
Clinical Utility of Eye Tracking in Assessing Distractibility in Children with Neurological Disorders or ADHD: A Cross-Sectional Study

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
Inclusion and Exclusion Criteria
2.2. Measurements and Procedures
2.2.1. Measurement of Parent-Reported Attention Problems
2.2.2. ADHD Diagnosis
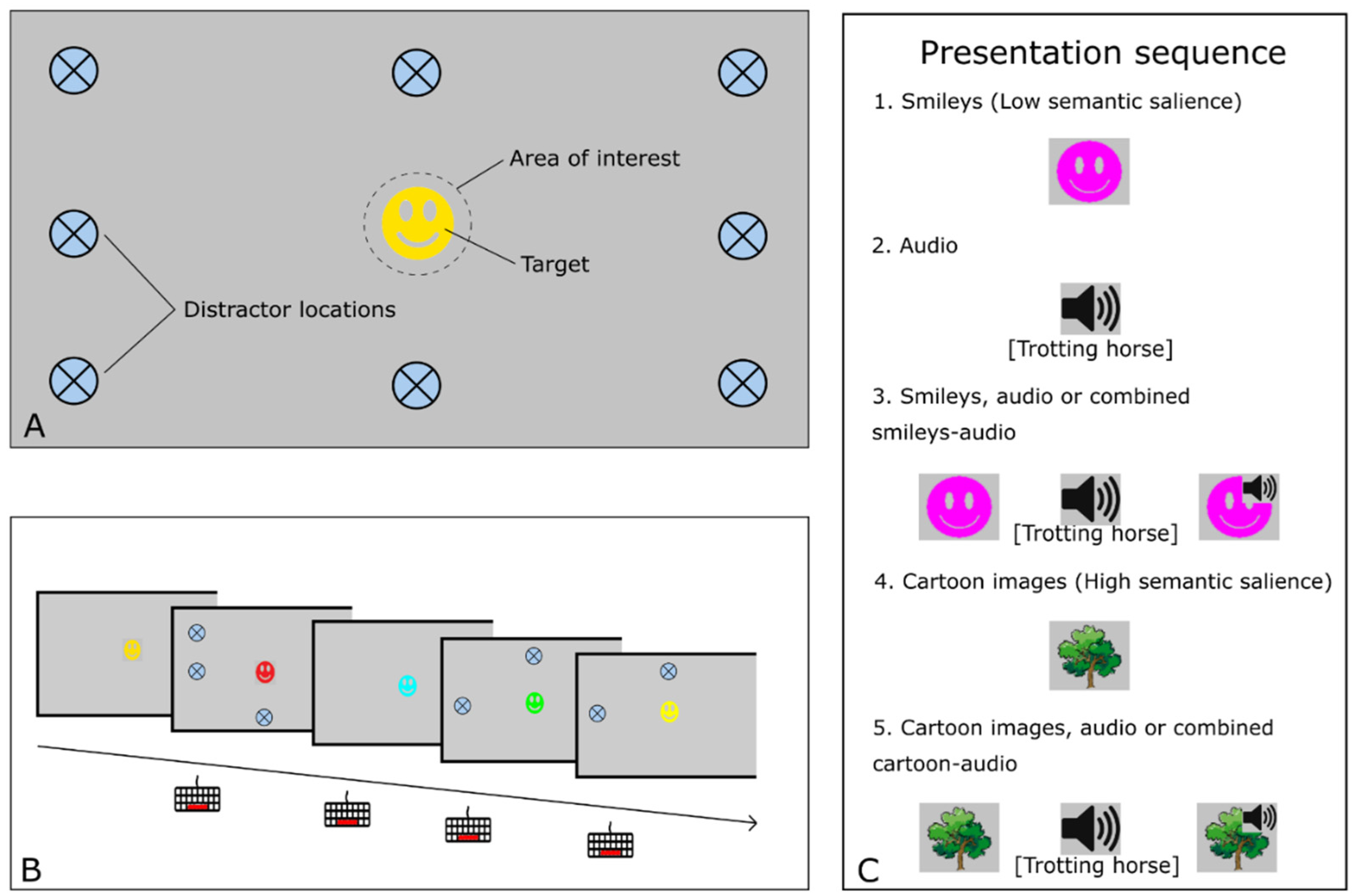
2.2.3. The IDistrack Measurement Setup
2.2.4. The IDistrack Task
2.3. Data Analysis and Statistics
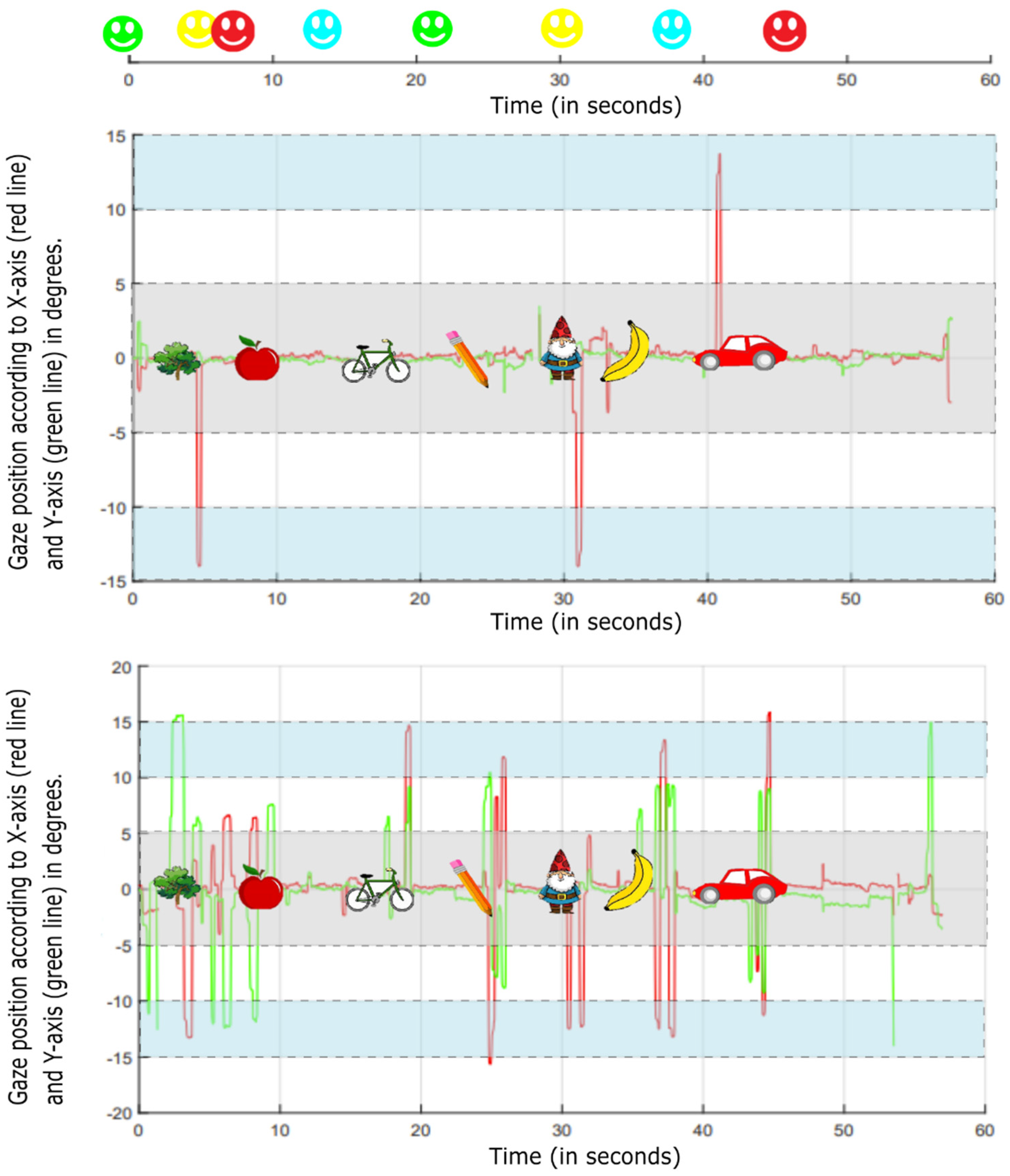
2.3.1. Area of Interest and Post-Calibration of the Gaze Data
2.3.2. Feature Calculation
2.3.3. Statistical Analysis
3. Results
3.1. Inclusion Criteria for Statistical Analysis
3.2. Homogeneity of Subgroups
3.3. IDistrack Outcome Measures in Relation to a Clinical ADHD Diagnosis
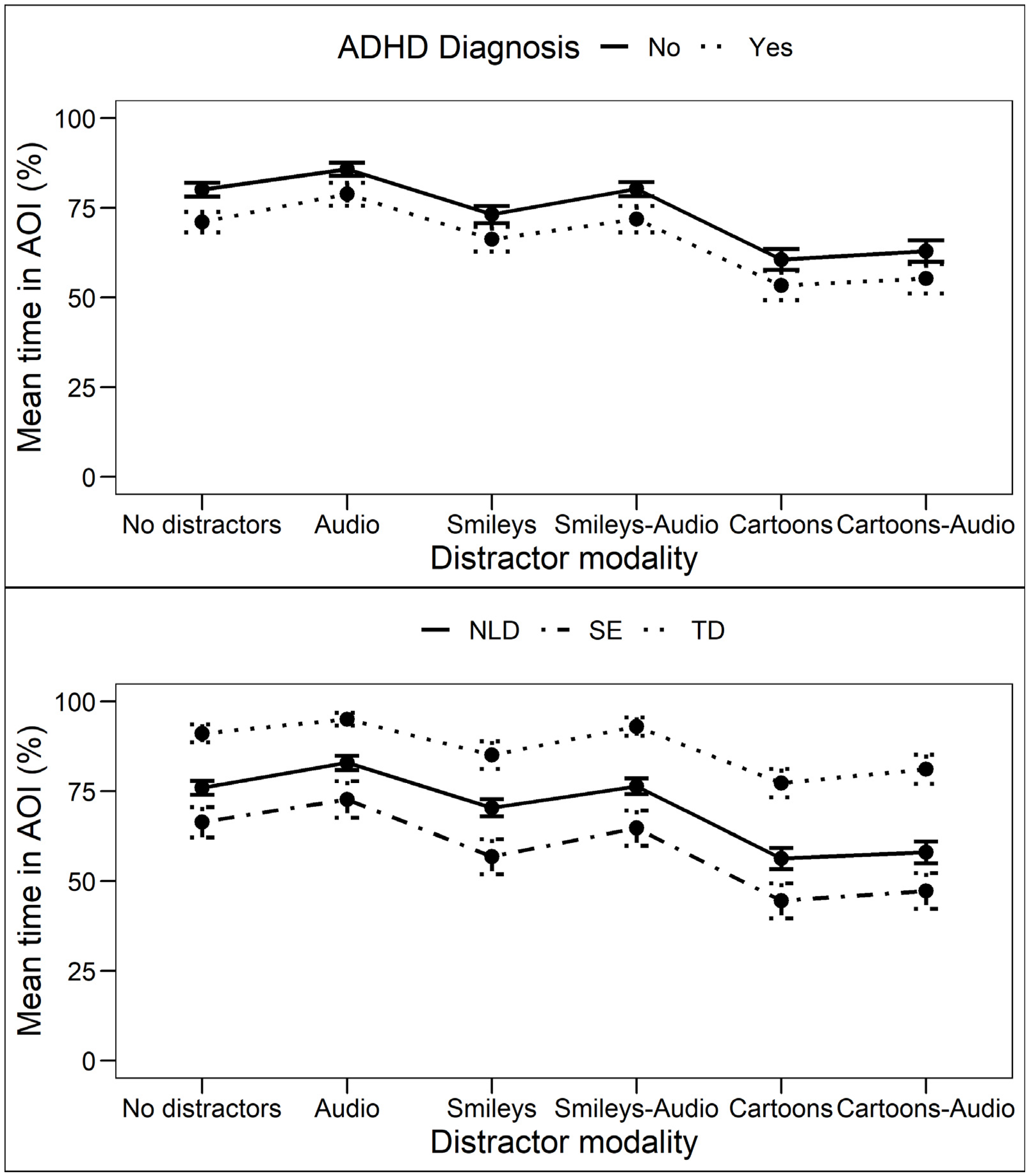
3.3.1. Time in Area of Interest (tAOI)
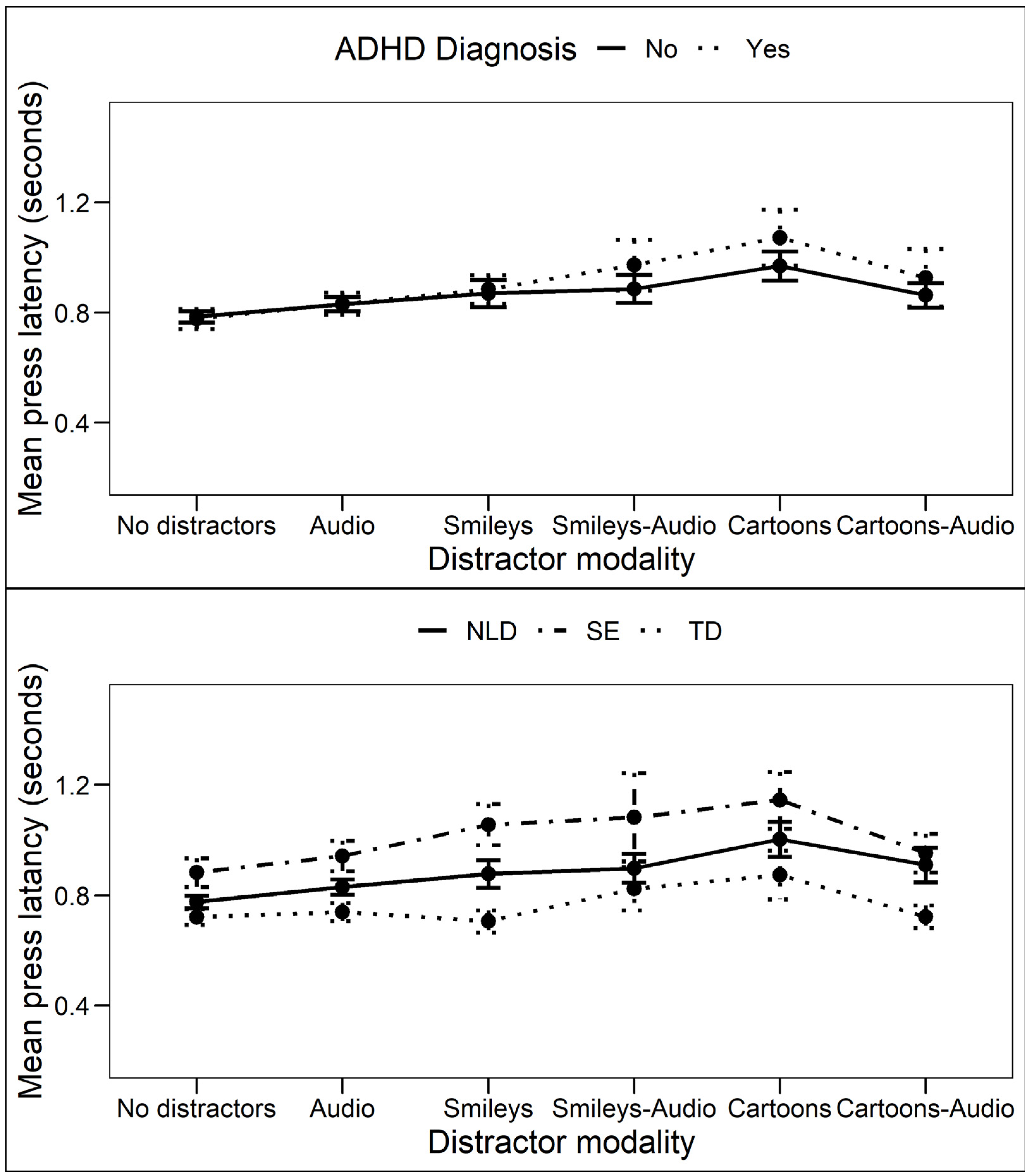
3.3.2. Press Latencies (PL)
3.4. IDistrack Outcome Measures in Relation to Neurological Disorder
3.4.1. Time in Area of Interest (tAOI)
3.4.2. Press Latencies (PL)
3.5. Correlation of Eye Movement Responses with Parent-Reported Attention Problems
4. Discussion
4.1. Limitations
4.2. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hendriksen, J.G.; Peijnenborgh, J.C.; Aldenkamp, A.P.; Vles, J.S. Diagnostic Overshadowing in a Population of Children with Neurological Disabilities: A Cross Sectional Descriptive Study on Acquired ADHD. Eur. J. Paediatr. Neurol. 2015, 19, 521–524. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association, D.S.; Association, A.P. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Forster, S.; Lavie, N. Establishing the Attention-Distractibility Trait. Psychol. Sci. 2016, 27, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Meier, M.E. Testing the Attention-Distractibility Trait. Mem. Cogn. 2021, 49, 1490–1504. [Google Scholar] [CrossRef] [PubMed]
- Cassuto, H.; Ben-Simon, A.; Berger, I. Using Environmental Distractors in the Diagnosis of ADHD. Front. Hum. Neurosci. 2013, 7, 805. [Google Scholar] [CrossRef] [PubMed]
- Berger, I.; Cassuto, H. The Effect of Environmental Distractors Incorporation into a CPT on Sustained Attention and ADHD Diagnosis among Adolescents. J. Neurosci. Methods 2014, 222, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I.; Petersen, S.E. The Attention System of the Human Brain. Annu. Rev. Neurosci. 1990, 13, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Posner, M.I. The Attention System of the Human Brain: 20 Years After. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Just, M.A.; Carpenter, P.A. A Theory of Reading: From Eye Fixations to Comprehension. Psychol. Rev. 1980, 87, 329–354. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Wang, Q.; Liu, D.; Wang, J.; Zhu, Z.; Feng, L. Eye Tracking Metrics to Screen and Assess Cognitive Impairment in Patients with Neurological Disorders. Neurol. Sci. 2020, 41, 1697–1704. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.T.; Luke, S.G. Best Practices in Eye Tracking Research. Int. J. Psychophysiol. 2020, 155, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Elbaum, T.; Braw, Y.; Lev, A.; Rassovsky, Y. Attention-Deficit/Hyperactivity Disorder (Adhd): Integrating the Moxo-Dcpt with an Eye Tracker Enhances Diagnostic Precision. Sensors 2020, 20, 6386. [Google Scholar] [CrossRef] [PubMed]
- Lev, A.; Braw, Y.; Elbaum, T.; Wagner, M.; Rassovsky, Y. Eye Tracking During a Continuous Performance Test: Utility for Assessing ADHD Patients. J. Atten. Disord. 2020, 26, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Itti, L.; Koch, C.; Niebur, E. A Model of Saliency-Based Visual Attention for Rapid Scene Analysis. IEEE Trans. Pattern Anal. Mach. Intell. 1998, 20, 1254–1259. [Google Scholar] [CrossRef]
- Kooiker, M.J.G.; van der Steen, J.; Pel, J.J.M. Development of Salience-Driven and Visually-Guided Eye Movement Responses. J. Vis. 2016, 16, 18. [Google Scholar] [CrossRef]
- Krasich, K.; Biggs, A.T.; Brockmole, J.R. Attention Capture during Visual Search: The Consequences of Distractor Appeal, Familiarity, and Frequency. Vis. Cogn. 2018, 27, 260–278. [Google Scholar] [CrossRef]
- Born, S.; Kerzel, D.; Theeuwes, J. Evidence for a Dissociation between the Control of Oculomotor Capture and Disengagement. Exp. Brain Res. 2010, 208, 621–631. [Google Scholar] [CrossRef]
- Biggs, A.T.; Kreager, R.D.; Gibson, B.S.; Villano, M.; Crowell, C.R. Semantic and Affective Salience: The Role of Meaning and Preference in Attentional Capture and Disengagement. J. Exp. Psychol. Hum. Percept. Perform. 2012, 38, 531–541. [Google Scholar] [CrossRef]
- Forster, S.; Lavie, N. Attentional Capture by Entirely Irrelevant Distractors. Vis. Cogn. 2008, 16, 200–214. [Google Scholar] [CrossRef]
- Faraone, S.V.; Asherson, P.; Banaschewski, T.; Biederman, J.; Buitelaar, J.K.; Ramos-Quiroga, J.A.; Rohde, L.A.; Sonuga-Barke, E.J.S.; Tannock, R.; Franke, B. Attention-Deficit/Hyperactivity Disorder. Nat. Rev. Dis. Prim. 2015, 1, 15020. [Google Scholar] [CrossRef] [PubMed]
- Papagiannopoulou, E.A.; Chitty, K.M.; Hermens, D.F.; Hickie, I.B.; Lagopoulos, J. A Systematic Review and Meta-Analysis of Eye-Tracking Studies in Children with Autism Spectrum Disorders. Soc. Neurosci. 2014, 9, 1–23. [Google Scholar] [CrossRef]
- Lisk, S.; Vaswani, A.; Linetzky, M.; Bar-Haim, Y.; Lau, J.Y.F. Systematic Review and Meta-Analysis: Eye-Tracking of Attention to Threat in Child and Adolescent Anxiety. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 88–99.e1. [Google Scholar] [CrossRef] [PubMed]
- Levantini, V.; Muratori, P.; Inguaggiato, E.; Masi, G.; Milone, A.; Valente, E.; Tonacci, A.; Billeci, L. EYES Are The Window to the Mind: Eye-Tracking Technology as a Novel Approach to Study Clinical Characteristics of ADHD. Psychiatry Res. 2020, 290, 113135. [Google Scholar] [CrossRef]
- Achenbach, T.; Rescorla, L. Manual for the ASEBA School-Age Forms & Profiles: Child Behavior Checklist for Ages 6–18, Teacher’s Report Form, Youth Self-Report; Burlington: University of Vermont, Research Center for Children, Youth & Families. 2001. Available online: https://cir.nii.ac.jp/crid/1571698599245104896 (accessed on 15 August 2022).
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. NparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50, 1–23. [Google Scholar] [CrossRef]
- Ijff, D.M.; Aldenkamp, A.P. Cognitive Side-Effects of Antiepileptic Drugs in Children. Handb. Clin. Neurol. 2013, 111, 707–718. [Google Scholar]
- Hessels, R.S.; Hooge, I.T.C. Eye Tracking in Developmental Cognitive Neuroscience–The Good, the Bad and the Ugly. Dev. Cogn. Neurosci. 2019, 40, 100710. [Google Scholar] [CrossRef] [PubMed]
- Slobodin, O.; Cassuto, H.; Berger, I. Age-Related Changes in Distractibility: Developmental Trajectory of Sustained Attention in ADHD. J. Atten. Disord. 2018, 22, 1333–1343. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ADHD Diagnosis | Subgroup | ||||
|---|---|---|---|---|---|
| Yes | No | SE | NLD | TD | |
| N | 45 | 96 | 21 | 95 | 25 |
| Gender (%): | |||||
| Male | 80% | 62% | 67% | 67% | 68% |
| Female | 20% | 38% | 33% | 33% | 32% |
| Age range | 6–16 | 6–17 | 7–12 | 6–17 | 6–15 |
| Mean age (SD) | 10.56 (2.54) | 10.06 (2.64) | 9.81 (1.54) | 10.59 (2.70) | 9.16 (2.70) |
| ADHD diagnosis (%): | 100% | 0% | 29% | 40% | 4% |
| Psychoactive medication (%): | |||||
| Anti-epileptic drugs | 7% | 5% | 29% | 2% | 0% |
| SSRI’s | 0% | 1% | 0% | 1% | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sweere, D.J.J.; Pel, J.J.M.; Kooiker, M.J.G.; van Dijk, J.P.; van Gemert, E.J.J.M.; Hurks, P.P.M.; Klinkenberg, S.; Vermeulen, R.J.; Hendriksen, J.G.M. Clinical Utility of Eye Tracking in Assessing Distractibility in Children with Neurological Disorders or ADHD: A Cross-Sectional Study. Brain Sci. 2022, 12, 1369. https://doi.org/10.3390/brainsci12101369
Sweere DJJ, Pel JJM, Kooiker MJG, van Dijk JP, van Gemert EJJM, Hurks PPM, Klinkenberg S, Vermeulen RJ, Hendriksen JGM. Clinical Utility of Eye Tracking in Assessing Distractibility in Children with Neurological Disorders or ADHD: A Cross-Sectional Study. Brain Sciences. 2022; 12(10):1369. https://doi.org/10.3390/brainsci12101369
Chicago/Turabian StyleSweere, Dirk J. J., Johan J. M. Pel, Marlou J. G. Kooiker, Johannes P. van Dijk, Elizabeth J. J. M. van Gemert, Petra P. M. Hurks, Sylvia Klinkenberg, R. Jeroen Vermeulen, and Jos G. M. Hendriksen. 2022. "Clinical Utility of Eye Tracking in Assessing Distractibility in Children with Neurological Disorders or ADHD: A Cross-Sectional Study" Brain Sciences 12, no. 10: 1369. https://doi.org/10.3390/brainsci12101369
APA StyleSweere, D. J. J., Pel, J. J. M., Kooiker, M. J. G., van Dijk, J. P., van Gemert, E. J. J. M., Hurks, P. P. M., Klinkenberg, S., Vermeulen, R. J., & Hendriksen, J. G. M. (2022). Clinical Utility of Eye Tracking in Assessing Distractibility in Children with Neurological Disorders or ADHD: A Cross-Sectional Study. Brain Sciences, 12(10), 1369. https://doi.org/10.3390/brainsci12101369