Disease: What Do We Know? Curr. Opin. Neurobiol. 2020, 61, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Barro, C.; Chitnis, T.; Weiner, H.L. Blood neurofilament light: A critical review of its application to neurologic disease. Ann. Clin. Transl. Neurol. 2020, 7, 2508–2523. [Google Scholar] [CrossRef]
- Alirezaei, Z.; Pourhanifeh, M.H.; Borran, S.; Nejati, M.; Mirzaei, H.; Hamblin, M.R. Neurofilament Light Chain as a Biomarker, and Correlation with Magnetic Resonance Imaging in Diagnosis of CNS-Related Disorders. Mol. Neurobiol. 2019, 57, 469–491. [Google Scholar] [CrossRef]
- Yun, G.S.; In, Y.N.; Kang, C.; Park, J.S.; You, Y.; Min, J.H.; Ahn, H.J.; Yoo, I.; Kim, S.W.; Oh, S.K.; et al. Development of a strategy for assessing blood-brain barrier disruption using serum S100 calcium-binding protein B and neuron-specific enolase in early stage of neuroemergencies: A preliminary study. Medicine 2022, 101, e29644. [Google Scholar] [CrossRef]
- Roh, H.T.; So, W.Y. The Effects of Aerobic Exercise Training on Oxidant-Antioxidant Balance, Neurotrophic Factor Levels, and Blood-Brain Barrier Function in Obese and Non-Obese Men. J. Sport Health Sci. 2017, 6, 447–453. [Google Scholar] [CrossRef]
- Roh, H.-T.; Cho, S.-Y.; Yoon, H.-G.; So, W.-Y. Effect of Exercise Intensity on Neurotrophic Factors and Blood–Brain Barrier Permeability Induced by Oxidative–Nitrosative Stress in Male College Students. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 239–246. [Google Scholar] [CrossRef]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P. Consort Statement for Randomized Trials of Nonphar-macologic Treatments: A 2017 Update and a Consort Extension for Nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, J.; Leitão, R.A.; Higuera-Matas, A.; Assis, M.A.; Coria, S.M.; Fontes-Ribeiro, C.; Ambrosio, E.; Silva, A.P. Extended-Access Methamphetamine Self-Administration Elicits Neuroinflammatory Response Along with Blood-Brain Barrier Breakdown. Brain Behav. Immun. 2017, 62, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Castellano, P.; Nwagbo, C.; Martinez, L.R.; Eugenin, E.A. Methamphetamine Compromises Gap Junctional Communi-cation in Astrocytes and Neurons. J. Neurochem. 2016, 137, 561–575. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, C.; Zheng, L.; Zhang, J. Peripheral Inflammatory Biomarkers of Methamphetamine Withdrawal Patients Based on the Neuro-Inflammation Hypothesis: The Possible Improvement Effect of Exercise. Front. Psychiatry 2021, 12, 795073. [Google Scholar] [CrossRef]
- Li, Y.; Re, G.-F.; Zhao, Y.; Wu, X.-C.; Zhou, R.-Y.; Kuang, Y.-Q.; Wang, K.-H. Long-term exercise at different intensities can reduce the inflammatory response in the brains of methamphetamine-treated mice. Biochem. Biophys. Res. Commun. 2022, 613, 201–206. [Google Scholar] [CrossRef]
- Ramirez, S.; Potula, R.; Fan, S.; Eidem, T.; Papugani, A.; Reichenbach, N.; Dykstra, H.; Weksler, B.B.; Romero, I.; Couraud, P.O.; et al. Methamphetamine Disrupts Blood–Brain Barrier Function by Induction of Oxidative Stress in Brain Endothelial Cells. J. Cereb. Blood Flow Metab. 2009, 29, 1933–1945. [Google Scholar] [CrossRef]
- Robertson, C.L.; Ishibashi, K.; Chudzynski, J.; Mooney, L.J.; Rawson, R.A.; Dolezal, B.A.; Cooper, C.B.; Brown, A.K.; Mandelkern, M.A.; London, E.D. Effect of Exercise Training on Striatal Dopamine D2/D3 Receptors in Methamphetamine Users During Behavioral Treatment. Neuropsychopharmacology 2016, 41, 1629–1636. [Google Scholar] [CrossRef]
- Mandyam, C.D.; Wee, S.; Eisch, A.; Richardson, H.N.; Koob, G.F. Methamphetamine Self-Administration and Voluntary Exercise Have Opposing Effects on Medial Prefrontal Cortex Gliogenesis. J. Neurosci. 2007, 27, 11442–11450. [Google Scholar] [CrossRef]
- Morales, A.; Lee, B.; Hellemann, G.; O’Neill, J.; London, E.D. Gray-matter volume in methamphetamine dependence: Cigarette smoking and changes with abstinence from methamphetamine. Drug Alcohol Depend. 2012, 125, 230–238. [Google Scholar] [CrossRef]
- Chang, L.; Cloak, C.; Patterson, K.; Grob, C.; Miller, E.; Ernst, T. Enlarged striatum in abstinent methamphetamine abusers: A possible compensatory response. Biol. Psychiatry 2005, 57, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Ruan, X.; Zhong, N.; Yang, Z.; Fan, X.; Zhuang, W.; Du, J.; Jiang, H.; Zhao, M. Gray Matter Volume Showed Dynamic Al-terations in Methamphetamine Users at 6 and 12 months Abstinence: A Longitudinal Voxel-Based Morphometry Study. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 81, 350–355. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | MAC (n = 30) | MAE (n = 30) | Z/t | p | |
|---|---|---|---|---|---|
| Age | 33.90 ± 4.12 | 32.97 ± 4.16 | 0.872 | 0.387 | |
| Height | 168.96 ± 6.60 | 169.26 ± 4.45 | −0.394 | 0.693 | |
| Weight | 70.54 ± 8.90 | 68.14 ± 8.51 | −1.146 | 0.143 | |
| DSM-V | Mild | 7 (23.3%) | 8 (26.7%) | −0.205 | 0.838 |
| Moderate | 13 (43.3%) | 10 (33.3%) | |||
| Severe | 10 (33.3%) | 12 (40%) | |||
| educational level | primary school | 9 (30%) | 10 (33.3%) | 0.480 | 0.631 |
| junior high school | 12 (40%) | 13 (43.3%) | |||
| High School and Secondary School | 8 (26.7%) | 6 (20%) | |||
| College and above | 1 (3.4%) | 1 (3.4%) | |||
| drug use time | 109.64 ± 43.59 | 109.97 ± 56.23 | −0.024 | 0.981 | |
| C | <0.1 g | 7 (23.3%) | 4 (13.3%) | 0.480 | 0.631 |
| 0.1–0.3 g | 12 (40.0%) | 8 (26.7%) | |||
| 0.4–1.0 g | 10 (33.3%) | 16 (53.3%) | |||
| >1.0 g | 1 (3.3%) | 2 (6.7%) | |||
| Number of compulsory isolation and detoxification | The first time | 24 (80.0%) | 22 (73.3%) | −0.664 | 0.506 |
| The second time | 6 (20.0%) | 7 (23.3%) | |||
| The third time | 0 (0%) | 1 (1.7%) | |||
| Group | MAC (n = 30) | MAE (n = 30) | Z | p |
|---|---|---|---|---|
| NSE (ng/mL) | 9.08 (7.93~10.43) | 10.12 (8.09~15.65) | −1.242 | 0.214 |
| S100B (ng/mL) | 1.43 (1.05~2.19) | 1.85 (1.00~2.94) | −0.517 | 0.605 |
| Markers | Group | after Exercise | Difference | Z | p |
|---|---|---|---|---|---|
| NSE (ng/mL) | MAC (n = 28) | 12.51 ± 10.67 | 0.03 (−1.18~1.16) | −2.586 | 0.010 |
| MAE (n = 28) | 12.55 ± 11.02 | −1.51 (−3.99~0.31) ** | |||
| S100B (ng/mL) | MAC (n = 28) | 1.77 ± 2.67 | 0.60 (0.21~1.04) | −0.503 | 0.615 |
| MAE (n = 28) | 2.13 ± 3.36 | 0.66 (0.40~0.95) |
| Group | MAC (n = 30) | MAE (n = 30) | t | p | 95 CI |
|---|---|---|---|---|---|
| NfL (pg/mL) | 5.66 ± 1.99 | 6.52 ± 2.07 | −1.630 | 0.109 | −1.901~1.945 |
| Group | after Exercise | Difference | t | p |
|---|---|---|---|---|
| MAC (n = 28) | 5.06 ± 1.74 | 0.60 ± 1.21 | −3.348 | 0.001 |
| MAE (n = 28) | 4.85 ± 1.70 | 1.75 ± 1.40 *** |
| Markers | Group | after Exercise | Difference | Z | p |
|---|---|---|---|---|---|
| NfL (pg/mL) | MAC | 5.06 ± 1.72 | 0.38 (−0.24~1.60) | −7.600 | 0.001 |
| MAE | 4.77 ± 1.69 | 1.80 (0.81~2.60) *** | |||
| NSE (ng/mL) | MAC | 12.24 ± 10.32 | −0.14 (−1.24~1.03) | −6.940 | 0.001 |
| MAE | 12.33 ± 10.79 | 1.49 (−0.11~4.08) *** | |||
| S100b (ng/mL) | MAC | 1.70 ± 2.58 | 0.55 (0.21~1.02) | −1.956 | 0.051 |
| MAE | 2.06 ± 3.30 | 0.66 (0.41~1.05) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Z.; Xu, J.; Jin, Y.; Wang, L.; Li, X. Effects of Aerobic Exercise on Markers of Brain Injury in Methamphetamine-Dependent Individuals: A Randomized Controlled Trial. Brain Sci. 2022, 12, 1521. https://doi.org/10.3390/brainsci12111521
Zhu Z, Xu J, Jin Y, Wang L, Li X. Effects of Aerobic Exercise on Markers of Brain Injury in Methamphetamine-Dependent Individuals: A Randomized Controlled Trial. Brain Sciences. 2022; 12(11):1521. https://doi.org/10.3390/brainsci12111521
Chicago/Turabian StyleZhu, Zhicheng, Jisheng Xu, Yu Jin, Lu Wang, and Xue Li. 2022. "Effects of Aerobic Exercise on Markers of Brain Injury in Methamphetamine-Dependent Individuals: A Randomized Controlled Trial" Brain Sciences 12, no. 11: 1521. https://doi.org/10.3390/brainsci12111521
APA StyleZhu, Z., Xu, J., Jin, Y., Wang, L., & Li, X. (2022). Effects of Aerobic Exercise on Markers of Brain Injury in Methamphetamine-Dependent Individuals: A Randomized Controlled Trial. Brain Sciences, 12(11), 1521. https://doi.org/10.3390/brainsci12111521